Nursing Medical Forms Report: Analysis of Patient Documentation
VerifiedAdded on 2022/09/02
|35
|7937
|27
Report
AI Summary
This report provides a detailed analysis of various nursing medical forms, including letters to clinics, dictation forms, Holter reports, discharge summaries, and consultation forms related to cardiology and other medical specialties. The report examines forms from different chapters, each containing specific patient information, medical histories, and treatment plans. The forms cover diverse patient cases, detailing symptoms, diagnoses, medications, and follow-up instructions. The report highlights key aspects of each form, such as patient demographics, chief complaints, past medical history, physical examination findings, laboratory data, and treatment plans. It also includes operative reports and consultation notes, offering a comprehensive overview of patient care documentation within a healthcare setting. The report is a valuable resource for understanding the structure, content, and purpose of medical forms used in nursing practice and patient care.

Running head: NURSING
MEDICAL FORM
Name of the Student
Name of the University
Author Note
MEDICAL FORM
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1NURSING
Table of Contents
Chapter 2....................................................................................................................................2
Form 1: Letter to Memorial Clinic.........................................................................................2
Form 2: Dictating form..........................................................................................................4
Form 3: Holter........................................................................................................................7
Form 4: Discharge summary..................................................................................................8
Form 5- Cardiac surgery consult..........................................................................................12
Chapter 3..................................................................................................................................16
Form 1- Consultation...........................................................................................................16
Form 2- Operative report.....................................................................................................18
Form 3- Merwin Letter to Memorial Clinic.........................................................................19
Form 4- Infectious diseases consult.....................................................................................20
Form 5- Consultation form...................................................................................................21
Chapter 4..................................................................................................................................27
Form 1: HRP........................................................................................................................27
Form 2- CT report................................................................................................................29
Form 3..................................................................................................................................30
Form 4..................................................................................................................................31
Form 5- Operative report.....................................................................................................32
Table of Contents
Chapter 2....................................................................................................................................2
Form 1: Letter to Memorial Clinic.........................................................................................2
Form 2: Dictating form..........................................................................................................4
Form 3: Holter........................................................................................................................7
Form 4: Discharge summary..................................................................................................8
Form 5- Cardiac surgery consult..........................................................................................12
Chapter 3..................................................................................................................................16
Form 1- Consultation...........................................................................................................16
Form 2- Operative report.....................................................................................................18
Form 3- Merwin Letter to Memorial Clinic.........................................................................19
Form 4- Infectious diseases consult.....................................................................................20
Form 5- Consultation form...................................................................................................21
Chapter 4..................................................................................................................................27
Form 1: HRP........................................................................................................................27
Form 2- CT report................................................................................................................29
Form 3..................................................................................................................................30
Form 4..................................................................................................................................31
Form 5- Operative report.....................................................................................................32
2NURSING
Chapter 2
Form 1: Letter to Memorial Clinic
Dictated by: Jennifer Hector
Attention to: Anderson Phips (MD)/ Family Medicine/ Geriatrics
Address: 6249 Brock Street Lebanon 37106
Date: December 17
Patient name: Julia Paternoster
Date of birth: 3/8
Dear doctor Phips,
I saw your patient Julia Paternoster. As you know, Julia is a 70 year old female who had an
episode of palpitation approximately five days prior to this consultation. She went to the
emergency room and was diagnosed with paroxysmal atrial fibrillation. She was sent to the
emergency room and then aspirin was added later on by me. She states that she gets
occasional non:erosional gas pains in her chest. She also has dyspnea on exhaustion after
climbing one flight of stairs. She denies any PMD. She does have chronic edema or a chronic
anemia. She denies any dizziness or any syncope. The risk factor for coronary artery disease
include hypertension, diabetes, hypercholesterolemia, cigarette smoking until 20 years ago
and a positive family history. The past medical history is remarkable for us now. She drinks
occasional alcohol.
She is allergic to sofa embaetrin.
Patients medication at present includes fosomex 70 mg weekly, advene 250 1 puff BID,
Octose, Zeroxilin 2.5 mgpo daily and aspirin 325 mgpo daily.
Chapter 2
Form 1: Letter to Memorial Clinic
Dictated by: Jennifer Hector
Attention to: Anderson Phips (MD)/ Family Medicine/ Geriatrics
Address: 6249 Brock Street Lebanon 37106
Date: December 17
Patient name: Julia Paternoster
Date of birth: 3/8
Dear doctor Phips,
I saw your patient Julia Paternoster. As you know, Julia is a 70 year old female who had an
episode of palpitation approximately five days prior to this consultation. She went to the
emergency room and was diagnosed with paroxysmal atrial fibrillation. She was sent to the
emergency room and then aspirin was added later on by me. She states that she gets
occasional non:erosional gas pains in her chest. She also has dyspnea on exhaustion after
climbing one flight of stairs. She denies any PMD. She does have chronic edema or a chronic
anemia. She denies any dizziness or any syncope. The risk factor for coronary artery disease
include hypertension, diabetes, hypercholesterolemia, cigarette smoking until 20 years ago
and a positive family history. The past medical history is remarkable for us now. She drinks
occasional alcohol.
She is allergic to sofa embaetrin.
Patients medication at present includes fosomex 70 mg weekly, advene 250 1 puff BID,
Octose, Zeroxilin 2.5 mgpo daily and aspirin 325 mgpo daily.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3NURSING
On physical examination in my office, patient had a blood pressure of 150 to over 70 on a
regular pulse of 65. She had 1 to 2 centimeter juggler lenus distention at 90 degrees. She had
a right carotid bruit, she had a few scattered bronchi and tweezes bilaterally. She had normal
first and second heart sounds and there were no murmurs. Abdomen was benign with active
bowel sounds. There was no organomegaly, there was 1+ edema bilaterally. Her
electrocardiogram demonstrated a sinus bradycardia with right bundle branch block. Because
of this episode of probable paroxysmal atrial fibrillation and her shortness of breath, I have
scheduled Julia for an echocardiogram. At this point I have not changed any medications, so
that she gets better control of her blood pressure. In addition, because of the right carotid
bruit, we will need a carotid ultrasound which I will schedule several weeks down the line.
Once I have further evaluated her paroxysmal atrial fibrillation, she will also require a stress
echocardiogram to rule out esquemea as a cause of her dyspnea on exertion. She has multiple
risk factors and would be at high risk for coronary artery disease. I will send you the results
of the tests when they are completed. Thank you very much for allowing me to participate in
the care of your patient.
Jennifer Hector
Cardiology
On physical examination in my office, patient had a blood pressure of 150 to over 70 on a
regular pulse of 65. She had 1 to 2 centimeter juggler lenus distention at 90 degrees. She had
a right carotid bruit, she had a few scattered bronchi and tweezes bilaterally. She had normal
first and second heart sounds and there were no murmurs. Abdomen was benign with active
bowel sounds. There was no organomegaly, there was 1+ edema bilaterally. Her
electrocardiogram demonstrated a sinus bradycardia with right bundle branch block. Because
of this episode of probable paroxysmal atrial fibrillation and her shortness of breath, I have
scheduled Julia for an echocardiogram. At this point I have not changed any medications, so
that she gets better control of her blood pressure. In addition, because of the right carotid
bruit, we will need a carotid ultrasound which I will schedule several weeks down the line.
Once I have further evaluated her paroxysmal atrial fibrillation, she will also require a stress
echocardiogram to rule out esquemea as a cause of her dyspnea on exertion. She has multiple
risk factors and would be at high risk for coronary artery disease. I will send you the results
of the tests when they are completed. Thank you very much for allowing me to participate in
the care of your patient.
Jennifer Hector
Cardiology
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4NURSING
Form 2: Dictating form
Dictated by: Tony Jackson
Patient name: Kramer Curmamery
Physician in charge: Anderson Phips, MD
Date of admission: May 13
Sex: Female
Age: 80
Date of birth: 1st February
Generic physician: Myself
Patient ID: 000123
Chief complain: Shortness of breath and palpitation periods
History of present ailments: 80 years old black female with CHF and atrial fibrillation, 3
weeks ago started to notice dyspnea. She went to see a cardiologist. During the last week she
has been experiencing palpitation associated with exertion dyspnea which has been getting
worse, paroxysmal dyspnea period. This patient denies any cough. She denies any abdominal
pain, nausea, vomiting or diarrhea period. She denies any fever, chills, recent travel, or recent
immobilization period. She denies any urinary symptoms period. She presented to the
cardiologist’s office today, and was diagnosed with an atrial fibrillation with rapid ventricular
responses and was sent to the hospital for directed machine cure.
Past medical history:
1. Peroxysmal atrial fibrillation
Form 2: Dictating form
Dictated by: Tony Jackson
Patient name: Kramer Curmamery
Physician in charge: Anderson Phips, MD
Date of admission: May 13
Sex: Female
Age: 80
Date of birth: 1st February
Generic physician: Myself
Patient ID: 000123
Chief complain: Shortness of breath and palpitation periods
History of present ailments: 80 years old black female with CHF and atrial fibrillation, 3
weeks ago started to notice dyspnea. She went to see a cardiologist. During the last week she
has been experiencing palpitation associated with exertion dyspnea which has been getting
worse, paroxysmal dyspnea period. This patient denies any cough. She denies any abdominal
pain, nausea, vomiting or diarrhea period. She denies any fever, chills, recent travel, or recent
immobilization period. She denies any urinary symptoms period. She presented to the
cardiologist’s office today, and was diagnosed with an atrial fibrillation with rapid ventricular
responses and was sent to the hospital for directed machine cure.
Past medical history:
1. Peroxysmal atrial fibrillation
5NURSING
2. Dyspnea period
3. Chronic diastolic heart failure
4. Hepatitis C
5. Osteoarthritis period
6. Non insulin dependent diabetes
Allergies: Codi that causes vermin
Medications:
1. Ptanol 100 mg PODAILY
2. Lasix 40 mg PODAILY
3. Spironolactone 50 mg PODAILY
4. Predexa 150 mg poBID
5. Clickpazide 2.5 mg PODAILY
6. Lipitoir 10 mg PODAILY
7. Alopurinol 100 mg PODAILY
Social History: A widdle, the patient is independent in her activities daily living period. Her
daughter is LNW. The patient does not drink and does not smoke. Her husband smoked
heavily however.
Family History: The patient was adopted and does not know her family history.
Review of systems: Positive for those mentioned in the history of ailments, otherwise
negative.
2. Dyspnea period
3. Chronic diastolic heart failure
4. Hepatitis C
5. Osteoarthritis period
6. Non insulin dependent diabetes
Allergies: Codi that causes vermin
Medications:
1. Ptanol 100 mg PODAILY
2. Lasix 40 mg PODAILY
3. Spironolactone 50 mg PODAILY
4. Predexa 150 mg poBID
5. Clickpazide 2.5 mg PODAILY
6. Lipitoir 10 mg PODAILY
7. Alopurinol 100 mg PODAILY
Social History: A widdle, the patient is independent in her activities daily living period. Her
daughter is LNW. The patient does not drink and does not smoke. Her husband smoked
heavily however.
Family History: The patient was adopted and does not know her family history.
Review of systems: Positive for those mentioned in the history of ailments, otherwise
negative.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6NURSING
Physical examination: General Colin, this is an elderly black lady in no acute distress period
vital signs following blood pressure a 130 over 80, respiratory 20 with 96% in room air,
temperature 97.4. Each EENT head normal cephalic a traumatic and reactive to light
extraocular movements intact, moist. Neck supple, no lymphanopathy no respiratory periods.
Normal respiratory periods. No murmurs, no gallops, no rubs. GI soft abdomen, normal
active bowel sounds. Non intended and non distended period. No sinuses no erythema period.
No lower exterminatory edema period. Alerted and oriented to times. No focal deficits cranial
nerves mostly intact.
Laboratory data: CBC shows normal wbc, hemoglobin and platelet count normal. Sodium
132, Bicarbonate 121, EON of 80, creatinine of 2.25, glucose of 111. TNI of 0.03. Chest X
ray shows no abnormalities, EEG shows atrial fibrillation with rapid ventricular response
with a heart rate of 130 no qst changes.
Impression: This is an 80 year old black lady with a history of atrial fibrillation and
congestive diastolic heart failure who presented to the FORS general medical center with the
following periods.
1. Dyspnea, atrial fibrillation with rapid ventricular response, doubt acute heart failure, given
no signs of congestive heart failure and blood record is associated with valium depletion,
secondary to diuresis period.
2. Chronic diastolic heart failure period.
3. Acute renal failure, pre renal secondary valium depletion period.
4. Valium depletion likely to be induced by diuresis period.
5. Type II diabetes mellitus period, hypertension.
Plan:
Physical examination: General Colin, this is an elderly black lady in no acute distress period
vital signs following blood pressure a 130 over 80, respiratory 20 with 96% in room air,
temperature 97.4. Each EENT head normal cephalic a traumatic and reactive to light
extraocular movements intact, moist. Neck supple, no lymphanopathy no respiratory periods.
Normal respiratory periods. No murmurs, no gallops, no rubs. GI soft abdomen, normal
active bowel sounds. Non intended and non distended period. No sinuses no erythema period.
No lower exterminatory edema period. Alerted and oriented to times. No focal deficits cranial
nerves mostly intact.
Laboratory data: CBC shows normal wbc, hemoglobin and platelet count normal. Sodium
132, Bicarbonate 121, EON of 80, creatinine of 2.25, glucose of 111. TNI of 0.03. Chest X
ray shows no abnormalities, EEG shows atrial fibrillation with rapid ventricular response
with a heart rate of 130 no qst changes.
Impression: This is an 80 year old black lady with a history of atrial fibrillation and
congestive diastolic heart failure who presented to the FORS general medical center with the
following periods.
1. Dyspnea, atrial fibrillation with rapid ventricular response, doubt acute heart failure, given
no signs of congestive heart failure and blood record is associated with valium depletion,
secondary to diuresis period.
2. Chronic diastolic heart failure period.
3. Acute renal failure, pre renal secondary valium depletion period.
4. Valium depletion likely to be induced by diuresis period.
5. Type II diabetes mellitus period, hypertension.
Plan:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7NURSING
1. Admin to medicine
2. Starting 1800 calorie American Diabetes Association Diet
3. No Lasix or spironolactone
4. Daily weights
5. Restricted inputs and outputs to be recorded.
6. SMA 6 in the morning testing specimen
7. 50 mg medicine every six hours
8. Continue home medications.
9. Ending period
10. Notify pulmonary medicine period
11. Notify your PCP, Dr. Phips
This is Tony Jackson, ending dictation.
Form 3: Holter
Dictated by: Tony Jackson
Patient name: Kramer Curmamery
Following physician: Tony Jackson
Date of exam: May 13
Sex: Female
Age: 80
Date of birth: February 1st
1. Admin to medicine
2. Starting 1800 calorie American Diabetes Association Diet
3. No Lasix or spironolactone
4. Daily weights
5. Restricted inputs and outputs to be recorded.
6. SMA 6 in the morning testing specimen
7. 50 mg medicine every six hours
8. Continue home medications.
9. Ending period
10. Notify pulmonary medicine period
11. Notify your PCP, Dr. Phips
This is Tony Jackson, ending dictation.
Form 3: Holter
Dictated by: Tony Jackson
Patient name: Kramer Curmamery
Following physician: Tony Jackson
Date of exam: May 13
Sex: Female
Age: 80
Date of birth: February 1st
8NURSING
Patient ID: 000123
Indications from monitoring: Symptoms suspected of cardiac blockage suppressed by light
headedness.
Cardiac diagnosis: Atrial fibrillation
Relevant medical history: Hypercholesterolemia, hypertension
Cardiac medications: Clipaside, Prodexa, Lowpresso, Lasix, Lippitoir
Report: Electrocardiogram was recorded for 24 hours during normal activities. This was
done as per variation of atrial fibrillation. She takes lowpresso 50 mg twice a day and carticin
240 mg twice a day.
The rhythm was atrial fibrillation with a rate varying between 46 and 128 bpm. The
average rate was 77 bpm. The slowest rate occurred at 14:44 am. The longest R:R interval
was 2 second at 2:47 am.
68 ventricular atopic beats, with all single period, no symptoms recorded in the diary.
Summary: The rhythm is atrial fibrillation with low controlled ventricular response rate.
There are small numbers of ventricular atopic beats, which were all single. Please copy
Anderson Phips family medicine geriatrics Philips Chaff Nephrology.
This is Tony Jackson end of dictation.
Form 4: Discharge summary
Dictated by: Tony Jackson
Patient name: Kramer Curmamery
Following physician: Tony Jackson
Patient ID: 000123
Indications from monitoring: Symptoms suspected of cardiac blockage suppressed by light
headedness.
Cardiac diagnosis: Atrial fibrillation
Relevant medical history: Hypercholesterolemia, hypertension
Cardiac medications: Clipaside, Prodexa, Lowpresso, Lasix, Lippitoir
Report: Electrocardiogram was recorded for 24 hours during normal activities. This was
done as per variation of atrial fibrillation. She takes lowpresso 50 mg twice a day and carticin
240 mg twice a day.
The rhythm was atrial fibrillation with a rate varying between 46 and 128 bpm. The
average rate was 77 bpm. The slowest rate occurred at 14:44 am. The longest R:R interval
was 2 second at 2:47 am.
68 ventricular atopic beats, with all single period, no symptoms recorded in the diary.
Summary: The rhythm is atrial fibrillation with low controlled ventricular response rate.
There are small numbers of ventricular atopic beats, which were all single. Please copy
Anderson Phips family medicine geriatrics Philips Chaff Nephrology.
This is Tony Jackson end of dictation.
Form 4: Discharge summary
Dictated by: Tony Jackson
Patient name: Kramer Curmamery
Following physician: Tony Jackson
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9NURSING
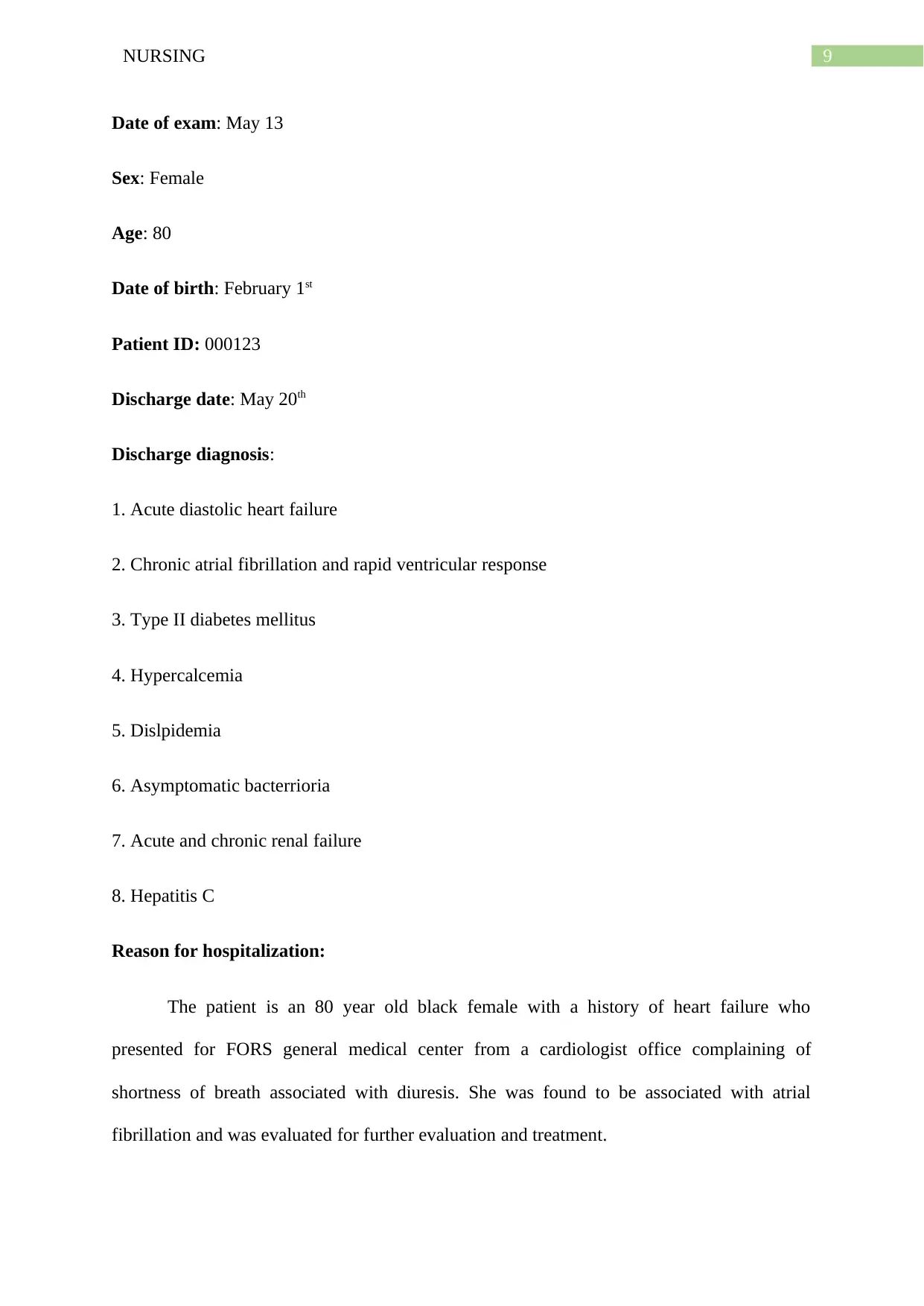
Date of exam: May 13
Sex: Female
Age: 80
Date of birth: February 1st
Patient ID: 000123
Discharge date: May 20th
Discharge diagnosis:
1. Acute diastolic heart failure
2. Chronic atrial fibrillation and rapid ventricular response
3. Type II diabetes mellitus
4. Hypercalcemia
5. Dislpidemia
6. Asymptomatic bacterrioria
7. Acute and chronic renal failure
8. Hepatitis C
Reason for hospitalization:
The patient is an 80 year old black female with a history of heart failure who
presented for FORS general medical center from a cardiologist office complaining of
shortness of breath associated with diuresis. She was found to be associated with atrial
fibrillation and was evaluated for further evaluation and treatment.
Date of exam: May 13
Sex: Female
Age: 80
Date of birth: February 1st
Patient ID: 000123
Discharge date: May 20th
Discharge diagnosis:
1. Acute diastolic heart failure
2. Chronic atrial fibrillation and rapid ventricular response
3. Type II diabetes mellitus
4. Hypercalcemia
5. Dislpidemia
6. Asymptomatic bacterrioria
7. Acute and chronic renal failure
8. Hepatitis C
Reason for hospitalization:
The patient is an 80 year old black female with a history of heart failure who
presented for FORS general medical center from a cardiologist office complaining of
shortness of breath associated with diuresis. She was found to be associated with atrial
fibrillation and was evaluated for further evaluation and treatment.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10NURSING
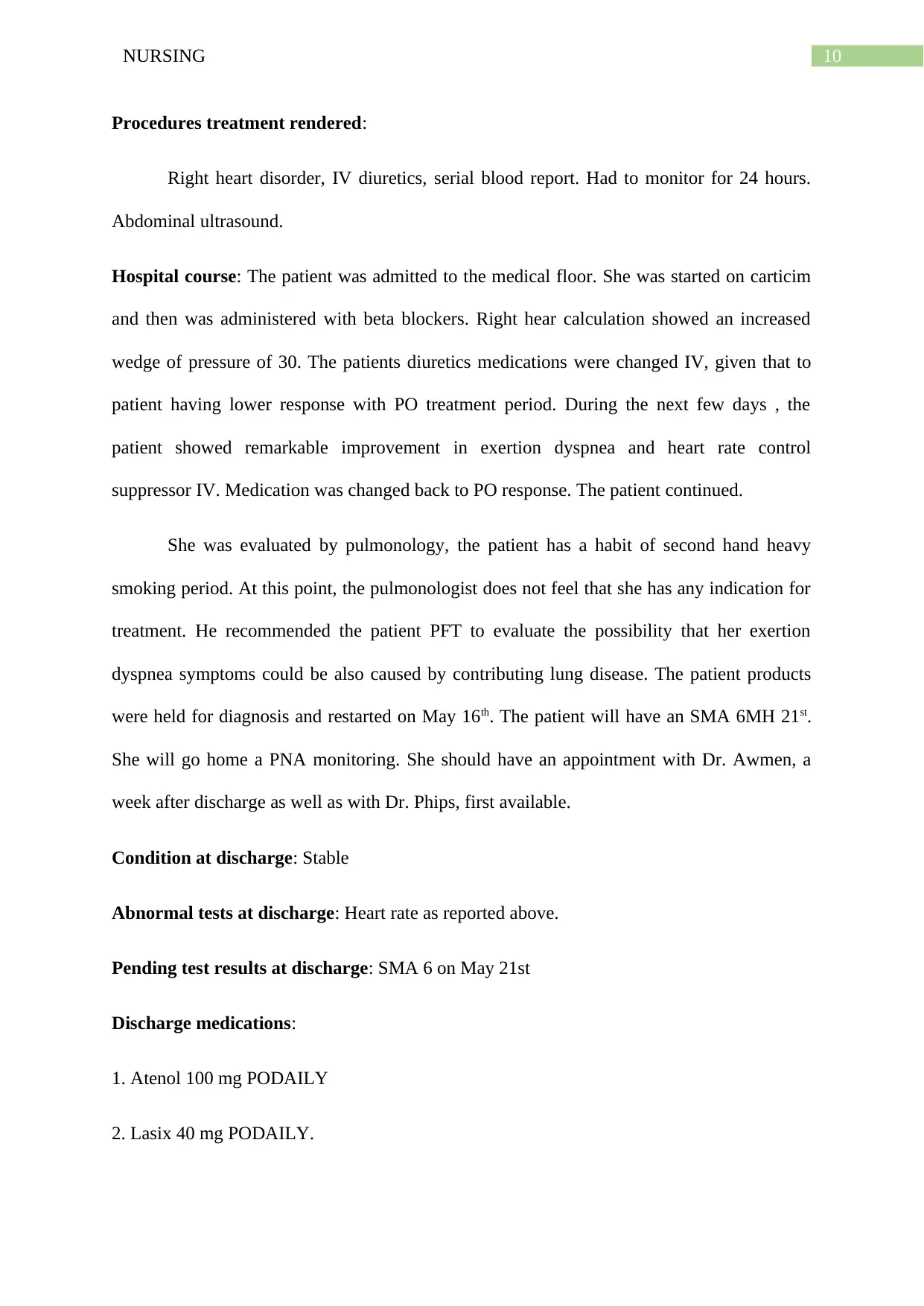
Procedures treatment rendered:
Right heart disorder, IV diuretics, serial blood report. Had to monitor for 24 hours.
Abdominal ultrasound.
Hospital course: The patient was admitted to the medical floor. She was started on carticim
and then was administered with beta blockers. Right hear calculation showed an increased
wedge of pressure of 30. The patients diuretics medications were changed IV, given that to
patient having lower response with PO treatment period. During the next few days , the
patient showed remarkable improvement in exertion dyspnea and heart rate control
suppressor IV. Medication was changed back to PO response. The patient continued.
She was evaluated by pulmonology, the patient has a habit of second hand heavy
smoking period. At this point, the pulmonologist does not feel that she has any indication for
treatment. He recommended the patient PFT to evaluate the possibility that her exertion
dyspnea symptoms could be also caused by contributing lung disease. The patient products
were held for diagnosis and restarted on May 16th. The patient will have an SMA 6MH 21st.
She will go home a PNA monitoring. She should have an appointment with Dr. Awmen, a
week after discharge as well as with Dr. Phips, first available.
Condition at discharge: Stable
Abnormal tests at discharge: Heart rate as reported above.
Pending test results at discharge: SMA 6 on May 21st
Discharge medications:
1. Atenol 100 mg PODAILY
2. Lasix 40 mg PODAILY.
Procedures treatment rendered:
Right heart disorder, IV diuretics, serial blood report. Had to monitor for 24 hours.
Abdominal ultrasound.
Hospital course: The patient was admitted to the medical floor. She was started on carticim
and then was administered with beta blockers. Right hear calculation showed an increased
wedge of pressure of 30. The patients diuretics medications were changed IV, given that to
patient having lower response with PO treatment period. During the next few days , the
patient showed remarkable improvement in exertion dyspnea and heart rate control
suppressor IV. Medication was changed back to PO response. The patient continued.
She was evaluated by pulmonology, the patient has a habit of second hand heavy
smoking period. At this point, the pulmonologist does not feel that she has any indication for
treatment. He recommended the patient PFT to evaluate the possibility that her exertion
dyspnea symptoms could be also caused by contributing lung disease. The patient products
were held for diagnosis and restarted on May 16th. The patient will have an SMA 6MH 21st.
She will go home a PNA monitoring. She should have an appointment with Dr. Awmen, a
week after discharge as well as with Dr. Phips, first available.
Condition at discharge: Stable
Abnormal tests at discharge: Heart rate as reported above.
Pending test results at discharge: SMA 6 on May 21st
Discharge medications:
1. Atenol 100 mg PODAILY
2. Lasix 40 mg PODAILY.
11NURSING
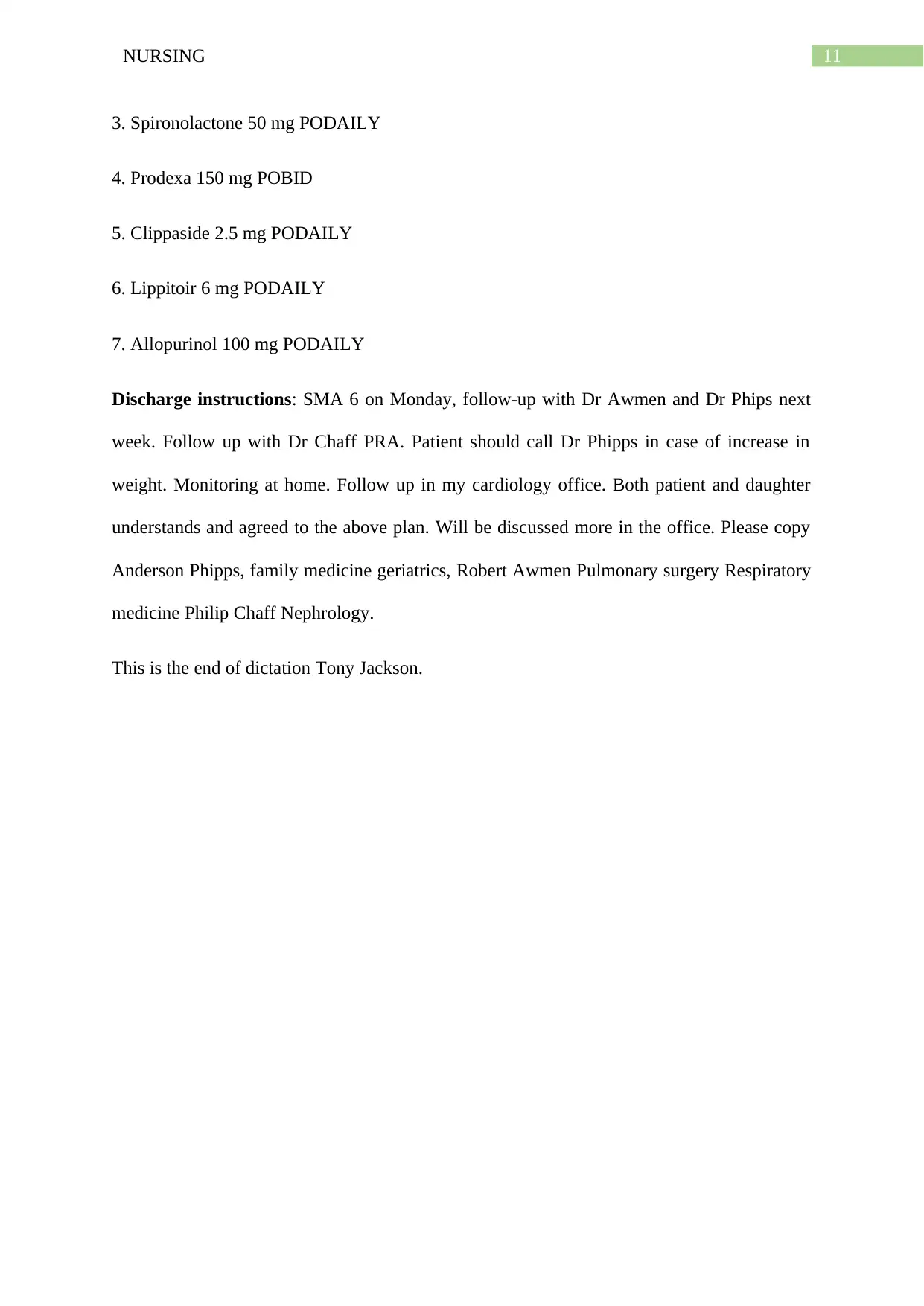
3. Spironolactone 50 mg PODAILY
4. Prodexa 150 mg POBID
5. Clippaside 2.5 mg PODAILY
6. Lippitoir 6 mg PODAILY
7. Allopurinol 100 mg PODAILY
Discharge instructions: SMA 6 on Monday, follow-up with Dr Awmen and Dr Phips next
week. Follow up with Dr Chaff PRA. Patient should call Dr Phipps in case of increase in
weight. Monitoring at home. Follow up in my cardiology office. Both patient and daughter
understands and agreed to the above plan. Will be discussed more in the office. Please copy
Anderson Phipps, family medicine geriatrics, Robert Awmen Pulmonary surgery Respiratory
medicine Philip Chaff Nephrology.
This is the end of dictation Tony Jackson.
3. Spironolactone 50 mg PODAILY
4. Prodexa 150 mg POBID
5. Clippaside 2.5 mg PODAILY
6. Lippitoir 6 mg PODAILY
7. Allopurinol 100 mg PODAILY
Discharge instructions: SMA 6 on Monday, follow-up with Dr Awmen and Dr Phips next
week. Follow up with Dr Chaff PRA. Patient should call Dr Phipps in case of increase in
weight. Monitoring at home. Follow up in my cardiology office. Both patient and daughter
understands and agreed to the above plan. Will be discussed more in the office. Please copy
Anderson Phipps, family medicine geriatrics, Robert Awmen Pulmonary surgery Respiratory
medicine Philip Chaff Nephrology.
This is the end of dictation Tony Jackson.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 35
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.