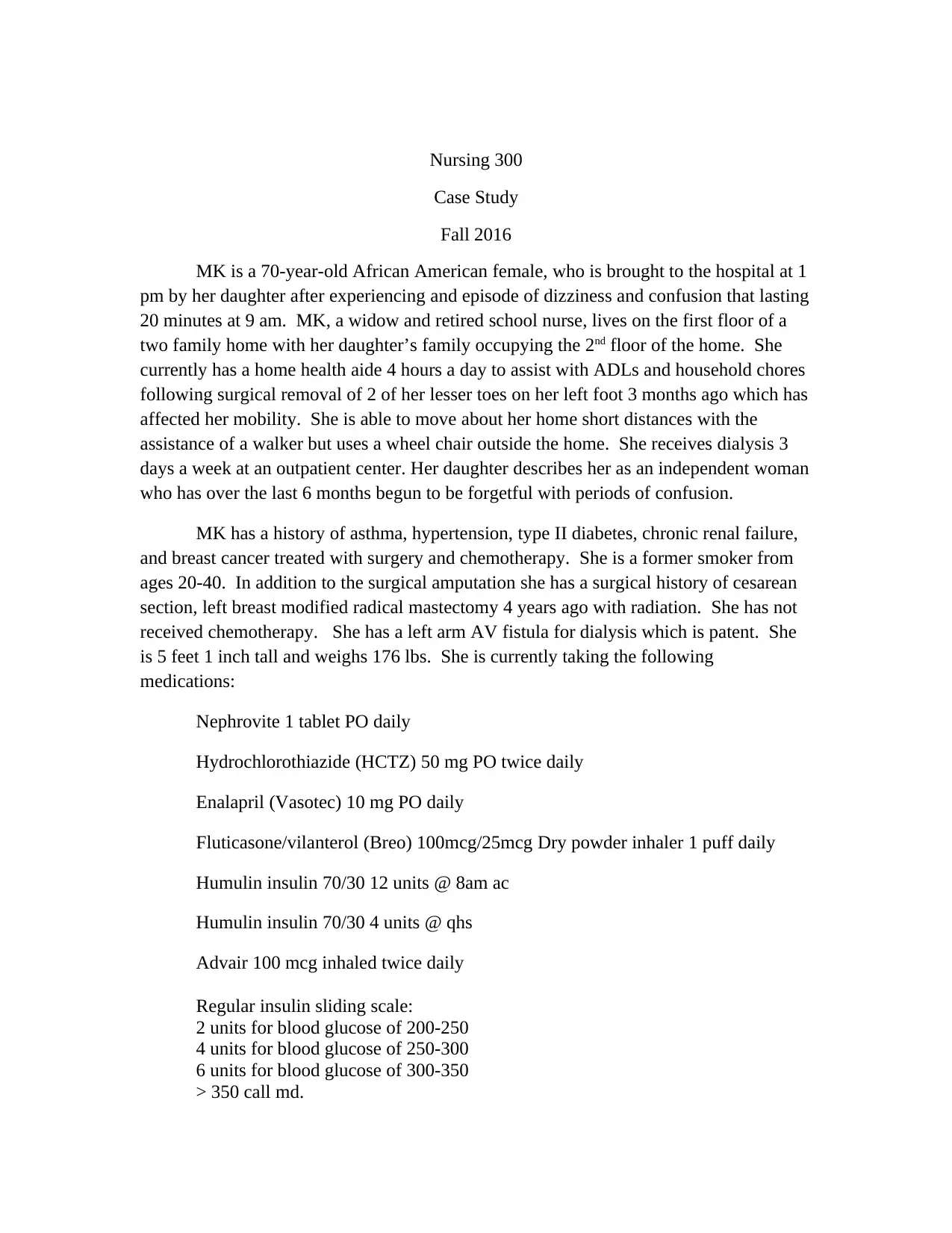
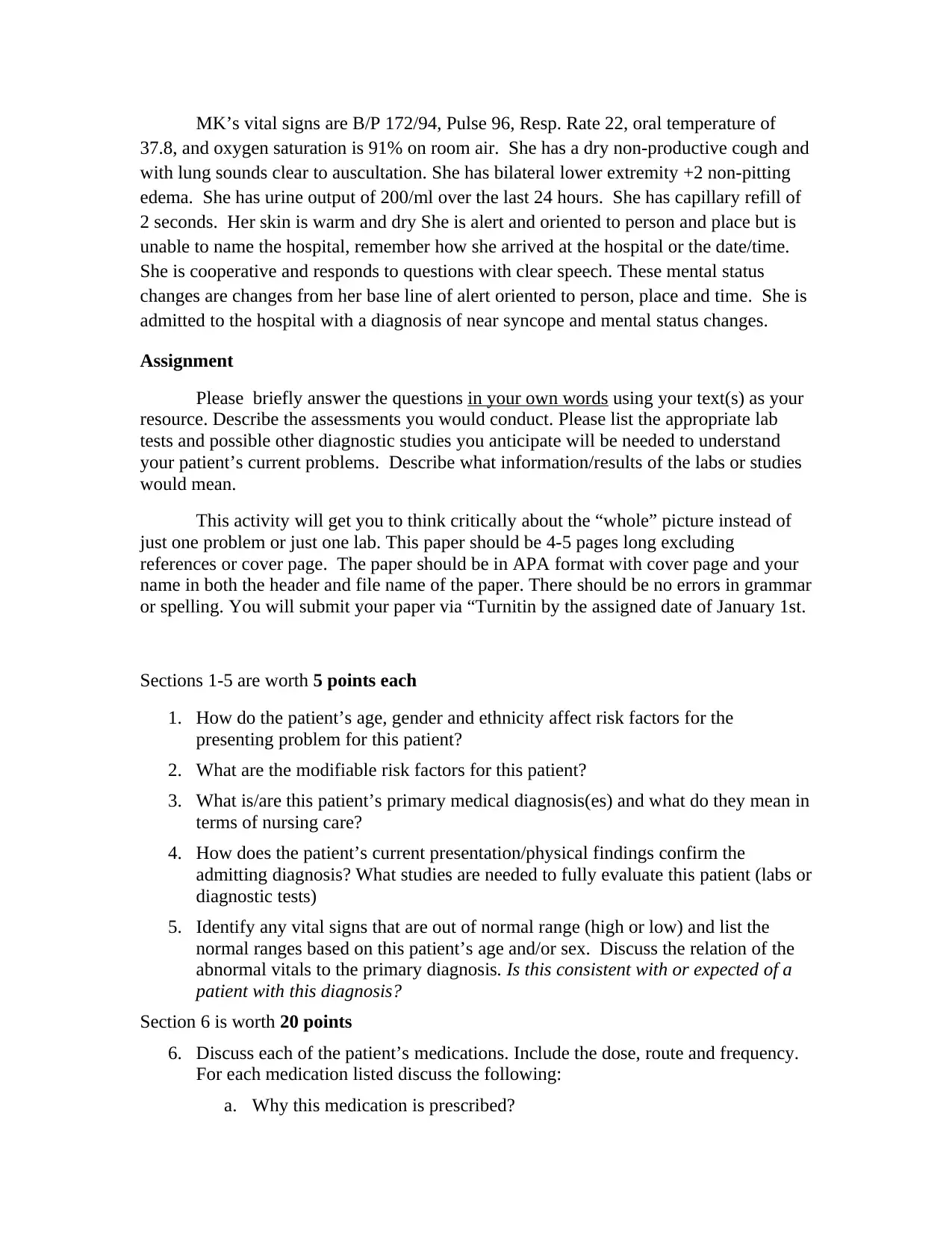
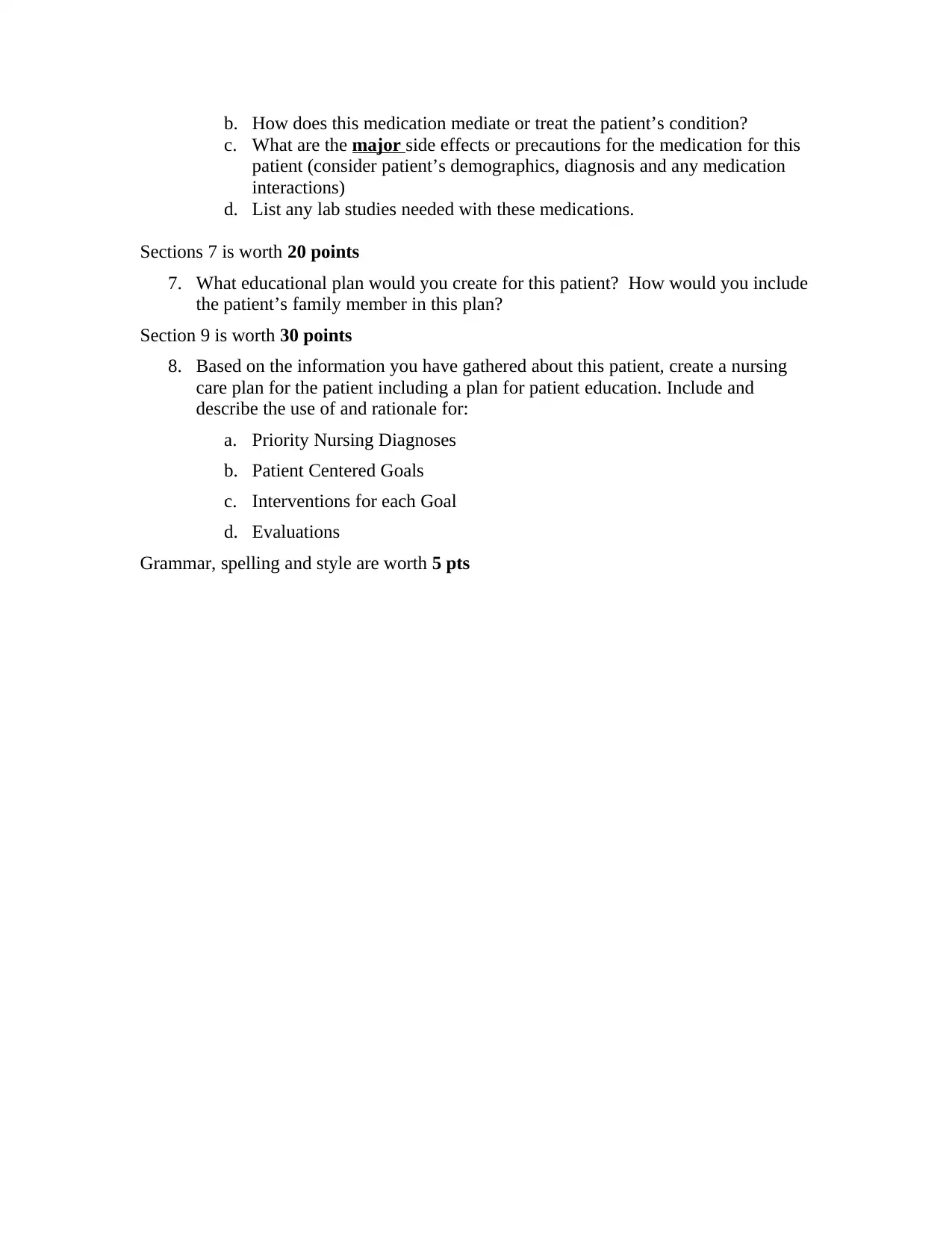
Nursing 300 Case Study Fall 2016
VerifiedAdded on 2019/09/16
|3
|992
|479
Case Study
AI Summary
This document presents a comprehensive case study of a 70-year-old African American female patient, MK, admitted to the hospital with near syncope and mental status changes. The assignment requires a detailed analysis of the patient's medical history, current medications, and vital signs. It includes questions on risk factors, primary diagnoses, and the relationship between physical findings and the admitting diagnosis. The assignment also requires a thorough medication review, an educational plan for the patient and family, and the creation of a nursing care plan with priority nursing diagnoses, patient-centered goals, interventions, and evaluations. The case study is designed to promote critical thinking and a holistic approach to patient care.
1 out of 3
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.