Implantable Cardioverter Defibrillator: Comprehensive Nursing Care
VerifiedAdded on 2023/05/27
|4
|1184
|408
Presentation
AI Summary
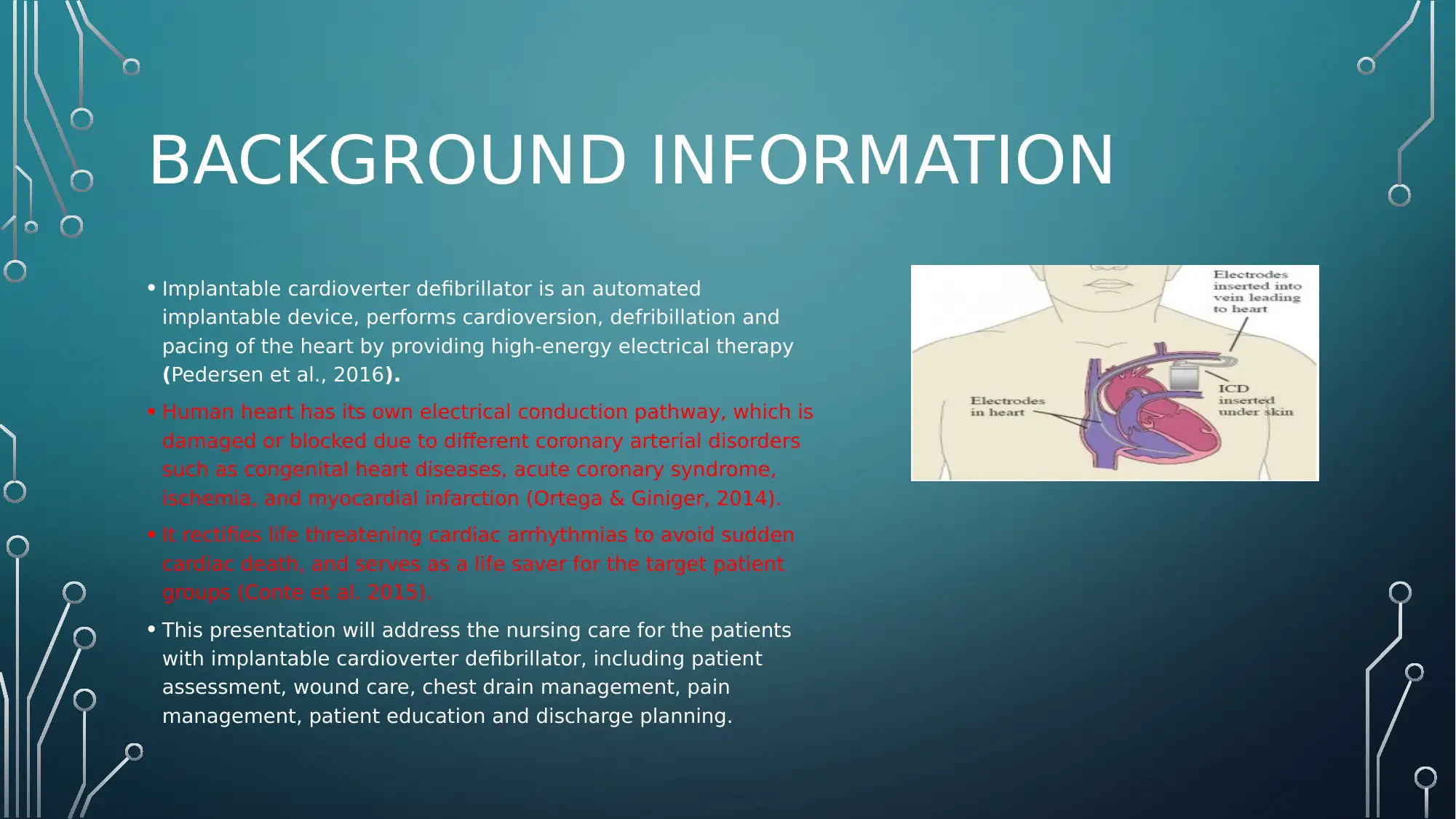
This presentation provides an overview of nursing care for patients with implantable cardioverter defibrillators (ICDs). It covers essential aspects such as patient assessment (including vital signs, physical assessment, and wound site assessment), wound care (emphasizing infection control and sterile dressing techniques), chest drain management, pain management (utilizing pain assessment scales and cautious analgesia administration), patient education on lifestyle changes and precautionary measures, and discharge planning. The presentation highlights the importance of addressing potential discomfort issues and ensuring patients understand when to seek medical help, with references to relevant research and clinical guidelines.
1 out of 4
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.