Health Professional Report for Guardianship Application - NCAT Review
VerifiedAdded on 2022/11/13
|5
|1072
|364
Report
AI Summary
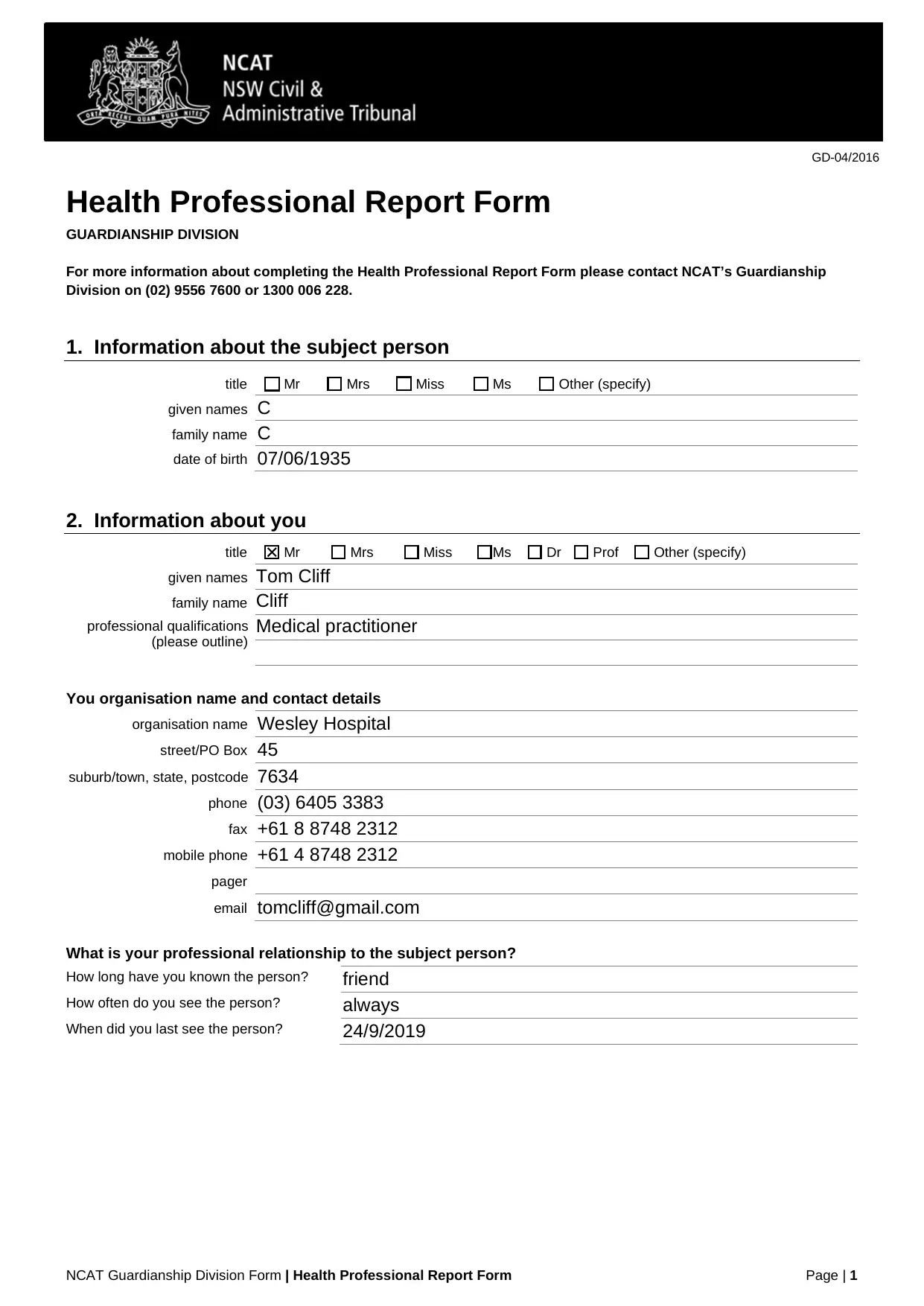
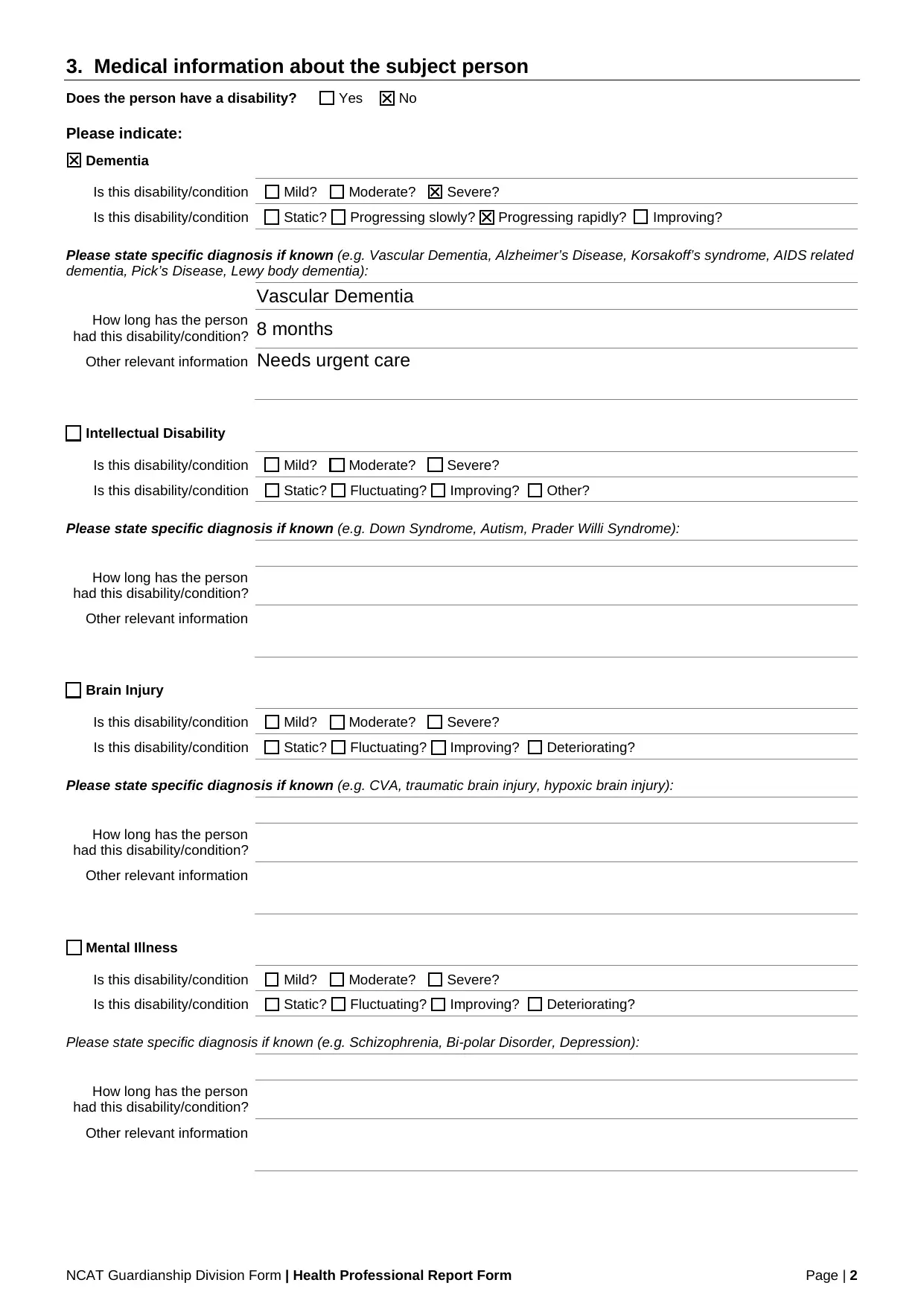
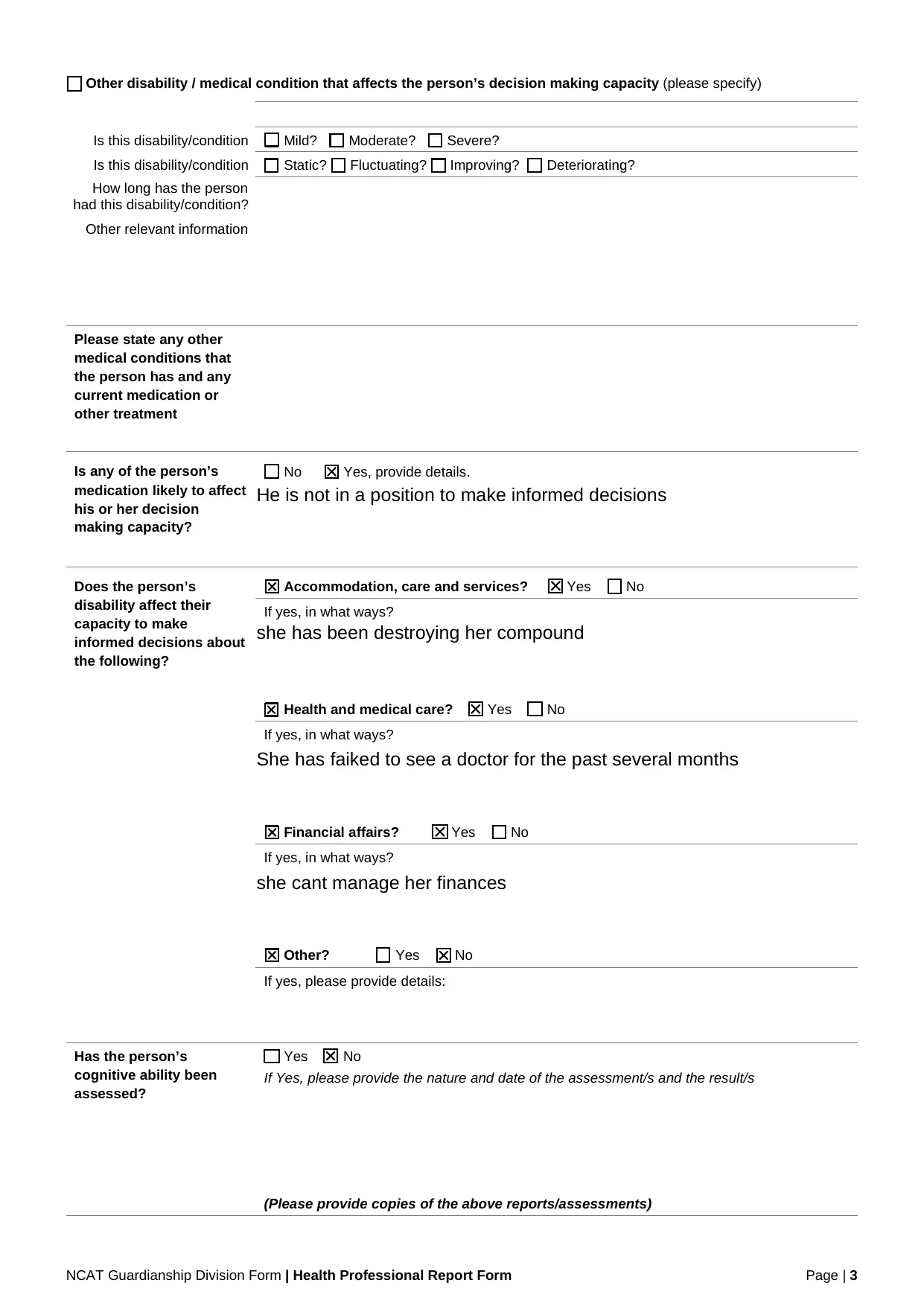
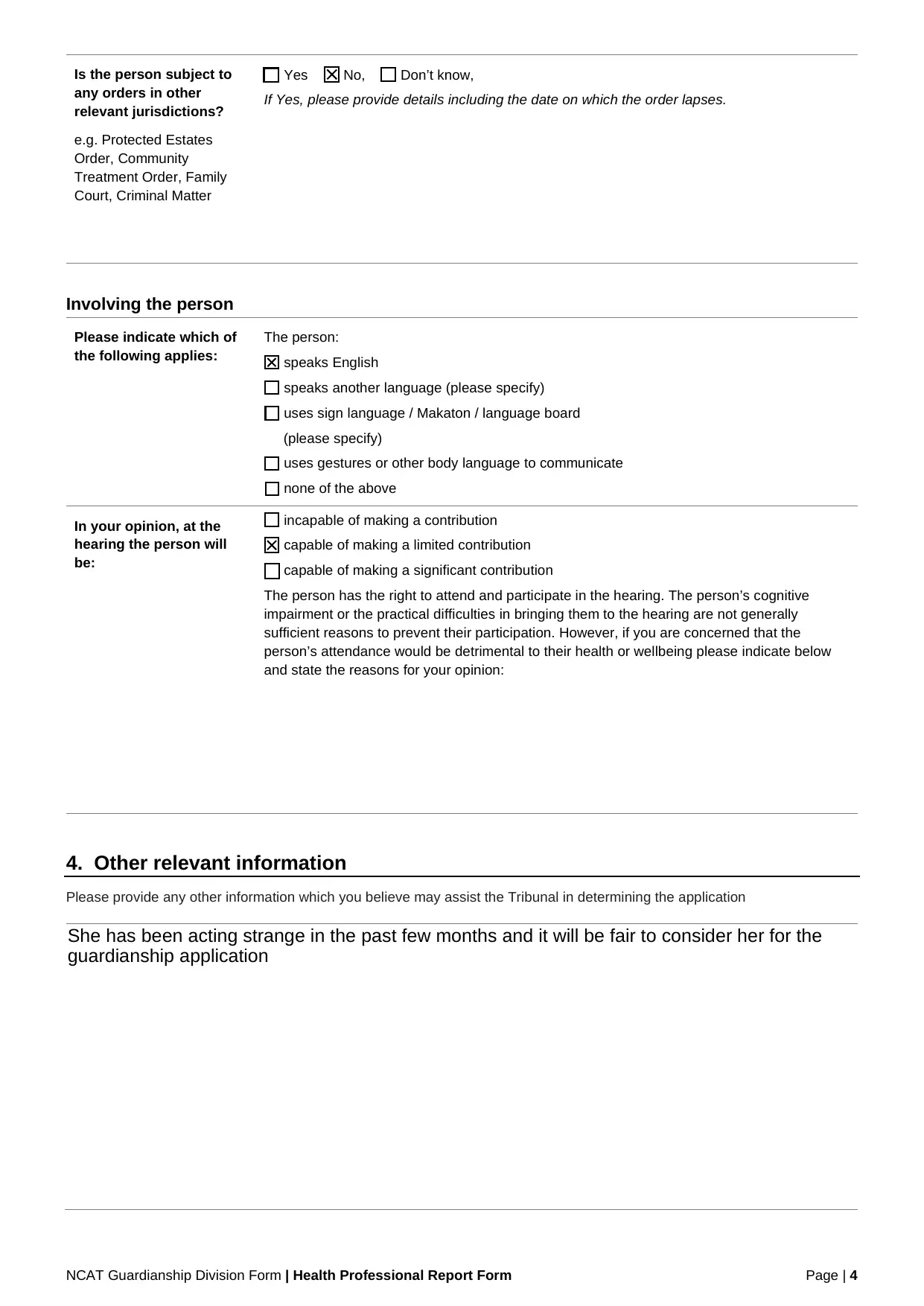
This assignment presents a Health Professional Report completed by Dr. Tom Cliff, a medical practitioner, regarding Mrs. C, an 84-year-old woman. The report, submitted to the NCAT Guardianship Division, details Mrs. C's medical condition, specifically Vascular Dementia, and its impact on her decision-making capacity. The report indicates Mrs. C's deteriorating condition, including her inability to manage her finances, make informed decisions about her accommodation, and her failure to seek medical attention. Dr. Cliff assesses her cognitive abilities and provides opinions on her capacity to participate in a hearing, suggesting that her attendance may not be in her best interest. The report also includes relevant information about Mrs. C's behavior, observed by her neighbors, which led to the guardianship application. The report concludes with a declaration from Dr. Cliff, attesting to the accuracy of the information and opinions provided. The report is a critical component of the guardianship application process, providing essential medical and cognitive assessments to aid the Tribunal in making decisions about Mrs. C's care and well-being.
1 out of 5


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.