NURS2006 Project: Chlorhexidine for VAP Prevention in ICU Settings
VerifiedAdded on 2023/06/16
|11
|4123
|120
Report
AI Summary
This report outlines a clinical practice improvement (CPI) project focused on preventing ventilator-associated pneumonia (VAP) in intensive care units (ICUs) through chlorhexidine gluconate (CHX) oral care. The project aims to reduce VAP rates by 50% within five months by implementing a consistent CHX oral care protocol. The report highlights the relevance of clinical governance, particularly risk management, in reducing healthcare-associated infections (HAIs). It emphasizes the significance of addressing VAP due to its high mortality rate, increased hospital stays, and associated costs. The key stakeholders include the board of directors, project coordinator, nurses, and caregivers. The Plan-Do-Study-Act (PDSA) tool is utilized for the CPI, involving literature review, implementation of CHX oral care, monitoring of VAP reduction rates, and adjustments based on the outcomes. The intervention includes training nurses on proper CHX oral care procedures, performing oral care sessions six times a day, and documenting progress. Potential barriers to implementation, such as nurses' adherence and workload, are addressed through education, goal setting, and feedback mechanisms to ensure the project's sustainability and success.
NURS2006 ASSIGNMENT 3
Clinical Practice Improvement Project Report
Student Name, FAN and ID:
Type your assignment into the white spaces in the template and the rows will
expand as much as you need them to.ie Alex Smith smit0000 ID 1234567
Project Title:
Prevention of ventilator associated pneumonia (VAP) in Mobury intensive care units (ICUs)
through chlorhexidine gluconate (CHX) oral care
Project Aim:
The aim of the project is to reduce the VAP in Mobury ICUs by 50% in 5 months through
prevention by chlorhexidine gluconate oral care
VAP is a common hospital acquired infection (HAI) that occurs when bacteria is being aspirated
into the lungs after 48 hours of intubation (Hunter 2012). VAP is one of the HAI that is leading
cause of death in ICUs and its prevention is important for improved outcomes in its reduction. This
condition of VAP occurs due to little are provided to the patients in ICU under assisted ventilation
and gradually, progress to lungs and bacteria accumulation within oral region that matures to
VAP. This infection is often fatal; however, it can be managed. Prevention can largely address VAP
condition to occur through proper oral care and hygiene. CHX has been used for the prevention of
colonization of bacteria from travelling into lungs leading to VAP (Charles et al. 2014).
Relevance of Clinical Governance to your project
Clinical Governance is a defined system that work through National Health Service (NHS)
organizations who are accountable for continuously improving the quality of healthcare services
and safeguarding the high standards of care through creation of an environment in which clinical
care can excel and flourish (Specchia et al. 2015). Seven pillars or areas of activity are present in
clinical governance ensuring that high quality healthcare services are provided to service users.
This includes service user, public involvement and carer, clinical audit, risk management, staffing
management, education and training, clinical effectiveness and information. Among all these, the
most relevant pillar for the project is the risk management. The nurses need to implement the
approach of CHX oral care to reduce the risk of HAI and prevent VAP that is associated with it. This
clinical governance pillar defines the reduction and prevention of VAP that can be linked to this
Clinical Practice Improvement Project Report
Student Name, FAN and ID:
Type your assignment into the white spaces in the template and the rows will
expand as much as you need them to.ie Alex Smith smit0000 ID 1234567
Project Title:
Prevention of ventilator associated pneumonia (VAP) in Mobury intensive care units (ICUs)
through chlorhexidine gluconate (CHX) oral care
Project Aim:
The aim of the project is to reduce the VAP in Mobury ICUs by 50% in 5 months through
prevention by chlorhexidine gluconate oral care
VAP is a common hospital acquired infection (HAI) that occurs when bacteria is being aspirated
into the lungs after 48 hours of intubation (Hunter 2012). VAP is one of the HAI that is leading
cause of death in ICUs and its prevention is important for improved outcomes in its reduction. This
condition of VAP occurs due to little are provided to the patients in ICU under assisted ventilation
and gradually, progress to lungs and bacteria accumulation within oral region that matures to
VAP. This infection is often fatal; however, it can be managed. Prevention can largely address VAP
condition to occur through proper oral care and hygiene. CHX has been used for the prevention of
colonization of bacteria from travelling into lungs leading to VAP (Charles et al. 2014).
Relevance of Clinical Governance to your project
Clinical Governance is a defined system that work through National Health Service (NHS)
organizations who are accountable for continuously improving the quality of healthcare services
and safeguarding the high standards of care through creation of an environment in which clinical
care can excel and flourish (Specchia et al. 2015). Seven pillars or areas of activity are present in
clinical governance ensuring that high quality healthcare services are provided to service users.
This includes service user, public involvement and carer, clinical audit, risk management, staffing
management, education and training, clinical effectiveness and information. Among all these, the
most relevant pillar for the project is the risk management. The nurses need to implement the
approach of CHX oral care to reduce the risk of HAI and prevent VAP that is associated with it. This
clinical governance pillar defines the reduction and prevention of VAP that can be linked to this
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
project, as nurses need to perform hygiene and oral care in ventilator-assisted patients in ICU and
provide evidence based intervention strategies to prevent VAP (Davoodi et al. 2014). CHX bathing
will enable to prevent bacteria to colonize and enter lungs in ventilator assisted ICU patients and
in turn reduce the incident of VAP in this particular setting.
Evidence that the issue / problem is worth solving:
The second most common nosocomial infection is pneumonia in critically ill patients that affects
27% of them or 86% pneumonias associated with mechanical ventilation termed VAP (Bassi et al.
2014). It accounts for 60% of deaths from HAIs having mortality rate of 33% and greatly increases
the patient time in ICU by 3 to 6 days (Barbier et al. 2013). VAP is s global issue estimating to
generate increased costs and pose burden on the healthcare system on a whole. The hospital days
are increased with an average of 12 days due to this hospital acquired lower respiratory tract
infection and pose additional costs per patient. National Infection Surveillance System (NNIS) by
Centres for Disease Control and Prevention (CDC) reported that patients who receive continuous
mechanical ventilation have highest risk of developing VAP as compared to patients who were not
receiving mechanical ventilation (Bouadma, Wolff and Lucet 2012).
The quality of care delivered to ICU patients is pertinent in the health outcomes or in
acquiring infections. Criticaally ill patients who are intubated in ICUs through endotracheal route
are temporarily or permanently ventilated if prevention measures are not adopted stringently.
Elliott et al. (2015) stated that a study conducted across 14 ICUs in Australia revealed that VAP
rates were 28% and therefore, prevention strategies are important to be implemented. VAP is a
serious risk influenced by immune function, severity of illness, duration of invasive ventilation or
physiological reserves. VAP incidence is a serious challenge for healthcare settings increasing the
duration of hospital stays, higher costs of treatment and high mortality rates. This depicts that
reduction and prevention of VAP need implementation of strategies and tested interventions that
improve patient safety and reduction of untoward outcomes. In ICUs, oral care importance is well
documented for VAP prevention for ensuring patient safety and better health outcomes. CHX is a
prescribed solution for oral care that is licensed, administered in critical healthcare settings along
with routine hygiene practices for the prevention of VAP among critically ill patients in ICUs. CHX is
a broad-spectrum anti-bacterial solution, it kills plaque and prevent bacterial colonization in lungs
that migrate from mouth during aspiration that a ventilated patient is risked for (Özçaka et al.
2012).
Key Stakeholders:
The key stakeholders for this project could be board of directors, project coordinator, nurses or
provide evidence based intervention strategies to prevent VAP (Davoodi et al. 2014). CHX bathing
will enable to prevent bacteria to colonize and enter lungs in ventilator assisted ICU patients and
in turn reduce the incident of VAP in this particular setting.
Evidence that the issue / problem is worth solving:
The second most common nosocomial infection is pneumonia in critically ill patients that affects
27% of them or 86% pneumonias associated with mechanical ventilation termed VAP (Bassi et al.
2014). It accounts for 60% of deaths from HAIs having mortality rate of 33% and greatly increases
the patient time in ICU by 3 to 6 days (Barbier et al. 2013). VAP is s global issue estimating to
generate increased costs and pose burden on the healthcare system on a whole. The hospital days
are increased with an average of 12 days due to this hospital acquired lower respiratory tract
infection and pose additional costs per patient. National Infection Surveillance System (NNIS) by
Centres for Disease Control and Prevention (CDC) reported that patients who receive continuous
mechanical ventilation have highest risk of developing VAP as compared to patients who were not
receiving mechanical ventilation (Bouadma, Wolff and Lucet 2012).
The quality of care delivered to ICU patients is pertinent in the health outcomes or in
acquiring infections. Criticaally ill patients who are intubated in ICUs through endotracheal route
are temporarily or permanently ventilated if prevention measures are not adopted stringently.
Elliott et al. (2015) stated that a study conducted across 14 ICUs in Australia revealed that VAP
rates were 28% and therefore, prevention strategies are important to be implemented. VAP is a
serious risk influenced by immune function, severity of illness, duration of invasive ventilation or
physiological reserves. VAP incidence is a serious challenge for healthcare settings increasing the
duration of hospital stays, higher costs of treatment and high mortality rates. This depicts that
reduction and prevention of VAP need implementation of strategies and tested interventions that
improve patient safety and reduction of untoward outcomes. In ICUs, oral care importance is well
documented for VAP prevention for ensuring patient safety and better health outcomes. CHX is a
prescribed solution for oral care that is licensed, administered in critical healthcare settings along
with routine hygiene practices for the prevention of VAP among critically ill patients in ICUs. CHX is
a broad-spectrum anti-bacterial solution, it kills plaque and prevent bacterial colonization in lungs
that migrate from mouth during aspiration that a ventilated patient is risked for (Özçaka et al.
2012).
Key Stakeholders:
The key stakeholders for this project could be board of directors, project coordinator, nurses or
caregivers.
Board of Directors: The recognized group who would jointly oversee the project and provide
permission for implementing the intervention
Project coordinator: Plan and coordinate the CHX oral care program and ensure the successful
implementation of the intervention along with budget maintenance.
Nurses: They will perform the CHX oral care among the critically ill patients in ICUs under
mechanical ventilation and document reduction rates
Caregivers: Assist in the implementation of the project by looking for risk, supporting and helping
nurses when required
CPI Tool:
A study conducted by Shi et al. (2013) illustrated that quality improvement plan through CHX oral
care can reduce the incidence and prevent VAP along with oral care and deep oral suctioning at
least twice a day. Therefore, Plan-Do-Study-Act (PDSA) tool will be used for the clinical practice
improvement in the ICU setting.
Plan: Literature review of evidence-based practice regarding CHX oral care targets the bacterial
colonisation in the lungs that can cause VAP in intubated patients. The statistics will be gathered
regarding the VAP infections in ICUs among mechanical ventilated patients, as it is the baseline
information required before the implementation of CHX oral care.
We are going to implement a consistent 4 months CHX oral care targeting pneumonia
bacteria and prevent VAP infections in ICU setting among critically ill patients.
We are hopeful that implementation of this intervention can prevent VAP conditions by
around 50% at the end of four months
Steps for execution
Nurses need to understand the benefits of this intervention and related information that
reduce the incidence of VAP and its prevention in ICUs. Nurses should be educated about
the correct CHX oral care procedure through a handbook that gives description of the
steps in text and pictures involved in the oral care using CHX solution.
The nurses and caregivers should be encouraged by the project coordinator assisted by
nurse leader to be engaged in the oral care at appropriate intervals. It is advised to
perform oral care sessions 6 times a day where two out of six oral care sessions should
Board of Directors: The recognized group who would jointly oversee the project and provide
permission for implementing the intervention
Project coordinator: Plan and coordinate the CHX oral care program and ensure the successful
implementation of the intervention along with budget maintenance.
Nurses: They will perform the CHX oral care among the critically ill patients in ICUs under
mechanical ventilation and document reduction rates
Caregivers: Assist in the implementation of the project by looking for risk, supporting and helping
nurses when required
CPI Tool:
A study conducted by Shi et al. (2013) illustrated that quality improvement plan through CHX oral
care can reduce the incidence and prevent VAP along with oral care and deep oral suctioning at
least twice a day. Therefore, Plan-Do-Study-Act (PDSA) tool will be used for the clinical practice
improvement in the ICU setting.
Plan: Literature review of evidence-based practice regarding CHX oral care targets the bacterial
colonisation in the lungs that can cause VAP in intubated patients. The statistics will be gathered
regarding the VAP infections in ICUs among mechanical ventilated patients, as it is the baseline
information required before the implementation of CHX oral care.
We are going to implement a consistent 4 months CHX oral care targeting pneumonia
bacteria and prevent VAP infections in ICU setting among critically ill patients.
We are hopeful that implementation of this intervention can prevent VAP conditions by
around 50% at the end of four months
Steps for execution
Nurses need to understand the benefits of this intervention and related information that
reduce the incidence of VAP and its prevention in ICUs. Nurses should be educated about
the correct CHX oral care procedure through a handbook that gives description of the
steps in text and pictures involved in the oral care using CHX solution.
The nurses and caregivers should be encouraged by the project coordinator assisted by
nurse leader to be engaged in the oral care at appropriate intervals. It is advised to
perform oral care sessions 6 times a day where two out of six oral care sessions should
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
include CHX performed every 12 hours.
Application of training session for nurses for one week to meet the expectations of the
project and coordinator work to make adjustments for the successful implementation of
the proposed intervention
Do: In this step, the plan will be executed where the ICU oral care through CHX will be preformed.
The performing of subglottic suctioning, ensuring proper ETT cuff inflation and proper brushing
time for more than two minutes are steps involved in oral hygiene care. Brushes should be used if
required to remove soft debris and visible plaque by using soft brush that makes small circular
movements and clean gums, tongue and palate (Alhazzani et al. 2013).
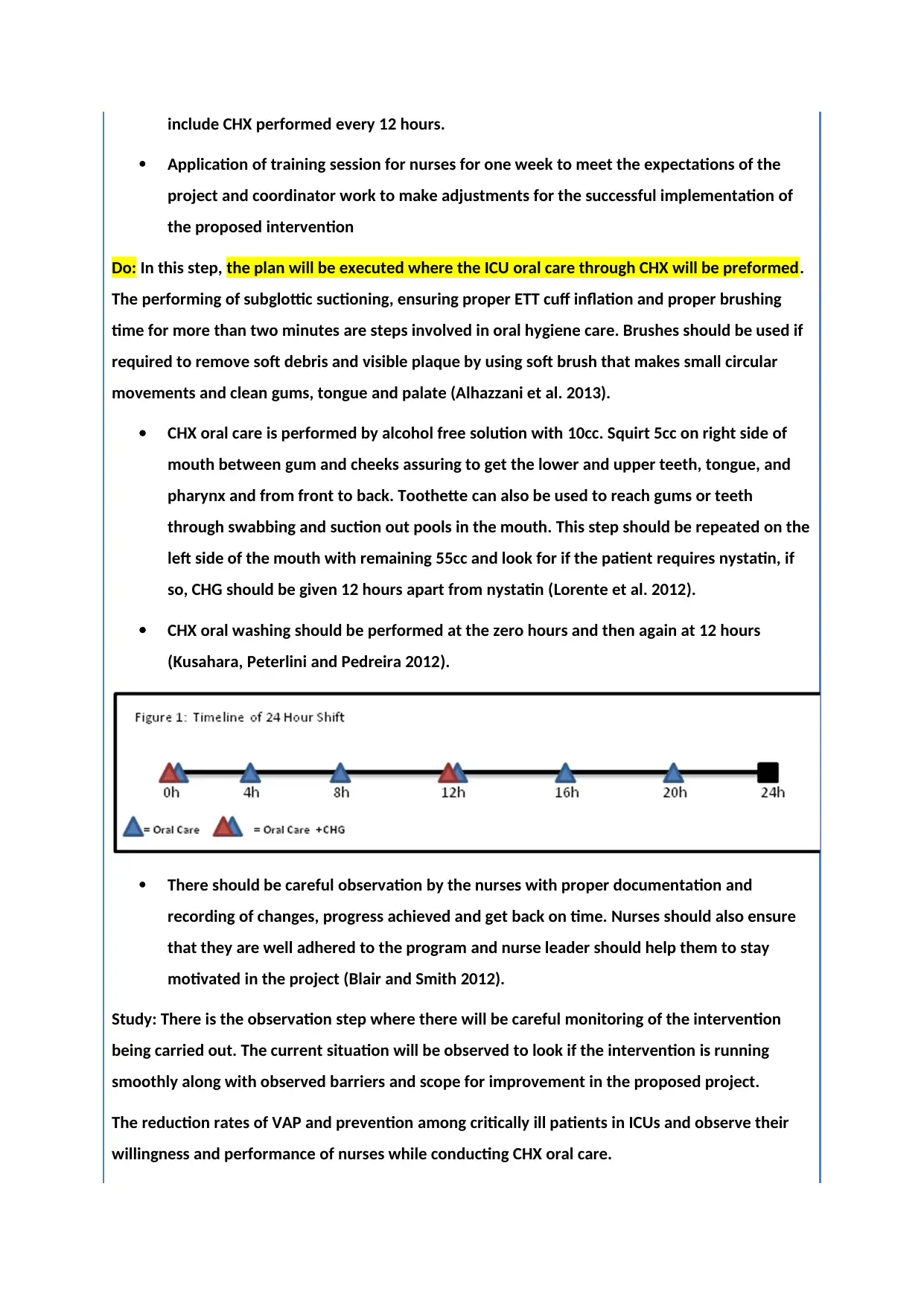
CHX oral care is performed by alcohol free solution with 10cc. Squirt 5cc on right side of
mouth between gum and cheeks assuring to get the lower and upper teeth, tongue, and
pharynx and from front to back. Toothette can also be used to reach gums or teeth
through swabbing and suction out pools in the mouth. This step should be repeated on the
left side of the mouth with remaining 55cc and look for if the patient requires nystatin, if
so, CHG should be given 12 hours apart from nystatin (Lorente et al. 2012).
CHX oral washing should be performed at the zero hours and then again at 12 hours
(Kusahara, Peterlini and Pedreira 2012).
There should be careful observation by the nurses with proper documentation and
recording of changes, progress achieved and get back on time. Nurses should also ensure
that they are well adhered to the program and nurse leader should help them to stay
motivated in the project (Blair and Smith 2012).
Study: There is the observation step where there will be careful monitoring of the intervention
being carried out. The current situation will be observed to look if the intervention is running
smoothly along with observed barriers and scope for improvement in the proposed project.
The reduction rates of VAP and prevention among critically ill patients in ICUs and observe their
willingness and performance of nurses while conducting CHX oral care.
Application of training session for nurses for one week to meet the expectations of the
project and coordinator work to make adjustments for the successful implementation of
the proposed intervention
Do: In this step, the plan will be executed where the ICU oral care through CHX will be preformed.
The performing of subglottic suctioning, ensuring proper ETT cuff inflation and proper brushing
time for more than two minutes are steps involved in oral hygiene care. Brushes should be used if
required to remove soft debris and visible plaque by using soft brush that makes small circular
movements and clean gums, tongue and palate (Alhazzani et al. 2013).
CHX oral care is performed by alcohol free solution with 10cc. Squirt 5cc on right side of
mouth between gum and cheeks assuring to get the lower and upper teeth, tongue, and
pharynx and from front to back. Toothette can also be used to reach gums or teeth
through swabbing and suction out pools in the mouth. This step should be repeated on the
left side of the mouth with remaining 55cc and look for if the patient requires nystatin, if
so, CHG should be given 12 hours apart from nystatin (Lorente et al. 2012).
CHX oral washing should be performed at the zero hours and then again at 12 hours
(Kusahara, Peterlini and Pedreira 2012).
There should be careful observation by the nurses with proper documentation and
recording of changes, progress achieved and get back on time. Nurses should also ensure
that they are well adhered to the program and nurse leader should help them to stay
motivated in the project (Blair and Smith 2012).
Study: There is the observation step where there will be careful monitoring of the intervention
being carried out. The current situation will be observed to look if the intervention is running
smoothly along with observed barriers and scope for improvement in the proposed project.
The reduction rates of VAP and prevention among critically ill patients in ICUs and observe their
willingness and performance of nurses while conducting CHX oral care.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Act: The willingness and adherence of nurses to perform CHX oral care and look for changes
required if the program did not live up to the expectation of reducing 50% of VAP cases in ICUs.
Moreover, as patients are already in co-morbid conditions, the outcome of the interventions were
not favourable and as expected.
Requirement of more rigorous training and education provided to nurses to create awareness and
make them capable of performing CHX oral care in critically ill patients.
Summary of proposed interventions:
The patients who are under the assisted ventilation in ICUs suffer from VAP where the bacteria
colonize in the lungs after aspiration from mouth and become a major cause of mortality among
the critically ill patients. This also increases the length of hospital stays by 3 to 6 days with higher
treatment costs and poses challenges to the healthcare system as a whole (Cutler and Sluman
2014).
The first phase of the plan will be designing of the CPI project, finances, budgeting and necessary
equipments list required for the project to be presented to the Board of Directors and finance
department of the hospital.
Training will be organized for the nurses of the ICU ward under the supervision of nurse leader for
performing CHX oral care in critically ill patients. CHX oral care has shown to prevent VAP
associated conditions in patients who are under mechanical ventilation temporarily or
permanently. Training will help to educate nurses about the importance of CHX oral care for VAP
prevention and reduction of associated risk.
This program will be carried out for 4 months under the supervision of nurse leader and project
coordinator. The CHX oral washing will be performed with two sessions every 12 hours out of six
oral care sessions. The improvements made in the reduction and prevention of the infection by
this intervention will be supervised along with careful monitoring to see the adherence and
performance of nurses in the program. The nurses should be motivated to work and monitor their
performance through proper documentation and frequent rounds to the ICUs. Feedback should
also be obtained from the supervisors to know the effectiveness of the program.
Barriers to implementation and sustaining change:
Various barriers to implementation of the program may be observed that require documentation
and plan to sustain change.
Nurses’ adherence to the program can influence the successful implementation of CHX oral care in
ICU setting. Nurses’ unwillingness to perform the oral care as it may pose extra workload on them
required if the program did not live up to the expectation of reducing 50% of VAP cases in ICUs.
Moreover, as patients are already in co-morbid conditions, the outcome of the interventions were
not favourable and as expected.
Requirement of more rigorous training and education provided to nurses to create awareness and
make them capable of performing CHX oral care in critically ill patients.
Summary of proposed interventions:
The patients who are under the assisted ventilation in ICUs suffer from VAP where the bacteria
colonize in the lungs after aspiration from mouth and become a major cause of mortality among
the critically ill patients. This also increases the length of hospital stays by 3 to 6 days with higher
treatment costs and poses challenges to the healthcare system as a whole (Cutler and Sluman
2014).
The first phase of the plan will be designing of the CPI project, finances, budgeting and necessary
equipments list required for the project to be presented to the Board of Directors and finance
department of the hospital.
Training will be organized for the nurses of the ICU ward under the supervision of nurse leader for
performing CHX oral care in critically ill patients. CHX oral care has shown to prevent VAP
associated conditions in patients who are under mechanical ventilation temporarily or
permanently. Training will help to educate nurses about the importance of CHX oral care for VAP
prevention and reduction of associated risk.
This program will be carried out for 4 months under the supervision of nurse leader and project
coordinator. The CHX oral washing will be performed with two sessions every 12 hours out of six
oral care sessions. The improvements made in the reduction and prevention of the infection by
this intervention will be supervised along with careful monitoring to see the adherence and
performance of nurses in the program. The nurses should be motivated to work and monitor their
performance through proper documentation and frequent rounds to the ICUs. Feedback should
also be obtained from the supervisors to know the effectiveness of the program.
Barriers to implementation and sustaining change:
Various barriers to implementation of the program may be observed that require documentation
and plan to sustain change.
Nurses’ adherence to the program can influence the successful implementation of CHX oral care in
ICU setting. Nurses’ unwillingness to perform the oral care as it may pose extra workload on them
and distracted from performing it as advised.
Nurses need to be properly educated about the importance of CHX oral washing in VAP prevention
and risk reduction
Plan specific goals every week for the nurses to keep them motivated and study their level of
commitment in executing the intervention.
Get feedback and find out perceived barriers to CHX oral care and addressing it through weekly
goals. There might also be inaccurate documentation by nurses that can lead to unsatisfied
outcome and lack of necessary knowledge and skills that is required to perform CHX oral care.
Cost consideration regarding acquiring of necessary facilities and resources also act as potential
barriers to implementation of CHX oral care in ICU among critically ill patients.
Evaluation of the project:
Evaluation strategies can be used for determining the success of the project.
Before and after evaluation is important where the proper knowledge and documentation by the
nurses before and after the program will be evaluated.
The rates of VAP before and after the implementation of the project will be statistically
represented in the form of spreadsheets or bar graphs helpful for the evaluation of program
success.
The success of the project can be evaluated by receiving feedback from supervisors and comparing
the infection rates before and after the completion of program.
Proper documentation and obtained feedback can be helpful in evaluating the knowledge level,
motivation and perceptions of nurses at the initial stages and after the completion of the project.
Clinical auditing at regular intervals can also be helpful in the evaluation of the project.
References
Nurses need to be properly educated about the importance of CHX oral washing in VAP prevention
and risk reduction
Plan specific goals every week for the nurses to keep them motivated and study their level of
commitment in executing the intervention.
Get feedback and find out perceived barriers to CHX oral care and addressing it through weekly
goals. There might also be inaccurate documentation by nurses that can lead to unsatisfied
outcome and lack of necessary knowledge and skills that is required to perform CHX oral care.
Cost consideration regarding acquiring of necessary facilities and resources also act as potential
barriers to implementation of CHX oral care in ICU among critically ill patients.
Evaluation of the project:
Evaluation strategies can be used for determining the success of the project.
Before and after evaluation is important where the proper knowledge and documentation by the
nurses before and after the program will be evaluated.
The rates of VAP before and after the implementation of the project will be statistically
represented in the form of spreadsheets or bar graphs helpful for the evaluation of program
success.
The success of the project can be evaluated by receiving feedback from supervisors and comparing
the infection rates before and after the completion of program.
Proper documentation and obtained feedback can be helpful in evaluating the knowledge level,
motivation and perceptions of nurses at the initial stages and after the completion of the project.
Clinical auditing at regular intervals can also be helpful in the evaluation of the project.
References
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Alhazzani, W., Smith, O., Muscedere, J., Medd, J. and Cook, D., 2013. Toothbrushing for critically ill
mechanically ventilated patients: a systematic review and meta-analysis of randomized trials
evaluating ventilator-associated pneumonia. Critical care medicine, 41(2), pp.646-655.
Barbier, F., Andremont, A., Wolff, M. and Bouadma, L., 2013. Hospital-acquired pneumonia and
ventilator-associated pneumonia: recent advances in epidemiology and management. Current
opinion in pulmonary medicine, 19(3), pp.216-228.
Bassi, G.L., Ferrer, M., Marti, J.D., Comaru, T. and Torres, A., 2014, August. Ventilator-associated
pneumonia. In Seminars in respiratory and critical care medicine (Vol. 35, No. 04, pp. 469-481).
Thieme Medical Publishers.
Blair, W. and Smith, B., 2012. Nursing documentation: frameworks and barriers. Contemporary
nurse, 41(2), pp.160-168.
Bouadma, L., Wolff, M. and Lucet, J.C., 2012. Ventilator-associated pneumonia and its
prevention. Current opinion in infectious diseases, 25(4), pp.395-404.
Charles, M.P., Kali, A., Easow, J.M., Joseph, N.M., Ravishankar, M., Srinivasan, S., Kumar, S. and
Umadevi, S., 2014. Ventilator-associated pneumonia. The Australasian medical journal, 7(8), p.334.
Cutler, L.R. and Sluman, P., 2014. Reducing ventilator associated pneumonia in adult patients
through high standards of oral care: A historical control study. Intensive and Critical Care
Nursing, 30(2), pp.61-68.
Davoodi, R., Soltanifar, A., Sh, R., Sabouri, G., Asadi, M., Takbiri, A. and Koleini, F., 2014. Clinical
Governance&58; Efficacy of Establishment in Mashhad Hospital. Patient Safety and Quality
Improvement Journal, 2(1), pp.48-52.
Elliott, D., Elliott, R., Burrell, A., Harrigan, P., Murgo, M., Rolls, K. and Sibbritt, D., 2015. Incidence of
ventilator-associated pneumonia in Australasian intensive care units: use of a consensus-developed
clinical surveillance checklist in a multisite prospective audit. BMJ open, 5(10), p.e008924.
Hunter, J.D., 2012. Ventilator associated pneumonia. Bmj, 344(e3325), p.e3225.
Kusahara, D.M., Peterlini, M.A.S. and Pedreira, M.L.G., 2012. Oral care with 0.12% chlorhexidine for
the prevention of ventilator-associated pneumonia in critically ill children: randomised, controlled
and double blind trial. International journal of nursing studies, 49(11), pp.1354-1363.
Lorente, L., Lecuona, M., Jiménez, A., Palmero, S., Pastor, E., Lafuente, N., Ramos, M.J., Mora, M.L.
and Sierra, A., 2012. Ventilator-associated pneumonia with or without toothbrushing: a randomized
controlled trial. European journal of clinical microbiology & infectious diseases, 31(10), pp.2621-
2629.
Özçaka, Ö., Başoğlu, Ö.K., Buduneli, N., Taşbakan, M.S., Bacakoğlu, F. and Kinane, D.F., 2012.
Chlorhexidine decreases the risk of ventilator associated pneumonia in intensive care unit patients:‐
a randomized clinical trial. Journal of periodontal research, 47(5), pp.584-592.
mechanically ventilated patients: a systematic review and meta-analysis of randomized trials
evaluating ventilator-associated pneumonia. Critical care medicine, 41(2), pp.646-655.
Barbier, F., Andremont, A., Wolff, M. and Bouadma, L., 2013. Hospital-acquired pneumonia and
ventilator-associated pneumonia: recent advances in epidemiology and management. Current
opinion in pulmonary medicine, 19(3), pp.216-228.
Bassi, G.L., Ferrer, M., Marti, J.D., Comaru, T. and Torres, A., 2014, August. Ventilator-associated
pneumonia. In Seminars in respiratory and critical care medicine (Vol. 35, No. 04, pp. 469-481).
Thieme Medical Publishers.
Blair, W. and Smith, B., 2012. Nursing documentation: frameworks and barriers. Contemporary
nurse, 41(2), pp.160-168.
Bouadma, L., Wolff, M. and Lucet, J.C., 2012. Ventilator-associated pneumonia and its
prevention. Current opinion in infectious diseases, 25(4), pp.395-404.
Charles, M.P., Kali, A., Easow, J.M., Joseph, N.M., Ravishankar, M., Srinivasan, S., Kumar, S. and
Umadevi, S., 2014. Ventilator-associated pneumonia. The Australasian medical journal, 7(8), p.334.
Cutler, L.R. and Sluman, P., 2014. Reducing ventilator associated pneumonia in adult patients
through high standards of oral care: A historical control study. Intensive and Critical Care
Nursing, 30(2), pp.61-68.
Davoodi, R., Soltanifar, A., Sh, R., Sabouri, G., Asadi, M., Takbiri, A. and Koleini, F., 2014. Clinical
Governance&58; Efficacy of Establishment in Mashhad Hospital. Patient Safety and Quality
Improvement Journal, 2(1), pp.48-52.
Elliott, D., Elliott, R., Burrell, A., Harrigan, P., Murgo, M., Rolls, K. and Sibbritt, D., 2015. Incidence of
ventilator-associated pneumonia in Australasian intensive care units: use of a consensus-developed
clinical surveillance checklist in a multisite prospective audit. BMJ open, 5(10), p.e008924.
Hunter, J.D., 2012. Ventilator associated pneumonia. Bmj, 344(e3325), p.e3225.
Kusahara, D.M., Peterlini, M.A.S. and Pedreira, M.L.G., 2012. Oral care with 0.12% chlorhexidine for
the prevention of ventilator-associated pneumonia in critically ill children: randomised, controlled
and double blind trial. International journal of nursing studies, 49(11), pp.1354-1363.
Lorente, L., Lecuona, M., Jiménez, A., Palmero, S., Pastor, E., Lafuente, N., Ramos, M.J., Mora, M.L.
and Sierra, A., 2012. Ventilator-associated pneumonia with or without toothbrushing: a randomized
controlled trial. European journal of clinical microbiology & infectious diseases, 31(10), pp.2621-
2629.
Özçaka, Ö., Başoğlu, Ö.K., Buduneli, N., Taşbakan, M.S., Bacakoğlu, F. and Kinane, D.F., 2012.
Chlorhexidine decreases the risk of ventilator associated pneumonia in intensive care unit patients:‐
a randomized clinical trial. Journal of periodontal research, 47(5), pp.584-592.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

Shi, Z., Xie, H., Wang, P., Zhang, Q., Wu, Y., Chen, E., Ng, L., Worthington, H.V., Needleman, I. and
Furness, S., 2013. Oral hygiene care for critically ill patients to prevent ventilator-associated
pneumonia. Cochrane Database Syst Rev, 8.
Specchia, M.L., Poscia, A., Volpe, M., Parente, P., Capizzi, S., Cambieri, A., Damiani, G., Ricciardi, W.
and De Belvis, A.G., 2015. Does clinical governance influence the appropriateness of hospital
stay?. BMC health services research, 15(1), p.142.
Furness, S., 2013. Oral hygiene care for critically ill patients to prevent ventilator-associated
pneumonia. Cochrane Database Syst Rev, 8.
Specchia, M.L., Poscia, A., Volpe, M., Parente, P., Capizzi, S., Cambieri, A., Damiani, G., Ricciardi, W.
and De Belvis, A.G., 2015. Does clinical governance influence the appropriateness of hospital
stay?. BMC health services research, 15(1), p.142.
NURS2006 Assignment 3 - CPI paper Marking Rubric
PERFORMANCE STANDARD
CATEGORY &
WEIGHTING Excellent Work Good Work Passing Work Unsatisfactory work
Project Aim
and Evidence
the issue is
worth solving
20%
Aim succinct & clearly
defined. All evidence
relevant & rigorous.
Shows a very high level of
insight & relevance to the
issue.
(17-20)
Aim well defined.
Some irrelevant
information but most
evidence relevant &
rigorous. Shows a very
good level of insight &
relevance to the issue.
(13-16.5)
Aim stated with some
ambiguity. Some evidence
relevant and rigorous,
Acceptable level of
insight.
Quite a lot of irrelevant
information is present.
May be overlong/ too
brief
(10-12.5)
Aim not clearly stated
Most evidence is not
relevant or rigorous.
Poor level of insight &
relevance to the issue.
Significant amount of
irrelevant/ missing
information.
(0–9.5)
Relevance of
Clinical
Governance to
your project
10%
Succinct and highly
relevant discussion of the
relevant pillar of clinical
governance related to the
chosen clinical issue.
(9-10)
Succinct and mostly
relevant discussion of the
relevant pillar of clinical
governance related to the
chosen clinical issue.
(7-8.5)
Adequate discussion of
the relevant pillar of
clinical governance
related to the chosen
clinical issue.
Some parts not relevant
Overlong / too brief, may
be missing relevant
information.
(5-6.5)
Inadequate discussion of
the relevant pillar of
clinical governance
related to the chosen
clinical issue. Overlong /
too brief, may be missing
a significant amount of
relevant information
(0-4.5)
Key
Stakeholders
5%
Identifies most relevant
key stakeholders.
Discusses clearly how they
could be involved in the
project.
Succinctly and expertly
written. Very high level of
insight into the role of
stakeholders.
(4.5 - 5)
Identifies some relevant
key stakeholders and
adequately discusses how
they could be involved in
the project.
Very well written. Good
level of insight into the
role of stakeholders.
(3.5-4.25)
Identifies a few relevant
key stakeholders.
Mentions briefly how they
could be involved. Quite
well written but contains
some irrelevant
information, or minor
information is missing.
Adequate level of insight
into the stakeholder role.
(2.5 – 3.25- )
Contains irrelevant
information, or major
information is missing.
Inappropriate or no key
stakeholders are
identified Poor insight
into the stakeholder role.
(0-2)
Clinical Practice
Improvement
Tool
20%
Describes a relevant CPI
tool Very clearly discusses
how it could be used to
address the aim and
implement the
interventions. Succinctly
and expertly written with
no omissions of relevant
information.
(17-20)
Describes a relevant CPI
tool Discusses quite
clearly how the tool could
be used to address the
aim and implement the
interventions. Well
written but may contain
some irrelevant
information, or some
minor information is
missing
(13-16.5)
Describes a relevant CPI
tool and adequately
discusses how the tool
could be used to address
the aim and implement
the interventions.
Not succinct, contains
irrelevant information,
significant information is
missing
(10-12.5)
A relevant CPI tool is not
identified. There is no
adequate discussion of
how the tool could be
used to meet the aim or
implement the
interventions.
Contains irrelevant
information or some
major information is
missing.
(0–9.5)
Summary of
proposed
interventions
20%
All relevant interventions
are discussed very well.
Project outline is very
clear and the relevance to
clinical practice is very
high.
Most relevant
interventions discussed
quite well.
Project outline is clear &
relevance to clinical
practice is good. Contains
some irrelevant
information, minor
information may be
missing.
Acceptable level of
relevant interventions
discussed.
Project outline mostly
clear, although it may be
unclear how the project
would actually be
implemented in clinical
practice due to
irrelevant/missing info
Some elements missing or
incomplete. May contain
large amounts of
irrelevant information.
Project poorly described
and it is unclear what the
project actually entails or
its relevance to clinical
practice.
PERFORMANCE STANDARD
CATEGORY &
WEIGHTING Excellent Work Good Work Passing Work Unsatisfactory work
Project Aim
and Evidence
the issue is
worth solving
20%
Aim succinct & clearly
defined. All evidence
relevant & rigorous.
Shows a very high level of
insight & relevance to the
issue.
(17-20)
Aim well defined.
Some irrelevant
information but most
evidence relevant &
rigorous. Shows a very
good level of insight &
relevance to the issue.
(13-16.5)
Aim stated with some
ambiguity. Some evidence
relevant and rigorous,
Acceptable level of
insight.
Quite a lot of irrelevant
information is present.
May be overlong/ too
brief
(10-12.5)
Aim not clearly stated
Most evidence is not
relevant or rigorous.
Poor level of insight &
relevance to the issue.
Significant amount of
irrelevant/ missing
information.
(0–9.5)
Relevance of
Clinical
Governance to
your project
10%
Succinct and highly
relevant discussion of the
relevant pillar of clinical
governance related to the
chosen clinical issue.
(9-10)
Succinct and mostly
relevant discussion of the
relevant pillar of clinical
governance related to the
chosen clinical issue.
(7-8.5)
Adequate discussion of
the relevant pillar of
clinical governance
related to the chosen
clinical issue.
Some parts not relevant
Overlong / too brief, may
be missing relevant
information.
(5-6.5)
Inadequate discussion of
the relevant pillar of
clinical governance
related to the chosen
clinical issue. Overlong /
too brief, may be missing
a significant amount of
relevant information
(0-4.5)
Key
Stakeholders
5%
Identifies most relevant
key stakeholders.
Discusses clearly how they
could be involved in the
project.
Succinctly and expertly
written. Very high level of
insight into the role of
stakeholders.
(4.5 - 5)
Identifies some relevant
key stakeholders and
adequately discusses how
they could be involved in
the project.
Very well written. Good
level of insight into the
role of stakeholders.
(3.5-4.25)
Identifies a few relevant
key stakeholders.
Mentions briefly how they
could be involved. Quite
well written but contains
some irrelevant
information, or minor
information is missing.
Adequate level of insight
into the stakeholder role.
(2.5 – 3.25- )
Contains irrelevant
information, or major
information is missing.
Inappropriate or no key
stakeholders are
identified Poor insight
into the stakeholder role.
(0-2)
Clinical Practice
Improvement
Tool
20%
Describes a relevant CPI
tool Very clearly discusses
how it could be used to
address the aim and
implement the
interventions. Succinctly
and expertly written with
no omissions of relevant
information.
(17-20)
Describes a relevant CPI
tool Discusses quite
clearly how the tool could
be used to address the
aim and implement the
interventions. Well
written but may contain
some irrelevant
information, or some
minor information is
missing
(13-16.5)
Describes a relevant CPI
tool and adequately
discusses how the tool
could be used to address
the aim and implement
the interventions.
Not succinct, contains
irrelevant information,
significant information is
missing
(10-12.5)
A relevant CPI tool is not
identified. There is no
adequate discussion of
how the tool could be
used to meet the aim or
implement the
interventions.
Contains irrelevant
information or some
major information is
missing.
(0–9.5)
Summary of
proposed
interventions
20%
All relevant interventions
are discussed very well.
Project outline is very
clear and the relevance to
clinical practice is very
high.
Most relevant
interventions discussed
quite well.
Project outline is clear &
relevance to clinical
practice is good. Contains
some irrelevant
information, minor
information may be
missing.
Acceptable level of
relevant interventions
discussed.
Project outline mostly
clear, although it may be
unclear how the project
would actually be
implemented in clinical
practice due to
irrelevant/missing info
Some elements missing or
incomplete. May contain
large amounts of
irrelevant information.
Project poorly described
and it is unclear what the
project actually entails or
its relevance to clinical
practice.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
(17-20) (13-16.5) (10-12.5) (0–9.5)
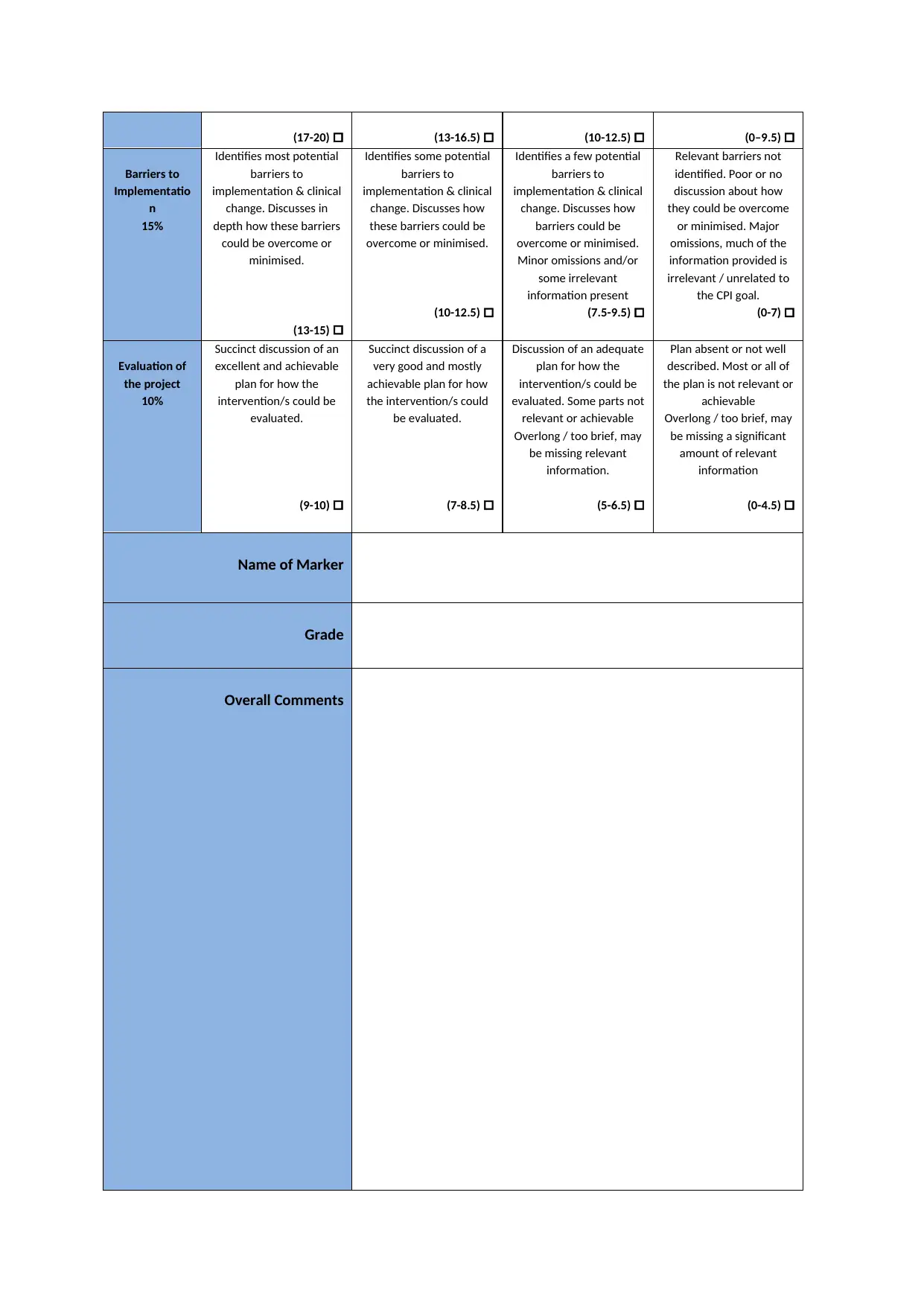
Barriers to
Implementatio
n
15%
Identifies most potential
barriers to
implementation & clinical
change. Discusses in
depth how these barriers
could be overcome or
minimised.
(13-15)
Identifies some potential
barriers to
implementation & clinical
change. Discusses how
these barriers could be
overcome or minimised.
(10-12.5)
Identifies a few potential
barriers to
implementation & clinical
change. Discusses how
barriers could be
overcome or minimised.
Minor omissions and/or
some irrelevant
information present
(7.5-9.5)
Relevant barriers not
identified. Poor or no
discussion about how
they could be overcome
or minimised. Major
omissions, much of the
information provided is
irrelevant / unrelated to
the CPI goal.
(0-7)
Evaluation of
the project
10%
Succinct discussion of an
excellent and achievable
plan for how the
intervention/s could be
evaluated.
(9-10)
Succinct discussion of a
very good and mostly
achievable plan for how
the intervention/s could
be evaluated.
(7-8.5)
Discussion of an adequate
plan for how the
intervention/s could be
evaluated. Some parts not
relevant or achievable
Overlong / too brief, may
be missing relevant
information.
(5-6.5)
Plan absent or not well
described. Most or all of
the plan is not relevant or
achievable
Overlong / too brief, may
be missing a significant
amount of relevant
information
(0-4.5)
Name of Marker
Grade
Overall Comments
Barriers to
Implementatio
n
15%
Identifies most potential
barriers to
implementation & clinical
change. Discusses in
depth how these barriers
could be overcome or
minimised.
(13-15)
Identifies some potential
barriers to
implementation & clinical
change. Discusses how
these barriers could be
overcome or minimised.
(10-12.5)
Identifies a few potential
barriers to
implementation & clinical
change. Discusses how
barriers could be
overcome or minimised.
Minor omissions and/or
some irrelevant
information present
(7.5-9.5)
Relevant barriers not
identified. Poor or no
discussion about how
they could be overcome
or minimised. Major
omissions, much of the
information provided is
irrelevant / unrelated to
the CPI goal.
(0-7)
Evaluation of
the project
10%
Succinct discussion of an
excellent and achievable
plan for how the
intervention/s could be
evaluated.
(9-10)
Succinct discussion of a
very good and mostly
achievable plan for how
the intervention/s could
be evaluated.
(7-8.5)
Discussion of an adequate
plan for how the
intervention/s could be
evaluated. Some parts not
relevant or achievable
Overlong / too brief, may
be missing relevant
information.
(5-6.5)
Plan absent or not well
described. Most or all of
the plan is not relevant or
achievable
Overlong / too brief, may
be missing a significant
amount of relevant
information
(0-4.5)
Name of Marker
Grade
Overall Comments
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1 out of 11
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.