Systematic Review: Nursing Resources and Patient Outcomes in ICUs
VerifiedAdded on 2023/03/20
|19
|13553
|52
Report
AI Summary
This report presents a systematic review of the literature on the impact of nursing resources on patient outcomes in intensive care units (ICUs). The review, published in the International Journal of Nursing Studies, examines 15 studies to evaluate the relationship between nursing resources (nurse-patient ratios, nurses' education, training, and experience) and patient outcomes, including mortality and adverse events. The findings reveal that some studies found a statistical relationship between nursing resources and both mortality and adverse events, while others reported associations with mortality only or found no significant relationship. The review highlights the methodological challenges in this area, including the observational and retrospective nature of many studies, and suggests the need for future research, including multi-center prospective studies. The main explanatory mechanisms were the lack of time for nurses to perform preventative measures, or for patient surveillance.
Review
Nursing resources and patient outcomes in intensive car
A systematic review of the literature
Elizabeth Westa,*, Nicholas Maysb, Anne Marie Raffertyc,
Kathy Rowand, Colin Sandersonb
aSchool of Health and Social Care,University of Greenwich,Southwood Site,Avery Hill Road,Eltham, London SE9 2UG,UK
bLondon School of Hygiene and Tropical Medicine, Keppel Street,London WC1E 7HT,UK
c Florence Nightingale School of Nursing and Midwifery,King’s College London,James Clerk Maxwell Building,
57 Waterloo Road, London SE1 8WA,UK
dIntensive Care National Audit and Research Centre,Tavistock House,Tavistock Square,London WC1H 9HR,USA
Received 7 November 2006; received in revised form 25 May 2007; accepted 3 July 2007
Abstract
Objectives:To evaluate the empirical evidence linking nursing resources to patient outcomes in intensive care se
framework for future research in this area.
Background:Concerns about patient safety and the quality of care are driving research on the clinical and cost-e
health care interventions, including the deployment of human resources. This is particularly important in intens
large proportion of the health care budget is consumed and where nursing staff is the main item of expenditure
tions about staffing levels have been made but may not be evidence based and may not always be achieved in
Methods:We searched systematically for studies of the impact of nursing resources (e.g. nurse–patient ratios, n
education,training and experience) on patientoutcomes,including mortality and adverse events,in adultintensive care.
Abstracts of articles were reviewed and retrieved if they investigated the relationship between nursing resourc
outcomes.Characteristics of the studies were tabulated and the quality of the studies assessed.
Results:Of the 15 studies included in this review, two reported a statistical relationship between nursing resourc
mortality and adverse events, one reported an association to mortality only, seven studies reported that they c
null hypothesis of no relationship to mortality and 10 studies (out of 10 that tested the hypothesis) reported a r
adverse events. The main explanatory mechanisms were the lack of time for nurses to perform preventative m
patientsurveillance.The nurses’ role in pain controlwas noted by one author.Studies were mainly observationaland
retrospective and varied in scope from 1 to 52 units. Recommendations for future research include developing
linking nursing resources to patient outcomes, and designing large multi-centre prospective studies that link pa
nursing care on a shift-by-shift basis over time.
# 2007 Elsevier Ltd.All rights reserved.
Keywords:Nursing; Outcomes assessment; Hospital mortality; Complications; Intensive care; Health services research
What is already known about the topic?
A previous systematic review concluded thatthere is
currently insufficientevidence to rejectthe hypothesis
www.elsevier.com/ijns
Available online at www.sciencedirect.com
International Journal of Nursing Studies 46 (2009) 993–1011
* Corresponding author.Tel.: +44 1865 512 938.
E-mail address: Lizwestbarron@googlemail.com (E.West).
0020-7489/$ – see front matter # 2007 Elsevier Ltd.All rights reserved.
doi:10.1016/j.ijnurstu.2007.07.011
Nursing resources and patient outcomes in intensive car
A systematic review of the literature
Elizabeth Westa,*, Nicholas Maysb, Anne Marie Raffertyc,
Kathy Rowand, Colin Sandersonb
aSchool of Health and Social Care,University of Greenwich,Southwood Site,Avery Hill Road,Eltham, London SE9 2UG,UK
bLondon School of Hygiene and Tropical Medicine, Keppel Street,London WC1E 7HT,UK
c Florence Nightingale School of Nursing and Midwifery,King’s College London,James Clerk Maxwell Building,
57 Waterloo Road, London SE1 8WA,UK
dIntensive Care National Audit and Research Centre,Tavistock House,Tavistock Square,London WC1H 9HR,USA
Received 7 November 2006; received in revised form 25 May 2007; accepted 3 July 2007
Abstract
Objectives:To evaluate the empirical evidence linking nursing resources to patient outcomes in intensive care se
framework for future research in this area.
Background:Concerns about patient safety and the quality of care are driving research on the clinical and cost-e
health care interventions, including the deployment of human resources. This is particularly important in intens
large proportion of the health care budget is consumed and where nursing staff is the main item of expenditure
tions about staffing levels have been made but may not be evidence based and may not always be achieved in
Methods:We searched systematically for studies of the impact of nursing resources (e.g. nurse–patient ratios, n
education,training and experience) on patientoutcomes,including mortality and adverse events,in adultintensive care.
Abstracts of articles were reviewed and retrieved if they investigated the relationship between nursing resourc
outcomes.Characteristics of the studies were tabulated and the quality of the studies assessed.
Results:Of the 15 studies included in this review, two reported a statistical relationship between nursing resourc
mortality and adverse events, one reported an association to mortality only, seven studies reported that they c
null hypothesis of no relationship to mortality and 10 studies (out of 10 that tested the hypothesis) reported a r
adverse events. The main explanatory mechanisms were the lack of time for nurses to perform preventative m
patientsurveillance.The nurses’ role in pain controlwas noted by one author.Studies were mainly observationaland
retrospective and varied in scope from 1 to 52 units. Recommendations for future research include developing
linking nursing resources to patient outcomes, and designing large multi-centre prospective studies that link pa
nursing care on a shift-by-shift basis over time.
# 2007 Elsevier Ltd.All rights reserved.
Keywords:Nursing; Outcomes assessment; Hospital mortality; Complications; Intensive care; Health services research
What is already known about the topic?
A previous systematic review concluded thatthere is
currently insufficientevidence to rejectthe hypothesis
www.elsevier.com/ijns
Available online at www.sciencedirect.com
International Journal of Nursing Studies 46 (2009) 993–1011
* Corresponding author.Tel.: +44 1865 512 938.
E-mail address: Lizwestbarron@googlemail.com (E.West).
0020-7489/$ – see front matter # 2007 Elsevier Ltd.All rights reserved.
doi:10.1016/j.ijnurstu.2007.07.011
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
of no association between nursing resources and mortality
in intensive care.
Several non-systematic reviews suggest that there may be
a link between nurse staffing and the developmentof
adverse events among patients in intensive care.
There are many methodologicaldifficulties to be over-
come in conducting research in this area.
What this paper adds?
This paper describes and critiques studies of the impact of
nursing resources on mortality and adverse events in one
systematic review.
Focuses attention on the methods used and devises a way
of assessing the scientific rigour of observational studies
which are notoriously difficult to evaluate.
Finds that studies of adverse events in ICU were likely to
report significant relationships between staffing and out-
comes butthatthe number of positive associations was
small relative to the number of hypothesised relationships
tested.
Links study findings to features of research design.The
three studies thatfound a relationship between nursing
and mortality were small prospective studies whereas the
seven studies that found no association were large multi-
unit studies based on administrative data.
Shows that several studies that failed to reject the hypoth-
esis ofno association between staffing levels and out-
comes had little variation in staffing levels.
1. Introduction
Historians of criticalcare nursing trace its origins to
the increasing demand for health care in the 1950s and to
the invention of the ‘iron lung,’ a precursor of the modern
ventilator (Reis Miranda etal., 1998;Bennettand Bion,
1999;Fairman and Lynaugh,1998).Intensive care units
(ICUs) were notdesigned simply to care forthe most
seriously ill, but for those for whom survival was possible,
but not certain. Patients admitted to intensive care were to
be closely observed by skilled nurses capable ofinter-
vening clinically and of mobilising the resources of the
hospitalon their behalf.Although intensive care is often
associated with high technology,this can obscurethe
importance ofthe two cardinalorganisationalfeatures
of intensive care:triage and surveillance (Fairman and
Lynaugh,1998;Sandelowski,2000).Advances in tech-
nology are tools to support staff in monitoring and treating
patients who are critically ill,rather than a substitute for
skilled health care staff (Sandelowski,2000;Westet al.,
2004).
For many, intensive care is central to the activities of the
hospital because its function is so clearly aligned with the
main goalof saving lives.Clinicians and managers have
often maintained staffing levels in ICU by,for example,
closing beds in other parts of the hospital, transferring staff
from other parts of the hospital or employing agency nur
(DoH, 2000a).Recommendations aboutstaffing in ICUs
have been in place since the late 1960s in the UK and the
‘gold standard’ of one nurse to each ICU patient is widely
accepted (British Medical Association, 1967; Royal Colleg
of Nursing, 2000, 2003). However, there is now a great d
of uncertainty and debate aboutthe levels of staffing and
skill mix that are required for patient safety.
Criticalto Success,a reportby the AuditCommission
(1999), found wide variations in the numbers and grades
staff employed in ICUs in the UK and in the number of
nurses who were supernumerary (i.e. not engaged in dire
patient care). They also found that mortality was unexpec
edly high in some UK ICUs,but they were unable to
establish whether or not this was linked to different staffi
levels. The report recommended a more flexible approach
nurse staffing but this is difficult to implement in the abse
of good measuresof staffresources,patientneedsand
outcomes.There isclearly a need forsound empirical
evidence to guide decisions about the deploymentof staff
to ensure patientsafety and improve both the quality and
cost-effectiveness of care.
2. Purpose of the study
This paper reviews empiricalevidence aboutthe link
between nursing resources and patient outcomes in inten
sive care,assessesits strengthsand weaknesses,and
identifies where furtherresearch is required.The focus
is on whetherand to whatextentcharacteristics ofthe
nursing workforce,such asthe numberof nursesper
patient and the skill mix of the nursing staff,affect rates
of mortality and adverse events,such as post-operative
complications and hospital-acquired infections.Although
there is a burgeoning literature on organisational behavio
in intensive care, including topics such as, communicatio
and collaboration within teams,we focuson variables
associated with the conceptof human capital(Becker,
1964),in this case,the number of nurses and their levels
of education,training and experience.Limiting the scope
of the review in this way allows closerscrutiny ofthe
quality of papers included. This is important because man
of the studies in this area are observationalratherthan
experimental,and as such arenotoriously difficultto
evaluate (Downs and Black,1998).
Much is already known about the importance of medic
staff in intensive care.Pronovost et al. (2002) reviewed 26
observational studies of the impact of ICU physician staffi
patterns on patient outcomes and concluded that high in
sity physician staffing (a closed ICU or one where consult
tion with an intensivist is mandatory) was associated with
reduced hospital and ICU mortality and length of stay. Th
research question addressed here is whetherthere is any
evidence that patterns of nurse staffing are similarly imp
cated in patient outcomes.
E. West et al. / International Journal of Nursing Studies 46 (2009) 993–1011994
in intensive care.
Several non-systematic reviews suggest that there may be
a link between nurse staffing and the developmentof
adverse events among patients in intensive care.
There are many methodologicaldifficulties to be over-
come in conducting research in this area.
What this paper adds?
This paper describes and critiques studies of the impact of
nursing resources on mortality and adverse events in one
systematic review.
Focuses attention on the methods used and devises a way
of assessing the scientific rigour of observational studies
which are notoriously difficult to evaluate.
Finds that studies of adverse events in ICU were likely to
report significant relationships between staffing and out-
comes butthatthe number of positive associations was
small relative to the number of hypothesised relationships
tested.
Links study findings to features of research design.The
three studies thatfound a relationship between nursing
and mortality were small prospective studies whereas the
seven studies that found no association were large multi-
unit studies based on administrative data.
Shows that several studies that failed to reject the hypoth-
esis ofno association between staffing levels and out-
comes had little variation in staffing levels.
1. Introduction
Historians of criticalcare nursing trace its origins to
the increasing demand for health care in the 1950s and to
the invention of the ‘iron lung,’ a precursor of the modern
ventilator (Reis Miranda etal., 1998;Bennettand Bion,
1999;Fairman and Lynaugh,1998).Intensive care units
(ICUs) were notdesigned simply to care forthe most
seriously ill, but for those for whom survival was possible,
but not certain. Patients admitted to intensive care were to
be closely observed by skilled nurses capable ofinter-
vening clinically and of mobilising the resources of the
hospitalon their behalf.Although intensive care is often
associated with high technology,this can obscurethe
importance ofthe two cardinalorganisationalfeatures
of intensive care:triage and surveillance (Fairman and
Lynaugh,1998;Sandelowski,2000).Advances in tech-
nology are tools to support staff in monitoring and treating
patients who are critically ill,rather than a substitute for
skilled health care staff (Sandelowski,2000;Westet al.,
2004).
For many, intensive care is central to the activities of the
hospital because its function is so clearly aligned with the
main goalof saving lives.Clinicians and managers have
often maintained staffing levels in ICU by,for example,
closing beds in other parts of the hospital, transferring staff
from other parts of the hospital or employing agency nur
(DoH, 2000a).Recommendations aboutstaffing in ICUs
have been in place since the late 1960s in the UK and the
‘gold standard’ of one nurse to each ICU patient is widely
accepted (British Medical Association, 1967; Royal Colleg
of Nursing, 2000, 2003). However, there is now a great d
of uncertainty and debate aboutthe levels of staffing and
skill mix that are required for patient safety.
Criticalto Success,a reportby the AuditCommission
(1999), found wide variations in the numbers and grades
staff employed in ICUs in the UK and in the number of
nurses who were supernumerary (i.e. not engaged in dire
patient care). They also found that mortality was unexpec
edly high in some UK ICUs,but they were unable to
establish whether or not this was linked to different staffi
levels. The report recommended a more flexible approach
nurse staffing but this is difficult to implement in the abse
of good measuresof staffresources,patientneedsand
outcomes.There isclearly a need forsound empirical
evidence to guide decisions about the deploymentof staff
to ensure patientsafety and improve both the quality and
cost-effectiveness of care.
2. Purpose of the study
This paper reviews empiricalevidence aboutthe link
between nursing resources and patient outcomes in inten
sive care,assessesits strengthsand weaknesses,and
identifies where furtherresearch is required.The focus
is on whetherand to whatextentcharacteristics ofthe
nursing workforce,such asthe numberof nursesper
patient and the skill mix of the nursing staff,affect rates
of mortality and adverse events,such as post-operative
complications and hospital-acquired infections.Although
there is a burgeoning literature on organisational behavio
in intensive care, including topics such as, communicatio
and collaboration within teams,we focuson variables
associated with the conceptof human capital(Becker,
1964),in this case,the number of nurses and their levels
of education,training and experience.Limiting the scope
of the review in this way allows closerscrutiny ofthe
quality of papers included. This is important because man
of the studies in this area are observationalratherthan
experimental,and as such arenotoriously difficultto
evaluate (Downs and Black,1998).
Much is already known about the importance of medic
staff in intensive care.Pronovost et al. (2002) reviewed 26
observational studies of the impact of ICU physician staffi
patterns on patient outcomes and concluded that high in
sity physician staffing (a closed ICU or one where consult
tion with an intensivist is mandatory) was associated with
reduced hospital and ICU mortality and length of stay. Th
research question addressed here is whetherthere is any
evidence that patterns of nurse staffing are similarly imp
cated in patient outcomes.
E. West et al. / International Journal of Nursing Studies 46 (2009) 993–1011994
3. Methods
3.1.Search strategy
Previous authors have drawn attention to the difficulties
of defining standard search terms in this area.Pronovost
et al. (2002), for example, reported that their comprehensive
search for empirical evidence on physician staffing patterns
did not uncover some of their own work. Carmel and Rowan
(2001) note that their review of the literature on organisa-
tional factors related to patient mortality was hampered by
the fact that electronic databases tend to adopt a biomedical-
intervention perspective. We therefore used many different
terms and strategies to try to ensure thatthe search for
relevant articles was as complete as possible:
Unit labels intensive care units; intensive care; surgical
intensive care; critical care; high dependency;
open,closed,critically ill
Outcomes outcome assessment, treatment outcomes,
mortality,morbidity,adverse events,infections,
length of stay,complications,error/s,
readmission/s,admission/s
Nursing nursing staff,hospital staffing
Workforce labour force,health care workforce,manpower,
workforce policy,training,education,nurse/s,
number,size,staffing levels,ratio/s, skill mix,
substitution, specialisation,training,education,
grade/s, staff development, human resources, HR
management, personnel staffing and scheduling
Workload volume of activity,workload
Methods multi-level modelling, case mix adjustment, risk
adjustment, APACHE, SAPS, case-control study,
retrospective study
The ‘related articles’feature in Pubmed was used in
locating studies, as was Google Scholar. The bibliographies
of articles retrieved atthe beginning ofthe search were
scanned for new references.
3.2.Inclusion and exclusion criteria
Studies were included if they were conducted exclusively
in intensive or critical care settings and allowed data on one or
more of the nursing workforce variables to be related to data
on mortality or adverse events.Studies conducted in acute
medical and surgical units or in neonatal or paediatric inten-
sive care were excluded because these settings are so different
that they warrant separate reviews. Single-unit studies were
included. Only studies published in English in refereed jour-
nals between 1990 and 2006 were included. The only quality
criterion that was used to selected studies was that they had to
have employed some method of risk adjustment. In summary,
studies were included if they met the following criteria:
Conducted exclusively in one or more adult ICUs
Dependent variable was mortality or adverse events
Human capitalcharacteristics of the nursing workforce
formed at least one of the independent variables
Published in English between 1990 and 2006
Used some form of risk adjustment
The first author read all the abstracts and retrieved all t
articles that in her judgement met these criteria.
3.3.Previous reviews
Several reviews have already been conducted in this ar
Carmel and Rowan (2001) found in 63 publications about 5
different studies of the organisation of intensive care, whic
they grouped into eightcategories:staffing,teamwork,
volume and pressure of work, protocols, admission to inte
sive care, technology, structure and error. Articles on staffi
were the most common and fell into a number of different
strands of research on management and personnel, intens
vist-led units,medicaland nursing intensity and nursing
autonomy.Five studies focussed on the impactof nursing
intensity (mainly nurse–patientratios,butone study also
examined levelof nurse qualifications)on mortality,but
none were able to rejectthe hypothesis of no association.
This was a usefulsource ofinformation aboutstudies
published prior to 2000.
Numata etal. (2006) reviewed the literature on nurse–
patientratiosand mortality in ICUsand identified nine
observationalstudies,five of which were included in a
meta-analysis.The unadjusted risk ratios of nurse staffing
(high versus low) on hospitalmortality were combined to
give a pooled estimate of 0.65 (95% CI 0.47–0.91).How-
ever,after adjusting for covariates the association between
staffing and mortality became non-significant in all but on
study (Tarnow-Mordiet al., 2000).Numata etal. (2006)
acknowledged that their meta-analysis was based on a sm
number of studies, four of which were conducted in the sa
region of the United States. They concluded that there wa
insufficient evidence to support an independent associatio
between nurses staffing levels and the mortality of critical
ill patients.They identified arangeof methodological
challenges: lack of an agreed operational definition of nurs
staffing, lack of variation in staffing levels in some studies
staffing levels which varied from shift-to-shift measured at
one pointin time,confounding factorsnot included or
controlled in any way,failure to use statisticalmethods
appropriate for the research design,crude methods of risk
adjustment due to the use of administrative databases and
tendency to analyse hospital mortality without considering
the care that the patient received outside the unit.
Both of the above reviews focussed on mortality as the
key variable to be explained, but there is a growing literat
on the impact of nursing on a much broader range of patie
outcomes,including safety,adverse events and complica-
tions, as well as patients’ and relatives’ satisfaction with c
and their subjective experiences of it. Williams et al. (2003
conducted a rapid review of different aspects of workload
E. West et al. / International Journal of Nursing Studies 46 (2009) 993–1011 995
3.1.Search strategy
Previous authors have drawn attention to the difficulties
of defining standard search terms in this area.Pronovost
et al. (2002), for example, reported that their comprehensive
search for empirical evidence on physician staffing patterns
did not uncover some of their own work. Carmel and Rowan
(2001) note that their review of the literature on organisa-
tional factors related to patient mortality was hampered by
the fact that electronic databases tend to adopt a biomedical-
intervention perspective. We therefore used many different
terms and strategies to try to ensure thatthe search for
relevant articles was as complete as possible:
Unit labels intensive care units; intensive care; surgical
intensive care; critical care; high dependency;
open,closed,critically ill
Outcomes outcome assessment, treatment outcomes,
mortality,morbidity,adverse events,infections,
length of stay,complications,error/s,
readmission/s,admission/s
Nursing nursing staff,hospital staffing
Workforce labour force,health care workforce,manpower,
workforce policy,training,education,nurse/s,
number,size,staffing levels,ratio/s, skill mix,
substitution, specialisation,training,education,
grade/s, staff development, human resources, HR
management, personnel staffing and scheduling
Workload volume of activity,workload
Methods multi-level modelling, case mix adjustment, risk
adjustment, APACHE, SAPS, case-control study,
retrospective study
The ‘related articles’feature in Pubmed was used in
locating studies, as was Google Scholar. The bibliographies
of articles retrieved atthe beginning ofthe search were
scanned for new references.
3.2.Inclusion and exclusion criteria
Studies were included if they were conducted exclusively
in intensive or critical care settings and allowed data on one or
more of the nursing workforce variables to be related to data
on mortality or adverse events.Studies conducted in acute
medical and surgical units or in neonatal or paediatric inten-
sive care were excluded because these settings are so different
that they warrant separate reviews. Single-unit studies were
included. Only studies published in English in refereed jour-
nals between 1990 and 2006 were included. The only quality
criterion that was used to selected studies was that they had to
have employed some method of risk adjustment. In summary,
studies were included if they met the following criteria:
Conducted exclusively in one or more adult ICUs
Dependent variable was mortality or adverse events
Human capitalcharacteristics of the nursing workforce
formed at least one of the independent variables
Published in English between 1990 and 2006
Used some form of risk adjustment
The first author read all the abstracts and retrieved all t
articles that in her judgement met these criteria.
3.3.Previous reviews
Several reviews have already been conducted in this ar
Carmel and Rowan (2001) found in 63 publications about 5
different studies of the organisation of intensive care, whic
they grouped into eightcategories:staffing,teamwork,
volume and pressure of work, protocols, admission to inte
sive care, technology, structure and error. Articles on staffi
were the most common and fell into a number of different
strands of research on management and personnel, intens
vist-led units,medicaland nursing intensity and nursing
autonomy.Five studies focussed on the impactof nursing
intensity (mainly nurse–patientratios,butone study also
examined levelof nurse qualifications)on mortality,but
none were able to rejectthe hypothesis of no association.
This was a usefulsource ofinformation aboutstudies
published prior to 2000.
Numata etal. (2006) reviewed the literature on nurse–
patientratiosand mortality in ICUsand identified nine
observationalstudies,five of which were included in a
meta-analysis.The unadjusted risk ratios of nurse staffing
(high versus low) on hospitalmortality were combined to
give a pooled estimate of 0.65 (95% CI 0.47–0.91).How-
ever,after adjusting for covariates the association between
staffing and mortality became non-significant in all but on
study (Tarnow-Mordiet al., 2000).Numata etal. (2006)
acknowledged that their meta-analysis was based on a sm
number of studies, four of which were conducted in the sa
region of the United States. They concluded that there wa
insufficient evidence to support an independent associatio
between nurses staffing levels and the mortality of critical
ill patients.They identified arangeof methodological
challenges: lack of an agreed operational definition of nurs
staffing, lack of variation in staffing levels in some studies
staffing levels which varied from shift-to-shift measured at
one pointin time,confounding factorsnot included or
controlled in any way,failure to use statisticalmethods
appropriate for the research design,crude methods of risk
adjustment due to the use of administrative databases and
tendency to analyse hospital mortality without considering
the care that the patient received outside the unit.
Both of the above reviews focussed on mortality as the
key variable to be explained, but there is a growing literat
on the impact of nursing on a much broader range of patie
outcomes,including safety,adverse events and complica-
tions, as well as patients’ and relatives’ satisfaction with c
and their subjective experiences of it. Williams et al. (2003
conducted a rapid review of different aspects of workload
E. West et al. / International Journal of Nursing Studies 46 (2009) 993–1011 995
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
ICUs, including the policy context and secular trends. They
identified 12 studies of nurse staffing,and presented evi-
dence for a positive effectof increased nurse staffing on
patient outcomes. More recently, Carayon and Gurses (2005)
conducted a wide ranging review ofthe literature.Their
main goalwas to devise a ‘human factorsengineering’
framework to guide modification ofthe work setting to
improve patient safety and to improve the quality of nurses’
work lives in ICUs. They cite several studies that have shown
thatmedicalerrorsare common in ICUsand may be
attributable to problems in communication between nurses
and physicians,to impaired access to information,and to
high intensity nursing workloads. They identified 22 studies
in all,but made no attempt to evaluate them or aggregate
their findings. They concluded that there were at least four
differentkinds of workload associated with the unit,job,
patient and situation. Most studies to date have focussed on
workload associated with the first two: the unit or the patient.
Each of the above reviewsmakesa contribution to
knowledge aboutworkforce,workload and outcomesin
intensive care.The emerging consensus seems to be that
while there is some evidence that the nursing workforce has
an impacton patients’risksof adverse events,there is
insufficient evidence of a link with mortality. This presents
a puzzle because some of the adverse events studied have
known links to mortality.Why would nursing workforce
characteristics affect the more proximate events but not the
final outcome? The process of dying is likely to be one of an
accumulation of adverse events as the patientdeteriorates
and clinicians take increasing risks in an attempt to save their
life. It seems important then to begin to integrate these two
separate strands of work into one coherent analysis.
This study uses systematic review methods to identify
and appraise empiricalevidence aboutthe impactof any
human capital characteristic of the nursing workforce (such
as skill mix, education or employments status, in addition to
nurse–patient ratios) on any patient outcomes,particularly
adverse events such as post-operative infections and mor-
tality.It adds to the literature a deeper description of the
methodsused and attemptsto evaluate the quality and
scientific rigour of the studies reviewed.
4. Results of the literature search
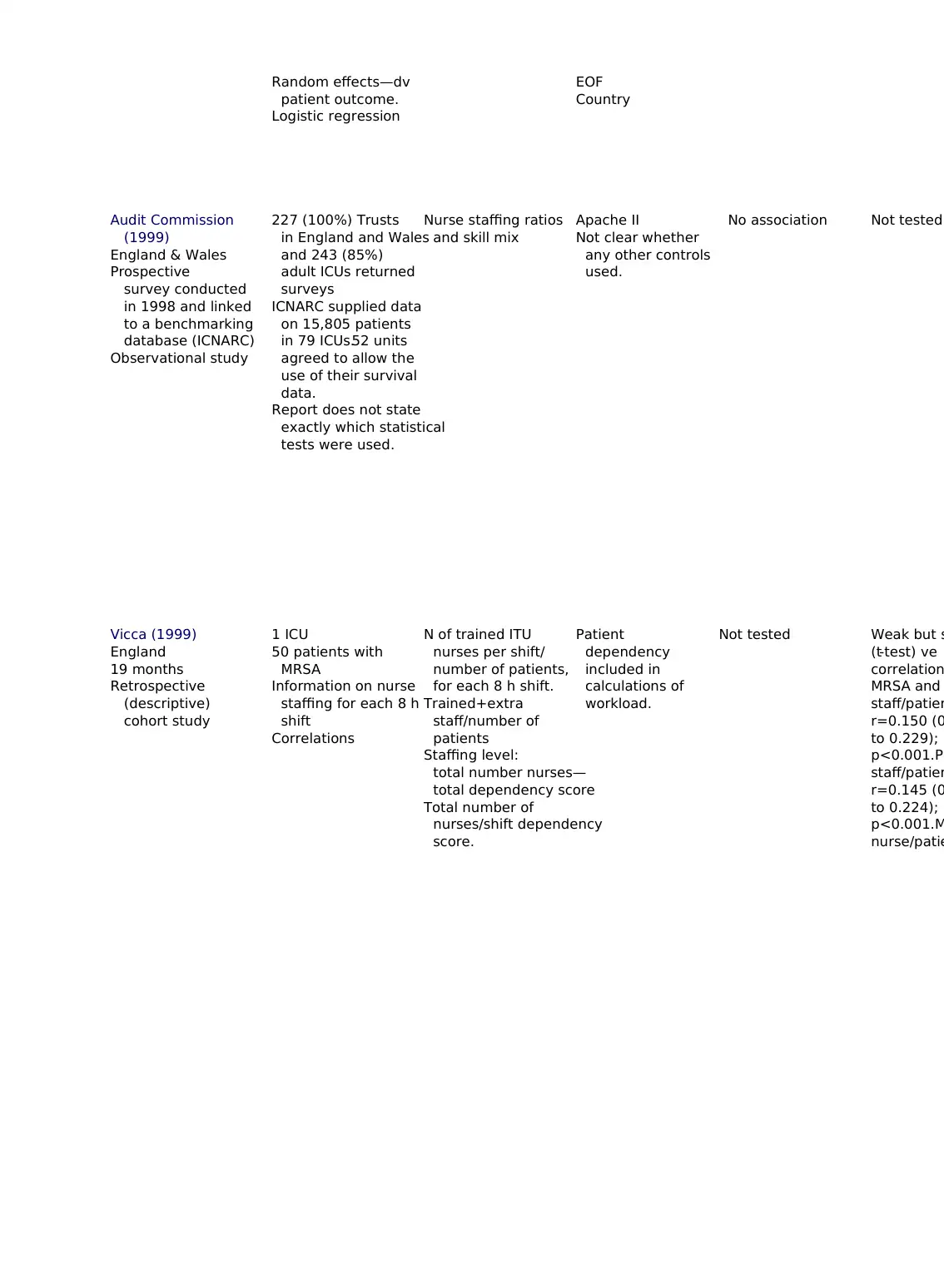
Fifteen studies were identified. Table 1 in the appendix to
this paper shows the key features of each study,including
location,research design,sample,sources of data,nursing
variables,outcome variables,factors adjusted for,findings
and comments.
4.1.Study quality
Research designs employed in this field divide into the
quasi-experimentalsuch as case controlor cohortstudies
with an emphasison directcomparison ofresultsfor
matched groups,and more ‘natural’ observationalstudies
which rely on multivariate analysis to adjust for the effect
known confounders. Quasi-experimental studies (case co
trol and cohort designs) try to come as close to an experi
as possible with random assignmentto ‘treatment’and
‘control’groupswith differentlevels ofexposure to an
intervention,e.g.patients exposed to high levels ofstaff
compared with patients exposed to low staffing levels. No
experimental research designs are more familiar in the so
sciences,where ithasbeen argued thatif a significant
relationship persists after partialing out the effects of con
founding variables (robust dependence), then a causal re
tionshipcan be said to exist (Goldthorpe,2000).In
observationalstudiesof this type there are no ‘control’
group or ‘treatment’ groups and the effects of confoundin
variables are controlled statistically. Although quasi-expe
mental studies do also use multi-variate statistics they te
do so to compensate for failures in matching case and co
groups rather than their main strategy.For the purposes of
this paperthereforewe makea very cleardistinction
between these two types of studies because the differenc
are relevantto the ways in which the studies should be
evaluated.
A great number of tools exist for evaluating randomise
trials (Moher etal.,1995).Downs and Black (1998) also
devised a quality checklistfor non-randomised as wellas
randomised studies buttheir work only extends as far as
quasi-experimental designs. To date, we are not aware of
systematic attempt to develop measures of quality for stu
of this type and so we designed a rudimentary measure
focussing on the following areasas a preliminary step
towards more formal attempts to establish criteria for obs
vational studies.
1. Geographical scope (4): The numbers of patient and un
in the study. The concern here is with how far the resu
can be generalised to other populations, and the geogr
phical coverage of the study is salient. High scores wou
be given to a census or random sample of units across
nation ora large geographicalarea.Medium scores
would be given to a study of a smaller number of units
and a low score would be given to a single-unit study.
2. Quality ofdata (4):How and why were the data were
collected.High scores would be assigned to data that
were collected prospectively to answer the specific que
tions in the study. Low scores would be given to studie
that use data collected for other purposes,e.g. adminis-
trative data.
3. Validity of key independent variables (4): How sensitive
and specific are the key workforce measures as indicat
of the number and quality of nurses available to indivi-
dualpatients? Nurse–patientratios are often averaged
overlong periods oftime and may be simply dichot-
omised into ‘high’ or ‘low.’ High scores would be given
the information on nurses was collected over time and
linked to individualpatients.Medium scores would be
E. West et al. / International Journal of Nursing Studies 46 (2009) 993–1011996
identified 12 studies of nurse staffing,and presented evi-
dence for a positive effectof increased nurse staffing on
patient outcomes. More recently, Carayon and Gurses (2005)
conducted a wide ranging review ofthe literature.Their
main goalwas to devise a ‘human factorsengineering’
framework to guide modification ofthe work setting to
improve patient safety and to improve the quality of nurses’
work lives in ICUs. They cite several studies that have shown
thatmedicalerrorsare common in ICUsand may be
attributable to problems in communication between nurses
and physicians,to impaired access to information,and to
high intensity nursing workloads. They identified 22 studies
in all,but made no attempt to evaluate them or aggregate
their findings. They concluded that there were at least four
differentkinds of workload associated with the unit,job,
patient and situation. Most studies to date have focussed on
workload associated with the first two: the unit or the patient.
Each of the above reviewsmakesa contribution to
knowledge aboutworkforce,workload and outcomesin
intensive care.The emerging consensus seems to be that
while there is some evidence that the nursing workforce has
an impacton patients’risksof adverse events,there is
insufficient evidence of a link with mortality. This presents
a puzzle because some of the adverse events studied have
known links to mortality.Why would nursing workforce
characteristics affect the more proximate events but not the
final outcome? The process of dying is likely to be one of an
accumulation of adverse events as the patientdeteriorates
and clinicians take increasing risks in an attempt to save their
life. It seems important then to begin to integrate these two
separate strands of work into one coherent analysis.
This study uses systematic review methods to identify
and appraise empiricalevidence aboutthe impactof any
human capital characteristic of the nursing workforce (such
as skill mix, education or employments status, in addition to
nurse–patient ratios) on any patient outcomes,particularly
adverse events such as post-operative infections and mor-
tality.It adds to the literature a deeper description of the
methodsused and attemptsto evaluate the quality and
scientific rigour of the studies reviewed.
4. Results of the literature search
Fifteen studies were identified. Table 1 in the appendix to
this paper shows the key features of each study,including
location,research design,sample,sources of data,nursing
variables,outcome variables,factors adjusted for,findings
and comments.
4.1.Study quality
Research designs employed in this field divide into the
quasi-experimentalsuch as case controlor cohortstudies
with an emphasison directcomparison ofresultsfor
matched groups,and more ‘natural’ observationalstudies
which rely on multivariate analysis to adjust for the effect
known confounders. Quasi-experimental studies (case co
trol and cohort designs) try to come as close to an experi
as possible with random assignmentto ‘treatment’and
‘control’groupswith differentlevels ofexposure to an
intervention,e.g.patients exposed to high levels ofstaff
compared with patients exposed to low staffing levels. No
experimental research designs are more familiar in the so
sciences,where ithasbeen argued thatif a significant
relationship persists after partialing out the effects of con
founding variables (robust dependence), then a causal re
tionshipcan be said to exist (Goldthorpe,2000).In
observationalstudiesof this type there are no ‘control’
group or ‘treatment’ groups and the effects of confoundin
variables are controlled statistically. Although quasi-expe
mental studies do also use multi-variate statistics they te
do so to compensate for failures in matching case and co
groups rather than their main strategy.For the purposes of
this paperthereforewe makea very cleardistinction
between these two types of studies because the differenc
are relevantto the ways in which the studies should be
evaluated.
A great number of tools exist for evaluating randomise
trials (Moher etal.,1995).Downs and Black (1998) also
devised a quality checklistfor non-randomised as wellas
randomised studies buttheir work only extends as far as
quasi-experimental designs. To date, we are not aware of
systematic attempt to develop measures of quality for stu
of this type and so we designed a rudimentary measure
focussing on the following areasas a preliminary step
towards more formal attempts to establish criteria for obs
vational studies.
1. Geographical scope (4): The numbers of patient and un
in the study. The concern here is with how far the resu
can be generalised to other populations, and the geogr
phical coverage of the study is salient. High scores wou
be given to a census or random sample of units across
nation ora large geographicalarea.Medium scores
would be given to a study of a smaller number of units
and a low score would be given to a single-unit study.
2. Quality ofdata (4):How and why were the data were
collected.High scores would be assigned to data that
were collected prospectively to answer the specific que
tions in the study. Low scores would be given to studie
that use data collected for other purposes,e.g. adminis-
trative data.
3. Validity of key independent variables (4): How sensitive
and specific are the key workforce measures as indicat
of the number and quality of nurses available to indivi-
dualpatients? Nurse–patientratios are often averaged
overlong periods oftime and may be simply dichot-
omised into ‘high’ or ‘low.’ High scores would be given
the information on nurses was collected over time and
linked to individualpatients.Medium scores would be
E. West et al. / International Journal of Nursing Studies 46 (2009) 993–1011996
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
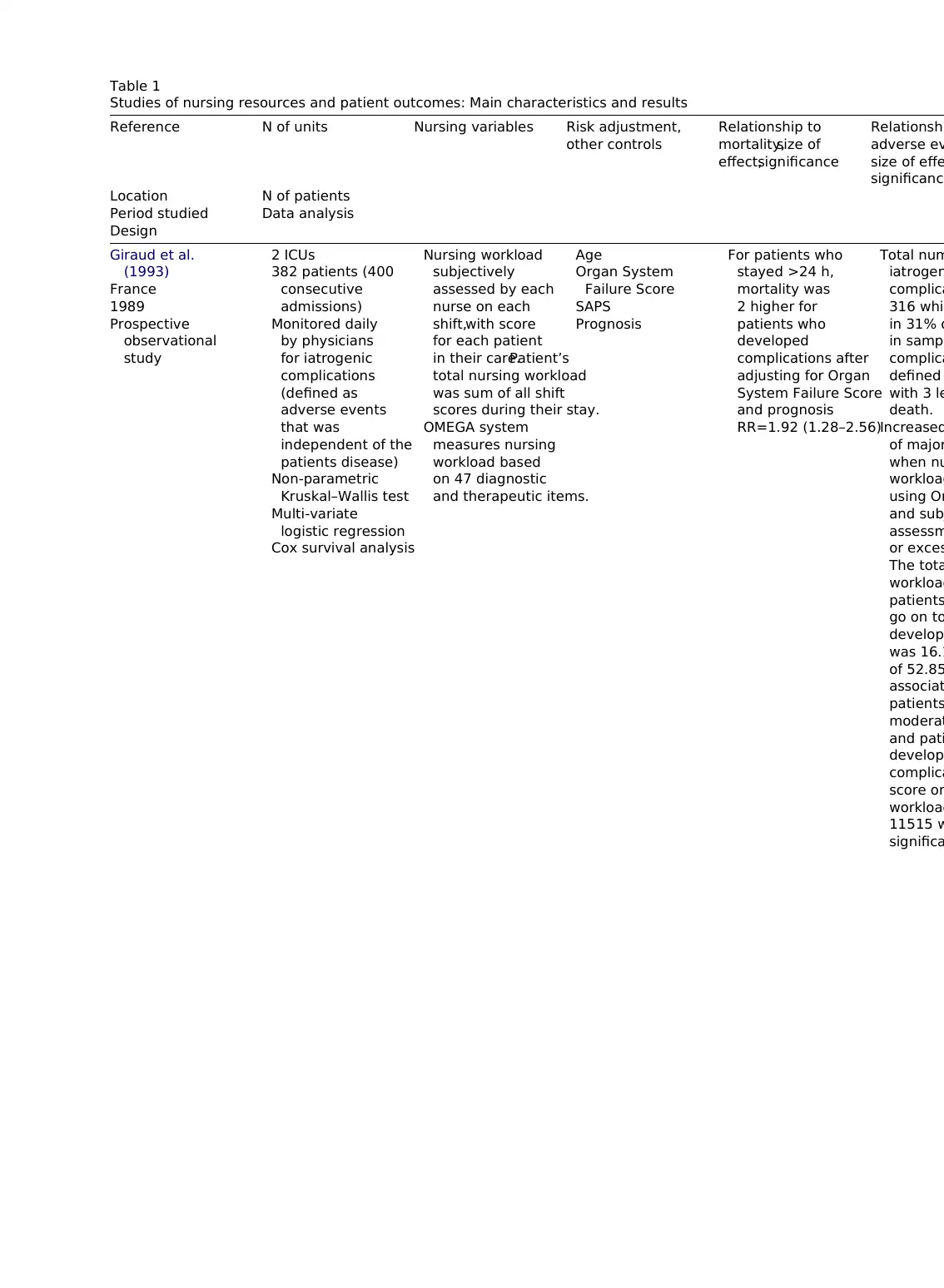
Table 1
Studies of nursing resources and patient outcomes: Main characteristics and results
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Giraud et al.
(1993)
France
1989
Prospective
observational
study
2 ICUs
382 patients (400
consecutive
admissions)
Monitored daily
by physicians
for iatrogenic
complications
(defined as
adverse events
that was
independent of the
patients disease)
Non-parametric
Kruskal–Wallis test
Multi-variate
logistic regression
Cox survival analysis
Nursing workload
subjectively
assessed by each
nurse on each
shift,with score
for each patient
in their care.Patient’s
total nursing workload
was sum of all shift
scores during their stay.
OMEGA system
measures nursing
workload based
on 47 diagnostic
and therapeutic items.
Age
Organ System
Failure Score
SAPS
Prognosis
For patients who
stayed >24 h,
mortality was
2 higher for
patients who
developed
complications after
adjusting for Organ
System Failure Score
and prognosis
RR=1.92 (1.28–2.56)
Total num
iatrogen
complica
316 whic
in 31% o
in sampl
complica
defined
with 3 le
death.
Increased
of major
when nu
workload
using Om
and sub
assessm
or exces
The tota
workload
patients
go on to
develop
was 16.1
of 52.85
associat
patients
moderat
and pati
develop
complica
score on
workload
11515 w
significa
Studies of nursing resources and patient outcomes: Main characteristics and results
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Giraud et al.
(1993)
France
1989
Prospective
observational
study
2 ICUs
382 patients (400
consecutive
admissions)
Monitored daily
by physicians
for iatrogenic
complications
(defined as
adverse events
that was
independent of the
patients disease)
Non-parametric
Kruskal–Wallis test
Multi-variate
logistic regression
Cox survival analysis
Nursing workload
subjectively
assessed by each
nurse on each
shift,with score
for each patient
in their care.Patient’s
total nursing workload
was sum of all shift
scores during their stay.
OMEGA system
measures nursing
workload based
on 47 diagnostic
and therapeutic items.
Age
Organ System
Failure Score
SAPS
Prognosis
For patients who
stayed >24 h,
mortality was
2 higher for
patients who
developed
complications after
adjusting for Organ
System Failure Score
and prognosis
RR=1.92 (1.28–2.56)
Total num
iatrogen
complica
316 whic
in 31% o
in sampl
complica
defined
with 3 le
death.
Increased
of major
when nu
workload
using Om
and sub
assessm
or exces
The tota
workload
patients
go on to
develop
was 16.1
of 52.85
associat
patients
moderat
and pati
develop
complica
score on
workload
11515 w
significa
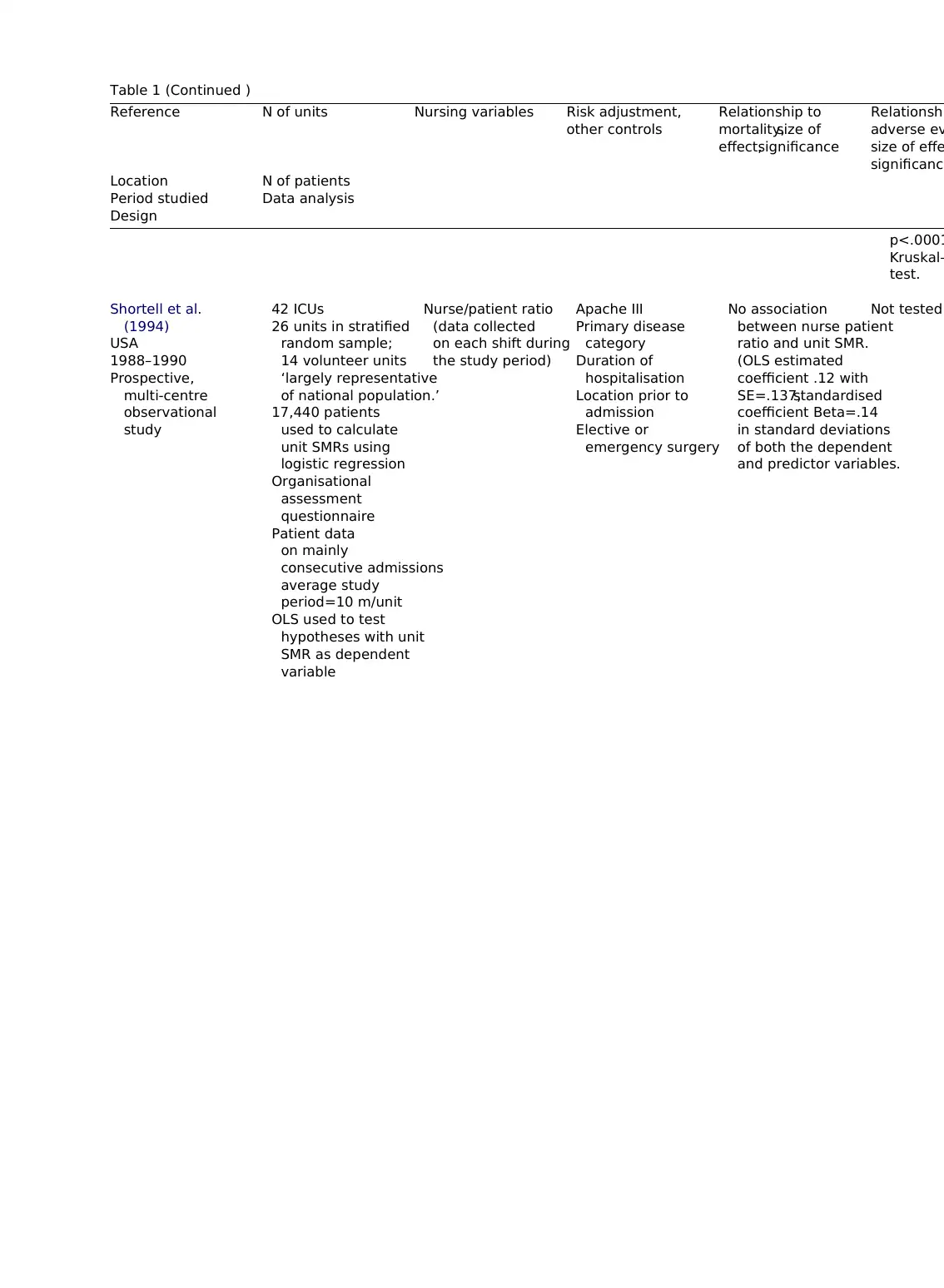
Table 1 (Continued )
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
p<.0001
Kruskal–
test.
Shortell et al.
(1994)
USA
1988–1990
Prospective,
multi-centre
observational
study
42 ICUs
26 units in stratified
random sample;
14 volunteer units
‘largely representative
of national population.’
17,440 patients
used to calculate
unit SMRs using
logistic regression
Organisational
assessment
questionnaire
Patient data
on mainly
consecutive admissions
average study
period=10 m/unit
OLS used to test
hypotheses with unit
SMR as dependent
variable
Nurse/patient ratio
(data collected
on each shift during
the study period)
Apache III
Primary disease
category
Duration of
hospitalisation
Location prior to
admission
Elective or
emergency surgery
No association
between nurse patient
ratio and unit SMR.
(OLS estimated
coefficient .12 with
SE=.137,standardised
coefficient Beta=.14
in standard deviations
of both the dependent
and predictor variables.
Not tested
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
p<.0001
Kruskal–
test.
Shortell et al.
(1994)
USA
1988–1990
Prospective,
multi-centre
observational
study
42 ICUs
26 units in stratified
random sample;
14 volunteer units
‘largely representative
of national population.’
17,440 patients
used to calculate
unit SMRs using
logistic regression
Organisational
assessment
questionnaire
Patient data
on mainly
consecutive admissions
average study
period=10 m/unit
OLS used to test
hypotheses with unit
SMR as dependent
variable
Nurse/patient ratio
(data collected
on each shift during
the study period)
Apache III
Primary disease
category
Duration of
hospitalisation
Location prior to
admission
Elective or
emergency surgery
No association
between nurse patient
ratio and unit SMR.
(OLS estimated
coefficient .12 with
SE=.137,standardised
coefficient Beta=.14
in standard deviations
of both the dependent
and predictor variables.
Not tested
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
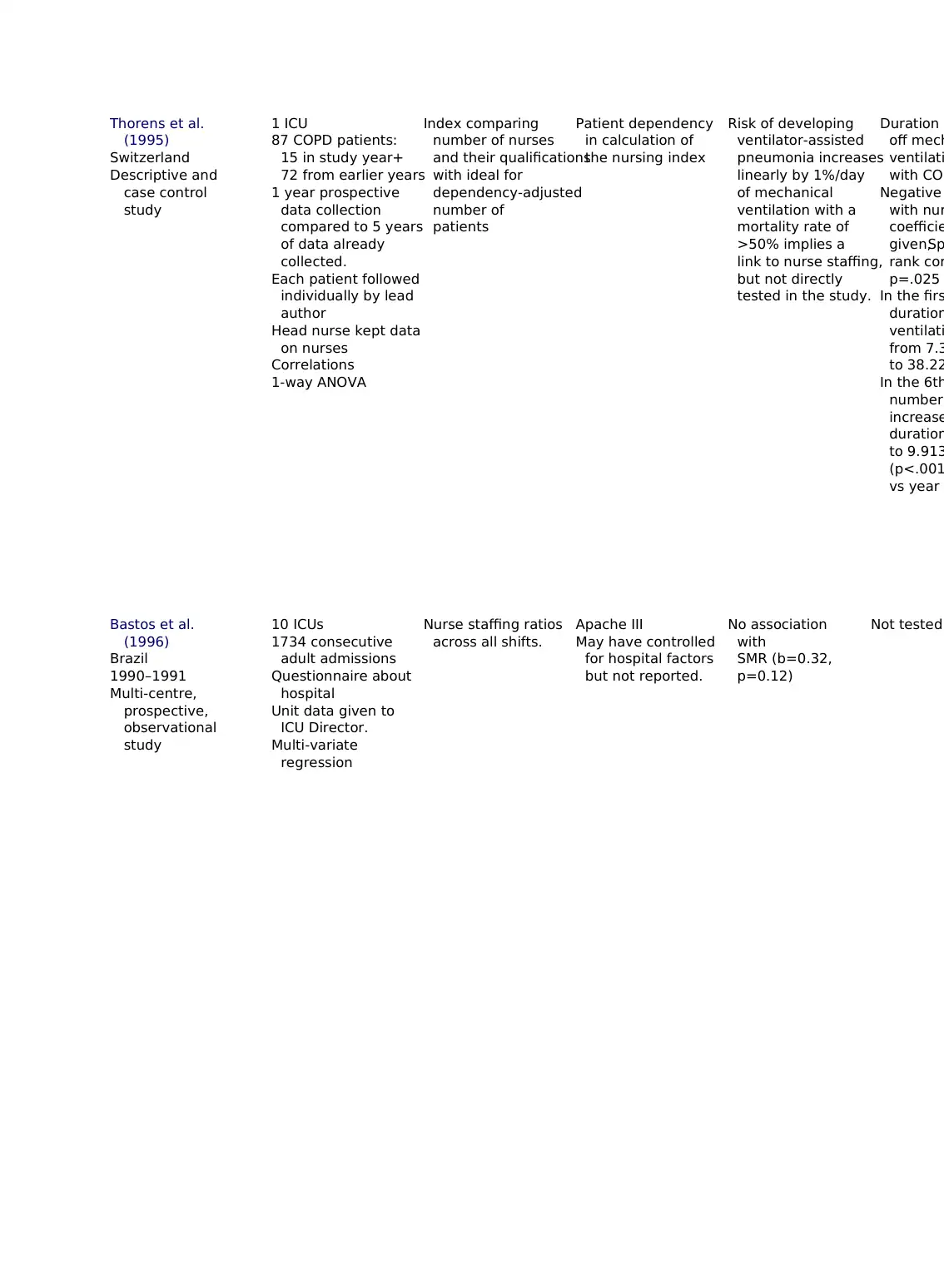
Thorens et al.
(1995)
Switzerland
Descriptive and
case control
study
1 ICU
87 COPD patients:
15 in study year+
72 from earlier years
1 year prospective
data collection
compared to 5 years
of data already
collected.
Each patient followed
individually by lead
author
Head nurse kept data
on nurses
Correlations
1-way ANOVA
Index comparing
number of nurses
and their qualifications
with ideal for
dependency-adjusted
number of
patients
Patient dependency
in calculation of
the nursing index
Risk of developing
ventilator-assisted
pneumonia increases
linearly by 1%/day
of mechanical
ventilation with a
mortality rate of
>50% implies a
link to nurse staffing,
but not directly
tested in the study.
Duration o
off mech
ventilati
with COP
Negative
with nur
coefficie
given,Sp
rank cor
p=.025
In the firs
duration
ventilati
from 7.3
to 38.22
In the 6th
number
increase
duration
to 9.913
(p<.001y
vs year 6
Bastos et al.
(1996)
Brazil
1990–1991
Multi-centre,
prospective,
observational
study
10 ICUs
1734 consecutive
adult admissions
Questionnaire about
hospital
Unit data given to
ICU Director.
Multi-variate
regression
Nurse staffing ratios
across all shifts.
Apache III
May have controlled
for hospital factors
but not reported.
No association
with
SMR (b=0.32,
p=0.12)
Not tested
(1995)
Switzerland
Descriptive and
case control
study
1 ICU
87 COPD patients:
15 in study year+
72 from earlier years
1 year prospective
data collection
compared to 5 years
of data already
collected.
Each patient followed
individually by lead
author
Head nurse kept data
on nurses
Correlations
1-way ANOVA
Index comparing
number of nurses
and their qualifications
with ideal for
dependency-adjusted
number of
patients
Patient dependency
in calculation of
the nursing index
Risk of developing
ventilator-assisted
pneumonia increases
linearly by 1%/day
of mechanical
ventilation with a
mortality rate of
>50% implies a
link to nurse staffing,
but not directly
tested in the study.
Duration o
off mech
ventilati
with COP
Negative
with nur
coefficie
given,Sp
rank cor
p=.025
In the firs
duration
ventilati
from 7.3
to 38.22
In the 6th
number
increase
duration
to 9.913
(p<.001y
vs year 6
Bastos et al.
(1996)
Brazil
1990–1991
Multi-centre,
prospective,
observational
study
10 ICUs
1734 consecutive
adult admissions
Questionnaire about
hospital
Unit data given to
ICU Director.
Multi-variate
regression
Nurse staffing ratios
across all shifts.
Apache III
May have controlled
for hospital factors
but not reported.
No association
with
SMR (b=0.32,
p=0.12)
Not tested
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
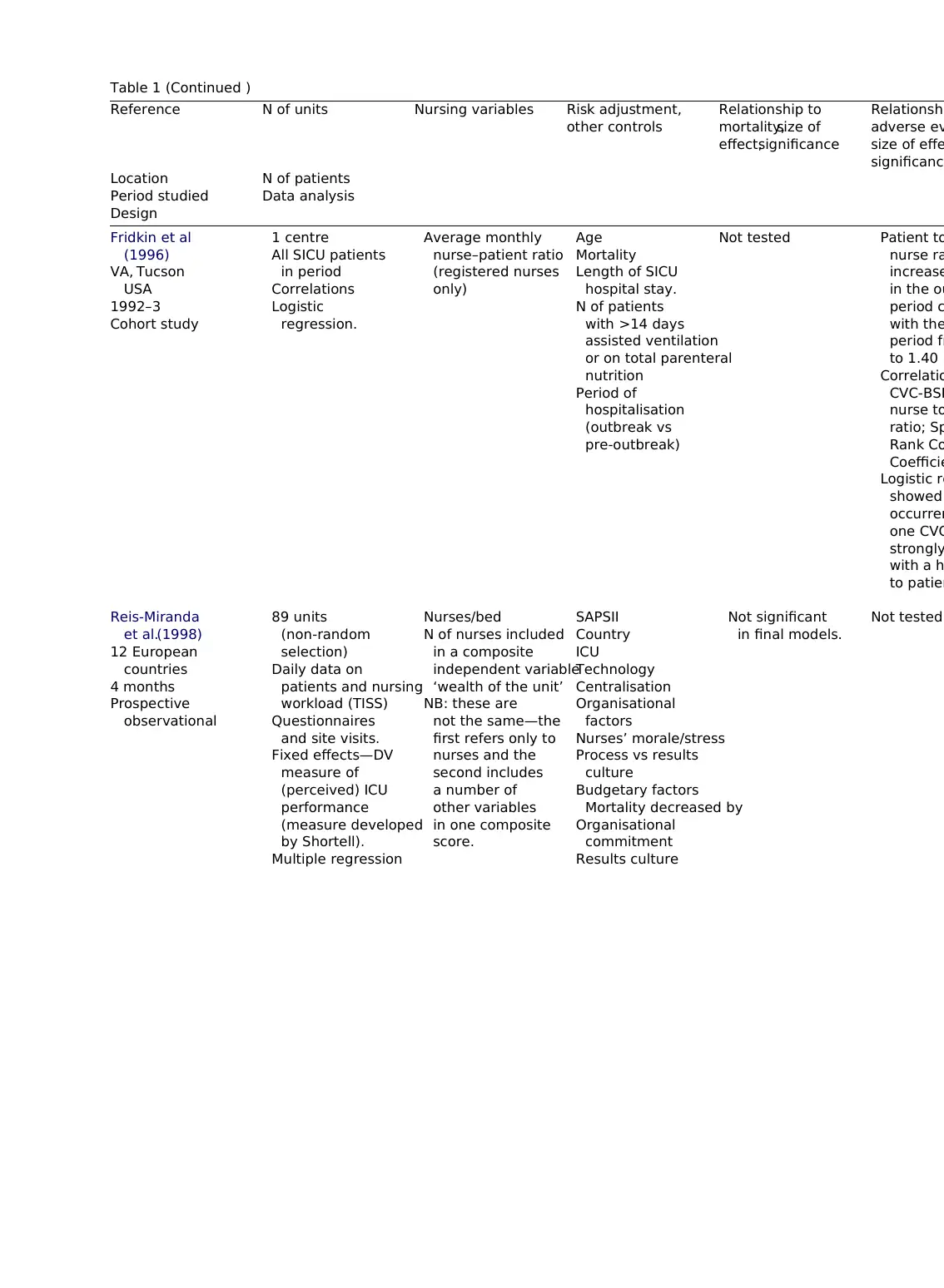
Table 1 (Continued )
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Fridkin et al
(1996)
VA, Tucson
USA
1992–3
Cohort study
1 centre
All SICU patients
in period
Correlations
Logistic
regression.
Average monthly
nurse–patient ratio
(registered nurses
only)
Age
Mortality
Length of SICU
hospital stay.
N of patients
with >14 days
assisted ventilation
or on total parenteral
nutrition
Period of
hospitalisation
(outbreak vs
pre-outbreak)
Not tested Patient to
nurse ra
increase
in the ou
period c
with the
period fr
to 1.40 (
Correlatio
CVC-BSI
nurse to
ratio; Sp
Rank Co
Coefficie
Logistic re
showed
occurren
one CVC
strongly
with a h
to patien
Reis-Miranda
et al.(1998)
12 European
countries
4 months
Prospective
observational
89 units
(non-random
selection)
Daily data on
patients and nursing
workload (TISS)
Questionnaires
and site visits.
Fixed effects—DV
measure of
(perceived) ICU
performance
(measure developed
by Shortell).
Multiple regression
Nurses/bed
N of nurses included
in a composite
independent variable
‘wealth of the unit’
NB: these are
not the same—the
first refers only to
nurses and the
second includes
a number of
other variables
in one composite
score.
SAPSII
Country
ICU
Technology
Centralisation
Organisational
factors
Nurses’ morale/stress
Process vs results
culture
Budgetary factors
Mortality decreased by
Organisational
commitment
Results culture
Not significant
in final models.
Not tested
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Fridkin et al
(1996)
VA, Tucson
USA
1992–3
Cohort study
1 centre
All SICU patients
in period
Correlations
Logistic
regression.
Average monthly
nurse–patient ratio
(registered nurses
only)
Age
Mortality
Length of SICU
hospital stay.
N of patients
with >14 days
assisted ventilation
or on total parenteral
nutrition
Period of
hospitalisation
(outbreak vs
pre-outbreak)
Not tested Patient to
nurse ra
increase
in the ou
period c
with the
period fr
to 1.40 (
Correlatio
CVC-BSI
nurse to
ratio; Sp
Rank Co
Coefficie
Logistic re
showed
occurren
one CVC
strongly
with a h
to patien
Reis-Miranda
et al.(1998)
12 European
countries
4 months
Prospective
observational
89 units
(non-random
selection)
Daily data on
patients and nursing
workload (TISS)
Questionnaires
and site visits.
Fixed effects—DV
measure of
(perceived) ICU
performance
(measure developed
by Shortell).
Multiple regression
Nurses/bed
N of nurses included
in a composite
independent variable
‘wealth of the unit’
NB: these are
not the same—the
first refers only to
nurses and the
second includes
a number of
other variables
in one composite
score.
SAPSII
Country
ICU
Technology
Centralisation
Organisational
factors
Nurses’ morale/stress
Process vs results
culture
Budgetary factors
Mortality decreased by
Organisational
commitment
Results culture
Not significant
in final models.
Not tested
Random effects—dv
patient outcome.
Logistic regression
EOF
Country
Audit Commission
(1999)
England & Wales
Prospective
survey conducted
in 1998 and linked
to a benchmarking
database (ICNARC)
Observational study
227 (100%) Trusts
in England and Wales
and 243 (85%)
adult ICUs returned
surveys
ICNARC supplied data
on 15,805 patients
in 79 ICUs.52 units
agreed to allow the
use of their survival
data.
Report does not state
exactly which statistical
tests were used.
Nurse staffing ratios
and skill mix
Apache II
Not clear whether
any other controls
used.
No association Not tested
Vicca (1999)
England
19 months
Retrospective
(descriptive)
cohort study
1 ICU
50 patients with
MRSA
Information on nurse
staffing for each 8 h
shift
Correlations
N of trained ITU
nurses per shift/
number of patients,
for each 8 h shift.
Trained+extra
staff/number of
patients
Staffing level:
total number nurses—
total dependency score
Total number of
nurses/shift dependency
score.
Patient
dependency
included in
calculations of
workload.
Not tested Weak but s
(t-test) ve
correlation
MRSA and
staff/patien
r=0.150 (0
to 0.229);
p<0.001.Pe
staff/patien
r=0.145 (0
to 0.224);
p<0.001.M
nurse/patie
patient outcome.
Logistic regression
EOF
Country
Audit Commission
(1999)
England & Wales
Prospective
survey conducted
in 1998 and linked
to a benchmarking
database (ICNARC)
Observational study
227 (100%) Trusts
in England and Wales
and 243 (85%)
adult ICUs returned
surveys
ICNARC supplied data
on 15,805 patients
in 79 ICUs.52 units
agreed to allow the
use of their survival
data.
Report does not state
exactly which statistical
tests were used.
Nurse staffing ratios
and skill mix
Apache II
Not clear whether
any other controls
used.
No association Not tested
Vicca (1999)
England
19 months
Retrospective
(descriptive)
cohort study
1 ICU
50 patients with
MRSA
Information on nurse
staffing for each 8 h
shift
Correlations
N of trained ITU
nurses per shift/
number of patients,
for each 8 h shift.
Trained+extra
staff/number of
patients
Staffing level:
total number nurses—
total dependency score
Total number of
nurses/shift dependency
score.
Patient
dependency
included in
calculations of
workload.
Not tested Weak but s
(t-test) ve
correlation
MRSA and
staff/patien
r=0.150 (0
to 0.229);
p<0.001.Pe
staff/patien
r=0.145 (0
to 0.224);
p<0.001.M
nurse/patie
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
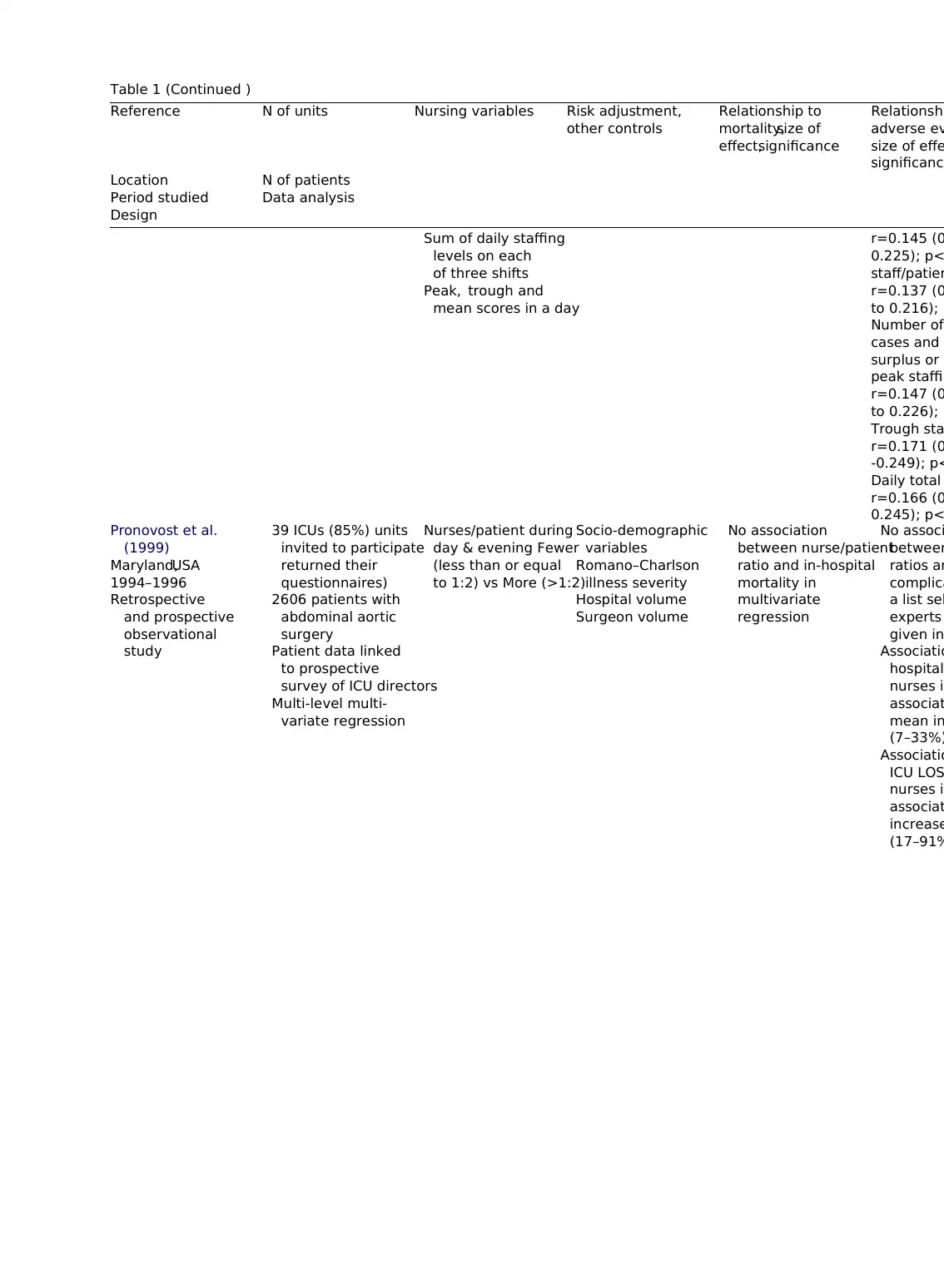
Table 1 (Continued )
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Sum of daily staffing
levels on each
of three shifts
Peak, trough and
mean scores in a day
r=0.145 (0
0.225); p<
staff/patien
r=0.137 (0
to 0.216); p
Number of
cases and
surplus or d
peak staffin
r=0.147 (0
to 0.226); p
Trough sta
r=0.171 (0
-0.249); p<
Daily total
r=0.166 (0
0.245); p<
Pronovost et al.
(1999)
Maryland,USA
1994–1996
Retrospective
and prospective
observational
study
39 ICUs (85%) units
invited to participate
returned their
questionnaires)
2606 patients with
abdominal aortic
surgery
Patient data linked
to prospective
survey of ICU directors
Multi-level multi-
variate regression
Nurses/patient during
day & evening Fewer
(less than or equal
to 1:2) vs More (>1:2)
Socio-demographic
variables
Romano–Charlson
illness severity
Hospital volume
Surgeon volume
No association
between nurse/patient
ratio and in-hospital
mortality in
multivariate
regression
No associ
between
ratios an
complica
a list sel
experts
given in
Associatio
hospital
nurses in
associat
mean in
(7–33%)
Associatio
ICU LOS
nurses in
associat
increase
(17–91%
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Sum of daily staffing
levels on each
of three shifts
Peak, trough and
mean scores in a day
r=0.145 (0
0.225); p<
staff/patien
r=0.137 (0
to 0.216); p
Number of
cases and
surplus or d
peak staffin
r=0.147 (0
to 0.226); p
Trough sta
r=0.171 (0
-0.249); p<
Daily total
r=0.166 (0
0.245); p<
Pronovost et al.
(1999)
Maryland,USA
1994–1996
Retrospective
and prospective
observational
study
39 ICUs (85%) units
invited to participate
returned their
questionnaires)
2606 patients with
abdominal aortic
surgery
Patient data linked
to prospective
survey of ICU directors
Multi-level multi-
variate regression
Nurses/patient during
day & evening Fewer
(less than or equal
to 1:2) vs More (>1:2)
Socio-demographic
variables
Romano–Charlson
illness severity
Hospital volume
Surgeon volume
No association
between nurse/patient
ratio and in-hospital
mortality in
multivariate
regression
No associ
between
ratios an
complica
a list sel
experts
given in
Associatio
hospital
nurses in
associat
mean in
(7–33%)
Associatio
ICU LOS
nurses in
associat
increase
(17–91%
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
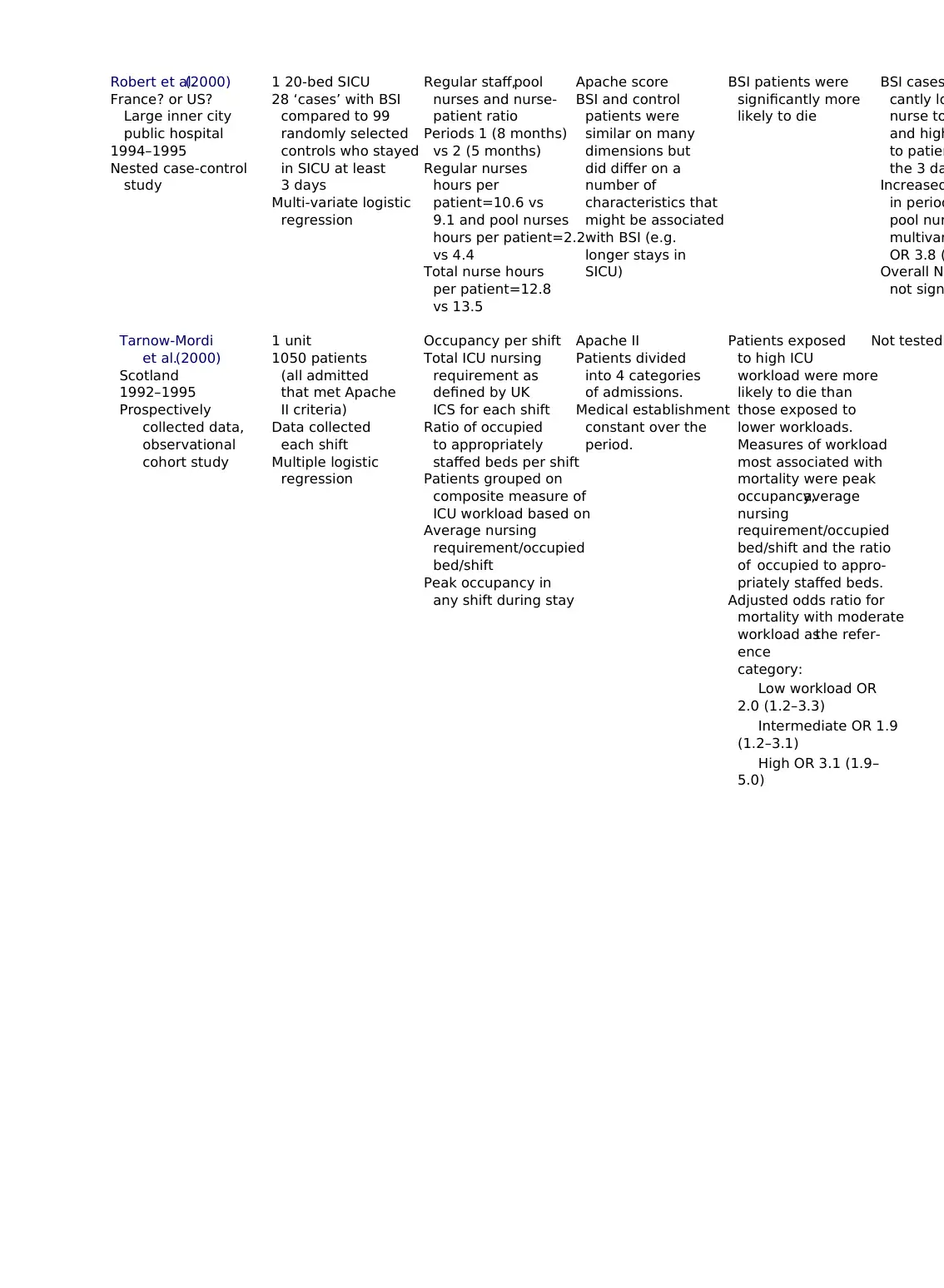
Robert et al.(2000)
France? or US?
Large inner city
public hospital
1994–1995
Nested case-control
study
1 20-bed SICU
28 ‘cases’ with BSI
compared to 99
randomly selected
controls who stayed
in SICU at least
3 days
Multi-variate logistic
regression
Regular staff,pool
nurses and nurse-
patient ratio
Periods 1 (8 months)
vs 2 (5 months)
Regular nurses
hours per
patient=10.6 vs
9.1 and pool nurses
hours per patient=2.2
vs 4.4
Total nurse hours
per patient=12.8
vs 13.5
Apache score
BSI and control
patients were
similar on many
dimensions but
did differ on a
number of
characteristics that
might be associated
with BSI (e.g.
longer stays in
SICU)
BSI patients were
significantly more
likely to die
BSI cases
cantly lo
nurse to
and high
to patien
the 3 da
Increased
in period
pool nur
multivar
OR 3.8 (
Overall N–
not sign
Tarnow-Mordi
et al.(2000)
Scotland
1992–1995
Prospectively
collected data,
observational
cohort study
1 unit
1050 patients
(all admitted
that met Apache
II criteria)
Data collected
each shift
Multiple logistic
regression
Occupancy per shift
Total ICU nursing
requirement as
defined by UK
ICS for each shift
Ratio of occupied
to appropriately
staffed beds per shift
Patients grouped on
composite measure of
ICU workload based on
Average nursing
requirement/occupied
bed/shift
Peak occupancy in
any shift during stay
Apache II
Patients divided
into 4 categories
of admissions.
Medical establishment
constant over the
period.
Patients exposed
to high ICU
workload were more
likely to die than
those exposed to
lower workloads.
Measures of workload
most associated with
mortality were peak
occupancy,average
nursing
requirement/occupied
bed/shift and the ratio
of occupied to appro-
priately staffed beds.
Adjusted odds ratio for
mortality with moderate
workload asthe refer-
ence
category:
Low workload OR
2.0 (1.2–3.3)
Intermediate OR 1.9
(1.2–3.1)
High OR 3.1 (1.9–
5.0)
Not tested
France? or US?
Large inner city
public hospital
1994–1995
Nested case-control
study
1 20-bed SICU
28 ‘cases’ with BSI
compared to 99
randomly selected
controls who stayed
in SICU at least
3 days
Multi-variate logistic
regression
Regular staff,pool
nurses and nurse-
patient ratio
Periods 1 (8 months)
vs 2 (5 months)
Regular nurses
hours per
patient=10.6 vs
9.1 and pool nurses
hours per patient=2.2
vs 4.4
Total nurse hours
per patient=12.8
vs 13.5
Apache score
BSI and control
patients were
similar on many
dimensions but
did differ on a
number of
characteristics that
might be associated
with BSI (e.g.
longer stays in
SICU)
BSI patients were
significantly more
likely to die
BSI cases
cantly lo
nurse to
and high
to patien
the 3 da
Increased
in period
pool nur
multivar
OR 3.8 (
Overall N–
not sign
Tarnow-Mordi
et al.(2000)
Scotland
1992–1995
Prospectively
collected data,
observational
cohort study
1 unit
1050 patients
(all admitted
that met Apache
II criteria)
Data collected
each shift
Multiple logistic
regression
Occupancy per shift
Total ICU nursing
requirement as
defined by UK
ICS for each shift
Ratio of occupied
to appropriately
staffed beds per shift
Patients grouped on
composite measure of
ICU workload based on
Average nursing
requirement/occupied
bed/shift
Peak occupancy in
any shift during stay
Apache II
Patients divided
into 4 categories
of admissions.
Medical establishment
constant over the
period.
Patients exposed
to high ICU
workload were more
likely to die than
those exposed to
lower workloads.
Measures of workload
most associated with
mortality were peak
occupancy,average
nursing
requirement/occupied
bed/shift and the ratio
of occupied to appro-
priately staffed beds.
Adjusted odds ratio for
mortality with moderate
workload asthe refer-
ence
category:
Low workload OR
2.0 (1.2–3.3)
Intermediate OR 1.9
(1.2–3.1)
High OR 3.1 (1.9–
5.0)
Not tested
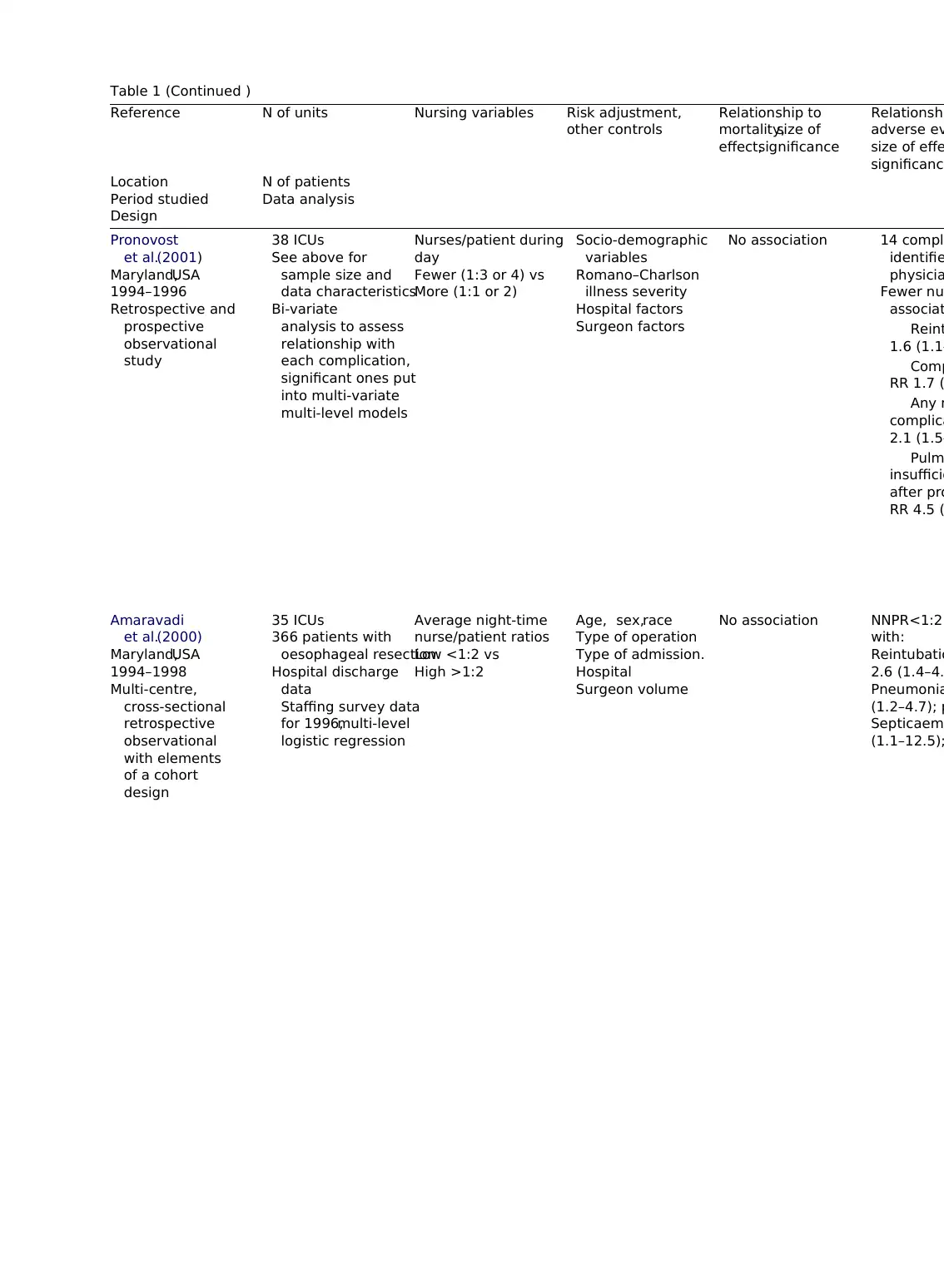
Table 1 (Continued )
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Pronovost
et al.(2001)
Maryland,USA
1994–1996
Retrospective and
prospective
observational
study
38 ICUs
See above for
sample size and
data characteristics
Bi-variate
analysis to assess
relationship with
each complication,
significant ones put
into multi-variate
multi-level models
Nurses/patient during
day
Fewer (1:3 or 4) vs
More (1:1 or 2)
Socio-demographic
variables
Romano–Charlson
illness severity
Hospital factors
Surgeon factors
No association 14 compli
identifie
physicia
Fewer nu
associat
Reint
1.6 (1.1–
Comp
RR 1.7 (
Any m
complica
2.1 (1.5–
Pulm
insufficie
after pro
RR 4.5 (
Amaravadi
et al.(2000)
Maryland,USA
1994–1998
Multi-centre,
cross-sectional
retrospective
observational
with elements
of a cohort
design
35 ICUs
366 patients with
oesophageal resection
Hospital discharge
data
Staffing survey data
for 1996,multi-level
logistic regression
Average night-time
nurse/patient ratios
Low <1:2 vs
High >1:2
Age, sex,race
Type of operation
Type of admission.
Hospital
Surgeon volume
No association NNPR<1:2
with:
Reintubatio
2.6 (1.4–4.
Pneumonia
(1.2–4.7); p
Septicaemi
(1.1–12.5);
Reference N of units Nursing variables Risk adjustment,
other controls
Relationship to
mortality,size of
effect,significance
Relationshi
adverse ev
size of effe
significance
Location N of patients
Period studied Data analysis
Design
Pronovost
et al.(2001)
Maryland,USA
1994–1996
Retrospective and
prospective
observational
study
38 ICUs
See above for
sample size and
data characteristics
Bi-variate
analysis to assess
relationship with
each complication,
significant ones put
into multi-variate
multi-level models
Nurses/patient during
day
Fewer (1:3 or 4) vs
More (1:1 or 2)
Socio-demographic
variables
Romano–Charlson
illness severity
Hospital factors
Surgeon factors
No association 14 compli
identifie
physicia
Fewer nu
associat
Reint
1.6 (1.1–
Comp
RR 1.7 (
Any m
complica
2.1 (1.5–
Pulm
insufficie
after pro
RR 4.5 (
Amaravadi
et al.(2000)
Maryland,USA
1994–1998
Multi-centre,
cross-sectional
retrospective
observational
with elements
of a cohort
design
35 ICUs
366 patients with
oesophageal resection
Hospital discharge
data
Staffing survey data
for 1996,multi-level
logistic regression
Average night-time
nurse/patient ratios
Low <1:2 vs
High >1:2
Age, sex,race
Type of operation
Type of admission.
Hospital
Surgeon volume
No association NNPR<1:2
with:
Reintubatio
2.6 (1.4–4.
Pneumonia
(1.2–4.7); p
Septicaemi
(1.1–12.5);
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 19
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.