Cardiogenic Shock Case Study: Nursing, Patient Erik Selvig Analysis
VerifiedAdded on 2022/10/15
|7
|1594
|18
Case Study
AI Summary
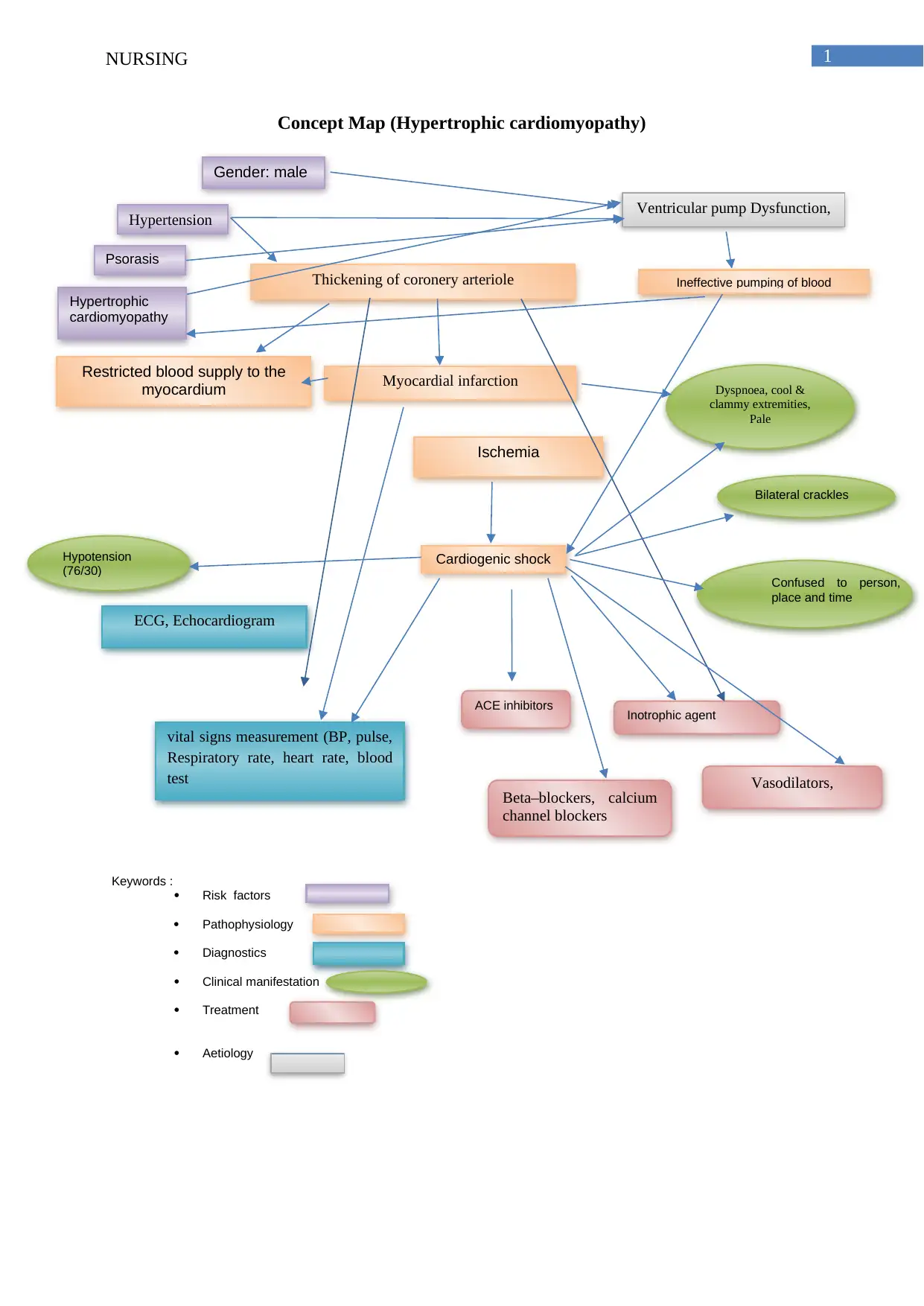
This case study examines the medical condition of Erik Selvig, who presented to the emergency department with worsening dyspnea and cool, clammy extremities, and a history of hypertension, psoriasis, and hypertrophic cardiomyopathy. Initial diagnosis revealed hypotension, an anterior ST myocardial infarction, and subsequent deterioration with bilateral crackles and confusion, leading to a diagnosis of cardiogenic shock due to ventricular pump dysfunction. The study explores the risk factors, including gender and pre-existing conditions like psoriasis and myocardial infarction, and delves into the pathophysiology, highlighting ischemia, hypotension, and the impact on organ perfusion. Diagnostic investigations, such as ECG and echocardiogram, are discussed, along with treatment options including inotropic agents, vasodilators, and beta-blockers. The case study underscores the complexity of cardiogenic shock and the importance of prompt diagnosis and management.

1 out of 7


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.