Clinical Neuropsychology Case Study: PSP Diagnosis and Intervention
VerifiedAdded on 2020/02/19
|14
|3098
|83
Case Study
AI Summary
This case study presents a detailed neuropsychological analysis of a 66-year-old Vietnamese woman diagnosed with Progressive Supranuclear Palsy (PSP). The study explores the patient's history, symptoms, and cognitive impairments, including difficulties with memory, understanding information, and problem-solving. It details the assessment of results, differential diagnosis, and additional investigations using tools like the MOCA test. The case study also outlines an intervention plan employing the SBAR tool and emphasizes the importance of communication and a multidisciplinary approach to manage the challenges associated with PSP, including dyspraxia and co-morbid conditions like high blood pressure. The analysis highlights the patient's cognitive decline and the need for tailored support to maintain autonomy and address potential feelings of depression.

Running head: CLINICAL NEUROPSYCHOLOGY
Name of the student
University name
Author’s note
Name of the student
University name
Author’s note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
CLINICAL NEUROPSYCHOLOGY
Table of Contents
Introduction......................................................................................................................................2
Presentation of the case history.......................................................................................................2
Assessment of results.......................................................................................................................4
Differential diagnosis.......................................................................................................................6
Additional investigation (refer to the appendix).............................................................................7
Intervention plan..............................................................................................................................8
Conclusion.......................................................................................................................................9
References......................................................................................................................................11
Appendix........................................................................................................................................14
CLINICAL NEUROPSYCHOLOGY
Table of Contents
Introduction......................................................................................................................................2
Presentation of the case history.......................................................................................................2
Assessment of results.......................................................................................................................4
Differential diagnosis.......................................................................................................................6
Additional investigation (refer to the appendix).............................................................................7
Intervention plan..............................................................................................................................8
Conclusion.......................................................................................................................................9
References......................................................................................................................................11
Appendix........................................................................................................................................14
2
CLINICAL NEUROPSYCHOLOGY
Introduction
Neuropsychological testing is a vast area covering the complexities associated with
cognition and processing of information. The unravelling and the execution of the information
goes through a number of mental layers. The fully processed information is then executed into a
number of desirable actions. Thus, neuropsychology relates the functioning of the brain with
cognition, emotion and behaviour of an individual. The nerves can be defined as a set of wires
which forms an entangling network within the brain and is responsible for transforming and
decoding the packets of information into useful behaviour.
Evidences and studies have pointed at chemical imbalances along with epigenetic
mechanisms to be responsible for the malfunctioning of the brain. The report here presents a
detailed analysis of the neuropsychological complexities associated with a patient suffering from
supranuclear palsy. The case study has been further evaluated with the help of differential
diagnostic tools and mechanisms. The report presents a well investigated intervention plan for
managing the challenges and the adversities associated with the disease
Presentation of the case history
In the present case study the patient had been seen to be suffering from Progressive
Supranuclear Palsy (PSP). The condition could be described as a gradual degeneration of the
major areas of the brain resulting in loss of cognition and analytical skills in a person. The
disease could not be related to specific community, race or geography and is equally present both
in the males and the females. As commented by Parsons et al. (2017), no strong genetic pre-
disposition or link could be found for development of PSP. Reported study and analysis have
CLINICAL NEUROPSYCHOLOGY
Introduction
Neuropsychological testing is a vast area covering the complexities associated with
cognition and processing of information. The unravelling and the execution of the information
goes through a number of mental layers. The fully processed information is then executed into a
number of desirable actions. Thus, neuropsychology relates the functioning of the brain with
cognition, emotion and behaviour of an individual. The nerves can be defined as a set of wires
which forms an entangling network within the brain and is responsible for transforming and
decoding the packets of information into useful behaviour.
Evidences and studies have pointed at chemical imbalances along with epigenetic
mechanisms to be responsible for the malfunctioning of the brain. The report here presents a
detailed analysis of the neuropsychological complexities associated with a patient suffering from
supranuclear palsy. The case study has been further evaluated with the help of differential
diagnostic tools and mechanisms. The report presents a well investigated intervention plan for
managing the challenges and the adversities associated with the disease
Presentation of the case history
In the present case study the patient had been seen to be suffering from Progressive
Supranuclear Palsy (PSP). The condition could be described as a gradual degeneration of the
major areas of the brain resulting in loss of cognition and analytical skills in a person. The
disease could not be related to specific community, race or geography and is equally present both
in the males and the females. As commented by Parsons et al. (2017), no strong genetic pre-
disposition or link could be found for development of PSP. Reported study and analysis have
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
CLINICAL NEUROPSYCHOLOGY
found a variant in the gene for Tau protein called the H1 Haplotype, which is present on
chromosome number 17 and had been have linked with PSP. However, as argued by Sweet et al.
(2015), the presence of environmental factors and stress can also result in the accumulation of
the Tau protein in the brain. The Tau protein is accumulated in an insoluble form in
hyperphosphorylated form resulting in neurofibrillary of gliofibrillary tangles.
The patient here is a 66 year old Vietnamese right handed lady with ten years of formal
school education and had been diagnosed with progressive Supranuclear Palsy. The patient had
been able to perform her daily set of activities independently, though she became relatively slow.
The patient has been prescribed Livadopa and Motilium for her current dose of medication. The
Livadopa had been prescribed to her for controlling the development of parkinson’s and
Parkinson like symptoms. The patient had difficulty in breathing, sleeping and swallowing at
night. The patient had been known to have a history of mild dyspraxia. Dyspraxia or
developmental coordination disorder may be classified as lack of sensory perception, spatial
awareness and coordination. Further test revealed right frontotemporal cortical abnormalities
which made the patient more functional towards the right side. This is because the right side of
the body is controlled by the left cerebrum and left side by the right cerebrum. As commented by
Towns et al. (2017), dyspraxia comes under the specific learning disabilities group affecting
the concentration and the memory of the patient. The patient had shown difficulty in following
the hand gestures along with poor retropulsion, where the locomotor ability of the person is
affected. Additional co-morbidities such as mild ataxic high blood pressure were also reported
in the patient.
CLINICAL NEUROPSYCHOLOGY
found a variant in the gene for Tau protein called the H1 Haplotype, which is present on
chromosome number 17 and had been have linked with PSP. However, as argued by Sweet et al.
(2015), the presence of environmental factors and stress can also result in the accumulation of
the Tau protein in the brain. The Tau protein is accumulated in an insoluble form in
hyperphosphorylated form resulting in neurofibrillary of gliofibrillary tangles.
The patient here is a 66 year old Vietnamese right handed lady with ten years of formal
school education and had been diagnosed with progressive Supranuclear Palsy. The patient had
been able to perform her daily set of activities independently, though she became relatively slow.
The patient has been prescribed Livadopa and Motilium for her current dose of medication. The
Livadopa had been prescribed to her for controlling the development of parkinson’s and
Parkinson like symptoms. The patient had difficulty in breathing, sleeping and swallowing at
night. The patient had been known to have a history of mild dyspraxia. Dyspraxia or
developmental coordination disorder may be classified as lack of sensory perception, spatial
awareness and coordination. Further test revealed right frontotemporal cortical abnormalities
which made the patient more functional towards the right side. This is because the right side of
the body is controlled by the left cerebrum and left side by the right cerebrum. As commented by
Towns et al. (2017), dyspraxia comes under the specific learning disabilities group affecting
the concentration and the memory of the patient. The patient had shown difficulty in following
the hand gestures along with poor retropulsion, where the locomotor ability of the person is
affected. Additional co-morbidities such as mild ataxic high blood pressure were also reported
in the patient.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
CLINICAL NEUROPSYCHOLOGY
Assessment of results
The patient had been seen to be suffering from a number of co-morbid conditions such as
mild dyspraxia along with supranuclear palsy. The Supranuclear palsy affects the cognition and
the processing power of the brain by causing gradual degeneration of the nerves (Sweet et al.
2015). Additionally, the patient had been found to possess mild ataxic high blood pressure. The
effects of dyspraxia along with supranuclear palsy could be related to slowed speech and
movements in the patient. The patient has shown a depressive behaviour throughout the
assessment session. This could be attributed to the locomotor impairments possessed by the
patient, which restricted her daily set of activities. Additionally, the patient had been suffering
from sleeping and swallowing difficulties especially at night. The situation could be attributed to
dysphagia where muscular and nervous tension might restrict the movement of the food down
the oesophagus. As mentioned by Golden & Vicente (2013), dysphagia is often confused with
the onset of Parkinson’s . However, dysphagia like symptoms could also be expressed in event of
Gastroeosophagul reflux disorder.
The clinical assessment of the symptoms expressed by the 66 year old lady suffering
from supranuclear palsy showed a variety of conditions which had been recorded for further
analysis. The data recorded from the neuropsychological testing of the patient were evaluated
further for the assessment of the severity of the clinical condition suffered by the patient. In this
context, the patient had reportedly provided a borderline response to the test. The scaled score
was recorded at 4.7, the index score was recorded at 75 and the patient recorded a percentile
score of 5th, which was near to the borderline. The data recorded helped in analysis of the mental
agility of the patient which further governs the responsiveness of the patient to particular
CLINICAL NEUROPSYCHOLOGY
Assessment of results
The patient had been seen to be suffering from a number of co-morbid conditions such as
mild dyspraxia along with supranuclear palsy. The Supranuclear palsy affects the cognition and
the processing power of the brain by causing gradual degeneration of the nerves (Sweet et al.
2015). Additionally, the patient had been found to possess mild ataxic high blood pressure. The
effects of dyspraxia along with supranuclear palsy could be related to slowed speech and
movements in the patient. The patient has shown a depressive behaviour throughout the
assessment session. This could be attributed to the locomotor impairments possessed by the
patient, which restricted her daily set of activities. Additionally, the patient had been suffering
from sleeping and swallowing difficulties especially at night. The situation could be attributed to
dysphagia where muscular and nervous tension might restrict the movement of the food down
the oesophagus. As mentioned by Golden & Vicente (2013), dysphagia is often confused with
the onset of Parkinson’s . However, dysphagia like symptoms could also be expressed in event of
Gastroeosophagul reflux disorder.
The clinical assessment of the symptoms expressed by the 66 year old lady suffering
from supranuclear palsy showed a variety of conditions which had been recorded for further
analysis. The data recorded from the neuropsychological testing of the patient were evaluated
further for the assessment of the severity of the clinical condition suffered by the patient. In this
context, the patient had reportedly provided a borderline response to the test. The scaled score
was recorded at 4.7, the index score was recorded at 75 and the patient recorded a percentile
score of 5th, which was near to the borderline. The data recorded helped in analysis of the mental
agility of the patient which further governs the responsiveness of the patient to particular
5
CLINICAL NEUROPSYCHOLOGY
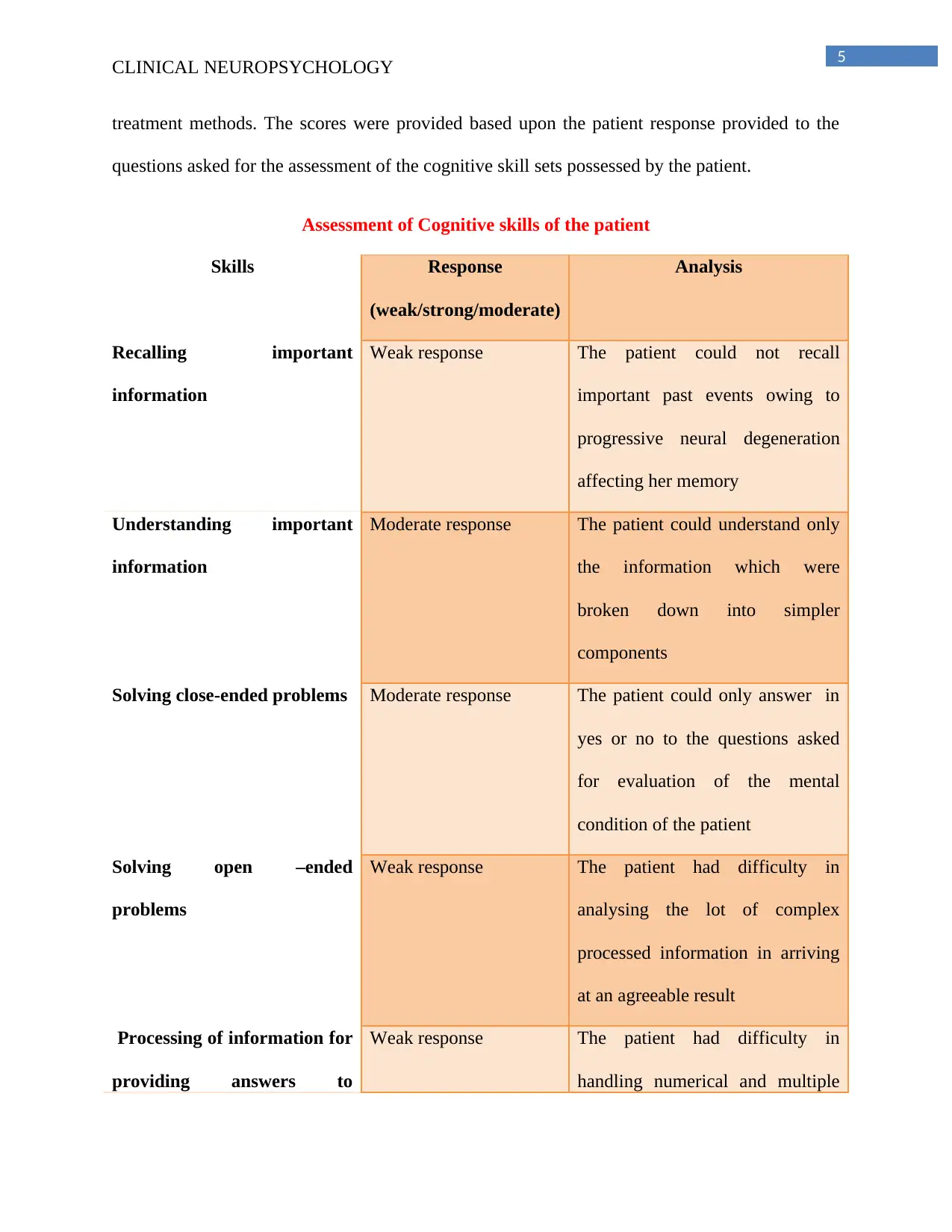
treatment methods. The scores were provided based upon the patient response provided to the
questions asked for the assessment of the cognitive skill sets possessed by the patient.
Assessment of Cognitive skills of the patient
Skills Response
(weak/strong/moderate)
Analysis
Recalling important
information
Weak response The patient could not recall
important past events owing to
progressive neural degeneration
affecting her memory
Understanding important
information
Moderate response The patient could understand only
the information which were
broken down into simpler
components
Solving close-ended problems Moderate response The patient could only answer in
yes or no to the questions asked
for evaluation of the mental
condition of the patient
Solving open –ended
problems
Weak response The patient had difficulty in
analysing the lot of complex
processed information in arriving
at an agreeable result
Processing of information for
providing answers to
Weak response The patient had difficulty in
handling numerical and multiple
CLINICAL NEUROPSYCHOLOGY
treatment methods. The scores were provided based upon the patient response provided to the
questions asked for the assessment of the cognitive skill sets possessed by the patient.
Assessment of Cognitive skills of the patient
Skills Response
(weak/strong/moderate)
Analysis
Recalling important
information
Weak response The patient could not recall
important past events owing to
progressive neural degeneration
affecting her memory
Understanding important
information
Moderate response The patient could understand only
the information which were
broken down into simpler
components
Solving close-ended problems Moderate response The patient could only answer in
yes or no to the questions asked
for evaluation of the mental
condition of the patient
Solving open –ended
problems
Weak response The patient had difficulty in
analysing the lot of complex
processed information in arriving
at an agreeable result
Processing of information for
providing answers to
Weak response The patient had difficulty in
handling numerical and multiple
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
CLINICAL NEUROPSYCHOLOGY
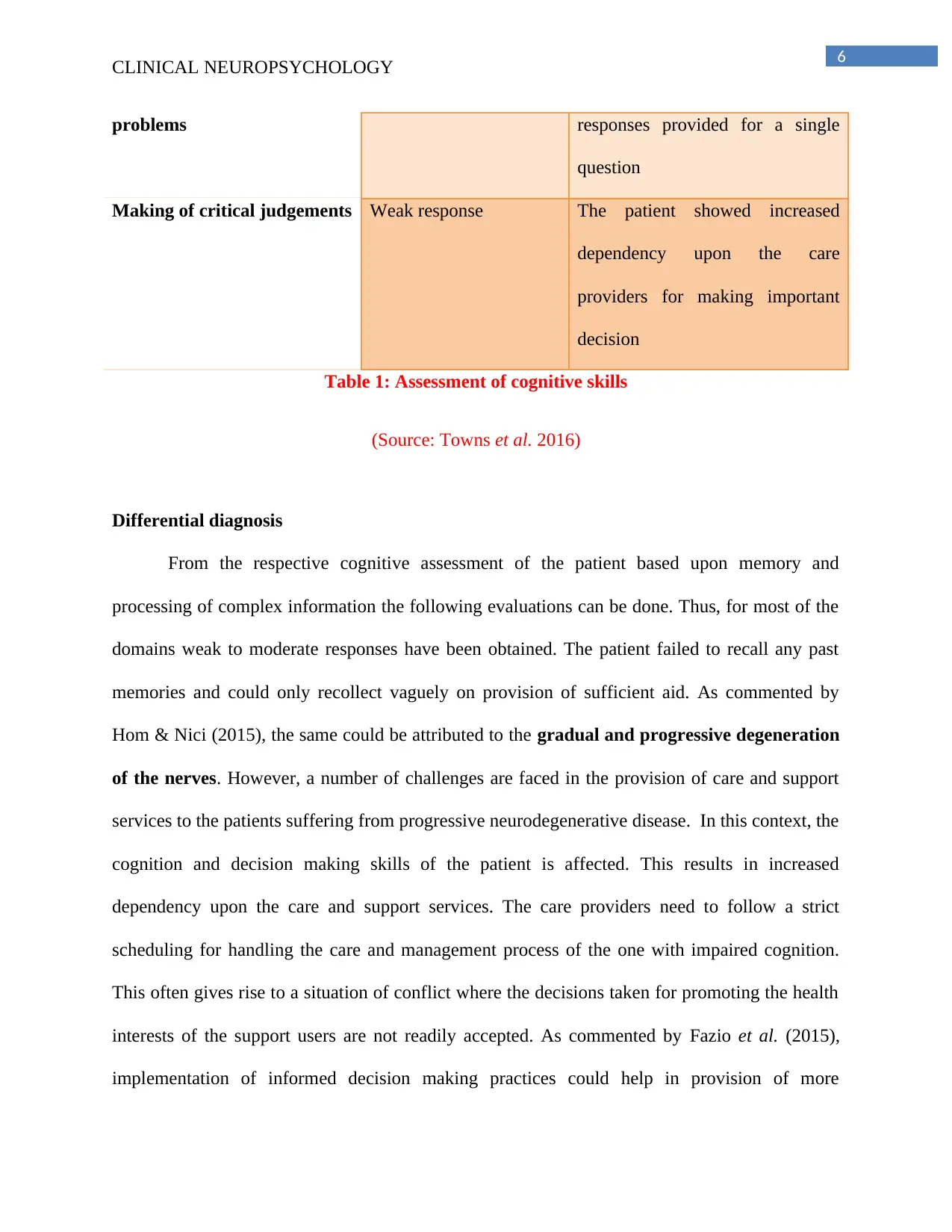
problems responses provided for a single
question
Making of critical judgements Weak response The patient showed increased
dependency upon the care
providers for making important
decision
Table 1: Assessment of cognitive skills
(Source: Towns et al. 2016)
Differential diagnosis
From the respective cognitive assessment of the patient based upon memory and
processing of complex information the following evaluations can be done. Thus, for most of the
domains weak to moderate responses have been obtained. The patient failed to recall any past
memories and could only recollect vaguely on provision of sufficient aid. As commented by
Hom & Nici (2015), the same could be attributed to the gradual and progressive degeneration
of the nerves. However, a number of challenges are faced in the provision of care and support
services to the patients suffering from progressive neurodegenerative disease. In this context, the
cognition and decision making skills of the patient is affected. This results in increased
dependency upon the care and support services. The care providers need to follow a strict
scheduling for handling the care and management process of the one with impaired cognition.
This often gives rise to a situation of conflict where the decisions taken for promoting the health
interests of the support users are not readily accepted. As commented by Fazio et al. (2015),
implementation of informed decision making practices could help in provision of more
CLINICAL NEUROPSYCHOLOGY
problems responses provided for a single
question
Making of critical judgements Weak response The patient showed increased
dependency upon the care
providers for making important
decision
Table 1: Assessment of cognitive skills
(Source: Towns et al. 2016)
Differential diagnosis
From the respective cognitive assessment of the patient based upon memory and
processing of complex information the following evaluations can be done. Thus, for most of the
domains weak to moderate responses have been obtained. The patient failed to recall any past
memories and could only recollect vaguely on provision of sufficient aid. As commented by
Hom & Nici (2015), the same could be attributed to the gradual and progressive degeneration
of the nerves. However, a number of challenges are faced in the provision of care and support
services to the patients suffering from progressive neurodegenerative disease. In this context, the
cognition and decision making skills of the patient is affected. This results in increased
dependency upon the care and support services. The care providers need to follow a strict
scheduling for handling the care and management process of the one with impaired cognition.
This often gives rise to a situation of conflict where the decisions taken for promoting the health
interests of the support users are not readily accepted. As commented by Fazio et al. (2015),
implementation of informed decision making practices could help in provision of more
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
CLINICAL NEUROPSYCHOLOGY
cooperative services to the support users. In this context, lack of communication often becomes a
limiting factor where the support professionals looking after the care needs of the patients may
not be able to receive complete and relevant information due to language barriers. Here, the
woman could barely speak or understand English.
Additional investigation (refer to the appendix)
The patient had a past history of developmental coordination disorder. Thus, the patient
had been subjected to a spectrum of disabilities, which affected her growth and optimal
development. Therefore, a simple argument could be made, where the patient became a victim to
progressive supranuclear palsy owing to long history of dyspraxia. The patient had difficulty in
swallowing as an exaggeration of the symptoms of PSP. The patient was also put on medication
such as Livadopa. The Livadopa had been seen to reduce the effect of Parkinson’s like symptoms
within an individual (Uzzell et al. 2013). In this context, multidisciplinary treatment options could
be used for provision of effective solution to the clinical distress faced by the patient over here.
The patient had been suffering from PSP along with exhibiting mild conditions for dyspraxia.
Therefore, the awareness to response and the decision making skills of the patient could be
severely impaired. This might affect the data collection procedure, where the patient may not be
able to report sufficient details to the care and support service provider. Thus, using evidence
based tools such as the Montreal Cognitive Assessment (MOCA) can be used to analyse the
mental health of the patient. The MOCA test is used to analyse the mild cognitive impairments in
individuals (Wiblin, Lee& Burn, 2017). It accesses the parameters such as attention, memory,
language skills, concentration along with thinking, calculating and visuoconstructional skills of
an individual. The time allotted for administering the test is a maximum of is approximately 10
minutes. A score of 26 or above is considered normal, however a score much below could
CLINICAL NEUROPSYCHOLOGY
cooperative services to the support users. In this context, lack of communication often becomes a
limiting factor where the support professionals looking after the care needs of the patients may
not be able to receive complete and relevant information due to language barriers. Here, the
woman could barely speak or understand English.
Additional investigation (refer to the appendix)
The patient had a past history of developmental coordination disorder. Thus, the patient
had been subjected to a spectrum of disabilities, which affected her growth and optimal
development. Therefore, a simple argument could be made, where the patient became a victim to
progressive supranuclear palsy owing to long history of dyspraxia. The patient had difficulty in
swallowing as an exaggeration of the symptoms of PSP. The patient was also put on medication
such as Livadopa. The Livadopa had been seen to reduce the effect of Parkinson’s like symptoms
within an individual (Uzzell et al. 2013). In this context, multidisciplinary treatment options could
be used for provision of effective solution to the clinical distress faced by the patient over here.
The patient had been suffering from PSP along with exhibiting mild conditions for dyspraxia.
Therefore, the awareness to response and the decision making skills of the patient could be
severely impaired. This might affect the data collection procedure, where the patient may not be
able to report sufficient details to the care and support service provider. Thus, using evidence
based tools such as the Montreal Cognitive Assessment (MOCA) can be used to analyse the
mental health of the patient. The MOCA test is used to analyse the mild cognitive impairments in
individuals (Wiblin, Lee& Burn, 2017). It accesses the parameters such as attention, memory,
language skills, concentration along with thinking, calculating and visuoconstructional skills of
an individual. The time allotted for administering the test is a maximum of is approximately 10
minutes. A score of 26 or above is considered normal, however a score much below could
8
CLINICAL NEUROPSYCHOLOGY
indicate moderate to severe cognitive impairments. In this context the patient recorded a score of
18 which is much below the normally accepted standard. Further patient data and analysis have
been provided though a table later.
The assessment method adopted here was simply questioning and reinstating the mere
facts to the patient in order to generate suitable responses which could be evaluated further for
designing of a suitable care plan for the patient. The MOCA framework mainly focuses upon
counselling methods for providing support and relief to the aggrieved patient. It justifies the
systematic diagnosis part where repeated questions are being asked to the patient in order to
arrive at the main problem statement.
Intervention plan
The intervention plan which could be implemented over here includes a SBAR tool
where the situation and patient background is assessment to provide a suitable recommendation.
The method could be simply implemented in order to analyse the loopholes present in the system
in the reporting and provision of effective treatment for PSP and associated co-morbidities. In
this context, effect communication procedures established within the clinical contexts can help in
the use of psychoanalytical and psychodynamic procedures for providing a comprehensive care
treatment plan. In this respect, the implementation of such methods can help in addressing the
specific concerns raised by the patient and their respective families. This helps in providing more
autonomy to the support user where the support user can choose from a wide area of clinical and
pharmacological treatment choices available.
Here, the patient had been suffering from supranuclear palsy where excessive
accumulation of the tau protein results in neurofibrillary tangles. The patient provides
CLINICAL NEUROPSYCHOLOGY
indicate moderate to severe cognitive impairments. In this context the patient recorded a score of
18 which is much below the normally accepted standard. Further patient data and analysis have
been provided though a table later.
The assessment method adopted here was simply questioning and reinstating the mere
facts to the patient in order to generate suitable responses which could be evaluated further for
designing of a suitable care plan for the patient. The MOCA framework mainly focuses upon
counselling methods for providing support and relief to the aggrieved patient. It justifies the
systematic diagnosis part where repeated questions are being asked to the patient in order to
arrive at the main problem statement.
Intervention plan
The intervention plan which could be implemented over here includes a SBAR tool
where the situation and patient background is assessment to provide a suitable recommendation.
The method could be simply implemented in order to analyse the loopholes present in the system
in the reporting and provision of effective treatment for PSP and associated co-morbidities. In
this context, effect communication procedures established within the clinical contexts can help in
the use of psychoanalytical and psychodynamic procedures for providing a comprehensive care
treatment plan. In this respect, the implementation of such methods can help in addressing the
specific concerns raised by the patient and their respective families. This helps in providing more
autonomy to the support user where the support user can choose from a wide area of clinical and
pharmacological treatment choices available.
Here, the patient had been suffering from supranuclear palsy where excessive
accumulation of the tau protein results in neurofibrillary tangles. The patient provides
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
CLINICAL NEUROPSYCHOLOGY
moderate responses to close ended questions, to understanding complex information only with
the help of an aid. Therefore, the cognition and decision making skills of an individual is
severely impacted under a degenerative disease. As commented by Salvatore et al. (2014),
increased dependence on other for decision making can reduce the autonomy of a service user.
This could result in the development of feelings of depression and agitation in an individual. In
this context, the registered nurse looking after the needs and concerns of the patient need to be
well connected with the doctors , psychologists, neurologists or other health care professionals.
This helps in providing catering to the emergency needs and demands of the support users. The
assessments methods could be expanded with due consultation with the doctors and other
healthcare professionals. As mentioned by Sako et al. (2017), inculcation of suitable diagnostic
and pharmacological intervention can help in catering to the developing needs of patient care.
Conclusion
On a concluding note, looking after the ones suffering from progressive neurodegenerative
requires increased cooperation from a number of healthcare channels along with expertise in the
areas of providing suitable intervention and care procedures for looking after the diverse and
complex issues faced by the patient. The patient here had been suffering from a number of
clinical and co-morbid conditions. Therefore, detailed medical along with diagnostic
interventions are required on a regular basis. This would help in accessing the progressive
improvement or deterioration in the health of the patient. Thus, implementation of effective
frameworks along with accessing the cognitive responses of the patient to a set of activities can
help in providing additional level of support services to the patient.
CLINICAL NEUROPSYCHOLOGY
moderate responses to close ended questions, to understanding complex information only with
the help of an aid. Therefore, the cognition and decision making skills of an individual is
severely impacted under a degenerative disease. As commented by Salvatore et al. (2014),
increased dependence on other for decision making can reduce the autonomy of a service user.
This could result in the development of feelings of depression and agitation in an individual. In
this context, the registered nurse looking after the needs and concerns of the patient need to be
well connected with the doctors , psychologists, neurologists or other health care professionals.
This helps in providing catering to the emergency needs and demands of the support users. The
assessments methods could be expanded with due consultation with the doctors and other
healthcare professionals. As mentioned by Sako et al. (2017), inculcation of suitable diagnostic
and pharmacological intervention can help in catering to the developing needs of patient care.
Conclusion
On a concluding note, looking after the ones suffering from progressive neurodegenerative
requires increased cooperation from a number of healthcare channels along with expertise in the
areas of providing suitable intervention and care procedures for looking after the diverse and
complex issues faced by the patient. The patient here had been suffering from a number of
clinical and co-morbid conditions. Therefore, detailed medical along with diagnostic
interventions are required on a regular basis. This would help in accessing the progressive
improvement or deterioration in the health of the patient. Thus, implementation of effective
frameworks along with accessing the cognitive responses of the patient to a set of activities can
help in providing additional level of support services to the patient.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
CLINICAL NEUROPSYCHOLOGY
References
Fazio, R. L., Sanders, J. F., Denney, R. L., Blake, M. L., Ott, S., Villanyi, E., ... & Ferreira, D.
(2015). The Official Journal of the National Academy of Neuropsychology Volume 30,
Number 4 2015. The Official Journal of the National Academy of
Neuropsychology, 30(4).
Golden, C. J., & Vicente, P. J. (Eds.). (2013). Foundations of clinical neuropsychology. Springer
Science & Business Media.
Hom, J., & Nici, J. (2015). Ralph M. Reitan: The Pioneer of Clinical Neuropsychology. Archives
of Clinical Neuropsychology, 30(8), 724-732.
Kim, Y. H., Ma, H. I., & Kim, Y. J. (2015). Utility of the midbrain tegmentum diameter in the
differential diagnosis of progressive supranuclear palsy from idiopathic Parkinson's
disease. Journal of Clinical Neurology, 11(3), 268-274.
Parsons, T. D., Carlew, A. R., Magtoto, J., & Stonecipher, K. (2017). The potential of function-
led virtual environments for ecologically valid measures of executive function in
experimental and clinical neuropsychology. Neuropsychological rehabilitation, 27(5),
777-807.
Sako, W., Murakami, N., Izumi, Y., & Kaji, R. (2017). Usefulness of the superior cerebellar
peduncle for differential diagnosis of progressive supranuclear palsy: A meta-
analysis. Journal of the Neurological Sciences, 378, 153-157.
Salvatore, C., Cerasa, A., Castiglioni, I., Gallivanone, F., Augimeri, A., Lopez, M., ... &
Quattrone, A. (2014). Machine learning on brain MRI data for differential diagnosis of
CLINICAL NEUROPSYCHOLOGY
References
Fazio, R. L., Sanders, J. F., Denney, R. L., Blake, M. L., Ott, S., Villanyi, E., ... & Ferreira, D.
(2015). The Official Journal of the National Academy of Neuropsychology Volume 30,
Number 4 2015. The Official Journal of the National Academy of
Neuropsychology, 30(4).
Golden, C. J., & Vicente, P. J. (Eds.). (2013). Foundations of clinical neuropsychology. Springer
Science & Business Media.
Hom, J., & Nici, J. (2015). Ralph M. Reitan: The Pioneer of Clinical Neuropsychology. Archives
of Clinical Neuropsychology, 30(8), 724-732.
Kim, Y. H., Ma, H. I., & Kim, Y. J. (2015). Utility of the midbrain tegmentum diameter in the
differential diagnosis of progressive supranuclear palsy from idiopathic Parkinson's
disease. Journal of Clinical Neurology, 11(3), 268-274.
Parsons, T. D., Carlew, A. R., Magtoto, J., & Stonecipher, K. (2017). The potential of function-
led virtual environments for ecologically valid measures of executive function in
experimental and clinical neuropsychology. Neuropsychological rehabilitation, 27(5),
777-807.
Sako, W., Murakami, N., Izumi, Y., & Kaji, R. (2017). Usefulness of the superior cerebellar
peduncle for differential diagnosis of progressive supranuclear palsy: A meta-
analysis. Journal of the Neurological Sciences, 378, 153-157.
Salvatore, C., Cerasa, A., Castiglioni, I., Gallivanone, F., Augimeri, A., Lopez, M., ... &
Quattrone, A. (2014). Machine learning on brain MRI data for differential diagnosis of
11
CLINICAL NEUROPSYCHOLOGY
Parkinson's disease and Progressive Supranuclear Palsy. Journal of Neuroscience
Methods, 222, 230-237.
Stamelou, M., & Höglinger, G. (2016). A review of treatment options for Progressive
Supranuclear Palsy. CNS drugs, 30(7), 629-636.
Steffen, T. M., Boeve, B. F., Petersen, C. M., Dvorak, L., & Kantarci, K. (2014). Long-term
exercise training for an individual with mixed corticobasal degeneration and progressive
supranuclear palsy features: 10-year case report follow-up. Physical therapy, 94(2), 289-
296.
Sweet, J. J., Benson, L. M., Nelson, N. W., & Moberg, P. J. (2015). The American Academy of
Clinical Neuropsychology, National Academy of Neuropsychology, and Society for
Clinical Neuropsychology (APA Division 40) 2015 TCN professional practice and
‘salary survey’: Professional practices, beliefs, and incomes of US
neuropsychologists. The Clinical Neuropsychologist, 29(8), 1069-1162.
Takigawa, H., Kitayama, M., Wada‐Isoe, K., Kowa, H., & Nakashima, K. (2016). Prevalence of
progressive supranuclear palsy in Yonago: change throughout a decade. Brain and
behavior, 6(12).
Towns, S. J., Hahn-Ketter, A. E., Halpern, J., & Block, C. K. (2017). Trainee perspectives on
postdoctoral recruitment in clinical neuropsychology: reflections on commentaries by
Bodin and Grote (2016) and Nelson et al.(2016). The Clinical Neuropsychologist, 1-6.
Uzzell, B. P., Ponton, M., & Ardila, A. (Eds.). (2013). International handbook of cross-cultural
neuropsychology. Psychology Press.
CLINICAL NEUROPSYCHOLOGY
Parkinson's disease and Progressive Supranuclear Palsy. Journal of Neuroscience
Methods, 222, 230-237.
Stamelou, M., & Höglinger, G. (2016). A review of treatment options for Progressive
Supranuclear Palsy. CNS drugs, 30(7), 629-636.
Steffen, T. M., Boeve, B. F., Petersen, C. M., Dvorak, L., & Kantarci, K. (2014). Long-term
exercise training for an individual with mixed corticobasal degeneration and progressive
supranuclear palsy features: 10-year case report follow-up. Physical therapy, 94(2), 289-
296.
Sweet, J. J., Benson, L. M., Nelson, N. W., & Moberg, P. J. (2015). The American Academy of
Clinical Neuropsychology, National Academy of Neuropsychology, and Society for
Clinical Neuropsychology (APA Division 40) 2015 TCN professional practice and
‘salary survey’: Professional practices, beliefs, and incomes of US
neuropsychologists. The Clinical Neuropsychologist, 29(8), 1069-1162.
Takigawa, H., Kitayama, M., Wada‐Isoe, K., Kowa, H., & Nakashima, K. (2016). Prevalence of
progressive supranuclear palsy in Yonago: change throughout a decade. Brain and
behavior, 6(12).
Towns, S. J., Hahn-Ketter, A. E., Halpern, J., & Block, C. K. (2017). Trainee perspectives on
postdoctoral recruitment in clinical neuropsychology: reflections on commentaries by
Bodin and Grote (2016) and Nelson et al.(2016). The Clinical Neuropsychologist, 1-6.
Uzzell, B. P., Ponton, M., & Ardila, A. (Eds.). (2013). International handbook of cross-cultural
neuropsychology. Psychology Press.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.