University Mental Health Nursing Case Study Report: Mary
VerifiedAdded on 2023/06/09
|11
|2571
|203
Report
AI Summary
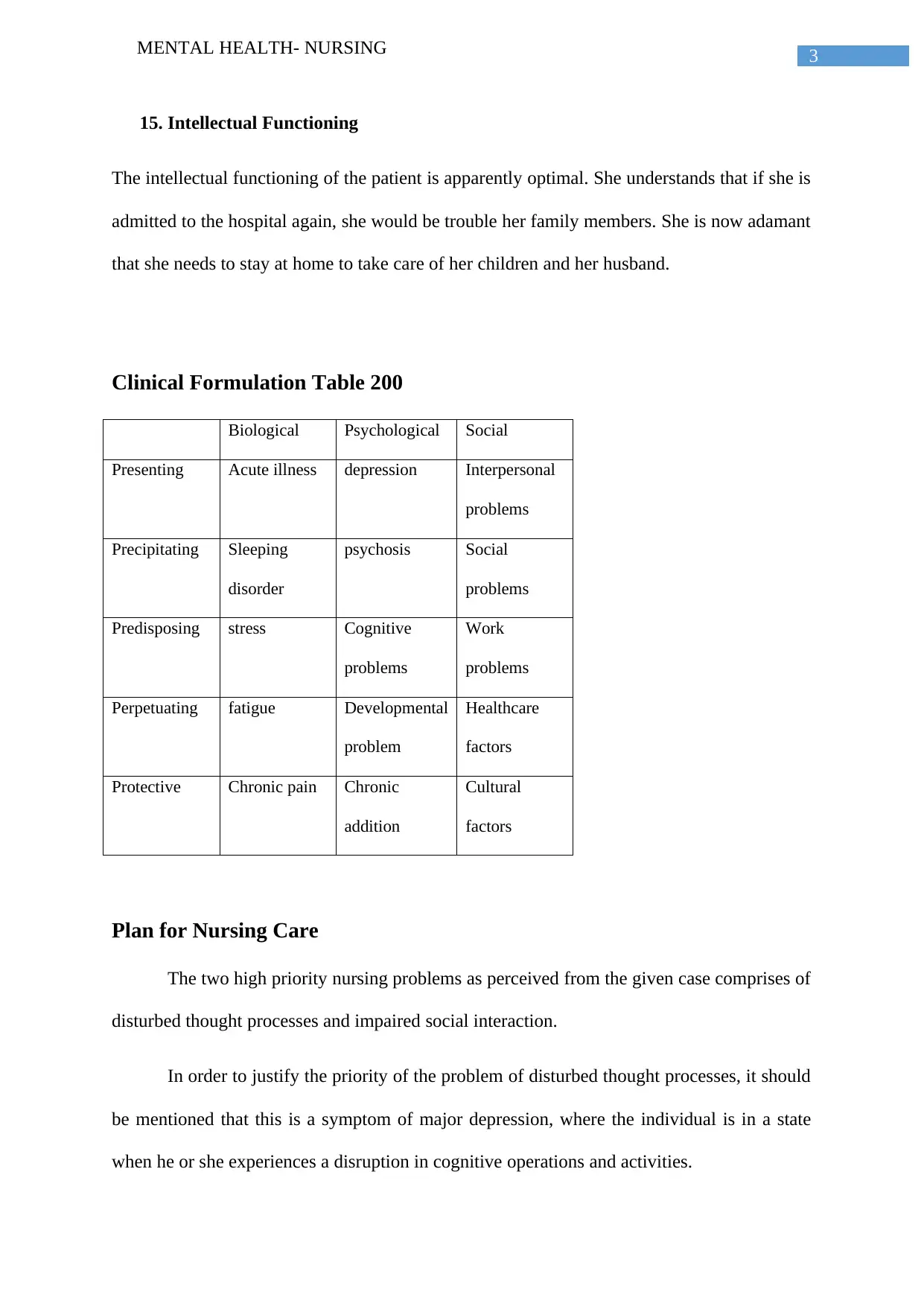
This report presents a comprehensive analysis of a mental health nursing case study focusing on a patient named Mary, diagnosed with depression. Part 1 of the report begins with a detailed mental status examination (MSE), assessing Mary's appearance, behavior, attitude, level of consciousness, speech, mood, affect, thought processes, thought content, suicidality, insight, judgment, attention span, memory, and intellectual functioning. A clinical formulation is then provided, summarizing biological, psychological, and social factors contributing to Mary's condition, followed by a prioritized nursing care plan addressing disturbed thought processes and impaired social interaction. The nursing interventions include determining the patient's cognitive function, providing ample time for responses, reducing responsibilities, identifying negative thoughts, and structuring family life. Interventions for impaired social interaction involve activities with minimal concentration, one-to-one activities, and group activities. Part 2 focuses on the therapeutic relationship, emphasizing its components and importance in predicting treatment response. The report also discusses cultural safety in providing care, highlighting the need for cultural competency and sensitivity to Mary's religious beliefs. Finally, the report explores recovery-oriented nursing care, aligning the interventions with the principles of self-direction, respect, person-centered care, empowerment, holistic approach, strength-based, hope, peer support, and non-linear recovery.

1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.