Neonatal Case Study: Hyperbilirubinemia, Assessment, and Interventions
VerifiedAdded on 2022/10/04
|8
|1729
|15
Case Study
AI Summary
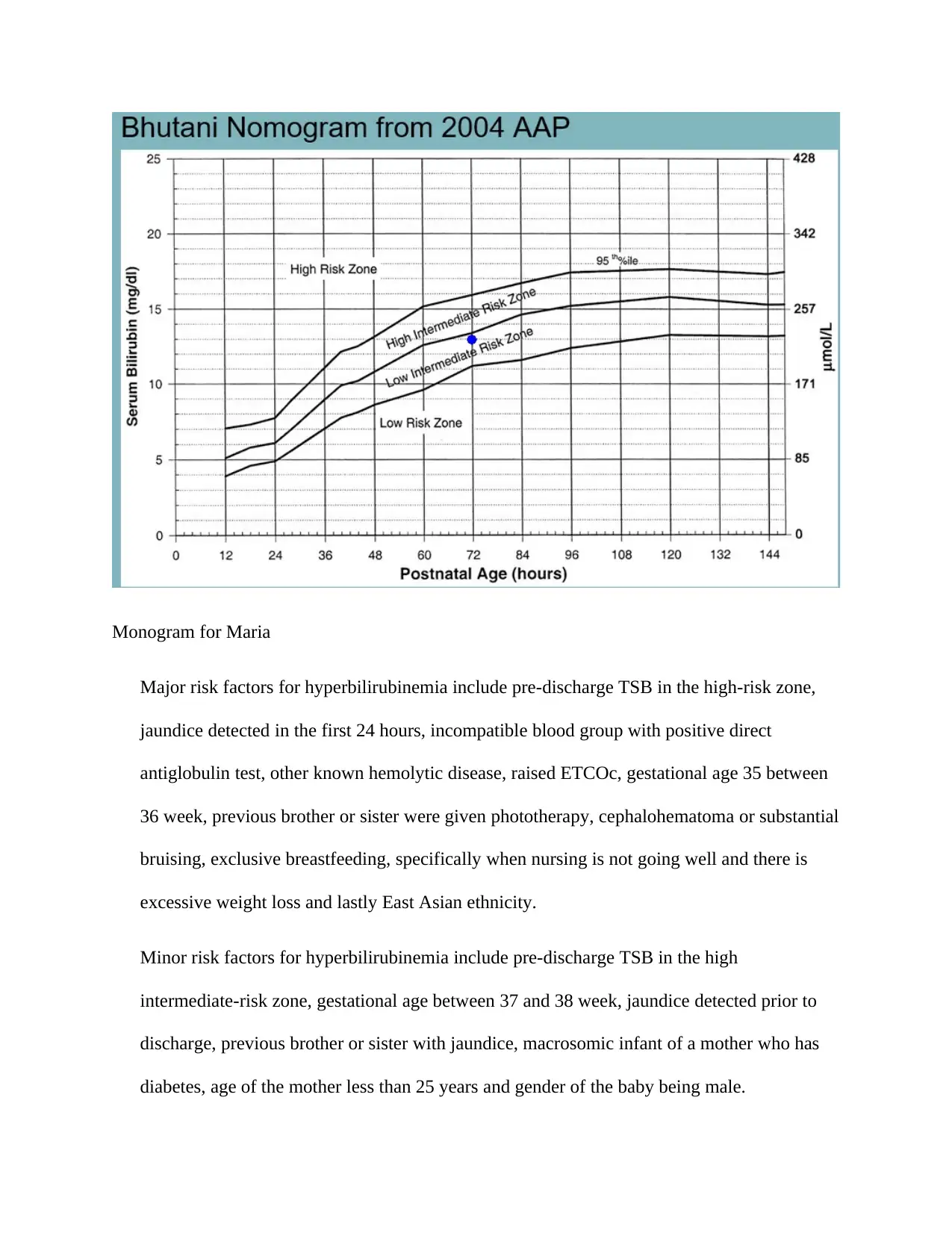
This case study focuses on a 2-day-old female newborn, Maria, presenting with symptoms of hyperbilirubinemia. The assessment reveals a N-PASS pain score of 5, indicating pain, and a yellow tint indicative of jaundice. The mother reports the baby is sleepy, has poor feeding, and is frustrated during breastfeeding. The assessment, using the SBAR format, highlights the need for delayed discharge and further investigation. Maria falls into the low-intermediate risk zone of hyperbilirubinemia based on the Bhutani Nomogram. The diagnosis is advancing pathological unconjugated hyperbilirubinemia, with an expected treatment plan of phototherapy. The case study outlines the treatment plan, potential complications such as bilirubin-induced neurologic dysfunction (BIND) and kernicterus, and family-centered interventions, including education about jaundice, home management, and the importance of follow-up. Bowlby's attachment theory is also applied, highlighting the importance of secure attachments. The nursing interventions include monitoring bilirubin levels, providing phototherapy, and educating the parents about the condition, its management, and potential complications. The expected outcomes are to control the jaundice, resolve it within the first week of life, and prevent CNS involvement. Further laboratory tests will be warranted if hyperbilirubinemia persists. References are provided in APA format, including peer-reviewed articles and textbook references, as per the assignment brief requirements.
1 out of 8


Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.