Compassionate Nursing Care: A Systematic Review - University 1
VerifiedAdded on 2023/06/12
|19
|4498
|85
Report
AI Summary
This report presents a systematic review of interventions aimed at enhancing compassionate nursing care. The review utilizes data from Medline, Cochrane Library, and CINAHL, focusing on terms like empathy, dignity, and patient-centered care. Studies were selected based on the Effective Workplace Culture Framework, assessing nurses' awareness of suffering, relational capacity, and actions to relieve suffering. The quality of included studies was graded as weak, medium, or strong, and data analysis involved qualitative methods to identify mechanisms and contexts for change. The findings categorize interventions into nurse support, care model-based, and staff training, highlighting the importance of factors such as time availability, nurse experience, and the work environment in delivering compassionate care. The report emphasizes the need for well-designed interventions and further research to strengthen compassionate care practices in nursing.

Compassionate Nursing Care 1
INTERVENTIONS FOR COMPASSIONATE NURSING CARE USING A
SYSETEMATIC REVIEW.
by
(name)
Course
Tutor
University
INTERVENTIONS FOR COMPASSIONATE NURSING CARE USING A
SYSETEMATIC REVIEW.
by
(name)
Course
Tutor
University
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Compassionate Nursing Care 2
1.0 Introduction
Nursing profession demands a practitioner to have a compassionate attitude towards their
clients (Francis, 2010). The department of health identified it as a high priority tow strengthen
deliverance of social care services that portrayed more compassionate care. Reviews into
qualitative research reports that it is a desire of a majority of the elderly people to receive warm
and humane connections established by nurses and other medical practitioners in a hospital
setting. They further stated that it would be of more comfort if the so said personnel developed a
personal touch with them especially in the wards. A four-month practical development program
was therefore formulated to under the heading “Creating Learning Environments for
Compassionate Care,” abbreviated as, CLECC. The program’s key aim is the promotion of
compassionate care to patients and patient oriented service by nurses. The study also targeted
ward leaders and their corresponding responsibilities and authority over nurses in attempt to
come up with the interventions applicable to improve compassionate care to patients (Craig et
al., 2013).
Targeted by the program also is the senior nurse, who plays a vital role in facilitating
initiatives aimed at promoting compassionate health care (Dewar, Nolan, 2013). Twice a week,
the chief nurse organized discussion with patients and other subordinate nurses so as to get a
clear understanding of the level of compassionate care that the patients were receiving. The
program involved daily rounds around all wards giving proper attention to all patients while at
the same time collecting views from the same patients about the kind of care that they were
receiving from the other nurses. Cases of complaints from patients who had received
uncompassionate care from any nurse were taken with deep seriousness and reported with
immediate effect to the senior nurse. Who was again very vigilant on such cases and
1.0 Introduction
Nursing profession demands a practitioner to have a compassionate attitude towards their
clients (Francis, 2010). The department of health identified it as a high priority tow strengthen
deliverance of social care services that portrayed more compassionate care. Reviews into
qualitative research reports that it is a desire of a majority of the elderly people to receive warm
and humane connections established by nurses and other medical practitioners in a hospital
setting. They further stated that it would be of more comfort if the so said personnel developed a
personal touch with them especially in the wards. A four-month practical development program
was therefore formulated to under the heading “Creating Learning Environments for
Compassionate Care,” abbreviated as, CLECC. The program’s key aim is the promotion of
compassionate care to patients and patient oriented service by nurses. The study also targeted
ward leaders and their corresponding responsibilities and authority over nurses in attempt to
come up with the interventions applicable to improve compassionate care to patients (Craig et
al., 2013).
Targeted by the program also is the senior nurse, who plays a vital role in facilitating
initiatives aimed at promoting compassionate health care (Dewar, Nolan, 2013). Twice a week,
the chief nurse organized discussion with patients and other subordinate nurses so as to get a
clear understanding of the level of compassionate care that the patients were receiving. The
program involved daily rounds around all wards giving proper attention to all patients while at
the same time collecting views from the same patients about the kind of care that they were
receiving from the other nurses. Cases of complaints from patients who had received
uncompassionate care from any nurse were taken with deep seriousness and reported with
immediate effect to the senior nurse. Who was again very vigilant on such cases and
Compassionate Nursing Care 3
apprehended any nurse reported with such behavior. The whole process was meant for
educational purposes and thus nurses with such behavior received adequate guidance for
transformational purposes.
2.0 Materials and methods
Various methods and materials were used throughout the whole program whereby, results
from various methods were compared and merged to obtain final results. The various factors that
influence compassion were the key drivers of the methods to be used in the study. Availability of
time is a key compelling factor towards provision of sufficient compassionate care by nurses to
patients (Dewar, Cook, 2014). It was observed that the more substantial amount of time was
availed to nurses while doing their routine rounds in the wards, the more time they had to spend
with patients. It was during such interactive moments that the patients got the chance to open up
and share their feelings with the nurse about their health conditions particularly pointing out
areas of improvement or deterioration. Patients pointed this as the most efficient move towards
improving compassionate care as they previously lacked anyone willing to dedicate enough time
to their situations. (Strada, 2018)
As more highly experienced nurses took turn in the ward, patients admitted that their
experience was directly attributable to the amount of compassionate care rendered to them. This
was a direct implication that the amount of clinical experience of the nurse is not the key
determinant of the amount of care that the nurse in question is capable of offering, the amount of
time that nurses undertook for acclimatizing is (Glembocki, Dunn, 2010). Nurses however
admitted that they were more often overwhelmed by the environment of work. Patients
commended majority of the elderly nurses who they deemed more experienced, for the amount
of compassionate care that they offered to them. They additionally pointed out that such nurses
apprehended any nurse reported with such behavior. The whole process was meant for
educational purposes and thus nurses with such behavior received adequate guidance for
transformational purposes.
2.0 Materials and methods
Various methods and materials were used throughout the whole program whereby, results
from various methods were compared and merged to obtain final results. The various factors that
influence compassion were the key drivers of the methods to be used in the study. Availability of
time is a key compelling factor towards provision of sufficient compassionate care by nurses to
patients (Dewar, Cook, 2014). It was observed that the more substantial amount of time was
availed to nurses while doing their routine rounds in the wards, the more time they had to spend
with patients. It was during such interactive moments that the patients got the chance to open up
and share their feelings with the nurse about their health conditions particularly pointing out
areas of improvement or deterioration. Patients pointed this as the most efficient move towards
improving compassionate care as they previously lacked anyone willing to dedicate enough time
to their situations. (Strada, 2018)
As more highly experienced nurses took turn in the ward, patients admitted that their
experience was directly attributable to the amount of compassionate care rendered to them. This
was a direct implication that the amount of clinical experience of the nurse is not the key
determinant of the amount of care that the nurse in question is capable of offering, the amount of
time that nurses undertook for acclimatizing is (Glembocki, Dunn, 2010). Nurses however
admitted that they were more often overwhelmed by the environment of work. Patients
commended majority of the elderly nurses who they deemed more experienced, for the amount
of compassionate care that they offered to them. They additionally pointed out that such nurses
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Compassionate Nursing Care 4
had dealt with a wide range of similar cases and thus knew how to handle them. Such nurses are
in addition considered to have already developed a personal touch with patients due to their
previous dealings.
2.1 search strategy.
Primary research for evaluation of compassionate care interventions was taken using a
systematic search that curtailed three databases which were; Medline, Cochrane library (included
is economic evaluation database, controlled trials central register, systematic reviews with
regards to Cochrane database, database of abstracts of reviews of effectiveness and the
assessment database of health technology cumulative index to nursing and allied health literature
(CINAHL) (Guyatt et al 2008). Terms used to relate to compassionate care however pose
numerous problems as there is no single agreed definition of the same. On the contrary a wide
range of terms are used inconsistently & interchangeably throughout the literature of healthcare.
While conducting the preliminary searches, the approach adopted to map the field was
inclusive and broad. Numerous terms in relation to compassionate care were pinpointed and
utilized while at the same time identifying a large number of studies that were related to one or
more of the key areas that have been mentioned above. It was through this mapping that chief
key words relevant to the area of study were identified (McCance, Slater & McCormack, 2009).
The key terms include; empathy, dignity, person-centered care, professional-patient relationship,
caring, relation-centered care and finally emotional intelligence (Dwan et al., 2013). It was also
the key words identifiable during the preliminary outsourcing that were used for final searches.
A combination of terms associable to compassion were merged with terms relating to
occupational groups and methods. (Chan and Altman, 2005)
had dealt with a wide range of similar cases and thus knew how to handle them. Such nurses are
in addition considered to have already developed a personal touch with patients due to their
previous dealings.
2.1 search strategy.
Primary research for evaluation of compassionate care interventions was taken using a
systematic search that curtailed three databases which were; Medline, Cochrane library (included
is economic evaluation database, controlled trials central register, systematic reviews with
regards to Cochrane database, database of abstracts of reviews of effectiveness and the
assessment database of health technology cumulative index to nursing and allied health literature
(CINAHL) (Guyatt et al 2008). Terms used to relate to compassionate care however pose
numerous problems as there is no single agreed definition of the same. On the contrary a wide
range of terms are used inconsistently & interchangeably throughout the literature of healthcare.
While conducting the preliminary searches, the approach adopted to map the field was
inclusive and broad. Numerous terms in relation to compassionate care were pinpointed and
utilized while at the same time identifying a large number of studies that were related to one or
more of the key areas that have been mentioned above. It was through this mapping that chief
key words relevant to the area of study were identified (McCance, Slater & McCormack, 2009).
The key terms include; empathy, dignity, person-centered care, professional-patient relationship,
caring, relation-centered care and finally emotional intelligence (Dwan et al., 2013). It was also
the key words identifiable during the preliminary outsourcing that were used for final searches.
A combination of terms associable to compassion were merged with terms relating to
occupational groups and methods. (Chan and Altman, 2005)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Compassionate Nursing Care 5
2.2 Selection
The framework that was used to guide in the selection was Effective Workplace Culture
Framework (Manley et al., 2011). Included were results from primary search that were aimed at
outcome comparison of the interventions that was designed to facilitate enhancement of nursing
care that was compassionate throughout any kind of setting and to clients in any particular group.
Designs that were eligible for selection were interrupted time series which could be either
controlled or uncontrolled before and after studies quasi random studies, or randomized
controlled trials which could again include cluster randomized trials. Exclusive student focused
studies were excluded out of such interventions as they were not directed towards behavioral
change of the nursing staff. (Nicholson, et al., 2010a)
Adopting a study that was inclusive in approach to areas that necessarily addressed
‘compassion’ was necessitated by deficit of conceptual clarity regarding comparison within the
literature (Cameron et al., 2013). The selection criteria developed was based on the four health
care compassion chief elements which are; nurses’ awareness of suffering and vulnerability,
actions of response aiming to relieve suffering while at the same time ensuring dignity, relational
capacity of nurses and empathy. Studies were included only if they met one or both of the
following criteria.
i. Preliminary outcomes assessing or evaluating quality of observed interaction or any other
compassion measure which could include responsive action and situational awareness,
and/or self-reports of nurses for compassion and /or their capacity and capability of
delivering compassionate care.
ii. Improving compassion in nursing care or a construct that is closely related i.e. relational
care, emotional care, and dignity as this was the primary and explicit goal of the
2.2 Selection
The framework that was used to guide in the selection was Effective Workplace Culture
Framework (Manley et al., 2011). Included were results from primary search that were aimed at
outcome comparison of the interventions that was designed to facilitate enhancement of nursing
care that was compassionate throughout any kind of setting and to clients in any particular group.
Designs that were eligible for selection were interrupted time series which could be either
controlled or uncontrolled before and after studies quasi random studies, or randomized
controlled trials which could again include cluster randomized trials. Exclusive student focused
studies were excluded out of such interventions as they were not directed towards behavioral
change of the nursing staff. (Nicholson, et al., 2010a)
Adopting a study that was inclusive in approach to areas that necessarily addressed
‘compassion’ was necessitated by deficit of conceptual clarity regarding comparison within the
literature (Cameron et al., 2013). The selection criteria developed was based on the four health
care compassion chief elements which are; nurses’ awareness of suffering and vulnerability,
actions of response aiming to relieve suffering while at the same time ensuring dignity, relational
capacity of nurses and empathy. Studies were included only if they met one or both of the
following criteria.
i. Preliminary outcomes assessing or evaluating quality of observed interaction or any other
compassion measure which could include responsive action and situational awareness,
and/or self-reports of nurses for compassion and /or their capacity and capability of
delivering compassionate care.
ii. Improving compassion in nursing care or a construct that is closely related i.e. relational
care, emotional care, and dignity as this was the primary and explicit goal of the
Compassionate Nursing Care 6
interventions. It could be achieved through addressing of nurses’ awareness of situation,
responsive action, moral attributes and relational capacity.
It was during the screening process that nurses met through frequent meetings to make
comparisons of independent selections formulate resolutions to disagreements and to top it all,
make decisions.
2.3 quality assessment
Attempt to represent the variation in quality of study as evidenced by results emanating
from the phase of initial mapping, and to again and inflict proper reflection on the strength of
evidence effectively, simple grading was undertaken in attempt to categorize strengths of points
of the retrieved underlying study designs. Weak, medium or strong ratings were assigned to
every study in regards of where the study design was based on the hierarchy of evidence for
effectiveness in tandem with an assessment of its design and execution (Greenhalgh, 2014;
Guyatt et al., 2008). Where there was explicit demonstration of equivalence between group
comparisons of treatment and control, such studies were ranked as top quality. Randomized
controlled trials (RCTs) and clusters randomized controlled trials were the study designs
involved and met the pre-mentioned conditions. (Chenoweth et al., 2014).
Medium rating was assigned where group equivalence was demonstrated through
comparisons between control and intervention groups but otherwise weakened by other issues of
methodology. Such issues included, limited sample size and groups allocation that were non-
random. Pre and post controlled studies using non-random allocation to groups and cluster
random controlled trials of small clusters were the designs used (Chenoweth et al., 2014). Low
quality ratings were assigned to other studies that were affected by significant methodological
interventions. It could be achieved through addressing of nurses’ awareness of situation,
responsive action, moral attributes and relational capacity.
It was during the screening process that nurses met through frequent meetings to make
comparisons of independent selections formulate resolutions to disagreements and to top it all,
make decisions.
2.3 quality assessment
Attempt to represent the variation in quality of study as evidenced by results emanating
from the phase of initial mapping, and to again and inflict proper reflection on the strength of
evidence effectively, simple grading was undertaken in attempt to categorize strengths of points
of the retrieved underlying study designs. Weak, medium or strong ratings were assigned to
every study in regards of where the study design was based on the hierarchy of evidence for
effectiveness in tandem with an assessment of its design and execution (Greenhalgh, 2014;
Guyatt et al., 2008). Where there was explicit demonstration of equivalence between group
comparisons of treatment and control, such studies were ranked as top quality. Randomized
controlled trials (RCTs) and clusters randomized controlled trials were the study designs
involved and met the pre-mentioned conditions. (Chenoweth et al., 2014).
Medium rating was assigned where group equivalence was demonstrated through
comparisons between control and intervention groups but otherwise weakened by other issues of
methodology. Such issues included, limited sample size and groups allocation that were non-
random. Pre and post controlled studies using non-random allocation to groups and cluster
random controlled trials of small clusters were the designs used (Chenoweth et al., 2014). Low
quality ratings were assigned to other studies that were affected by significant methodological
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Compassionate Nursing Care 7
shortcomings that weakened the possibility of demonstrating effectiveness. The pre-mentioned
quality assessments were conducted individually and merged with other ratings from other
nurses until there was attainment of consistent ratings. Each study was however analyzed using
the criteria of describing behavior change interventions that are group based as devised by Borek
et al. (2015).
2.4 data analysis
In order to pinpoint mechanisms, contexts and types of interventions necessary for
change, conducting a qualitative analysis was necessary through-out various interventions that
had been reported. The so said analysis was conducted through small groups and further on
enriched by discussing the process and emerging findings amongst all nurses. (Hall et al., 2009)
From each study, data was extracted and included outcomes and measurements, details
summarizing interventions sample and settings, study design and results. Results that had been
tabulated were used in generation of summary descriptions across all the key characteristics.
Studies that were heterogeneous in terms of methods, outcomes and interventions signified that a
more descriptive approach was merited as there was no warranting in meta-analysis (Brown et
al., 2013). It was through team discussions that the major types of outcomes and interventions
were agreed upon. Results on individual interventions and effectiveness were plotted against
chief types of outcomes and were used as the based on analysis of evaluating strategies through
types of interventions and evidence strength cutting across types of intervention and the nursing
field as a whole (Bridges et al., 2011). Recorded and tabulated were both group directional
differences wherever reported and the statistical significance of the reported differences.
shortcomings that weakened the possibility of demonstrating effectiveness. The pre-mentioned
quality assessments were conducted individually and merged with other ratings from other
nurses until there was attainment of consistent ratings. Each study was however analyzed using
the criteria of describing behavior change interventions that are group based as devised by Borek
et al. (2015).
2.4 data analysis
In order to pinpoint mechanisms, contexts and types of interventions necessary for
change, conducting a qualitative analysis was necessary through-out various interventions that
had been reported. The so said analysis was conducted through small groups and further on
enriched by discussing the process and emerging findings amongst all nurses. (Hall et al., 2009)
From each study, data was extracted and included outcomes and measurements, details
summarizing interventions sample and settings, study design and results. Results that had been
tabulated were used in generation of summary descriptions across all the key characteristics.
Studies that were heterogeneous in terms of methods, outcomes and interventions signified that a
more descriptive approach was merited as there was no warranting in meta-analysis (Brown et
al., 2013). It was through team discussions that the major types of outcomes and interventions
were agreed upon. Results on individual interventions and effectiveness were plotted against
chief types of outcomes and were used as the based on analysis of evaluating strategies through
types of interventions and evidence strength cutting across types of intervention and the nursing
field as a whole (Bridges et al., 2011). Recorded and tabulated were both group directional
differences wherever reported and the statistical significance of the reported differences.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Compassionate Nursing Care 8
3.0 Results
Presented are the review findings aimed at addressing each of the objectives of the
review. To begin with, a description of the study characteristics is done to portray an overview of
the studies that are used in evaluating interventions for compassionate care (McCormack B, et
al., 2010). Secondly is a presentation on evaluation of reporting interventions quality as
highlighted in the included studies with inclusion of foundations of their theoretical (Greenhalgh,
2014). Following will be a presentation on the evidence effectiveness of the interventions of the
studies and an analysis of quality of the evidence.
3.1 Study characteristics
The ultimate set of data was resolved to after twenty-four studies and comprised of 25
interventions. The types of interventions that were identified were three. Nurse support
interventions focused on appraisal of the nursing support staff and their wellbeing (Hartrick,
1997) which could be actualized through providing clinical supervision. Intervention based on
care model focused on introducing new care models to a service and could include person-
centered care. The third type of intervention was based on staff training and its main focus was
on developing new and knowledge skills amongst nursing including offering a training course in
communication and skills on empathy. (Nicholson, et al., 2010b)
Summary of findings, study design features and study characteristics reflected a wide
range of study setting that included care/nursing homes, hospital and the wider community.
(Higgins, Green, 2011). Apart from one, all the other studies on staff training were conducted in
a hospital setting. Out of eight interventions on care model, six of them were conducted in care
homes settings. studies based on nurse support interventions were conducted on outpatient
3.0 Results
Presented are the review findings aimed at addressing each of the objectives of the
review. To begin with, a description of the study characteristics is done to portray an overview of
the studies that are used in evaluating interventions for compassionate care (McCormack B, et
al., 2010). Secondly is a presentation on evaluation of reporting interventions quality as
highlighted in the included studies with inclusion of foundations of their theoretical (Greenhalgh,
2014). Following will be a presentation on the evidence effectiveness of the interventions of the
studies and an analysis of quality of the evidence.
3.1 Study characteristics
The ultimate set of data was resolved to after twenty-four studies and comprised of 25
interventions. The types of interventions that were identified were three. Nurse support
interventions focused on appraisal of the nursing support staff and their wellbeing (Hartrick,
1997) which could be actualized through providing clinical supervision. Intervention based on
care model focused on introducing new care models to a service and could include person-
centered care. The third type of intervention was based on staff training and its main focus was
on developing new and knowledge skills amongst nursing including offering a training course in
communication and skills on empathy. (Nicholson, et al., 2010b)
Summary of findings, study design features and study characteristics reflected a wide
range of study setting that included care/nursing homes, hospital and the wider community.
(Higgins, Green, 2011). Apart from one, all the other studies on staff training were conducted in
a hospital setting. Out of eight interventions on care model, six of them were conducted in care
homes settings. studies based on nurse support interventions were conducted on outpatient
Compassionate Nursing Care 9
oncology service, hospice at home, hospital settings and district nursing services. Study
participants were nurse managers, relatives, patients and nurses themselves.
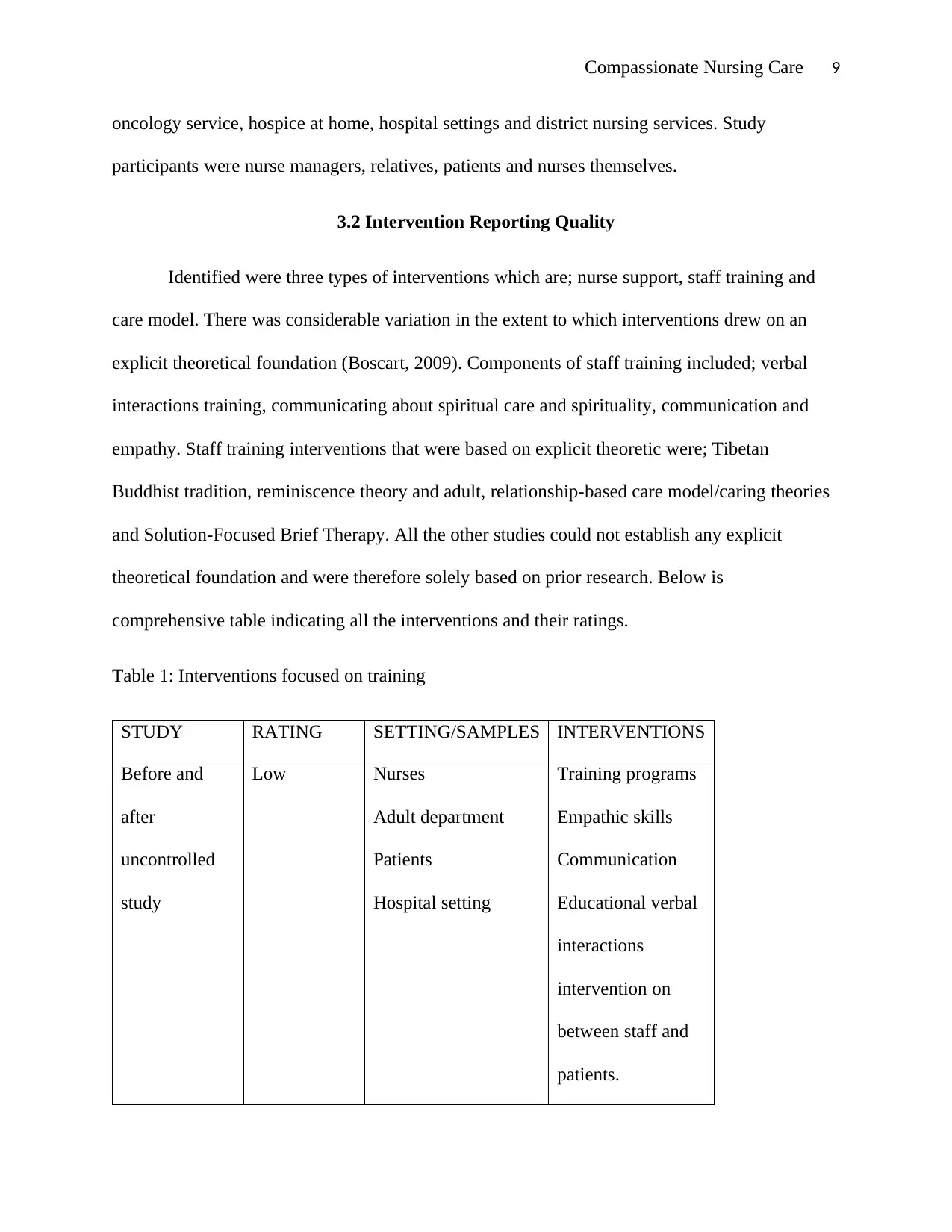
3.2 Intervention Reporting Quality
Identified were three types of interventions which are; nurse support, staff training and
care model. There was considerable variation in the extent to which interventions drew on an
explicit theoretical foundation (Boscart, 2009). Components of staff training included; verbal
interactions training, communicating about spiritual care and spirituality, communication and
empathy. Staff training interventions that were based on explicit theoretic were; Tibetan
Buddhist tradition, reminiscence theory and adult, relationship-based care model/caring theories
and Solution-Focused Brief Therapy. All the other studies could not establish any explicit
theoretical foundation and were therefore solely based on prior research. Below is
comprehensive table indicating all the interventions and their ratings.
Table 1: Interventions focused on training
STUDY RATING SETTING/SAMPLES INTERVENTIONS
Before and
after
uncontrolled
study
Low Nurses
Adult department
Patients
Hospital setting
Training programs
Empathic skills
Communication
Educational verbal
interactions
intervention on
between staff and
patients.
oncology service, hospice at home, hospital settings and district nursing services. Study
participants were nurse managers, relatives, patients and nurses themselves.
3.2 Intervention Reporting Quality
Identified were three types of interventions which are; nurse support, staff training and
care model. There was considerable variation in the extent to which interventions drew on an
explicit theoretical foundation (Boscart, 2009). Components of staff training included; verbal
interactions training, communicating about spiritual care and spirituality, communication and
empathy. Staff training interventions that were based on explicit theoretic were; Tibetan
Buddhist tradition, reminiscence theory and adult, relationship-based care model/caring theories
and Solution-Focused Brief Therapy. All the other studies could not establish any explicit
theoretical foundation and were therefore solely based on prior research. Below is
comprehensive table indicating all the interventions and their ratings.
Table 1: Interventions focused on training
STUDY RATING SETTING/SAMPLES INTERVENTIONS
Before and
after
uncontrolled
study
Low Nurses
Adult department
Patients
Hospital setting
Training programs
Empathic skills
Communication
Educational verbal
interactions
intervention on
between staff and
patients.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Compassionate Nursing Care 10
Workshop based
communication
skills training
Cluster
randomized
controlled
study
Medium Nurses
Patients
Hospital setting
A course in
physical
assessment
Empathy training
program
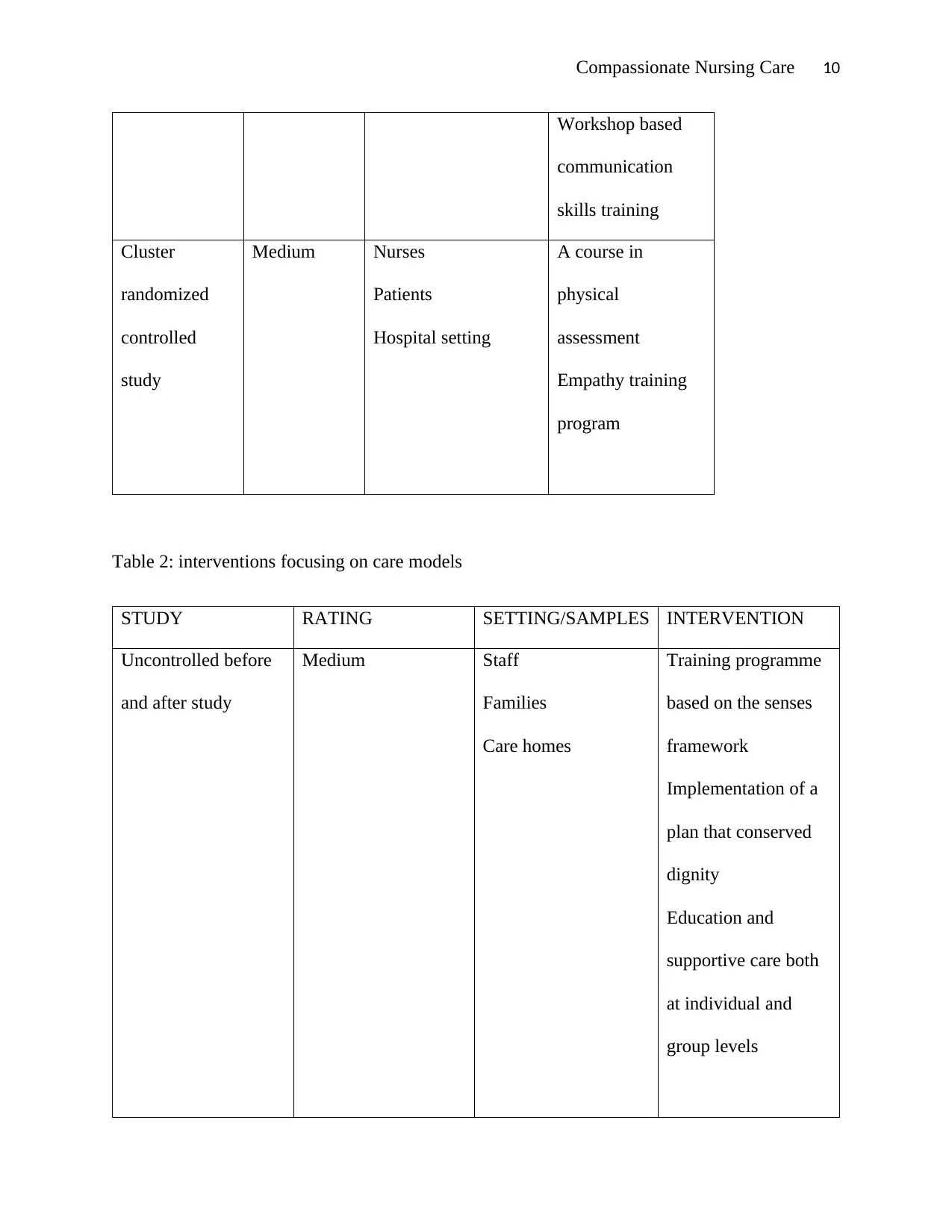
Table 2: interventions focusing on care models
STUDY RATING SETTING/SAMPLES INTERVENTION
Uncontrolled before
and after study
Medium Staff
Families
Care homes
Training programme
based on the senses
framework
Implementation of a
plan that conserved
dignity
Education and
supportive care both
at individual and
group levels
Workshop based
communication
skills training
Cluster
randomized
controlled
study
Medium Nurses
Patients
Hospital setting
A course in
physical
assessment
Empathy training
program
Table 2: interventions focusing on care models
STUDY RATING SETTING/SAMPLES INTERVENTION
Uncontrolled before
and after study
Medium Staff
Families
Care homes
Training programme
based on the senses
framework
Implementation of a
plan that conserved
dignity
Education and
supportive care both
at individual and
group levels
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
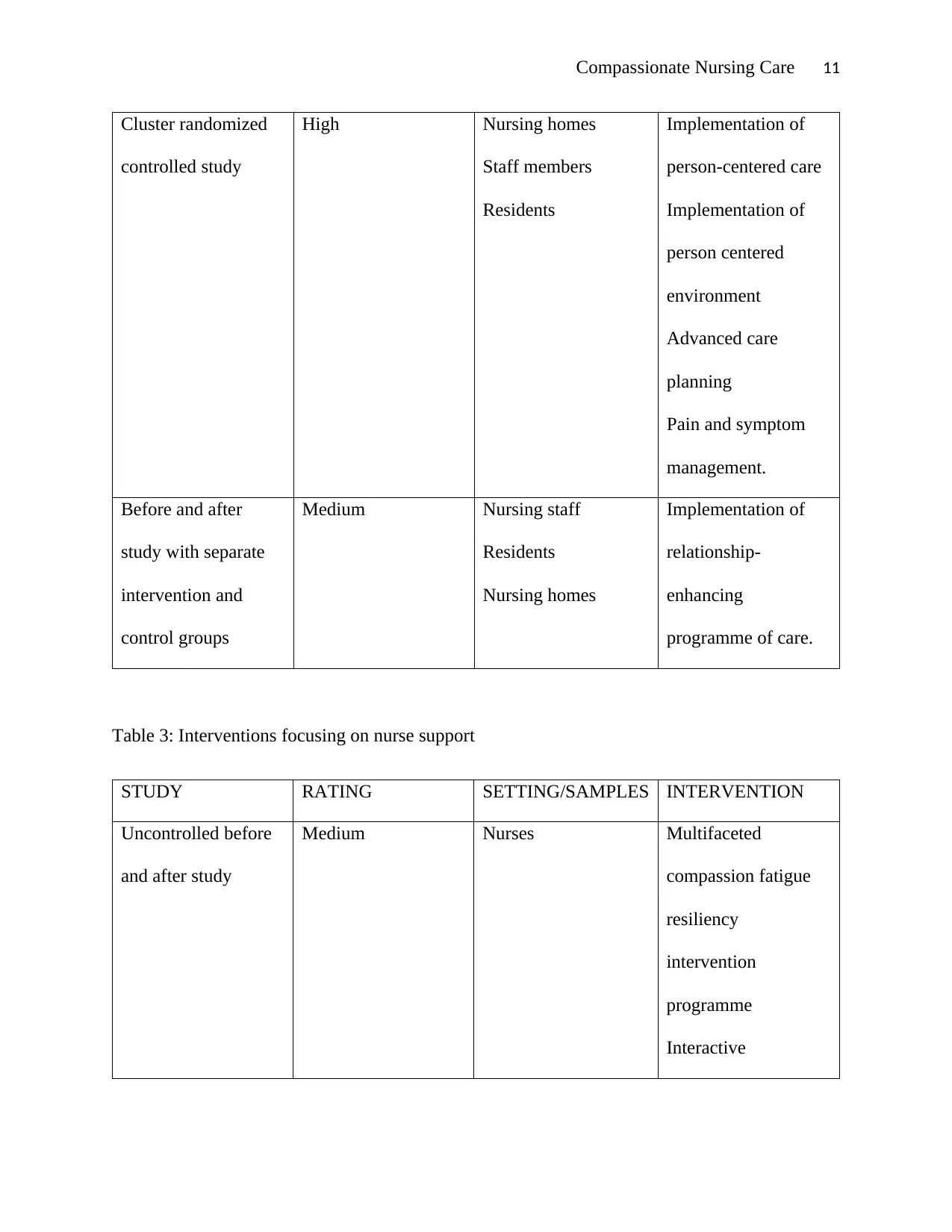
Compassionate Nursing Care 11
Cluster randomized
controlled study
High Nursing homes
Staff members
Residents
Implementation of
person-centered care
Implementation of
person centered
environment
Advanced care
planning
Pain and symptom
management.
Before and after
study with separate
intervention and
control groups
Medium Nursing staff
Residents
Nursing homes
Implementation of
relationship-
enhancing
programme of care.
Table 3: Interventions focusing on nurse support
STUDY RATING SETTING/SAMPLES INTERVENTION
Uncontrolled before
and after study
Medium Nurses Multifaceted
compassion fatigue
resiliency
intervention
programme
Interactive
Cluster randomized
controlled study
High Nursing homes
Staff members
Residents
Implementation of
person-centered care
Implementation of
person centered
environment
Advanced care
planning
Pain and symptom
management.
Before and after
study with separate
intervention and
control groups
Medium Nursing staff
Residents
Nursing homes
Implementation of
relationship-
enhancing
programme of care.
Table 3: Interventions focusing on nurse support
STUDY RATING SETTING/SAMPLES INTERVENTION
Uncontrolled before
and after study
Medium Nurses Multifaceted
compassion fatigue
resiliency
intervention
programme
Interactive
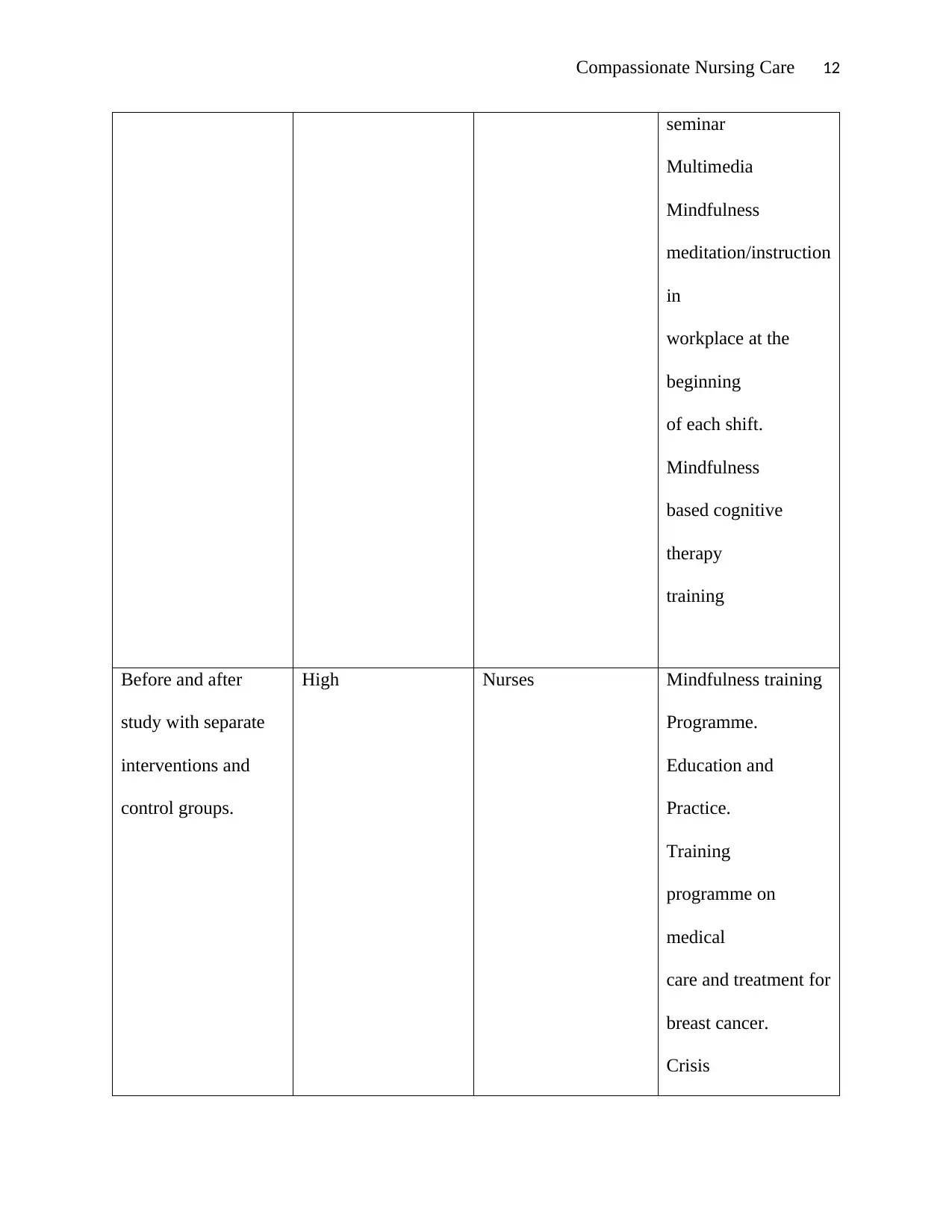
Compassionate Nursing Care 12
seminar
Multimedia
Mindfulness
meditation/instruction
in
workplace at the
beginning
of each shift.
Mindfulness
based cognitive
therapy
training
Before and after
study with separate
interventions and
control groups.
High Nurses Mindfulness training
Programme.
Education and
Practice.
Training
programme on
medical
care and treatment for
breast cancer.
Crisis
seminar
Multimedia
Mindfulness
meditation/instruction
in
workplace at the
beginning
of each shift.
Mindfulness
based cognitive
therapy
training
Before and after
study with separate
interventions and
control groups.
High Nurses Mindfulness training
Programme.
Education and
Practice.
Training
programme on
medical
care and treatment for
breast cancer.
Crisis
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 19
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.