ACU NRSG355: Time Management, Delegation, and Patient Care
VerifiedAdded on 2022/10/15
|12
|2956
|62
Homework Assignment
AI Summary
This document presents a detailed solution for the NRSG355 assignment, focusing on clinical integration and professional practice within a nursing context. The assignment addresses key aspects such as prioritization and delegation in critical situations, collaborative and therapeutic practices within multidisciplinary healthcare teams, provision and coordination of patient care, and effective time management strategies. The solution includes a structured approach to problem-solving, utilizing case studies to illustrate practical application of theoretical concepts. It emphasizes the importance of clinical decision-making, the roles of various healthcare professionals, and the significance of patient-centered care. Furthermore, the assignment highlights the challenges of staff shortages and the implementation of shared care models. The student provides well-supported rationales for all decisions, referencing relevant literature to support their claims. The document demonstrates a strong understanding of nursing principles and their application in real-world clinical scenarios. The assignment also covers the scope of practice and delegation, time management, and clinical decision-making.
1
TEMPLATE: NRSG355 WRITTEN ASSESSMENT
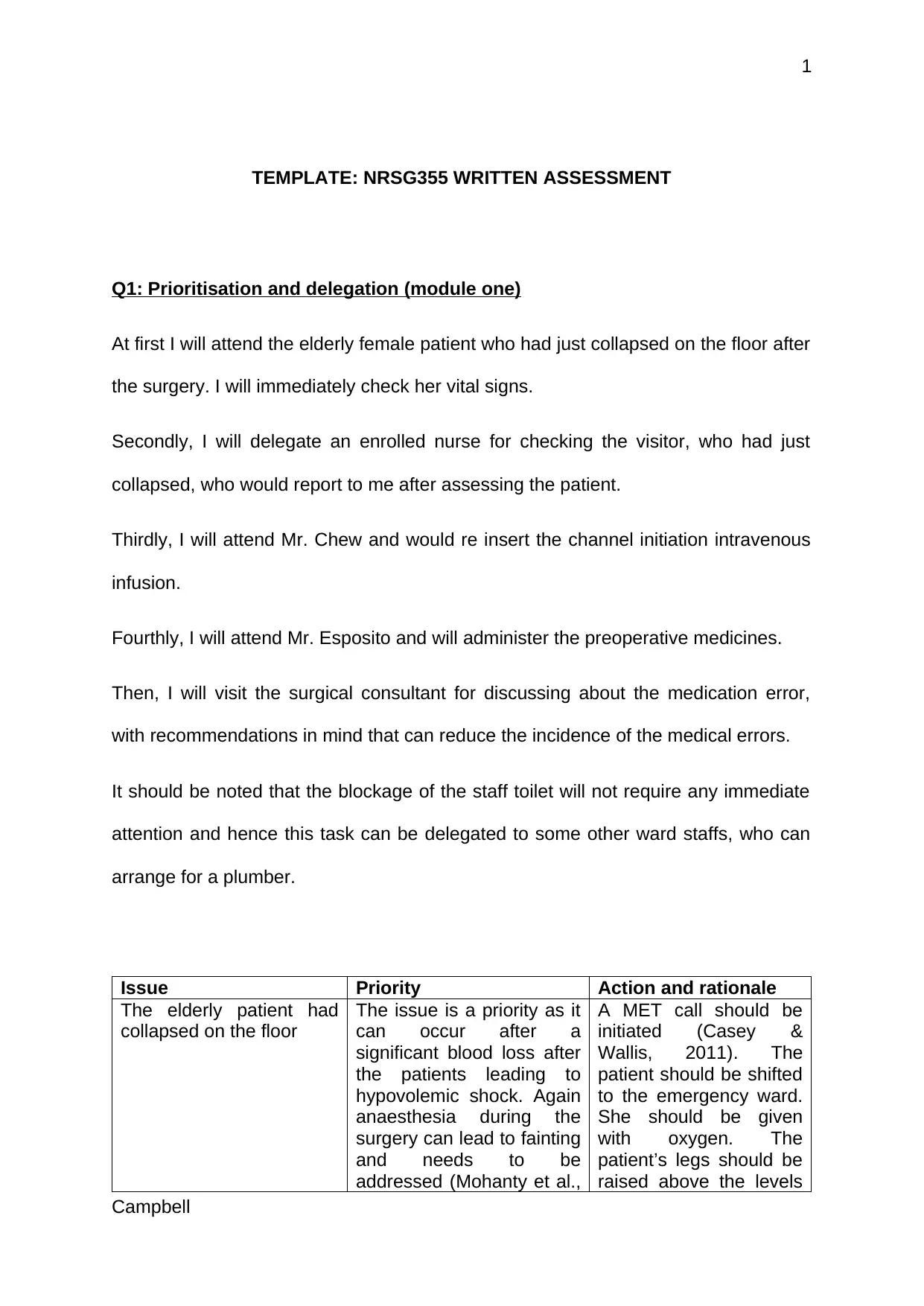
Q1: Prioritisation and delegation (module one)
At first I will attend the elderly female patient who had just collapsed on the floor after
the surgery. I will immediately check her vital signs.
Secondly, I will delegate an enrolled nurse for checking the visitor, who had just
collapsed, who would report to me after assessing the patient.
Thirdly, I will attend Mr. Chew and would re insert the channel initiation intravenous
infusion.
Fourthly, I will attend Mr. Esposito and will administer the preoperative medicines.
Then, I will visit the surgical consultant for discussing about the medication error,
with recommendations in mind that can reduce the incidence of the medical errors.
It should be noted that the blockage of the staff toilet will not require any immediate
attention and hence this task can be delegated to some other ward staffs, who can
arrange for a plumber.
Issue Priority Action and rationale
The elderly patient had
collapsed on the floor
The issue is a priority as it
can occur after a
significant blood loss after
the patients leading to
hypovolemic shock. Again
anaesthesia during the
surgery can lead to fainting
and needs to be
addressed (Mohanty et al.,
A MET call should be
initiated (Casey &
Wallis, 2011). The
patient should be shifted
to the emergency ward.
She should be given
with oxygen. The
patient’s legs should be
raised above the levels
Campbell
TEMPLATE: NRSG355 WRITTEN ASSESSMENT
Q1: Prioritisation and delegation (module one)
At first I will attend the elderly female patient who had just collapsed on the floor after
the surgery. I will immediately check her vital signs.
Secondly, I will delegate an enrolled nurse for checking the visitor, who had just
collapsed, who would report to me after assessing the patient.
Thirdly, I will attend Mr. Chew and would re insert the channel initiation intravenous
infusion.
Fourthly, I will attend Mr. Esposito and will administer the preoperative medicines.
Then, I will visit the surgical consultant for discussing about the medication error,
with recommendations in mind that can reduce the incidence of the medical errors.
It should be noted that the blockage of the staff toilet will not require any immediate
attention and hence this task can be delegated to some other ward staffs, who can
arrange for a plumber.
Issue Priority Action and rationale
The elderly patient had
collapsed on the floor
The issue is a priority as it
can occur after a
significant blood loss after
the patients leading to
hypovolemic shock. Again
anaesthesia during the
surgery can lead to fainting
and needs to be
addressed (Mohanty et al.,
A MET call should be
initiated (Casey &
Wallis, 2011). The
patient should be shifted
to the emergency ward.
She should be given
with oxygen. The
patient’s legs should be
raised above the levels
Campbell
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
2
2015). of the heart. If the
patient is not breathing,
CPR.
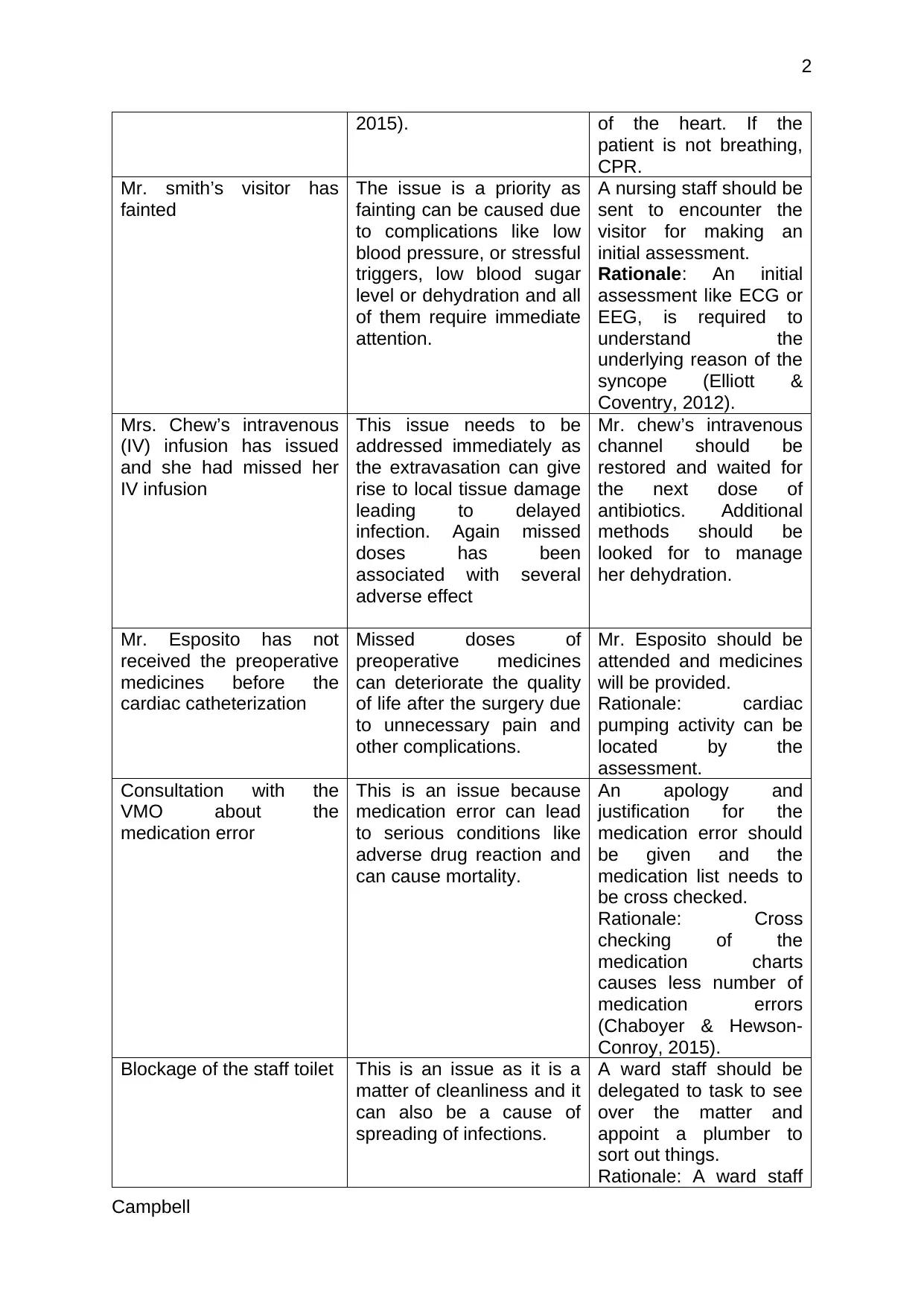
Mr. smith’s visitor has
fainted
The issue is a priority as
fainting can be caused due
to complications like low
blood pressure, or stressful
triggers, low blood sugar
level or dehydration and all
of them require immediate
attention.
A nursing staff should be
sent to encounter the
visitor for making an
initial assessment.
Rationale: An initial
assessment like ECG or
EEG, is required to
understand the
underlying reason of the
syncope (Elliott &
Coventry, 2012).
Mrs. Chew’s intravenous
(IV) infusion has issued
and she had missed her
IV infusion
This issue needs to be
addressed immediately as
the extravasation can give
rise to local tissue damage
leading to delayed
infection. Again missed
doses has been
associated with several
adverse effect
Mr. chew’s intravenous
channel should be
restored and waited for
the next dose of
antibiotics. Additional
methods should be
looked for to manage
her dehydration.
Mr. Esposito has not
received the preoperative
medicines before the
cardiac catheterization
Missed doses of
preoperative medicines
can deteriorate the quality
of life after the surgery due
to unnecessary pain and
other complications.
Mr. Esposito should be
attended and medicines
will be provided.
Rationale: cardiac
pumping activity can be
located by the
assessment.
Consultation with the
VMO about the
medication error
This is an issue because
medication error can lead
to serious conditions like
adverse drug reaction and
can cause mortality.
An apology and
justification for the
medication error should
be given and the
medication list needs to
be cross checked.
Rationale: Cross
checking of the
medication charts
causes less number of
medication errors
(Chaboyer & Hewson-
Conroy, 2015).
Blockage of the staff toilet This is an issue as it is a
matter of cleanliness and it
can also be a cause of
spreading of infections.
A ward staff should be
delegated to task to see
over the matter and
appoint a plumber to
sort out things.
Rationale: A ward staff
Campbell
2015). of the heart. If the
patient is not breathing,
CPR.
Mr. smith’s visitor has
fainted
The issue is a priority as
fainting can be caused due
to complications like low
blood pressure, or stressful
triggers, low blood sugar
level or dehydration and all
of them require immediate
attention.
A nursing staff should be
sent to encounter the
visitor for making an
initial assessment.
Rationale: An initial
assessment like ECG or
EEG, is required to
understand the
underlying reason of the
syncope (Elliott &
Coventry, 2012).
Mrs. Chew’s intravenous
(IV) infusion has issued
and she had missed her
IV infusion
This issue needs to be
addressed immediately as
the extravasation can give
rise to local tissue damage
leading to delayed
infection. Again missed
doses has been
associated with several
adverse effect
Mr. chew’s intravenous
channel should be
restored and waited for
the next dose of
antibiotics. Additional
methods should be
looked for to manage
her dehydration.
Mr. Esposito has not
received the preoperative
medicines before the
cardiac catheterization
Missed doses of
preoperative medicines
can deteriorate the quality
of life after the surgery due
to unnecessary pain and
other complications.
Mr. Esposito should be
attended and medicines
will be provided.
Rationale: cardiac
pumping activity can be
located by the
assessment.
Consultation with the
VMO about the
medication error
This is an issue because
medication error can lead
to serious conditions like
adverse drug reaction and
can cause mortality.
An apology and
justification for the
medication error should
be given and the
medication list needs to
be cross checked.
Rationale: Cross
checking of the
medication charts
causes less number of
medication errors
(Chaboyer & Hewson-
Conroy, 2015).
Blockage of the staff toilet This is an issue as it is a
matter of cleanliness and it
can also be a cause of
spreading of infections.
A ward staff should be
delegated to task to see
over the matter and
appoint a plumber to
sort out things.
Rationale: A ward staff
Campbell
3
will be deflated as this is
not an important issue to
be attended
immediately.
Q2: Collaborative and Therapeutic practice (module two)
(a) The Multidisciplinary team
i. Identify factors that determine which healthcare professionals are required to
be involved in a health care team?
The members of the multidisciplinary team includes physicians, nurses,
dieticians, physiotherapists, palliative care team, neurologist, occupational
therapist, a social workers, and psychologist and so on. The “teams” has been
found to be more effective than assigning health care professionals randomly to
the emergency rooms (Epstein, 2014). The members of the multidisciplinary
team depends upon the individual needs of the patient as well as the severity of
the clinical condition. A multidisciplinary team is formed on the basis of a plan of
care.
ii. Who should lead the health care team?
A team coordinator should be leading the health care team. Who will be included in
the health care team, depends upon the severity of the disease. It is not that that
doctors always should be the captain of the ship, but at times leaders can be a
physician, a pharmacist, a therapist or a nutritionist. Moreover they should focus on a
person-centred care (von Kodolitsch et al., 2016). A surgeon or an oncologist can
lead a multidisciplinary team for treating a cancer patient.
Campbell
will be deflated as this is
not an important issue to
be attended
immediately.
Q2: Collaborative and Therapeutic practice (module two)
(a) The Multidisciplinary team
i. Identify factors that determine which healthcare professionals are required to
be involved in a health care team?
The members of the multidisciplinary team includes physicians, nurses,
dieticians, physiotherapists, palliative care team, neurologist, occupational
therapist, a social workers, and psychologist and so on. The “teams” has been
found to be more effective than assigning health care professionals randomly to
the emergency rooms (Epstein, 2014). The members of the multidisciplinary
team depends upon the individual needs of the patient as well as the severity of
the clinical condition. A multidisciplinary team is formed on the basis of a plan of
care.
ii. Who should lead the health care team?
A team coordinator should be leading the health care team. Who will be included in
the health care team, depends upon the severity of the disease. It is not that that
doctors always should be the captain of the ship, but at times leaders can be a
physician, a pharmacist, a therapist or a nutritionist. Moreover they should focus on a
person-centred care (von Kodolitsch et al., 2016). A surgeon or an oncologist can
lead a multidisciplinary team for treating a cancer patient.
Campbell
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
4
iii. Who is the most important member of the health care team?
The patient is the most important member of a multidisciplinary team, as he/she
is the receiver of care. It is the duty of the physicians and the other medical
professionals to pay heed to the main member of the multidisciplinary team.
(b) Case study name: Case study 4
The case study gives the picture of a busy rehabilitation unit, where there had been
a recent turnover of the staffs in the physiotherapy department and a new
representation from the physiotherapy department has joined the healthcare team,
who is often absent and fails to provide patient updates.
i. Key issues identified
The key issues that has been identified is the recurring leave the worker had been
taking and his failure to provide patient updates.
Recurrent leaves can increase the workload on the other workers. Excessive
workload, on the other hand is related to stress and burnout among the other
workers. Again, missing patient updates can lead to clinical errors as nurses would
as work as per the instruction of physiotherapist. Lack of proper patient
documentation leads to negative patient outcomes.
ii. What strategies would you employ to address this situation?
In order to address such situation, I would at first enquire the reasons behind
the recurrent leaves. Leaves would only be granted for valid reasons. In case of any
Campbell
iii. Who is the most important member of the health care team?
The patient is the most important member of a multidisciplinary team, as he/she
is the receiver of care. It is the duty of the physicians and the other medical
professionals to pay heed to the main member of the multidisciplinary team.
(b) Case study name: Case study 4
The case study gives the picture of a busy rehabilitation unit, where there had been
a recent turnover of the staffs in the physiotherapy department and a new
representation from the physiotherapy department has joined the healthcare team,
who is often absent and fails to provide patient updates.
i. Key issues identified
The key issues that has been identified is the recurring leave the worker had been
taking and his failure to provide patient updates.
Recurrent leaves can increase the workload on the other workers. Excessive
workload, on the other hand is related to stress and burnout among the other
workers. Again, missing patient updates can lead to clinical errors as nurses would
as work as per the instruction of physiotherapist. Lack of proper patient
documentation leads to negative patient outcomes.
ii. What strategies would you employ to address this situation?
In order to address such situation, I would at first enquire the reasons behind
the recurrent leaves. Leaves would only be granted for valid reasons. In case of any
Campbell
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
5
health issue, the person will be suggested to visit a physicians. In valid cases, the
organisation would be ready to extend their hands of helps.
The staff should be called for a one-on-one conversation talking about the
misses occurring on part of the employee. He should be educated about the
importance of documentation. The employee should be kept under surveillance, yet
he should be given the full autonomy to carry out his tasks. A collaborative approach
along with the other health care team members would be useful in resolving any kind
of conflict (Kalishman, Stoddar & O’Sullivan, 2012). Close monitoring is necessary to
ensure that In case of repeated and intentional mistakes, the employee can be
penalised.
Q3: Provision and coordination of care (module three)
Questions that are needed to be asked to the nurse are as follows:-
As per the video links, Mr. Blogs has been suspected with Pneumonia, with the
formation of frothy sputum. He had a medical history of gastric ulcer, CVI (chronic
venous insufficiency) and a congestive heart failure. He is on 2L oxygen via nasal
prongs. He is having an IV infusion of Gentamycin. The urinal output is about 15
ml /day with reddish tinge indicating the presence of blood.
All these symptoms indicates towards the occurrence of urinary tract infection.
Urinary tract infection if left untreated, the infection can be carried from the lungs
through the blood stream and the urinary tract (Glassou, Hansen & Pedersen, 2017).
Assessment questions:-
Campbell
health issue, the person will be suggested to visit a physicians. In valid cases, the
organisation would be ready to extend their hands of helps.
The staff should be called for a one-on-one conversation talking about the
misses occurring on part of the employee. He should be educated about the
importance of documentation. The employee should be kept under surveillance, yet
he should be given the full autonomy to carry out his tasks. A collaborative approach
along with the other health care team members would be useful in resolving any kind
of conflict (Kalishman, Stoddar & O’Sullivan, 2012). Close monitoring is necessary to
ensure that In case of repeated and intentional mistakes, the employee can be
penalised.
Q3: Provision and coordination of care (module three)
Questions that are needed to be asked to the nurse are as follows:-
As per the video links, Mr. Blogs has been suspected with Pneumonia, with the
formation of frothy sputum. He had a medical history of gastric ulcer, CVI (chronic
venous insufficiency) and a congestive heart failure. He is on 2L oxygen via nasal
prongs. He is having an IV infusion of Gentamycin. The urinal output is about 15
ml /day with reddish tinge indicating the presence of blood.
All these symptoms indicates towards the occurrence of urinary tract infection.
Urinary tract infection if left untreated, the infection can be carried from the lungs
through the blood stream and the urinary tract (Glassou, Hansen & Pedersen, 2017).
Assessment questions:-
Campbell
6
Has the vital signs of the patient shown any improvement?
Where does he live? Has his next of kin (NOK) being notified?
What has the doctor suspected?
What are current tests that has been performed?
What is his GCS and resuscitation status?
Is he Nil-by- mouth? why?
Is he responding after the administration of the antibiotics?
Are there any specifications recommended by the doctor for this patient.
Assessments
The past medical records should be assessed once the patients gets into the ED.
After the admission procedure, all the vital signs of Mr. Blog, such as the
blood pressure, pulse rate, respiratory rate and the weight needs to be
checked.
Rationale: A chest x-ray needs to be scheduled, as the patient had been
suffering from Pneumonia. Measurement of body temperature is necessary,
as fever can be present due to infection (Miles et al., 2013). It is important to
measure the blood pressure as, too low pressure might indicate towards the
occurrence of septic shock. Again Pneumonia has been associated with
severe ischemic stroke causing elevated blood pressure.
A urine culture needs to be done in order find out the occurrence of UTI.
Rationale: For detecting the bacteria in the urine
A Duplex ultrasound can be done for the diagnosis of the chronic venous
insufficiency.
Rationale: It helps to examine the blood circulation through the body.
Campbell
Has the vital signs of the patient shown any improvement?
Where does he live? Has his next of kin (NOK) being notified?
What has the doctor suspected?
What are current tests that has been performed?
What is his GCS and resuscitation status?
Is he Nil-by- mouth? why?
Is he responding after the administration of the antibiotics?
Are there any specifications recommended by the doctor for this patient.
Assessments
The past medical records should be assessed once the patients gets into the ED.
After the admission procedure, all the vital signs of Mr. Blog, such as the
blood pressure, pulse rate, respiratory rate and the weight needs to be
checked.
Rationale: A chest x-ray needs to be scheduled, as the patient had been
suffering from Pneumonia. Measurement of body temperature is necessary,
as fever can be present due to infection (Miles et al., 2013). It is important to
measure the blood pressure as, too low pressure might indicate towards the
occurrence of septic shock. Again Pneumonia has been associated with
severe ischemic stroke causing elevated blood pressure.
A urine culture needs to be done in order find out the occurrence of UTI.
Rationale: For detecting the bacteria in the urine
A Duplex ultrasound can be done for the diagnosis of the chronic venous
insufficiency.
Rationale: It helps to examine the blood circulation through the body.
Campbell
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
7
Respiratory assessment can be made that consisted of inspection, palpation,
percussion and auscultation.
Rationale: Inspection of breathing patterns, skin colour can be assessed to
diagnose the presence of cyanosis. Palpation can be used for understanding
ventilation and percussion can be used to determine the inspissited fluid
accumulation due to pneumonia (van Vugt et al., 2017).
Skin check-To check the presence of cool or clammy skin.
Rationale: The skin colour might get bluish if there are insufficient oxygen
levels in the blood.
The patient should be assessed for fall risk by proper screening.
Rationale: Elderly patients are more prone to falls.
A pulse oximetry diagnosis is required to detect any occurrence of hypoxia.
Rationale: Hypoxia might result from lung damage due to infection.
Q4: Time management and delegation (module four)
Campbell
Respiratory assessment can be made that consisted of inspection, palpation,
percussion and auscultation.
Rationale: Inspection of breathing patterns, skin colour can be assessed to
diagnose the presence of cyanosis. Palpation can be used for understanding
ventilation and percussion can be used to determine the inspissited fluid
accumulation due to pneumonia (van Vugt et al., 2017).
Skin check-To check the presence of cool or clammy skin.
Rationale: The skin colour might get bluish if there are insufficient oxygen
levels in the blood.
The patient should be assessed for fall risk by proper screening.
Rationale: Elderly patients are more prone to falls.
A pulse oximetry diagnosis is required to detect any occurrence of hypoxia.
Rationale: Hypoxia might result from lung damage due to infection.
Q4: Time management and delegation (module four)
Campbell
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
8
It is evident from the case scenario, that there had been a shortage of staffs in
the clinical settings. In such a case, a shared care model can be used where the
skills and the knowledge of the health care professionals share a joint accountability
towards more than one patient (Campbell, Gilbert & Laustsen, 2010). This implied
surveillance and monitoring and swapping of the patient data and sharing skills and
knowledge between the disciplines.
According to the Nursing and the Midwifery Board of Australia, registered
nurses uses delegation, coordination, supervision, consultation in his/her
professional relationship for achieving improved health outcomes in the patient
(Nursing and Midwifery Board of Australia, 2017). It is role of the RNs to
appropriately delegate duties to the enrolled nurses within their scope of nursing
practice and effectively provides timely directions and supervision for ensuring that
the delegate practice had been safe and correct (Nursing and Midwifery Board of
Australia, 2017).
One of the registered nurse and one AIN can be taken during surgery for
assisting the 8 patients at the time of surgery. It is the duty of the registered to
provide a safe, appropriate and responsive quality of nursing to the patients. The
enrolled nurses would assist the registered nurse and the physician at the time of
surgery. Normally their tasks should include administration of the pre-operative
medications, dressing the patient before and during recuperating from the surgery.
They might have to change the dressing, or establishing a new IV line.
Another registered nurse, one enrolled nurse and 2 AINs can be recruited for
the care of the rest 14 patients. One AIN can be allotted to take care of five patients
at time under the observation of the registered nurse. The enrolled nurse is
Campbell
It is evident from the case scenario, that there had been a shortage of staffs in
the clinical settings. In such a case, a shared care model can be used where the
skills and the knowledge of the health care professionals share a joint accountability
towards more than one patient (Campbell, Gilbert & Laustsen, 2010). This implied
surveillance and monitoring and swapping of the patient data and sharing skills and
knowledge between the disciplines.
According to the Nursing and the Midwifery Board of Australia, registered
nurses uses delegation, coordination, supervision, consultation in his/her
professional relationship for achieving improved health outcomes in the patient
(Nursing and Midwifery Board of Australia, 2017). It is role of the RNs to
appropriately delegate duties to the enrolled nurses within their scope of nursing
practice and effectively provides timely directions and supervision for ensuring that
the delegate practice had been safe and correct (Nursing and Midwifery Board of
Australia, 2017).
One of the registered nurse and one AIN can be taken during surgery for
assisting the 8 patients at the time of surgery. It is the duty of the registered to
provide a safe, appropriate and responsive quality of nursing to the patients. The
enrolled nurses would assist the registered nurse and the physician at the time of
surgery. Normally their tasks should include administration of the pre-operative
medications, dressing the patient before and during recuperating from the surgery.
They might have to change the dressing, or establishing a new IV line.
Another registered nurse, one enrolled nurse and 2 AINs can be recruited for
the care of the rest 14 patients. One AIN can be allotted to take care of five patients
at time under the observation of the registered nurse. The enrolled nurse is
Campbell
9
responsible for doing infusing IV to the post-operative patients. An AIN can
accompany the enrolled nurse and assist them with the necessary equipment for the
provision of IV infusion. The AIN should have a strong communication, empathy and
customer service skills. They should also assist patients with their daily routine like
showering, dressing, toileting, eating, medication, mobility and exercise regimen.
One of the professional standard of the nurses are to plan and negotiate as of how
practice will be evaluated with a stipulated time frame. Inefficient time management
can cause adverse outcomes and even mortality.
Campbell
responsible for doing infusing IV to the post-operative patients. An AIN can
accompany the enrolled nurse and assist them with the necessary equipment for the
provision of IV infusion. The AIN should have a strong communication, empathy and
customer service skills. They should also assist patients with their daily routine like
showering, dressing, toileting, eating, medication, mobility and exercise regimen.
One of the professional standard of the nurses are to plan and negotiate as of how
practice will be evaluated with a stipulated time frame. Inefficient time management
can cause adverse outcomes and even mortality.
Campbell
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
10
Reference List (APA style)
Campbell, L., Gilbert, M. & Laustsen, G. (2010). Clinical coach for nursing
excellence. Access date: 23.9.2019. Retrieved from
http://ezproxy.acu.edu.au/login?url=http://ACU.eblib.com/patron/FullRecord.as
px?p=474457
Casey, A. & Wallis, A. (2011). Effective communication: Principle of nursing practice.
Nursing Standard 25(32), 35-37. Retrieved from
http://ezproxy.acu.edu.au/login?url=https://search.ebscohost.com/login.aspx?
direct=true&db=ccm &AN=2011015656&site=ehost-live
Chaboyer, W. & Hewson-Conroy, K. (2015). Quality and safety. In: L. Aitken, D.
Marshall & W. Chaboyer (Eds.). ACCCN’s Critical Care Nursing, 3rd Ed.
Chatswood, NSW: Elsevier.
Coleman, J. J., Hodson, J., Brooks, H. L., & Rosser, D. (2013). Missed medication
doses in hospitalised patients: a descriptive account of quality improvement
measures and time series analysis. International journal for quality in health
care : journal of the International Society for Quality in Health Care, 25(5),
564–572. doi:10.1093/intqhc/mzt044
Elliott, M. Campbell& Coventry, A. (2012). Critical care: the eight vital signs of patient
monitoring. British Journal of Nursing, 21(10), 621-625. Retrieved from
http://ezproxy.acu.edu.au/login?url=https://search.ebscohost.com/login.aspx?
direct=true&db=ccm &AN=2011651321&site=ehost-live
Campbell
Reference List (APA style)
Campbell, L., Gilbert, M. & Laustsen, G. (2010). Clinical coach for nursing
excellence. Access date: 23.9.2019. Retrieved from
http://ezproxy.acu.edu.au/login?url=http://ACU.eblib.com/patron/FullRecord.as
px?p=474457
Casey, A. & Wallis, A. (2011). Effective communication: Principle of nursing practice.
Nursing Standard 25(32), 35-37. Retrieved from
http://ezproxy.acu.edu.au/login?url=https://search.ebscohost.com/login.aspx?
direct=true&db=ccm &AN=2011015656&site=ehost-live
Chaboyer, W. & Hewson-Conroy, K. (2015). Quality and safety. In: L. Aitken, D.
Marshall & W. Chaboyer (Eds.). ACCCN’s Critical Care Nursing, 3rd Ed.
Chatswood, NSW: Elsevier.
Coleman, J. J., Hodson, J., Brooks, H. L., & Rosser, D. (2013). Missed medication
doses in hospitalised patients: a descriptive account of quality improvement
measures and time series analysis. International journal for quality in health
care : journal of the International Society for Quality in Health Care, 25(5),
564–572. doi:10.1093/intqhc/mzt044
Elliott, M. Campbell& Coventry, A. (2012). Critical care: the eight vital signs of patient
monitoring. British Journal of Nursing, 21(10), 621-625. Retrieved from
http://ezproxy.acu.edu.au/login?url=https://search.ebscohost.com/login.aspx?
direct=true&db=ccm &AN=2011651321&site=ehost-live
Campbell
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
11
Epstein N. E. (2014). Multidisciplinary in-hospital teams improve patient outcomes: A
review. Surgical neurology international, 5(Suppl 7), S295–S303.
doi:10.4103/2152-7806.139612
Glassou, E. N., Hansen, T. B., & Pedersen, A. B. (2017). Risk of pneumonia and
urinary tract infection within the first week after total hip arthroplasty and the
impact on survival. Clinical epidemiology, 9, 31–39.
doi:10.2147/CLEP.S122829
Kalishman, S., Stoddard, H. & O’Sullivan, P. (2012). Don’t manage the conflict:
transform it through collaboration. Medical Education, 46, 926-934. DOI:
10.1111/j.1365-2923.2012.04342.x
Miles, A., Moore, S., McFarlane, M., Lee, F., Allen, J., & Huckabee, M. L. (2013).
Comparison of cough reflex test against instrumental assessment of
aspiration. Physiology & behavior, 118, 25-31.
MND Australia (2017). Australia Fact Sheet on Multidisciplinary Teams. Retrieved
form:
http://www.mndaust.asn.au/Get-informed/Information-resources/Living_better
_for_longer/WEB- MND-Australia-Fact-Sheet-EB3-Multidisciplinary.aspx
Mohanty, S., Dabas, J., Tandon, M. S., Singh, D., & Gulati, U. (2015). Post-operative
acute circulatory collapse following craniofacial surgery: Rare event and rarer
cause. National journal of maxillofacial surgery, 6(1), 93–95.
doi:10.4103/0975-5950.168220
Nursing and Midwifery Board of Australia, (2017). Registered nurse standards for
practice. Access date: 23.9.2019. Retrieved from:
Campbell
Epstein N. E. (2014). Multidisciplinary in-hospital teams improve patient outcomes: A
review. Surgical neurology international, 5(Suppl 7), S295–S303.
doi:10.4103/2152-7806.139612
Glassou, E. N., Hansen, T. B., & Pedersen, A. B. (2017). Risk of pneumonia and
urinary tract infection within the first week after total hip arthroplasty and the
impact on survival. Clinical epidemiology, 9, 31–39.
doi:10.2147/CLEP.S122829
Kalishman, S., Stoddard, H. & O’Sullivan, P. (2012). Don’t manage the conflict:
transform it through collaboration. Medical Education, 46, 926-934. DOI:
10.1111/j.1365-2923.2012.04342.x
Miles, A., Moore, S., McFarlane, M., Lee, F., Allen, J., & Huckabee, M. L. (2013).
Comparison of cough reflex test against instrumental assessment of
aspiration. Physiology & behavior, 118, 25-31.
MND Australia (2017). Australia Fact Sheet on Multidisciplinary Teams. Retrieved
form:
http://www.mndaust.asn.au/Get-informed/Information-resources/Living_better
_for_longer/WEB- MND-Australia-Fact-Sheet-EB3-Multidisciplinary.aspx
Mohanty, S., Dabas, J., Tandon, M. S., Singh, D., & Gulati, U. (2015). Post-operative
acute circulatory collapse following craniofacial surgery: Rare event and rarer
cause. National journal of maxillofacial surgery, 6(1), 93–95.
doi:10.4103/0975-5950.168220
Nursing and Midwifery Board of Australia, (2017). Registered nurse standards for
practice. Access date: 23.9.2019. Retrieved from:
Campbell
12
https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/
Professional-standards/registered-nurse-standards-for-practice.aspx
Reissig, A., Gramegna, A., & Aliberti, S. (2012). The role of lung ultrasound in the
diagnosis and follow-up of community-acquired pneumonia. European journal
of internal medicine, 23(5), 391-397.
https://doi.org/10.1016/j.ejim.2012.01.003
van Vugt, S. F., Verheij, T. J., de Jong, P. A., Butler, C. C., Hood, K., Coenen, S., ...
& Broekhuizen, B. D. (2013). Diagnosing pneumonia in patients with acute
cough: clinical judgment compared to chest radiography. European
Respiratory Journal, 42(4), 1076-1082. DOI: 10.1183/09031936.00111012
von Kodolitsch, Y., Rybczynski, M., Vogler, M., Mir, T. S., Schüler, H., Kutsche, K.,
… Pyeritz, R. E. (2016). The role of the multidisciplinary health care team in
the management of patients with Marfan syndrome. Journal of
multidisciplinary healthcare, 9, 587–614. doi:10.2147/JMDH.S93680
Campbell
https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/
Professional-standards/registered-nurse-standards-for-practice.aspx
Reissig, A., Gramegna, A., & Aliberti, S. (2012). The role of lung ultrasound in the
diagnosis and follow-up of community-acquired pneumonia. European journal
of internal medicine, 23(5), 391-397.
https://doi.org/10.1016/j.ejim.2012.01.003
van Vugt, S. F., Verheij, T. J., de Jong, P. A., Butler, C. C., Hood, K., Coenen, S., ...
& Broekhuizen, B. D. (2013). Diagnosing pneumonia in patients with acute
cough: clinical judgment compared to chest radiography. European
Respiratory Journal, 42(4), 1076-1082. DOI: 10.1183/09031936.00111012
von Kodolitsch, Y., Rybczynski, M., Vogler, M., Mir, T. S., Schüler, H., Kutsche, K.,
… Pyeritz, R. E. (2016). The role of the multidisciplinary health care team in
the management of patients with Marfan syndrome. Journal of
multidisciplinary healthcare, 9, 587–614. doi:10.2147/JMDH.S93680
Campbell
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.