Nursing Assignment: Comprehensive Care Plan for C-Diff Infection
VerifiedAdded on 2020/05/03
|14
|4316
|111
Report
AI Summary
This nursing assignment focuses on the development of a comprehensive care plan for an 82-year-old male, Mr. James, admitted with a Clostridium difficile (C-Diff) infection. The assignment analyzes the patient's symptoms, including abdominal pain, watery diarrhea, and dehydration, and addresses the impact of the infection on his activities of daily living (ADLs), particularly eating, drinking, personal cleansing, dressing, and elimination. The care plan includes detailed nursing goals and interventions, such as dietary modifications, fluid management, and strict hand hygiene protocols to prevent the spread of infection. Nutritional screening tools like the Mini Nutritional Assessment (MNA) and Malnutrition Universal Screening Tool (MUST) are suggested for assessment. The assignment emphasizes the importance of monitoring the patient's condition, evaluating interventions, and ensuring the safe disposal of waste to prevent contamination. The Bristol stool chart is also used to track bowel movements. The goal is to restore fluid and electrolyte balance, promote normal appetite, and prevent the spread of the infection, thus ensuring comprehensive patient care.

Running head: NURSING ASSIGNMENT
Nursing assignment
Name of the Student
Name of the University
Author not
Nursing assignment
Name of the Student
Name of the University
Author not
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1NURSING ASSIGNMENT
In the recent years, Clostridium difficile (C-Diff) has emerged as major source of
morbidity among the older adults in long-term care (Lessa, Gould and McDonald 2012). The
clinical manifestations range from diarrhoeal illness to toxic megacolon and pseudomembranous
colitis. It is the most common infectious disease that is transmitted through spores in the stool
and can persist for weeks in the environment after infection (Blakney et al. 2015). Therefore,
environmental modification is required to decontaminate and reduce the severe infection.
Similarly, the given case study involves the in-depth analysis and nursing care plan for Mr.
James, an 82-year-old male admitted with C-Diff infection. He is currently showing symptoms
of abdominal pain, watery diarrhoea, loss of appetite, sudden weight loss and has an elevated
temperature of 38 degrees as the colon has inflamed forming raw tissues producing pseudo
membranous colitis. He is also complaining of lethargy affected by C-Diff that indicates severe
dehydration. There is lack of ability to perform the daily activities due to the severe infection and
so he requires assistance with activities of living (AoLs) (Rao et al. 2013). Personal dressing,
cleaning, safe environment, eating, drinking, elimination are some of the AoLs that require
modification for Mr. James. Apart from AOL’s modifications, proper nursing care plan is also
required for the proper management of the infection by identifying the risk factors, signs,
symptoms, nursing and medical management of the patient. However, there are issues related to
these AoLs and so, nursing care plan is necessary for Mr. James. Therefore, following discussion
involves the modifications in AoLs, the issues observed and proper nursing care plan for Mr.
James in the proper management of infection and patient care.
Eating and drinking is affected in Mr. James as due to diarrhoea, there is frequent active
fluid volume loss resulting in deficit in fluid volume. There are complications of diarrhoea that
compromises the health of the infected patient. Severe diarrhoea results in metabolic,
In the recent years, Clostridium difficile (C-Diff) has emerged as major source of
morbidity among the older adults in long-term care (Lessa, Gould and McDonald 2012). The
clinical manifestations range from diarrhoeal illness to toxic megacolon and pseudomembranous
colitis. It is the most common infectious disease that is transmitted through spores in the stool
and can persist for weeks in the environment after infection (Blakney et al. 2015). Therefore,
environmental modification is required to decontaminate and reduce the severe infection.
Similarly, the given case study involves the in-depth analysis and nursing care plan for Mr.
James, an 82-year-old male admitted with C-Diff infection. He is currently showing symptoms
of abdominal pain, watery diarrhoea, loss of appetite, sudden weight loss and has an elevated
temperature of 38 degrees as the colon has inflamed forming raw tissues producing pseudo
membranous colitis. He is also complaining of lethargy affected by C-Diff that indicates severe
dehydration. There is lack of ability to perform the daily activities due to the severe infection and
so he requires assistance with activities of living (AoLs) (Rao et al. 2013). Personal dressing,
cleaning, safe environment, eating, drinking, elimination are some of the AoLs that require
modification for Mr. James. Apart from AOL’s modifications, proper nursing care plan is also
required for the proper management of the infection by identifying the risk factors, signs,
symptoms, nursing and medical management of the patient. However, there are issues related to
these AoLs and so, nursing care plan is necessary for Mr. James. Therefore, following discussion
involves the modifications in AoLs, the issues observed and proper nursing care plan for Mr.
James in the proper management of infection and patient care.
Eating and drinking is affected in Mr. James as due to diarrhoea, there is frequent active
fluid volume loss resulting in deficit in fluid volume. There are complications of diarrhoea that
compromises the health of the infected patient. Severe diarrhoea results in metabolic,
2NURSING ASSIGNMENT
haemodynamic instability, and that result in lethargic condition and poor drinking and eating
patterns. The rapid propulsion of the intestinal contents through small bowels from the body
results in serious fluid deficit in the body. Moreover, the body wants to expel the foreign material
so that the body regains its normal digestion, however, the organs are unable to absorb excess
fluids that can absorbed by normal body. There is dehydration, impaired skin integrity due to
loss of moisture because of loose liquid stools (Surawicz et al. 2013). Similarly, the infection has
made him lose the ability to absorb the nutrients properly and that resulted in loss of appetite and
sudden weight loss. He is unable to digest the hard foods that irritate stomach like spicy foods or
raw vegetables. This depicts that nutrition plays an important role that has an impact on James
health as the infection resulted in dehydration being a common side effect of severe diarrhoea.
Another side effect of C.Diff infection that results in poor appetite and loss of weights is
malabsorption of nutrients. There is lack of nutrients like vitamin, sodium, potassium, calcium
and magnesium that result in weakness. This shows that dietary changes are required for Mr
James to regain weight and appetite (Leffler and Lamont 2015).
Nutritional screening can be used for the assessment of nutrition and fluid intake of
James. Nutritional screening tools like Mini Nutritional Assessment (MNA) can be used for
him, as it is a very reliable way for screening nutritional status and adding nutritional component
to the geriatric assessment. It identifies the nutritional status in him that identifies malnutrition
with a sensitivity of 98%, specificity 100% and 99% diagnostic accuracy among the individuals
above 65 years of age (Cereda 2012). Another screening tool Malnutrition Universal Screening
Tool (MUST) also assess nutritional level on three criteria; unintentional weight loss, BMI and
acute effect of disease that causes poor appetite and sudden weight loss (Poulia et al. 2012).
haemodynamic instability, and that result in lethargic condition and poor drinking and eating
patterns. The rapid propulsion of the intestinal contents through small bowels from the body
results in serious fluid deficit in the body. Moreover, the body wants to expel the foreign material
so that the body regains its normal digestion, however, the organs are unable to absorb excess
fluids that can absorbed by normal body. There is dehydration, impaired skin integrity due to
loss of moisture because of loose liquid stools (Surawicz et al. 2013). Similarly, the infection has
made him lose the ability to absorb the nutrients properly and that resulted in loss of appetite and
sudden weight loss. He is unable to digest the hard foods that irritate stomach like spicy foods or
raw vegetables. This depicts that nutrition plays an important role that has an impact on James
health as the infection resulted in dehydration being a common side effect of severe diarrhoea.
Another side effect of C.Diff infection that results in poor appetite and loss of weights is
malabsorption of nutrients. There is lack of nutrients like vitamin, sodium, potassium, calcium
and magnesium that result in weakness. This shows that dietary changes are required for Mr
James to regain weight and appetite (Leffler and Lamont 2015).
Nutritional screening can be used for the assessment of nutrition and fluid intake of
James. Nutritional screening tools like Mini Nutritional Assessment (MNA) can be used for
him, as it is a very reliable way for screening nutritional status and adding nutritional component
to the geriatric assessment. It identifies the nutritional status in him that identifies malnutrition
with a sensitivity of 98%, specificity 100% and 99% diagnostic accuracy among the individuals
above 65 years of age (Cereda 2012). Another screening tool Malnutrition Universal Screening
Tool (MUST) also assess nutritional level on three criteria; unintentional weight loss, BMI and
acute effect of disease that causes poor appetite and sudden weight loss (Poulia et al. 2012).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3NURSING ASSIGNMENT
The nursing assessment comprises of the abdominal discomfort, cramping, frequency,
liquid stools and pattern of defecation. This assessment is important for knowing the eating
patterns as these symptoms are linked to diarrhoea. Moreover, food intolerances, medications,
changes in eating pattern, tolerance to dairy products are also important for the assessment of
alterations in eating patterns that can cause intestinal function changes leading to diarrhoea.
Assessment is also required for hydration status as diarrhoea results in profound dehydration like
input and output, mucous membrane moisture and skin turgid (Shimizu et al. 2012). Due to
dehydration, there is dryness in the mucous membrane and decrease in skin turgidity along with
skin tenting. The nursing care plan for AoL issue in eating and drinking comprises of
maintaining the normal fluid volume at the patient’s functional level so that he remain hydrated,
maintain normal skin turgid and diet intake is equal to the output. The modifications are required
in diet that comprises of easily digestible foods and proper fluid intake so that electrolyte balance
is maintained in the body. Nurse also needs to look for lactose intolerance that is common side
effect of C. Diff along with gluten intolerance (Hooper et al. 2014).
Personal cleansing and dressing activities require modifications as they require attention
to reduce the transmission of infection and disease progression. As the infection spores are
persistent and viable in the environment, it is important to look for the personal hygiene like
hand hygiene, cleaning, dressing and personal protective equipments (PPEs). Due to diarrhoea,
James uses toilet frequently that may infect hands and it can spread through hand contamination.
This bacterium resides in the bowel and its multiplication produces toxins that cause diarrhoea. It
is highly infectious and spread rapidly through hand contamination, therefore, the strict hand
hygiene is required to reduce the spreading of germs and spore transmission through hands.
The nursing assessment comprises of the abdominal discomfort, cramping, frequency,
liquid stools and pattern of defecation. This assessment is important for knowing the eating
patterns as these symptoms are linked to diarrhoea. Moreover, food intolerances, medications,
changes in eating pattern, tolerance to dairy products are also important for the assessment of
alterations in eating patterns that can cause intestinal function changes leading to diarrhoea.
Assessment is also required for hydration status as diarrhoea results in profound dehydration like
input and output, mucous membrane moisture and skin turgid (Shimizu et al. 2012). Due to
dehydration, there is dryness in the mucous membrane and decrease in skin turgidity along with
skin tenting. The nursing care plan for AoL issue in eating and drinking comprises of
maintaining the normal fluid volume at the patient’s functional level so that he remain hydrated,
maintain normal skin turgid and diet intake is equal to the output. The modifications are required
in diet that comprises of easily digestible foods and proper fluid intake so that electrolyte balance
is maintained in the body. Nurse also needs to look for lactose intolerance that is common side
effect of C. Diff along with gluten intolerance (Hooper et al. 2014).
Personal cleansing and dressing activities require modifications as they require attention
to reduce the transmission of infection and disease progression. As the infection spores are
persistent and viable in the environment, it is important to look for the personal hygiene like
hand hygiene, cleaning, dressing and personal protective equipments (PPEs). Due to diarrhoea,
James uses toilet frequently that may infect hands and it can spread through hand contamination.
This bacterium resides in the bowel and its multiplication produces toxins that cause diarrhoea. It
is highly infectious and spread rapidly through hand contamination, therefore, the strict hand
hygiene is required to reduce the spreading of germs and spore transmission through hands.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4NURSING ASSIGNMENT
Personal dressing should also be clean and hygienic so that there is reduction in infection
transmission and spread of spores (Jetha 2014).
Personal hygiene assessment can be done through assessing the unwillingness or
inability of James to perform personal hygiene measures that would reflect self-care deficit.
Good hygiene like flossing, brushing, bathing should be assessed in James so that there should
be reduction in contamination of body fluids and transmission of pores. It can also be assessed
that PPE are being used James; hand washing is being performed by him after using toilet and
before eating (Farthing et al. 2013). All these assessments help to evaluate the personal hygiene
compliance in James. Functional Independence Measures (FIM) can be used for assessing self-
care items like dressing, bathing, brushing, grooming, bowel movement and toileting (Turolla et
al. 2013).
The nurse should help James to maintain good personal hygiene by washing hands
thoroughly using soap and water that removes the spores from the hand. Alcohol hands gels can
also be used to reduce the germ spreading before and after eating food. It prevents the spread of
infection as the spore transmission is prevented and as a result, the risk of getting C.Diff
infection would be reduced. The nurse should ensure that he uses gloves and decontaminate
hands after gloves removal with soap and water and should be encouraged to wash hands
regularly, nails kept clean, and short. Therefore, the nurse should evaluate his adherence to good
hand hygiene practices by performing hand washing that can reduce the incidence of spore
transmission and contamination (Dubberke et al. 2014).
The defecation or elimination is important in clostridium-infected patients as the stool
contains the spores. The safe disposal of the excrement is important as it helps in the prevention
Personal dressing should also be clean and hygienic so that there is reduction in infection
transmission and spread of spores (Jetha 2014).
Personal hygiene assessment can be done through assessing the unwillingness or
inability of James to perform personal hygiene measures that would reflect self-care deficit.
Good hygiene like flossing, brushing, bathing should be assessed in James so that there should
be reduction in contamination of body fluids and transmission of pores. It can also be assessed
that PPE are being used James; hand washing is being performed by him after using toilet and
before eating (Farthing et al. 2013). All these assessments help to evaluate the personal hygiene
compliance in James. Functional Independence Measures (FIM) can be used for assessing self-
care items like dressing, bathing, brushing, grooming, bowel movement and toileting (Turolla et
al. 2013).
The nurse should help James to maintain good personal hygiene by washing hands
thoroughly using soap and water that removes the spores from the hand. Alcohol hands gels can
also be used to reduce the germ spreading before and after eating food. It prevents the spread of
infection as the spore transmission is prevented and as a result, the risk of getting C.Diff
infection would be reduced. The nurse should ensure that he uses gloves and decontaminate
hands after gloves removal with soap and water and should be encouraged to wash hands
regularly, nails kept clean, and short. Therefore, the nurse should evaluate his adherence to good
hand hygiene practices by performing hand washing that can reduce the incidence of spore
transmission and contamination (Dubberke et al. 2014).
The defecation or elimination is important in clostridium-infected patients as the stool
contains the spores. The safe disposal of the excrement is important as it helps in the prevention
5NURSING ASSIGNMENT
of contamination of the patient’s clothing, hands and environment. The transport of the waste
and urine of the patients may contaminate the surrounding people and environment. This depicts
that elimination and disposal of waste should be safe through bedpans and urinals for proper
disinfection and cleaning. The stool contains spores in large amount that can infect healthy
people. Effective elimination of spores is important, as it can be helpful in the transmission of
spores and infection spread. There can also be abdominal tenderness that causes cramps and pain
due to continuous liquid bowel movements and so promotion of comfort is important for James
as it can result in emotional distress (McCune, Struthers and Hawkey 2014).
The assessment of elimination excrements and nursing care can be done through safe
disposal of waste and proper faecal transplantation. This is of critical importance by the nurse for
the prevention of contamination and soiling of hands, personal clothing and environment by
spores. Nurse should look that the excrements should be disposed safely to the soiled service
room and proper disinfection and cleaning of the patient after defecation. The nurses and
midwives should use washers and disinfectors after the elimination of waste and hand washing.
The nurse should teach James about hand washing after using toilet by using soap and water. In
this way, the nurse can provide care to James in the prevention and control of the spread of
infection. Bristol stool chart is important for the stool consistency pattern and in tracking daily
bowel movements as these are linked to diarrhoea (Burke and Lamont 2013).
From the above AoLs in the given case study, there are issues that require nursing goals
and interventions for the reduction of the infection spread and ensure patient care.
of contamination of the patient’s clothing, hands and environment. The transport of the waste
and urine of the patients may contaminate the surrounding people and environment. This depicts
that elimination and disposal of waste should be safe through bedpans and urinals for proper
disinfection and cleaning. The stool contains spores in large amount that can infect healthy
people. Effective elimination of spores is important, as it can be helpful in the transmission of
spores and infection spread. There can also be abdominal tenderness that causes cramps and pain
due to continuous liquid bowel movements and so promotion of comfort is important for James
as it can result in emotional distress (McCune, Struthers and Hawkey 2014).
The assessment of elimination excrements and nursing care can be done through safe
disposal of waste and proper faecal transplantation. This is of critical importance by the nurse for
the prevention of contamination and soiling of hands, personal clothing and environment by
spores. Nurse should look that the excrements should be disposed safely to the soiled service
room and proper disinfection and cleaning of the patient after defecation. The nurses and
midwives should use washers and disinfectors after the elimination of waste and hand washing.
The nurse should teach James about hand washing after using toilet by using soap and water. In
this way, the nurse can provide care to James in the prevention and control of the spread of
infection. Bristol stool chart is important for the stool consistency pattern and in tracking daily
bowel movements as these are linked to diarrhoea (Burke and Lamont 2013).
From the above AoLs in the given case study, there are issues that require nursing goals
and interventions for the reduction of the infection spread and ensure patient care.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6NURSING ASSIGNMENT
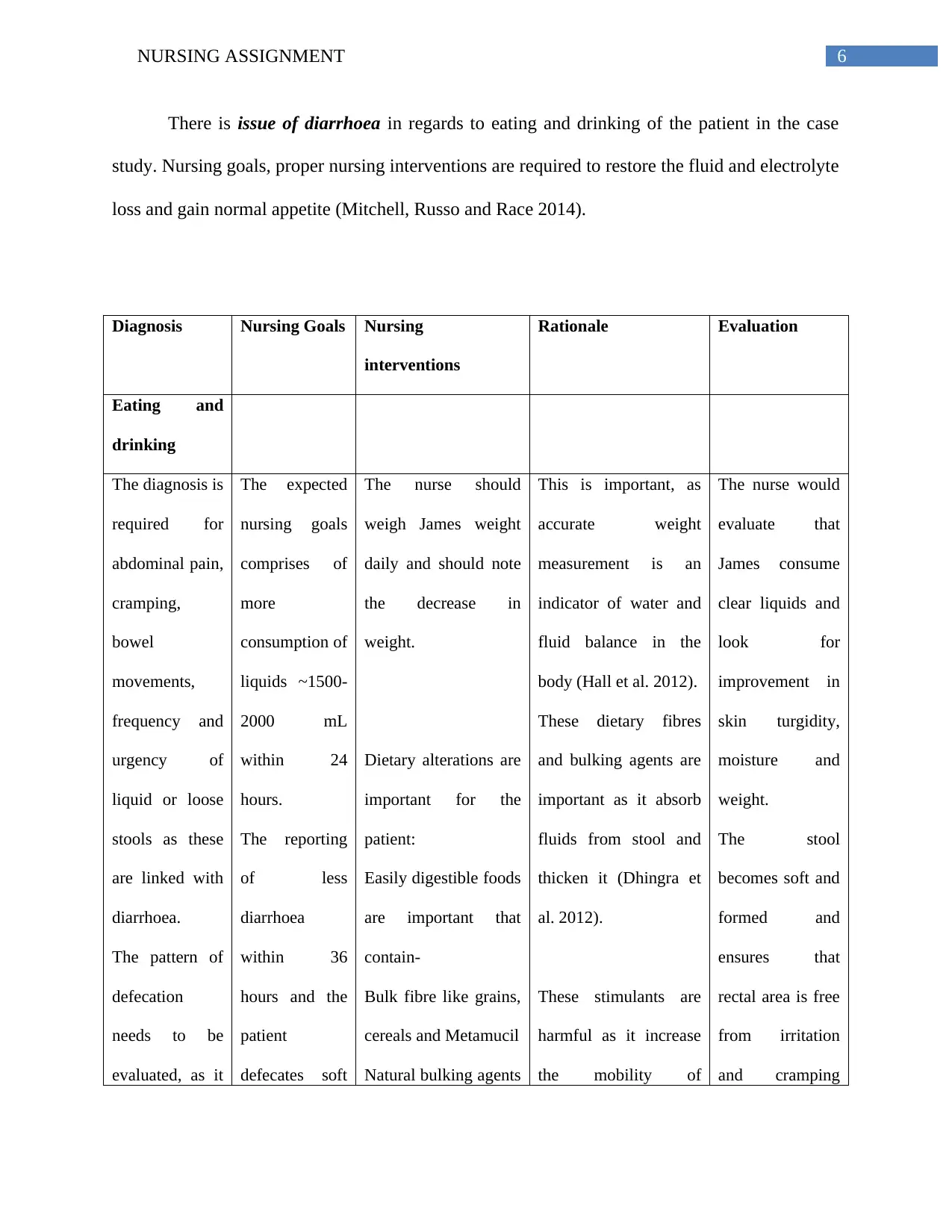
There is issue of diarrhoea in regards to eating and drinking of the patient in the case
study. Nursing goals, proper nursing interventions are required to restore the fluid and electrolyte
loss and gain normal appetite (Mitchell, Russo and Race 2014).
Diagnosis Nursing Goals Nursing
interventions
Rationale Evaluation
Eating and
drinking
The diagnosis is
required for
abdominal pain,
cramping,
bowel
movements,
frequency and
urgency of
liquid or loose
stools as these
are linked with
diarrhoea.
The pattern of
defecation
needs to be
evaluated, as it
The expected
nursing goals
comprises of
more
consumption of
liquids ~1500-
2000 mL
within 24
hours.
The reporting
of less
diarrhoea
within 36
hours and the
patient
defecates soft
The nurse should
weigh James weight
daily and should note
the decrease in
weight.
Dietary alterations are
important for the
patient:
Easily digestible foods
are important that
contain-
Bulk fibre like grains,
cereals and Metamucil
Natural bulking agents
This is important, as
accurate weight
measurement is an
indicator of water and
fluid balance in the
body (Hall et al. 2012).
These dietary fibres
and bulking agents are
important as it absorb
fluids from stool and
thicken it (Dhingra et
al. 2012).
These stimulants are
harmful as it increase
the mobility of
The nurse would
evaluate that
James consume
clear liquids and
look for
improvement in
skin turgidity,
moisture and
weight.
The stool
becomes soft and
formed and
ensures that
rectal area is free
from irritation
and cramping
There is issue of diarrhoea in regards to eating and drinking of the patient in the case
study. Nursing goals, proper nursing interventions are required to restore the fluid and electrolyte
loss and gain normal appetite (Mitchell, Russo and Race 2014).
Diagnosis Nursing Goals Nursing
interventions
Rationale Evaluation
Eating and
drinking
The diagnosis is
required for
abdominal pain,
cramping,
bowel
movements,
frequency and
urgency of
liquid or loose
stools as these
are linked with
diarrhoea.
The pattern of
defecation
needs to be
evaluated, as it
The expected
nursing goals
comprises of
more
consumption of
liquids ~1500-
2000 mL
within 24
hours.
The reporting
of less
diarrhoea
within 36
hours and the
patient
defecates soft
The nurse should
weigh James weight
daily and should note
the decrease in
weight.
Dietary alterations are
important for the
patient:
Easily digestible foods
are important that
contain-
Bulk fibre like grains,
cereals and Metamucil
Natural bulking agents
This is important, as
accurate weight
measurement is an
indicator of water and
fluid balance in the
body (Hall et al. 2012).
These dietary fibres
and bulking agents are
important as it absorb
fluids from stool and
thicken it (Dhingra et
al. 2012).
These stimulants are
harmful as it increase
the mobility of
The nurse would
evaluate that
James consume
clear liquids and
look for
improvement in
skin turgidity,
moisture and
weight.
The stool
becomes soft and
formed and
ensures that
rectal area is free
from irritation
and cramping
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING ASSIGNMENT
is important to
direct
treatment.
Food
intolerances,
tolerance to
dairy products,
changes in
eating pattern
as it can cause
intestinal
function
changes leading
to diarrhoea.
and formed
stool that
reliefs
cramping,
abdominal pain
with less or no
diarrhoea.
can be used like rice,
apples
There should be
avoidance of
stimulants like
caffeine.
The nurse should
encourage the patient
to intake fluids 1.5 to
2 L/24 hr and 200 mL
that provide
nutritional support.
The nurse should
encourage the patient
to eat frequent, but
small meals that can
be easily digestible by
him and causes
constipation.
For controlling
diarrhoea, the nurse
should make dietary
changes like
gastrointestinal tract
and worsen the
diarrhoea condition.
This increased fluid
intake replenishes the
fluid loss due to
continuous liquid
stools.
Starchy and blanchy
foods are
recommended before
starting to eat normal
food again (Slavin
2013).
These dietary
modifications aid in
slowing down the
passage of stool
with no negative
stools.
is important to
direct
treatment.
Food
intolerances,
tolerance to
dairy products,
changes in
eating pattern
as it can cause
intestinal
function
changes leading
to diarrhoea.
and formed
stool that
reliefs
cramping,
abdominal pain
with less or no
diarrhoea.
can be used like rice,
apples
There should be
avoidance of
stimulants like
caffeine.
The nurse should
encourage the patient
to intake fluids 1.5 to
2 L/24 hr and 200 mL
that provide
nutritional support.
The nurse should
encourage the patient
to eat frequent, but
small meals that can
be easily digestible by
him and causes
constipation.
For controlling
diarrhoea, the nurse
should make dietary
changes like
gastrointestinal tract
and worsen the
diarrhoea condition.
This increased fluid
intake replenishes the
fluid loss due to
continuous liquid
stools.
Starchy and blanchy
foods are
recommended before
starting to eat normal
food again (Slavin
2013).
These dietary
modifications aid in
slowing down the
passage of stool
with no negative
stools.
8NURSING ASSIGNMENT
avoidance of spicy
foods, fried and
encourage boiled or
braked foods.
through colon and help
to eliminate or reduce
diarrhoea (Mudgil and
Barak 2013).
Personal
cleansing and
dressing
The diagnosis is
required for the
self-care
activities like
disorderly
appearance,
ambulation,
grooming and
bathing self-
independently,
dressing and
feeding
independently
and
autonomously,
finishing of
toilet tasks and
maintaining
personal
The nursing
goals
comprises of
the
optimization of
independence
in performing
activities of
personal
dressing and
cleansing.
The patient can
execute
activities of
personal care
within his
ability and be
able to meet
his self-care
The nurse should
promote privacy
during dressing.
Frequent
encouragement needs
to be given so that it
can aid him in
dressing.
The clothing size
should be one size
longer.
The use of assistive
devices for dressing
by nurse can help the
patient in self-care
tasks.
The assessment of
This privacy need is
important for James, as
it is fundamental for
him, as he may fear of
privacy breaching.
This assistance can be
helpful so that his tasks
are smooth and do not
negate the attempts of
the patient.
This imparts comfort
and easier dressing.
This intervention can
help James to continue
independence and
autonomy in self-care
activity.
This would help to
The evaluation
can be done by
looking into
optimization of
independence
and autonomy.
There are
lifestyle changes
so that James is
able to meet the
self-care needs
and able to
recognize
individual needs
or weakness.
The tasks include
ability to feed,
dress, bathe,
groom,
avoidance of spicy
foods, fried and
encourage boiled or
braked foods.
through colon and help
to eliminate or reduce
diarrhoea (Mudgil and
Barak 2013).
Personal
cleansing and
dressing
The diagnosis is
required for the
self-care
activities like
disorderly
appearance,
ambulation,
grooming and
bathing self-
independently,
dressing and
feeding
independently
and
autonomously,
finishing of
toilet tasks and
maintaining
personal
The nursing
goals
comprises of
the
optimization of
independence
in performing
activities of
personal
dressing and
cleansing.
The patient can
execute
activities of
personal care
within his
ability and be
able to meet
his self-care
The nurse should
promote privacy
during dressing.
Frequent
encouragement needs
to be given so that it
can aid him in
dressing.
The clothing size
should be one size
longer.
The use of assistive
devices for dressing
by nurse can help the
patient in self-care
tasks.
The assessment of
This privacy need is
important for James, as
it is fundamental for
him, as he may fear of
privacy breaching.
This assistance can be
helpful so that his tasks
are smooth and do not
negate the attempts of
the patient.
This imparts comfort
and easier dressing.
This intervention can
help James to continue
independence and
autonomy in self-care
activity.
This would help to
The evaluation
can be done by
looking into
optimization of
independence
and autonomy.
There are
lifestyle changes
so that James is
able to meet the
self-care needs
and able to
recognize
individual needs
or weakness.
The tasks include
ability to feed,
dress, bathe,
groom,
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9NURSING ASSIGNMENT
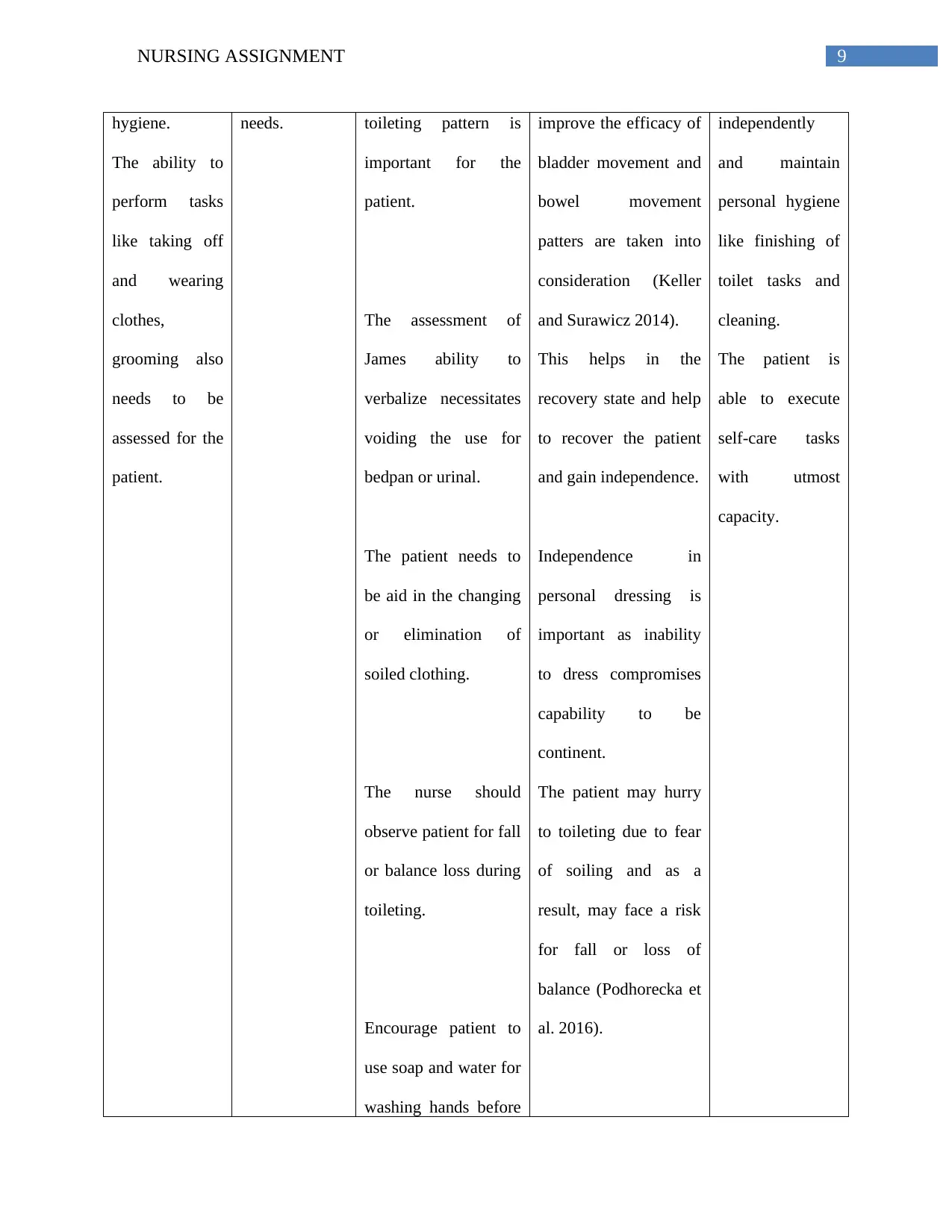
hygiene.
The ability to
perform tasks
like taking off
and wearing
clothes,
grooming also
needs to be
assessed for the
patient.
needs. toileting pattern is
important for the
patient.
The assessment of
James ability to
verbalize necessitates
voiding the use for
bedpan or urinal.
The patient needs to
be aid in the changing
or elimination of
soiled clothing.
The nurse should
observe patient for fall
or balance loss during
toileting.
Encourage patient to
use soap and water for
washing hands before
improve the efficacy of
bladder movement and
bowel movement
patters are taken into
consideration (Keller
and Surawicz 2014).
This helps in the
recovery state and help
to recover the patient
and gain independence.
Independence in
personal dressing is
important as inability
to dress compromises
capability to be
continent.
The patient may hurry
to toileting due to fear
of soiling and as a
result, may face a risk
for fall or loss of
balance (Podhorecka et
al. 2016).
independently
and maintain
personal hygiene
like finishing of
toilet tasks and
cleaning.
The patient is
able to execute
self-care tasks
with utmost
capacity.
hygiene.
The ability to
perform tasks
like taking off
and wearing
clothes,
grooming also
needs to be
assessed for the
patient.
needs. toileting pattern is
important for the
patient.
The assessment of
James ability to
verbalize necessitates
voiding the use for
bedpan or urinal.
The patient needs to
be aid in the changing
or elimination of
soiled clothing.
The nurse should
observe patient for fall
or balance loss during
toileting.
Encourage patient to
use soap and water for
washing hands before
improve the efficacy of
bladder movement and
bowel movement
patters are taken into
consideration (Keller
and Surawicz 2014).
This helps in the
recovery state and help
to recover the patient
and gain independence.
Independence in
personal dressing is
important as inability
to dress compromises
capability to be
continent.
The patient may hurry
to toileting due to fear
of soiling and as a
result, may face a risk
for fall or loss of
balance (Podhorecka et
al. 2016).
independently
and maintain
personal hygiene
like finishing of
toilet tasks and
cleaning.
The patient is
able to execute
self-care tasks
with utmost
capacity.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10NURSING ASSIGNMENT
and after eating and
toileting.
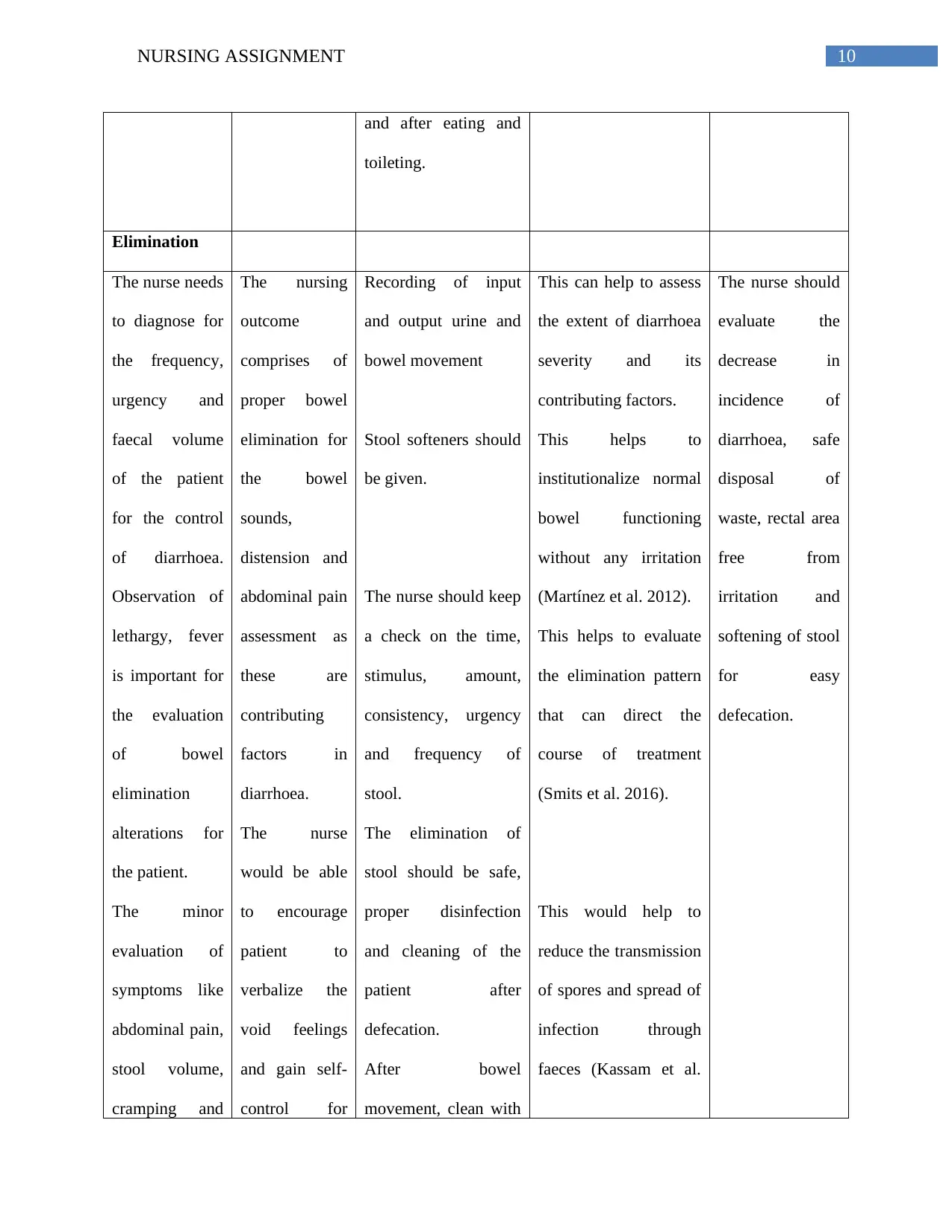
Elimination
The nurse needs
to diagnose for
the frequency,
urgency and
faecal volume
of the patient
for the control
of diarrhoea.
Observation of
lethargy, fever
is important for
the evaluation
of bowel
elimination
alterations for
the patient.
The minor
evaluation of
symptoms like
abdominal pain,
stool volume,
cramping and
The nursing
outcome
comprises of
proper bowel
elimination for
the bowel
sounds,
distension and
abdominal pain
assessment as
these are
contributing
factors in
diarrhoea.
The nurse
would be able
to encourage
patient to
verbalize the
void feelings
and gain self-
control for
Recording of input
and output urine and
bowel movement
Stool softeners should
be given.
The nurse should keep
a check on the time,
stimulus, amount,
consistency, urgency
and frequency of
stool.
The elimination of
stool should be safe,
proper disinfection
and cleaning of the
patient after
defecation.
After bowel
movement, clean with
This can help to assess
the extent of diarrhoea
severity and its
contributing factors.
This helps to
institutionalize normal
bowel functioning
without any irritation
(Martínez et al. 2012).
This helps to evaluate
the elimination pattern
that can direct the
course of treatment
(Smits et al. 2016).
This would help to
reduce the transmission
of spores and spread of
infection through
faeces (Kassam et al.
The nurse should
evaluate the
decrease in
incidence of
diarrhoea, safe
disposal of
waste, rectal area
free from
irritation and
softening of stool
for easy
defecation.
and after eating and
toileting.
Elimination
The nurse needs
to diagnose for
the frequency,
urgency and
faecal volume
of the patient
for the control
of diarrhoea.
Observation of
lethargy, fever
is important for
the evaluation
of bowel
elimination
alterations for
the patient.
The minor
evaluation of
symptoms like
abdominal pain,
stool volume,
cramping and
The nursing
outcome
comprises of
proper bowel
elimination for
the bowel
sounds,
distension and
abdominal pain
assessment as
these are
contributing
factors in
diarrhoea.
The nurse
would be able
to encourage
patient to
verbalize the
void feelings
and gain self-
control for
Recording of input
and output urine and
bowel movement
Stool softeners should
be given.
The nurse should keep
a check on the time,
stimulus, amount,
consistency, urgency
and frequency of
stool.
The elimination of
stool should be safe,
proper disinfection
and cleaning of the
patient after
defecation.
After bowel
movement, clean with
This can help to assess
the extent of diarrhoea
severity and its
contributing factors.
This helps to
institutionalize normal
bowel functioning
without any irritation
(Martínez et al. 2012).
This helps to evaluate
the elimination pattern
that can direct the
course of treatment
(Smits et al. 2016).
This would help to
reduce the transmission
of spores and spread of
infection through
faeces (Kassam et al.
The nurse should
evaluate the
decrease in
incidence of
diarrhoea, safe
disposal of
waste, rectal area
free from
irritation and
softening of stool
for easy
defecation.
11NURSING ASSIGNMENT
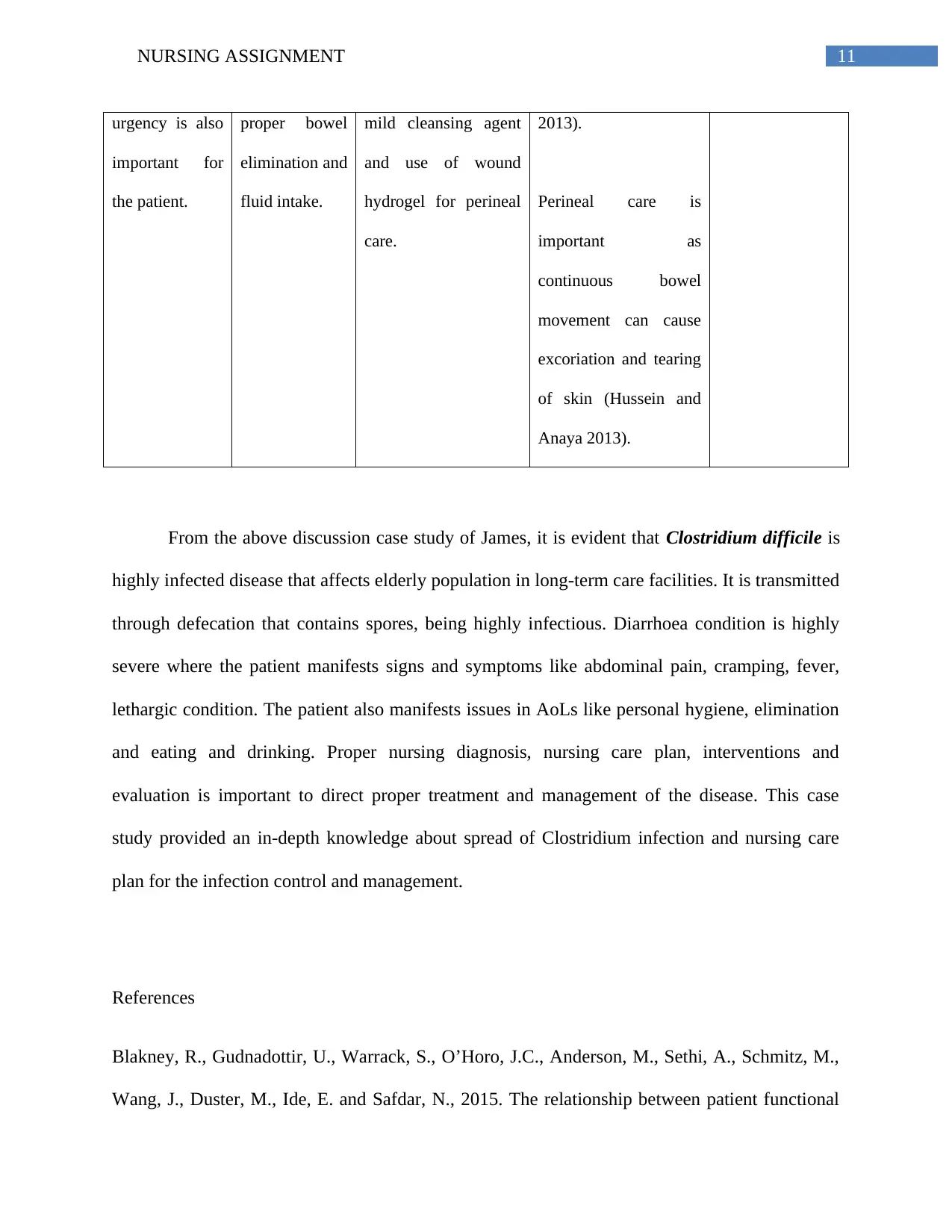
urgency is also
important for
the patient.
proper bowel
elimination and
fluid intake.
mild cleansing agent
and use of wound
hydrogel for perineal
care.
2013).
Perineal care is
important as
continuous bowel
movement can cause
excoriation and tearing
of skin (Hussein and
Anaya 2013).
From the above discussion case study of James, it is evident that Clostridium difficile is
highly infected disease that affects elderly population in long-term care facilities. It is transmitted
through defecation that contains spores, being highly infectious. Diarrhoea condition is highly
severe where the patient manifests signs and symptoms like abdominal pain, cramping, fever,
lethargic condition. The patient also manifests issues in AoLs like personal hygiene, elimination
and eating and drinking. Proper nursing diagnosis, nursing care plan, interventions and
evaluation is important to direct proper treatment and management of the disease. This case
study provided an in-depth knowledge about spread of Clostridium infection and nursing care
plan for the infection control and management.
References
Blakney, R., Gudnadottir, U., Warrack, S., O’Horo, J.C., Anderson, M., Sethi, A., Schmitz, M.,
Wang, J., Duster, M., Ide, E. and Safdar, N., 2015. The relationship between patient functional
urgency is also
important for
the patient.
proper bowel
elimination and
fluid intake.
mild cleansing agent
and use of wound
hydrogel for perineal
care.
2013).
Perineal care is
important as
continuous bowel
movement can cause
excoriation and tearing
of skin (Hussein and
Anaya 2013).
From the above discussion case study of James, it is evident that Clostridium difficile is
highly infected disease that affects elderly population in long-term care facilities. It is transmitted
through defecation that contains spores, being highly infectious. Diarrhoea condition is highly
severe where the patient manifests signs and symptoms like abdominal pain, cramping, fever,
lethargic condition. The patient also manifests issues in AoLs like personal hygiene, elimination
and eating and drinking. Proper nursing diagnosis, nursing care plan, interventions and
evaluation is important to direct proper treatment and management of the disease. This case
study provided an in-depth knowledge about spread of Clostridium infection and nursing care
plan for the infection control and management.
References
Blakney, R., Gudnadottir, U., Warrack, S., O’Horo, J.C., Anderson, M., Sethi, A., Schmitz, M.,
Wang, J., Duster, M., Ide, E. and Safdar, N., 2015. The relationship between patient functional
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.