NURS12154 Case Study: Medication Error, Ethics, & Legislation
VerifiedAdded on 2023/06/13
|9
|2376
|223
Case Study
AI Summary
This Coronial clinical case study examines the death of Mrs. T, a 74-year-old patient with a history of depression and other health issues, due to a medication error. Nurse B administered Nitrazepam instead of Mirtazapine, leading to a series of adverse events and ultimately, her death. The analysis highlights failures in adhering to National Safety and Quality Health Service (NSQHS) standards, particularly regarding double-checking medication orders. Ethical considerations, including veracity and non-maleficence, were violated by both nurses involved. The study also discusses relevant Australian drug regulations and emphasizes the importance of proper drug administration and adherence to ethical principles to prevent similar fatal errors in geriatric patients. Desklib provides resources like this to help students excel.

Running head: CORONIAL CLINICAL CASE STUDY
Coronial Clinical Case Summary
Name of Student
Name of University
Author Note
Coronial Clinical Case Summary
Name of Student
Name of University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1CORONIAL CLINICAL CASE STUDY
Medication errors are some of the preventable mistakes, which are a resultant of
erroneous administration of pharmaceuticals, which can jeopardize patient safety and even cause
fatality in extreme cases. A report provided by the IOS Press in Amsterdam, showed that nearly
251,000 people lose their lives as result of medication error annually in the United States
(Anderson Abrahamson & Na 2017). The report aims to describe a Coronial clinical
investigative case study of a patient named Mrs. T who expired due to clinical error governed by
the respondent nurse. The critical analysis of the nursing guide is to be described in the following
discussion will emphasize on the medication malpractice, ethical issues and legislative issue that
could arise in such cases.
The patient was under psychiatric review due to major depressive disorder and has a
history of depression, cholesystectomy, ischemic heart diseases and reoccurring urinary tract
infection. The patient was admitted to the hospital with dehydrated condition, which
subsequently deteriorated and was under constant monitoring and required assistance for
changing and other smaller activities. The patient was prepared for a transfer to a psychiatric
hospital. The associate unit manager, here and now referred to as nurse A had instructed the
registered nurse, here and now will be referred to as Nurse B to administer the patients
medications prior to her discharge to avoid re-hospitalization (Hasan et al., 2010). The nurse B
misread the medication chart and administered Nitrazepam or Mogadon 15mg that is an
antidepressant instead of mirtazapine or Avanza 15mg that is a potent sedative.
The National Safety and Quality Health Service (NSQHS) Standard in Australia has a set
of guideline for promotion of safety in health care, whose Standard 4 describes the medication
safety guidelines, “Clinical leaders and senior managers of a health service organisation
implement systems to reduce the occurrence of medication incidents, and improve the safety and
Medication errors are some of the preventable mistakes, which are a resultant of
erroneous administration of pharmaceuticals, which can jeopardize patient safety and even cause
fatality in extreme cases. A report provided by the IOS Press in Amsterdam, showed that nearly
251,000 people lose their lives as result of medication error annually in the United States
(Anderson Abrahamson & Na 2017). The report aims to describe a Coronial clinical
investigative case study of a patient named Mrs. T who expired due to clinical error governed by
the respondent nurse. The critical analysis of the nursing guide is to be described in the following
discussion will emphasize on the medication malpractice, ethical issues and legislative issue that
could arise in such cases.
The patient was under psychiatric review due to major depressive disorder and has a
history of depression, cholesystectomy, ischemic heart diseases and reoccurring urinary tract
infection. The patient was admitted to the hospital with dehydrated condition, which
subsequently deteriorated and was under constant monitoring and required assistance for
changing and other smaller activities. The patient was prepared for a transfer to a psychiatric
hospital. The associate unit manager, here and now referred to as nurse A had instructed the
registered nurse, here and now will be referred to as Nurse B to administer the patients
medications prior to her discharge to avoid re-hospitalization (Hasan et al., 2010). The nurse B
misread the medication chart and administered Nitrazepam or Mogadon 15mg that is an
antidepressant instead of mirtazapine or Avanza 15mg that is a potent sedative.
The National Safety and Quality Health Service (NSQHS) Standard in Australia has a set
of guideline for promotion of safety in health care, whose Standard 4 describes the medication
safety guidelines, “Clinical leaders and senior managers of a health service organisation
implement systems to reduce the occurrence of medication incidents, and improve the safety and
2CORONIAL CLINICAL CASE STUDY
quality of medicine use. Clinicians and other members of the workforce use the systems to safely
manage medicines” (Standard, Q. I. G., 2012). In light of the current case study provided, the
incident could have been avoided by completing independent double-checking by both nurse A
and nurse B, which was not seen in this case. This form of medication error is very common in
the healthcare industry (Jones 2014). The nurse A, showed lack of supervision, as she was
responsible to make sure that the order she provided was properly followed. The nurse B misread
the medication chart, which was a sign of carelessness on her behalf.
Double-checking is a widely accepted standard of clinical practice, which is very useful
to prevent errors in healthcare service (Hewitt, Chreim & Forster, 2016). The nurse B in this case
could have doubled checked the medication chart and stopped herself from administering a
sedative in place of an anti-depressant. The nurse also could have independently double checked
the medication procedure and prevented the medication error. This is a kind of supervision error
in the case for the nurse A, who is the senior authority in this case (Reid‐Searl, Moxham &
Happell, 2010). Since the above suggestions were not followed, it lead to the development of
loss of consciousness, hospital acquired pathogenesis, gastric aspiration and ultimately septic
shock, which gave rise to her death.
There are many ethical considerations to be undertaken in nursing practices, one of them
medication administration principles. It is important to recognize the patient’s problems and then
administer medication with respect to his or her need (Mitty et al., 2010). Assessment and
understanding of the kind of drug being used is also another consideration in the medication
ethics, which helps avoiding drug based adverse reaction. It is important to focus decision based
on the route in which the drug will be administered which is focused based on the patient’s needs
and state of health. Time of medication is another aspect, which needs to be considered when it
quality of medicine use. Clinicians and other members of the workforce use the systems to safely
manage medicines” (Standard, Q. I. G., 2012). In light of the current case study provided, the
incident could have been avoided by completing independent double-checking by both nurse A
and nurse B, which was not seen in this case. This form of medication error is very common in
the healthcare industry (Jones 2014). The nurse A, showed lack of supervision, as she was
responsible to make sure that the order she provided was properly followed. The nurse B misread
the medication chart, which was a sign of carelessness on her behalf.
Double-checking is a widely accepted standard of clinical practice, which is very useful
to prevent errors in healthcare service (Hewitt, Chreim & Forster, 2016). The nurse B in this case
could have doubled checked the medication chart and stopped herself from administering a
sedative in place of an anti-depressant. The nurse also could have independently double checked
the medication procedure and prevented the medication error. This is a kind of supervision error
in the case for the nurse A, who is the senior authority in this case (Reid‐Searl, Moxham &
Happell, 2010). Since the above suggestions were not followed, it lead to the development of
loss of consciousness, hospital acquired pathogenesis, gastric aspiration and ultimately septic
shock, which gave rise to her death.
There are many ethical considerations to be undertaken in nursing practices, one of them
medication administration principles. It is important to recognize the patient’s problems and then
administer medication with respect to his or her need (Mitty et al., 2010). Assessment and
understanding of the kind of drug being used is also another consideration in the medication
ethics, which helps avoiding drug based adverse reaction. It is important to focus decision based
on the route in which the drug will be administered which is focused based on the patient’s needs
and state of health. Time of medication is another aspect, which needs to be considered when it
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3CORONIAL CLINICAL CASE STUDY
comes to administration, and void loss of drug efficacy. It is important to keep record of the drug
administered to allow the next healthcare giver information to carry the duty forward. It is also
considered ethically sound to assess the rationale that is related to the administration of drug
with respect to the patient’s condition to avoid medication error (Richardson, Bromirski &
Hayden, 2012). The patient needs to be monitored to check whether or not the administered drug
is working to improve the patient’s condition or having any indication of adverse effect. In light
of the given case study, it can be observed that both the supervising nurse A and the nurse B
failed to show the necessary ethical principal which lead to the untimely demise of the patient.
The nurse B failed to assess the right drug for the patient, which lead to loss of consciousness.
The medical field is dependent on the flow of proper information to advocate to the
personal caring of the ailing patients. The patients are vulnerable in this form of profession and
their existence is dependent on the responsiveness of the care professionals. Veracity or truth
telling has an important role in this situation. It is unethical to withhold information in this form
of profession, as it can jeopardize the safety of the patient (Wolf 2012). Violation of veracity
can also result in the credibility loss and respect among care givers as well as patients. the case
study also reflects similar actions of violation of veracity as the supervising nurse A did not
mention, protest of complain against the nurse B when she fund that wrong medication had been
administered to the patient.
Non-maleficence is another term used in medical profession describing the act of not
indulging in intentional harm. This form of ethical principle is what the healthcare industry is
built upon. The vulnerability of the patient and the respecting acre plan is the duty of healthcare
givers (Johnstone, 2011). It is obligatory for a nursing caregiver to provide the patient with
beneficence as soon as possible keeping patient safety in mind. In the case of the coronial
comes to administration, and void loss of drug efficacy. It is important to keep record of the drug
administered to allow the next healthcare giver information to carry the duty forward. It is also
considered ethically sound to assess the rationale that is related to the administration of drug
with respect to the patient’s condition to avoid medication error (Richardson, Bromirski &
Hayden, 2012). The patient needs to be monitored to check whether or not the administered drug
is working to improve the patient’s condition or having any indication of adverse effect. In light
of the given case study, it can be observed that both the supervising nurse A and the nurse B
failed to show the necessary ethical principal which lead to the untimely demise of the patient.
The nurse B failed to assess the right drug for the patient, which lead to loss of consciousness.
The medical field is dependent on the flow of proper information to advocate to the
personal caring of the ailing patients. The patients are vulnerable in this form of profession and
their existence is dependent on the responsiveness of the care professionals. Veracity or truth
telling has an important role in this situation. It is unethical to withhold information in this form
of profession, as it can jeopardize the safety of the patient (Wolf 2012). Violation of veracity
can also result in the credibility loss and respect among care givers as well as patients. the case
study also reflects similar actions of violation of veracity as the supervising nurse A did not
mention, protest of complain against the nurse B when she fund that wrong medication had been
administered to the patient.
Non-maleficence is another term used in medical profession describing the act of not
indulging in intentional harm. This form of ethical principle is what the healthcare industry is
built upon. The vulnerability of the patient and the respecting acre plan is the duty of healthcare
givers (Johnstone, 2011). It is obligatory for a nursing caregiver to provide the patient with
beneficence as soon as possible keeping patient safety in mind. In the case of the coronial
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4CORONIAL CLINICAL CASE STUDY
investigation, I observed that both respondent nurses failed to take credibility for the incident and
took part in violation of the ethics of non-maleficence and administered wrong medication, and
did not even provide alternative methods to efflux the mistaken drug from the patient’s system.
This kind of violation of ethical is subjected to legal actions.
There are many laws that govern the usage of drugs and in case of patient; those
guidelines were not kept in mind. It is important to adhere to the legislative regulation of a
particular country while administering drugs, to avoid the repercussions followed by medication
errors (Choo, Hutchinson & Bucknall, 2010). The Australian government has a set of laws and
regulation to be followed in relation to the drug administration, which helps to maintain clinical
governance. The Health and Drugs Regulation Act in 1998 has a set of guidelines for the use,
storage and administration of various pharmaceutical drugs, which defines the standard practices
that need to be undertaken while administering drugs to patients safely (Scheduling basics,
2015). According to the government of Australia, Department of health, the following is the list
of scheduled drugs kept in mind while administering drugs are mentioned in the following
figure:
investigation, I observed that both respondent nurses failed to take credibility for the incident and
took part in violation of the ethics of non-maleficence and administered wrong medication, and
did not even provide alternative methods to efflux the mistaken drug from the patient’s system.
This kind of violation of ethical is subjected to legal actions.
There are many laws that govern the usage of drugs and in case of patient; those
guidelines were not kept in mind. It is important to adhere to the legislative regulation of a
particular country while administering drugs, to avoid the repercussions followed by medication
errors (Choo, Hutchinson & Bucknall, 2010). The Australian government has a set of laws and
regulation to be followed in relation to the drug administration, which helps to maintain clinical
governance. The Health and Drugs Regulation Act in 1998 has a set of guidelines for the use,
storage and administration of various pharmaceutical drugs, which defines the standard practices
that need to be undertaken while administering drugs to patients safely (Scheduling basics,
2015). According to the government of Australia, Department of health, the following is the list
of scheduled drugs kept in mind while administering drugs are mentioned in the following
figure:
5CORONIAL CLINICAL CASE STUDY
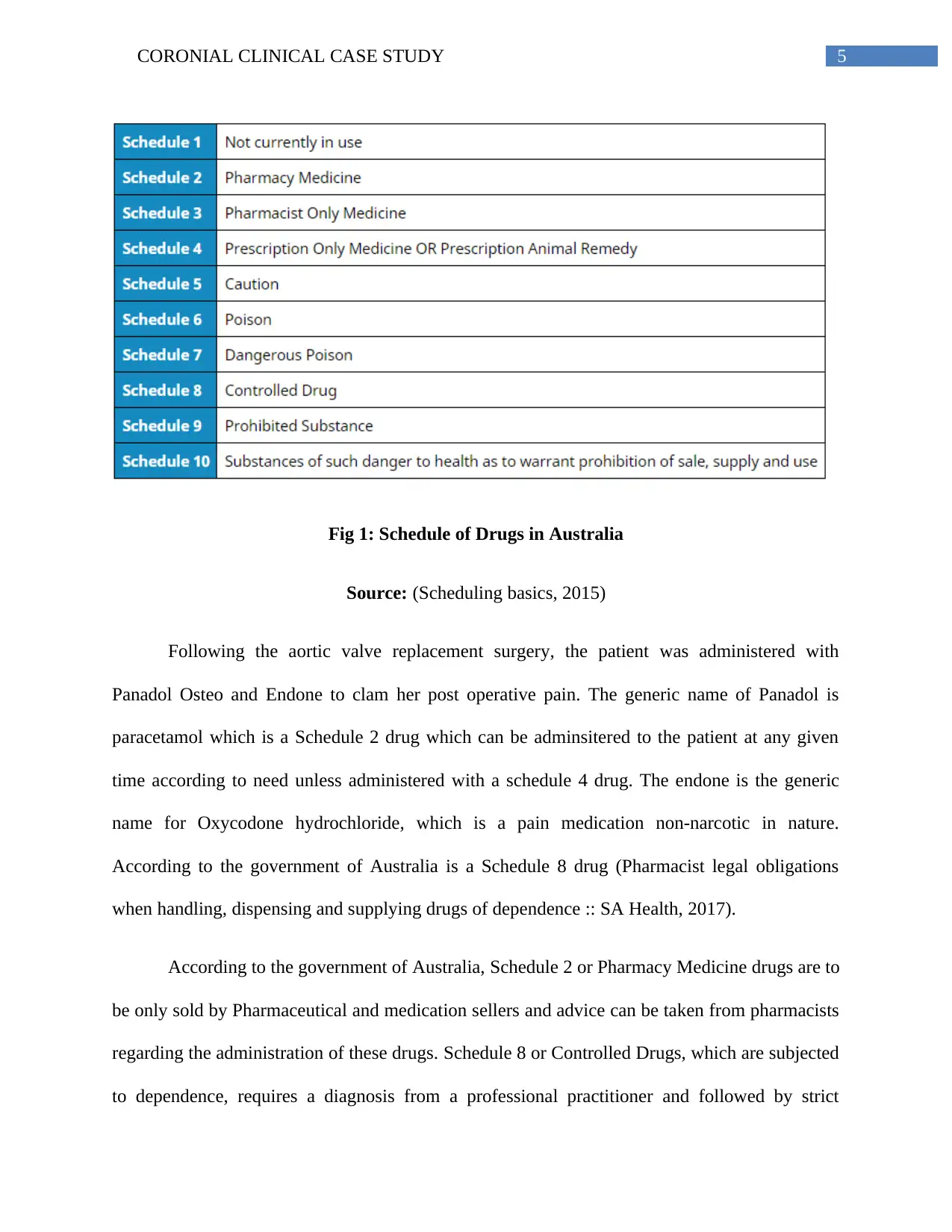
Fig 1: Schedule of Drugs in Australia
Source: (Scheduling basics, 2015)
Following the aortic valve replacement surgery, the patient was administered with
Panadol Osteo and Endone to clam her post operative pain. The generic name of Panadol is
paracetamol which is a Schedule 2 drug which can be adminsitered to the patient at any given
time according to need unless administered with a schedule 4 drug. The endone is the generic
name for Oxycodone hydrochloride, which is a pain medication non-narcotic in nature.
According to the government of Australia is a Schedule 8 drug (Pharmacist legal obligations
when handling, dispensing and supplying drugs of dependence :: SA Health, 2017).
According to the government of Australia, Schedule 2 or Pharmacy Medicine drugs are to
be only sold by Pharmaceutical and medication sellers and advice can be taken from pharmacists
regarding the administration of these drugs. Schedule 8 or Controlled Drugs, which are subjected
to dependence, requires a diagnosis from a professional practitioner and followed by strict
Fig 1: Schedule of Drugs in Australia
Source: (Scheduling basics, 2015)
Following the aortic valve replacement surgery, the patient was administered with
Panadol Osteo and Endone to clam her post operative pain. The generic name of Panadol is
paracetamol which is a Schedule 2 drug which can be adminsitered to the patient at any given
time according to need unless administered with a schedule 4 drug. The endone is the generic
name for Oxycodone hydrochloride, which is a pain medication non-narcotic in nature.
According to the government of Australia is a Schedule 8 drug (Pharmacist legal obligations
when handling, dispensing and supplying drugs of dependence :: SA Health, 2017).
According to the government of Australia, Schedule 2 or Pharmacy Medicine drugs are to
be only sold by Pharmaceutical and medication sellers and advice can be taken from pharmacists
regarding the administration of these drugs. Schedule 8 or Controlled Drugs, which are subjected
to dependence, requires a diagnosis from a professional practitioner and followed by strict
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6CORONIAL CLINICAL CASE STUDY
monitoring of the patient it is being administered to very carefully. The drugs can be supplied
only after reference from a medical practitioner and can only be dispensed by a pharmacist after
showing prescription (Pharmacist legal obligations when handling, dispensing and supplying
drugs of dependence :: SA Health, 2017). It is the responsibility of the nurse to identify the need
of the patient and then assess the type of scheduled drug being administered to the patient. In
case of coronial case study, the nursing supervisor as well as the registered nurse both refused to
adhere to the regulations of the nursing workforce and provide evidence for drug management
(Masters, 2015). The nurses in charge should have recognised the difference between the two
drugs, one was clearly an over the counter pharmaceutical and the other was a schedule 8
prescription analgesic. The nurse instead provided a strong sedative, which completely rendered
her unconscious.
The above description of the case of Mrs. T and the coronial investigative results made it
clear that the nursing staffs assigned to the patient clearly violated the act of veracity and non-
malefiscence, which lead to the untimely demise of the elderly patient who was already suffering
from mental illness. The nursing supervisor failed to show any responsibility towards
independent checking of her order, the type of drug being administered as well as failed to
truthfully adhere to the ethical principle. In conclusion, it can be said that for future nursing this
can be a lesson to ensure that the correct drug is being administered to the patient to avoid fatal
repercussion in geriatric patients.
monitoring of the patient it is being administered to very carefully. The drugs can be supplied
only after reference from a medical practitioner and can only be dispensed by a pharmacist after
showing prescription (Pharmacist legal obligations when handling, dispensing and supplying
drugs of dependence :: SA Health, 2017). It is the responsibility of the nurse to identify the need
of the patient and then assess the type of scheduled drug being administered to the patient. In
case of coronial case study, the nursing supervisor as well as the registered nurse both refused to
adhere to the regulations of the nursing workforce and provide evidence for drug management
(Masters, 2015). The nurses in charge should have recognised the difference between the two
drugs, one was clearly an over the counter pharmaceutical and the other was a schedule 8
prescription analgesic. The nurse instead provided a strong sedative, which completely rendered
her unconscious.
The above description of the case of Mrs. T and the coronial investigative results made it
clear that the nursing staffs assigned to the patient clearly violated the act of veracity and non-
malefiscence, which lead to the untimely demise of the elderly patient who was already suffering
from mental illness. The nursing supervisor failed to show any responsibility towards
independent checking of her order, the type of drug being administered as well as failed to
truthfully adhere to the ethical principle. In conclusion, it can be said that for future nursing this
can be a lesson to ensure that the correct drug is being administered to the patient to avoid fatal
repercussion in geriatric patients.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7CORONIAL CLINICAL CASE STUDY
References:
Anderson, J. G., Abrahamson, K., & Na, R. (2017). Your Health Care May Kill You: Medical
Errors. In ITCH (pp. 13-17).
Choo, J., Hutchinson, A., & Bucknall, T. (2010). Nurses' role in medication safety. Journal of
nursing management, 18(7), 853-861.
Hasan, O., Meltzer, D. O., Shaykevich, S. A., Bell, C. M., Kaboli, P. J., Auerbach, A. D., ... &
Schnipper, J. L. (2010). Hospital readmission in general medicine patients: a prediction
model. Journal of general internal medicine, 25(3), 211-219.
Hewitt, T., Chreim, S., & Forster, A. (2016). Double checking: a second look. Journal of
evaluation in clinical practice, 22(2), 267-274.
Johnstone, M. J. (2011). Nursing ethics and informed consent. Australian Nursing and Midwifery
Journal, 19(5), 29.
Jones, J. (2014). Misread labels as a cause of medication errors. AJN The American Journal of
Nursing, 114(3), 11.
Masters, K. (2015). Role development in professional nursing practice. Jones & Bartlett
Publishers.
Mitty, E., Resnick, B., Allen, J., Bakerjian, D., Hertz, J., Gardner, W., ... & Mezey, M. (2010).
Nursing delegation and medication administration in assisted living. Nursing
Administration Quarterly, 34(2), 162-171.
References:
Anderson, J. G., Abrahamson, K., & Na, R. (2017). Your Health Care May Kill You: Medical
Errors. In ITCH (pp. 13-17).
Choo, J., Hutchinson, A., & Bucknall, T. (2010). Nurses' role in medication safety. Journal of
nursing management, 18(7), 853-861.
Hasan, O., Meltzer, D. O., Shaykevich, S. A., Bell, C. M., Kaboli, P. J., Auerbach, A. D., ... &
Schnipper, J. L. (2010). Hospital readmission in general medicine patients: a prediction
model. Journal of general internal medicine, 25(3), 211-219.
Hewitt, T., Chreim, S., & Forster, A. (2016). Double checking: a second look. Journal of
evaluation in clinical practice, 22(2), 267-274.
Johnstone, M. J. (2011). Nursing ethics and informed consent. Australian Nursing and Midwifery
Journal, 19(5), 29.
Jones, J. (2014). Misread labels as a cause of medication errors. AJN The American Journal of
Nursing, 114(3), 11.
Masters, K. (2015). Role development in professional nursing practice. Jones & Bartlett
Publishers.
Mitty, E., Resnick, B., Allen, J., Bakerjian, D., Hertz, J., Gardner, W., ... & Mezey, M. (2010).
Nursing delegation and medication administration in assisted living. Nursing
Administration Quarterly, 34(2), 162-171.
8CORONIAL CLINICAL CASE STUDY
Pharmacist legal obligations when handling, dispensing and supplying drugs of dependence ::
SA Health. (2017). Sahealth.sa.gov.au. Retrieved 9 April 2018, from
http://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/
clinical+resources/clinical+topics/medicines+and+drugs/legal+control+over+medicines/
legal+requirements+for+the+prescription+and+supply+of+drugs+of+dependence/
pharmacist+legal+obligations+when+handling+dispensing+and+supplying+drugs+of+de
pendence
Reid‐Searl, K., Moxham, L., & Happell, B. (2010). Enhancing patient safety: the importance of
direct supervision for avoiding medication errors and near misses by undergraduate
nursing students. International Journal of Nursing Practice, 16(3), 225-232.
Richardson, B., Bromirski, B., & Hayden, A. (2012). Implementing a safe and reliable process
for medication administration. Clinical Nurse Specialist, 26(3), 169-176.
Scheduling basics. (2015). Therapeutic Goods Administration (TGA). Retrieved 9 April 2018,
from https://www.tga.gov.au/scheduling-basics
Standard, Q. I. G. (2012). Australian Commission on Safety and Quality in Health Care.
Wolf, Z. R. (2012). Nursing practice breakdowns: good and bad nursing. Medsurg
Nursing, 21(1), 16.
Pharmacist legal obligations when handling, dispensing and supplying drugs of dependence ::
SA Health. (2017). Sahealth.sa.gov.au. Retrieved 9 April 2018, from
http://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/
clinical+resources/clinical+topics/medicines+and+drugs/legal+control+over+medicines/
legal+requirements+for+the+prescription+and+supply+of+drugs+of+dependence/
pharmacist+legal+obligations+when+handling+dispensing+and+supplying+drugs+of+de
pendence
Reid‐Searl, K., Moxham, L., & Happell, B. (2010). Enhancing patient safety: the importance of
direct supervision for avoiding medication errors and near misses by undergraduate
nursing students. International Journal of Nursing Practice, 16(3), 225-232.
Richardson, B., Bromirski, B., & Hayden, A. (2012). Implementing a safe and reliable process
for medication administration. Clinical Nurse Specialist, 26(3), 169-176.
Scheduling basics. (2015). Therapeutic Goods Administration (TGA). Retrieved 9 April 2018,
from https://www.tga.gov.au/scheduling-basics
Standard, Q. I. G. (2012). Australian Commission on Safety and Quality in Health Care.
Wolf, Z. R. (2012). Nursing practice breakdowns: good and bad nursing. Medsurg
Nursing, 21(1), 16.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.