A Detailed Report on Nursing Care Strategies for COPD Patients
VerifiedAdded on 2020/03/23
|14
|3349
|44
Report
AI Summary
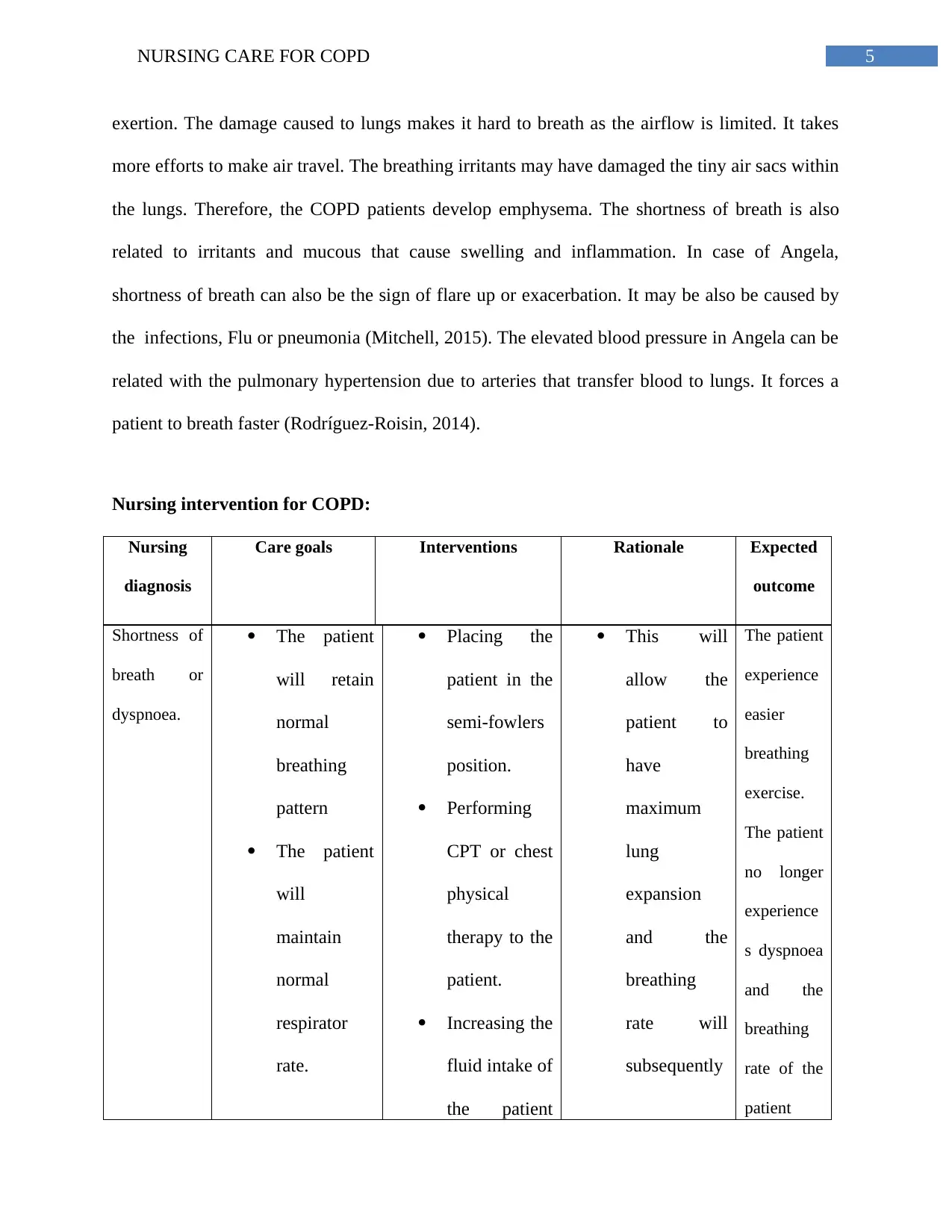
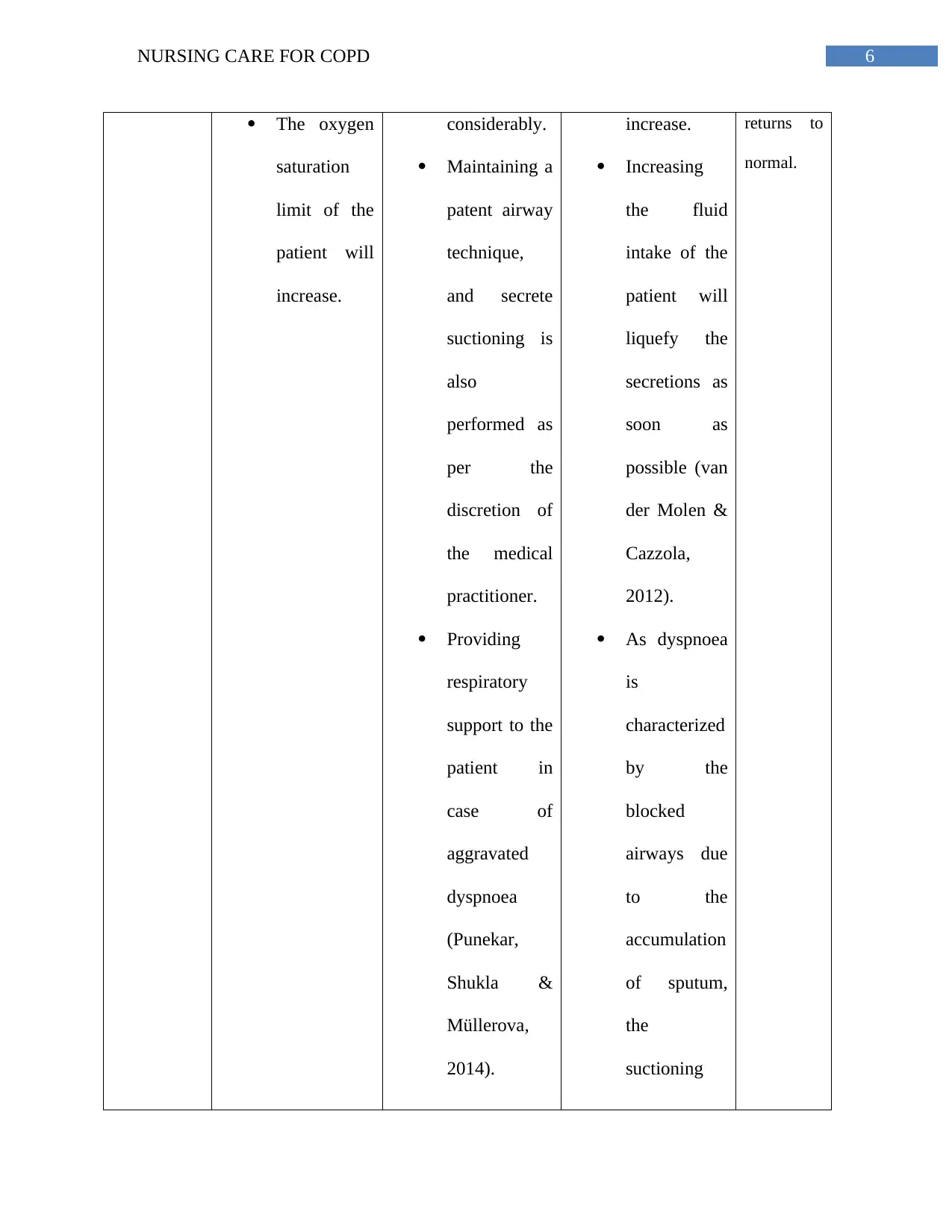
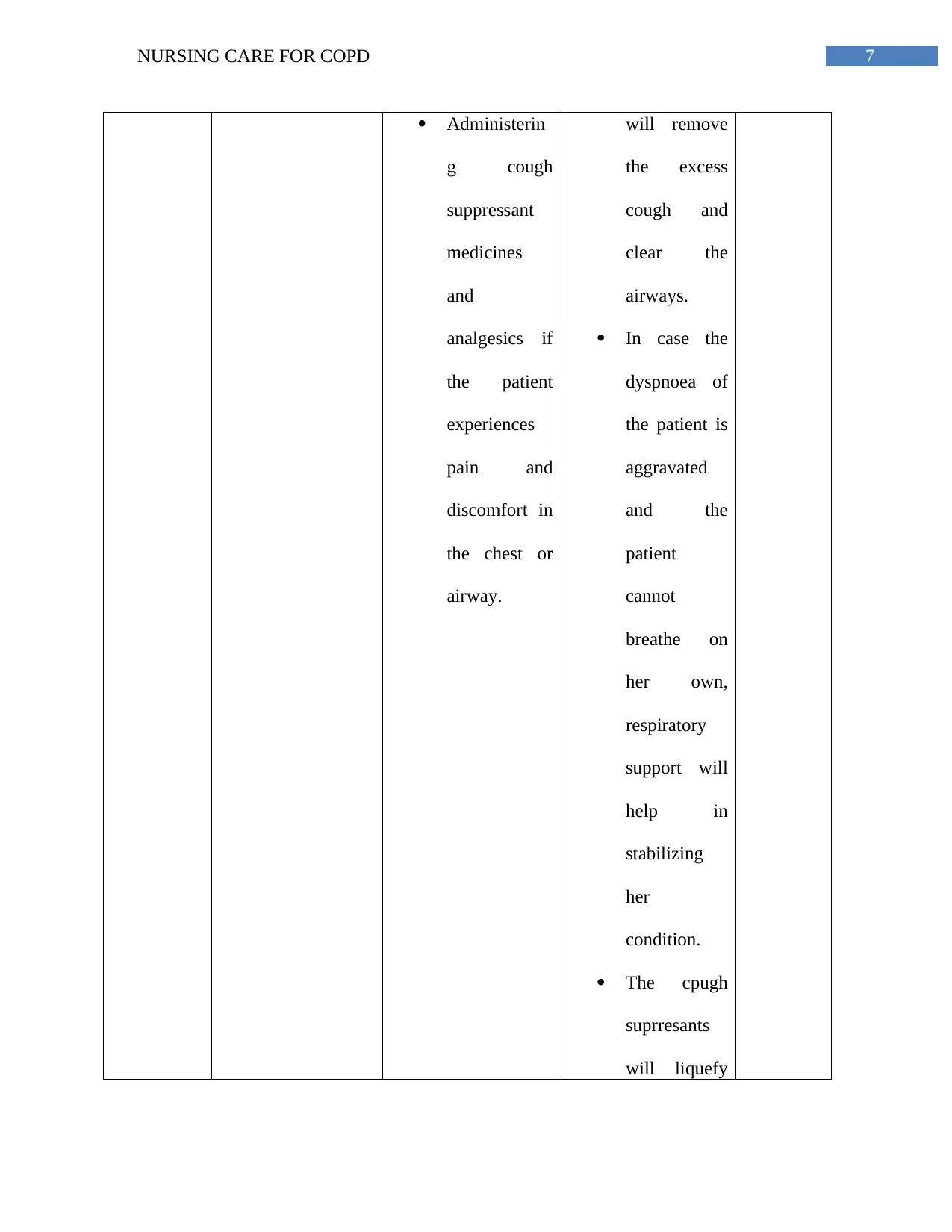
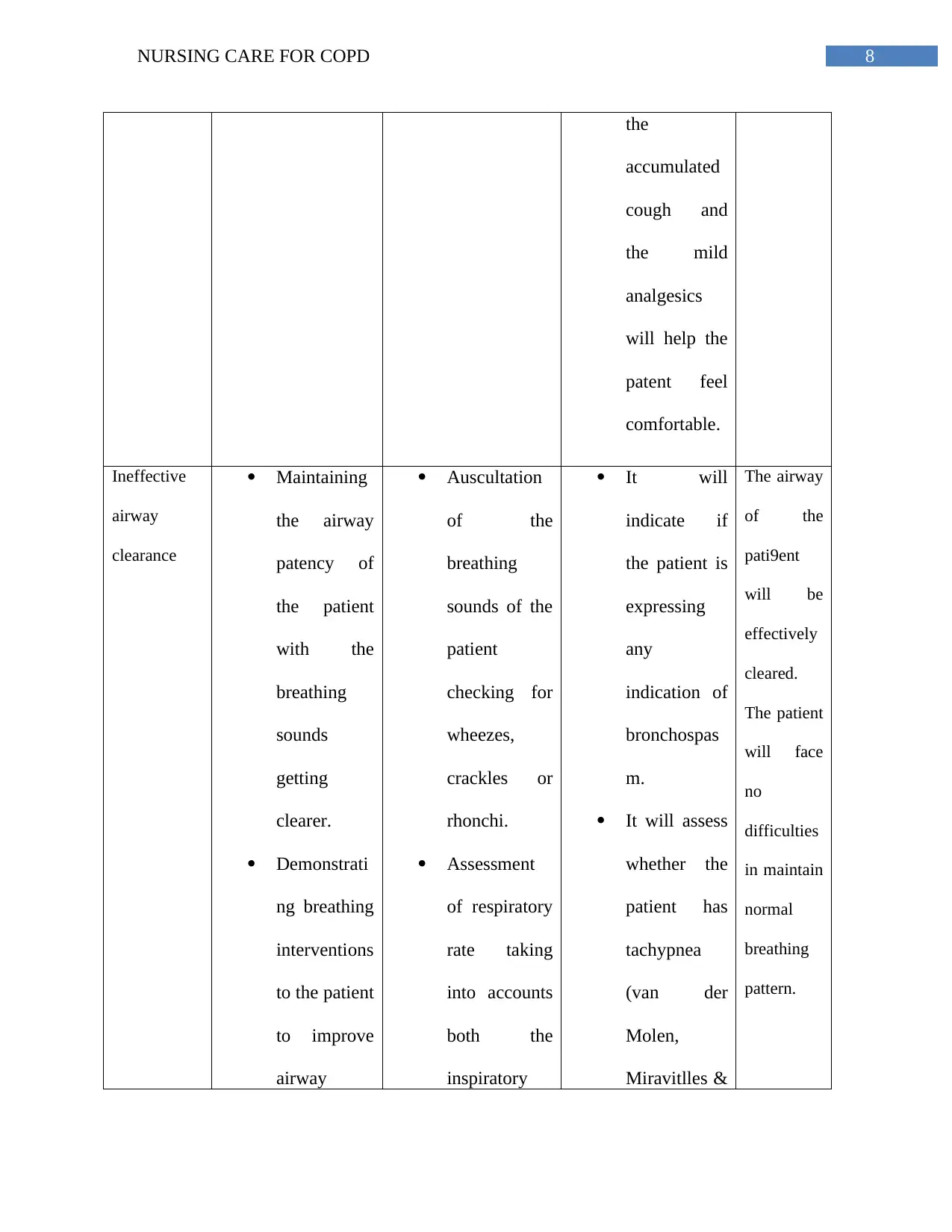
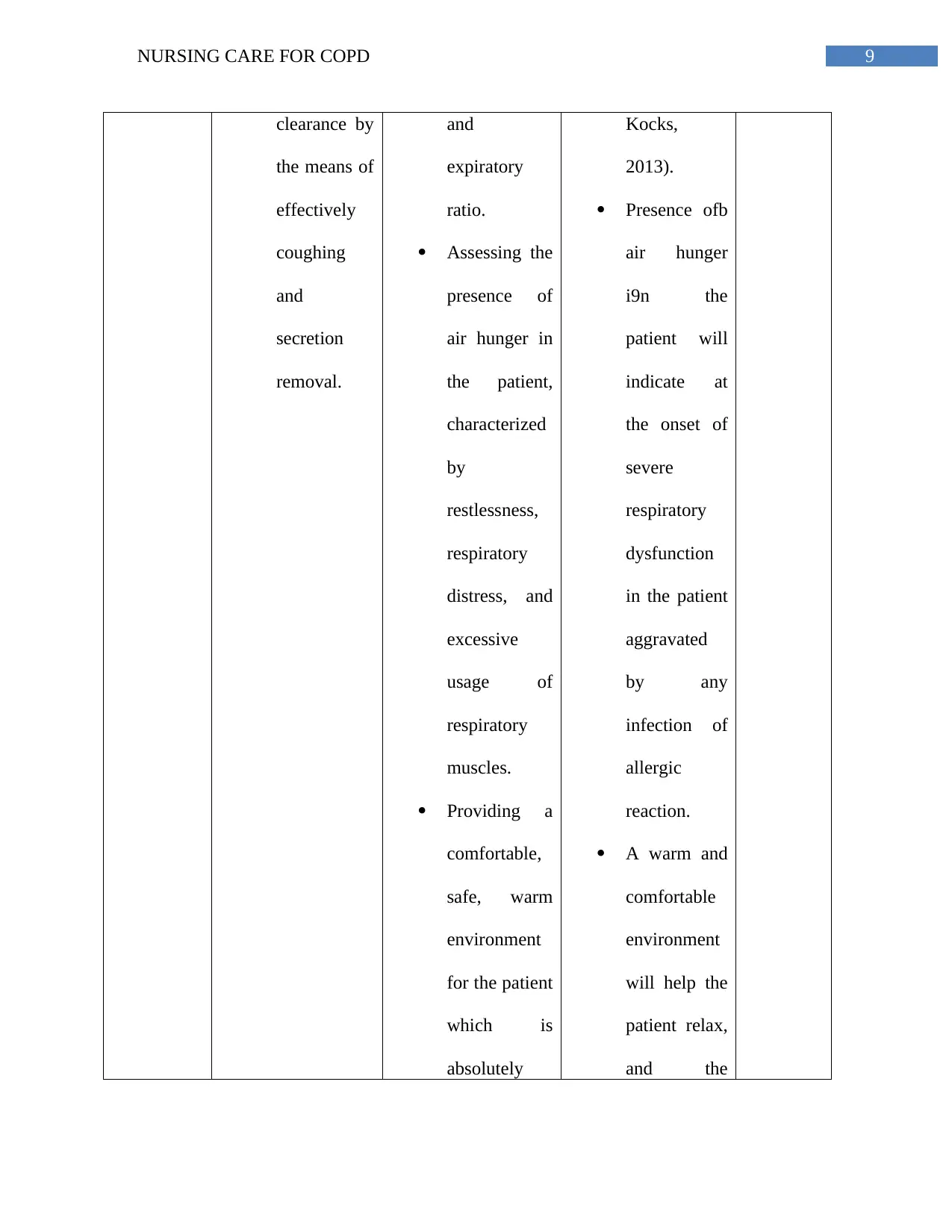
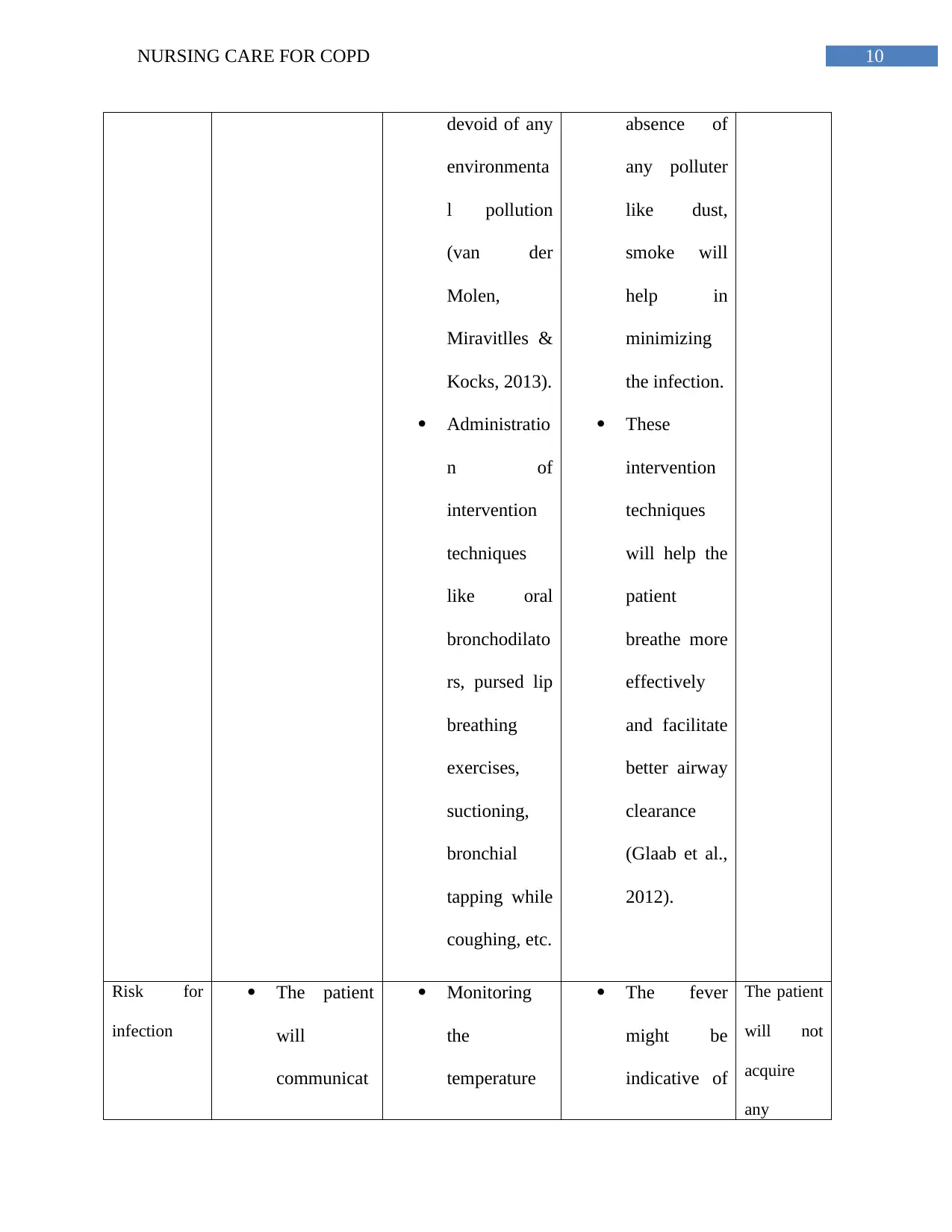
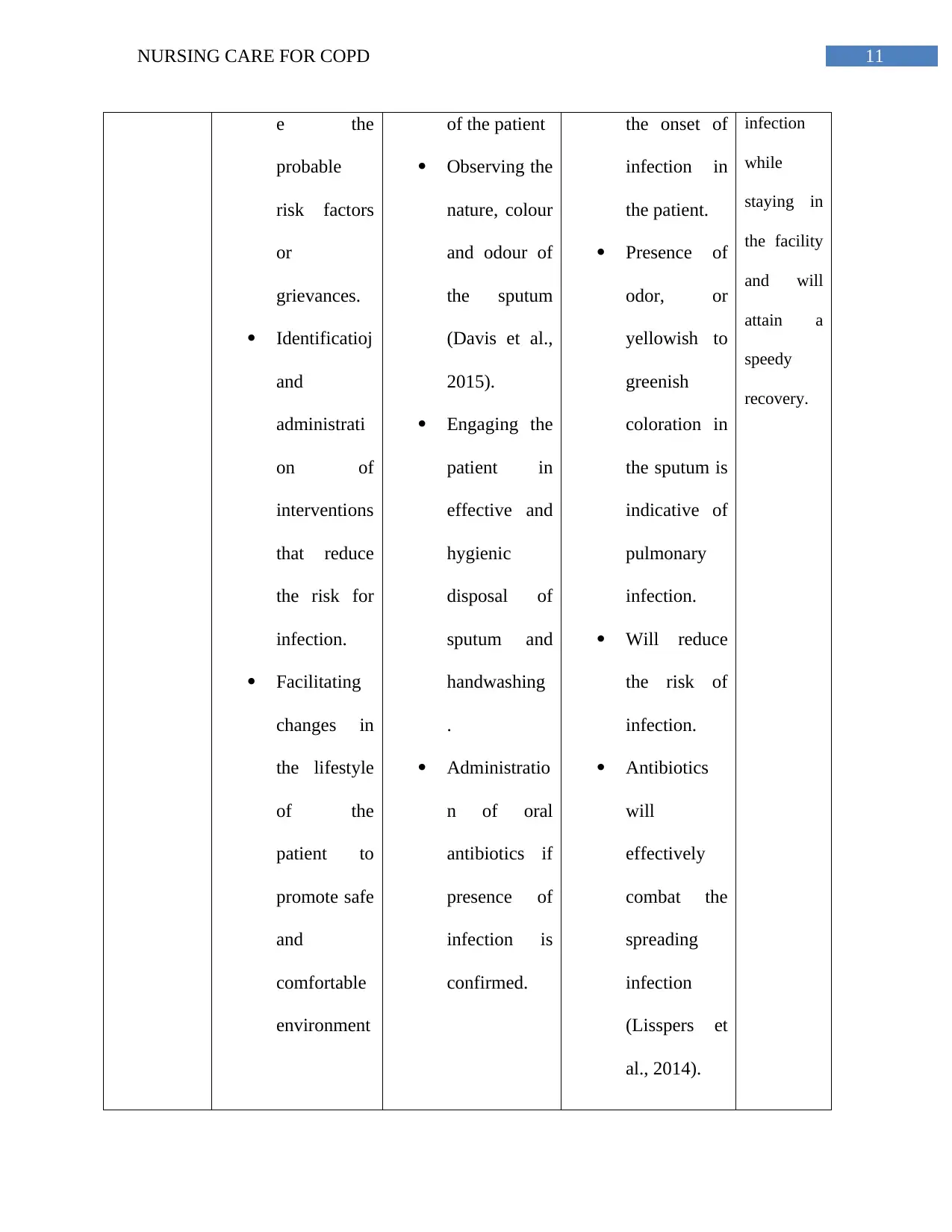
This report delves into the comprehensive nursing care required for patients diagnosed with Chronic Obstructive Pulmonary Disease (COPD). It begins with an introduction to COPD, its increasing prevalence, and its impact on global health, followed by an examination of the disease's complexity, chronicity, and associated comorbidities, such as diabetes and cardiovascular diseases. The report then analyzes a case study of a COPD patient, highlighting the interrelation of various factors affecting patient well-being, including physical and mental health, and the challenges faced by healthcare providers. Furthermore, it provides an in-depth understanding of COPD's pathophysiology, including airway inflammation, structural changes, and mucociliary dysfunction. The core of the report focuses on nursing interventions, encompassing nursing diagnoses, care goals, rationales, and expected outcomes, and it details interventions for dyspnea, ineffective airway clearance, and the risk of infection. The report also emphasizes the importance of health coaching, self-management strategies, patient empowerment, and advocacy, and it highlights the role of registered nurses in providing comprehensive care, including collaboration with other healthcare professionals. The report concludes by summarizing key aspects of COPD care and emphasizing the need for a multidisciplinary approach to improve patient outcomes.

1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.