Nursing Priorities: Status Asthmaticus - Simon's Case Study Analysis
VerifiedAdded on 2023/01/19
|23
|3456
|77
Essay
AI Summary
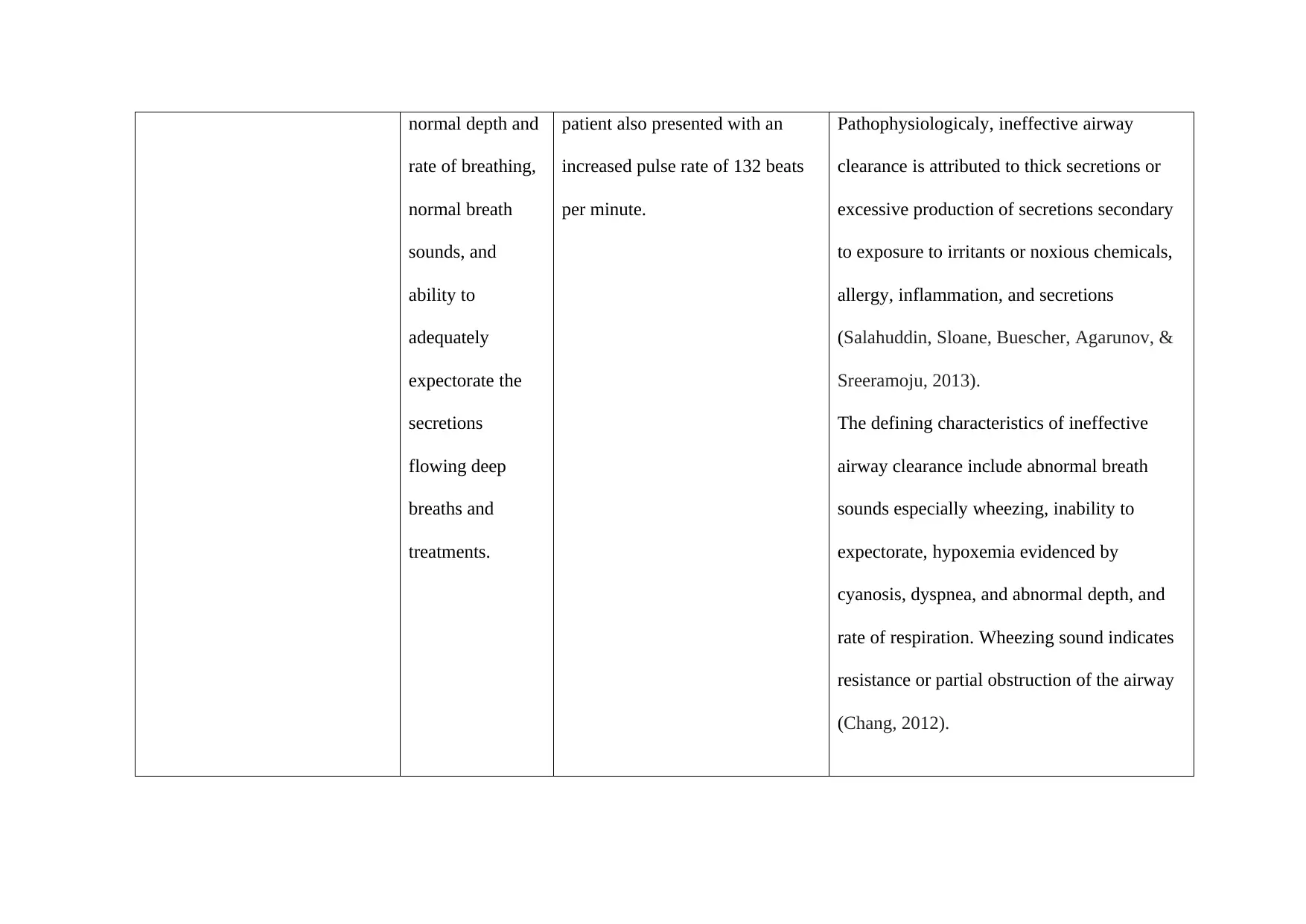
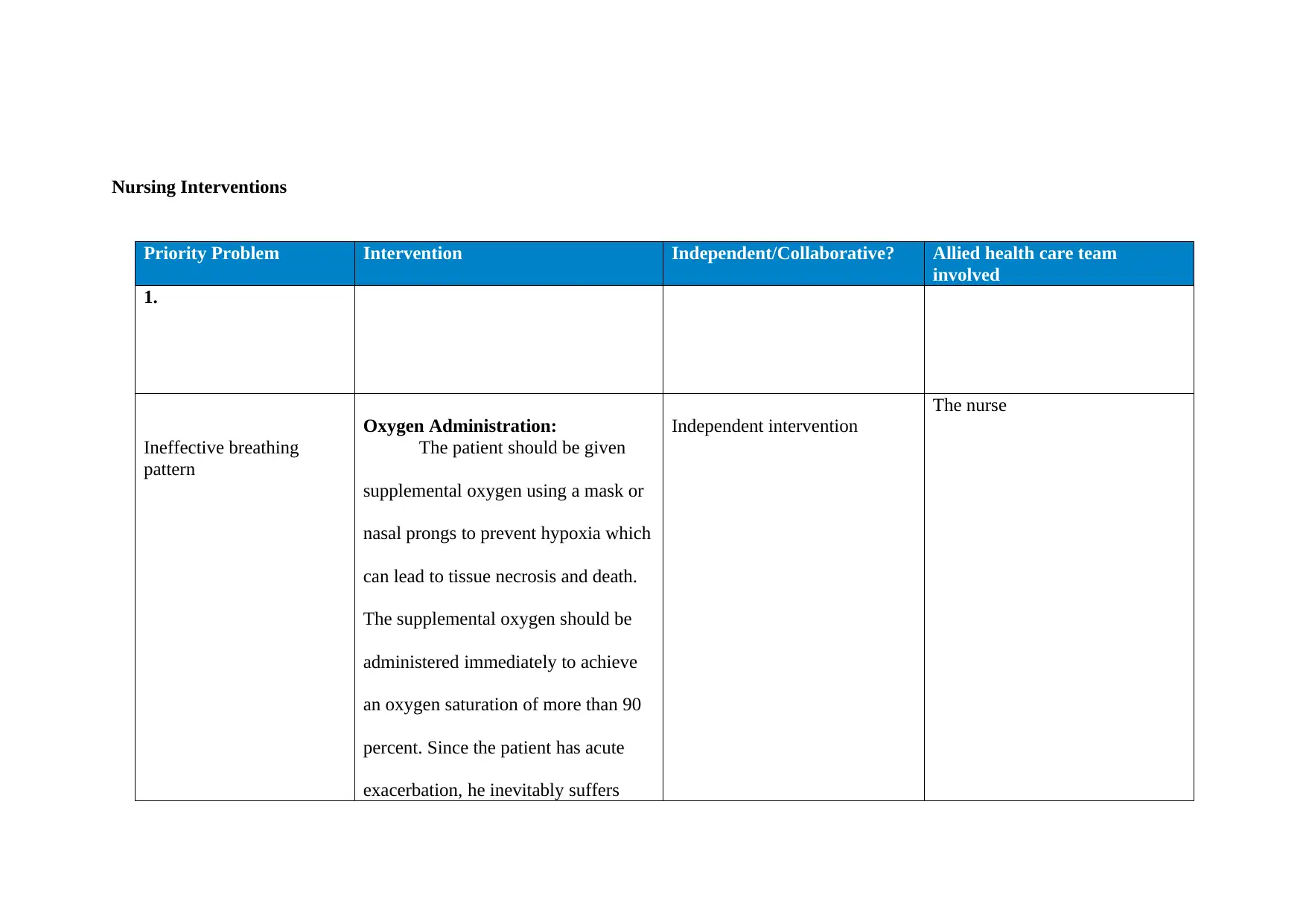
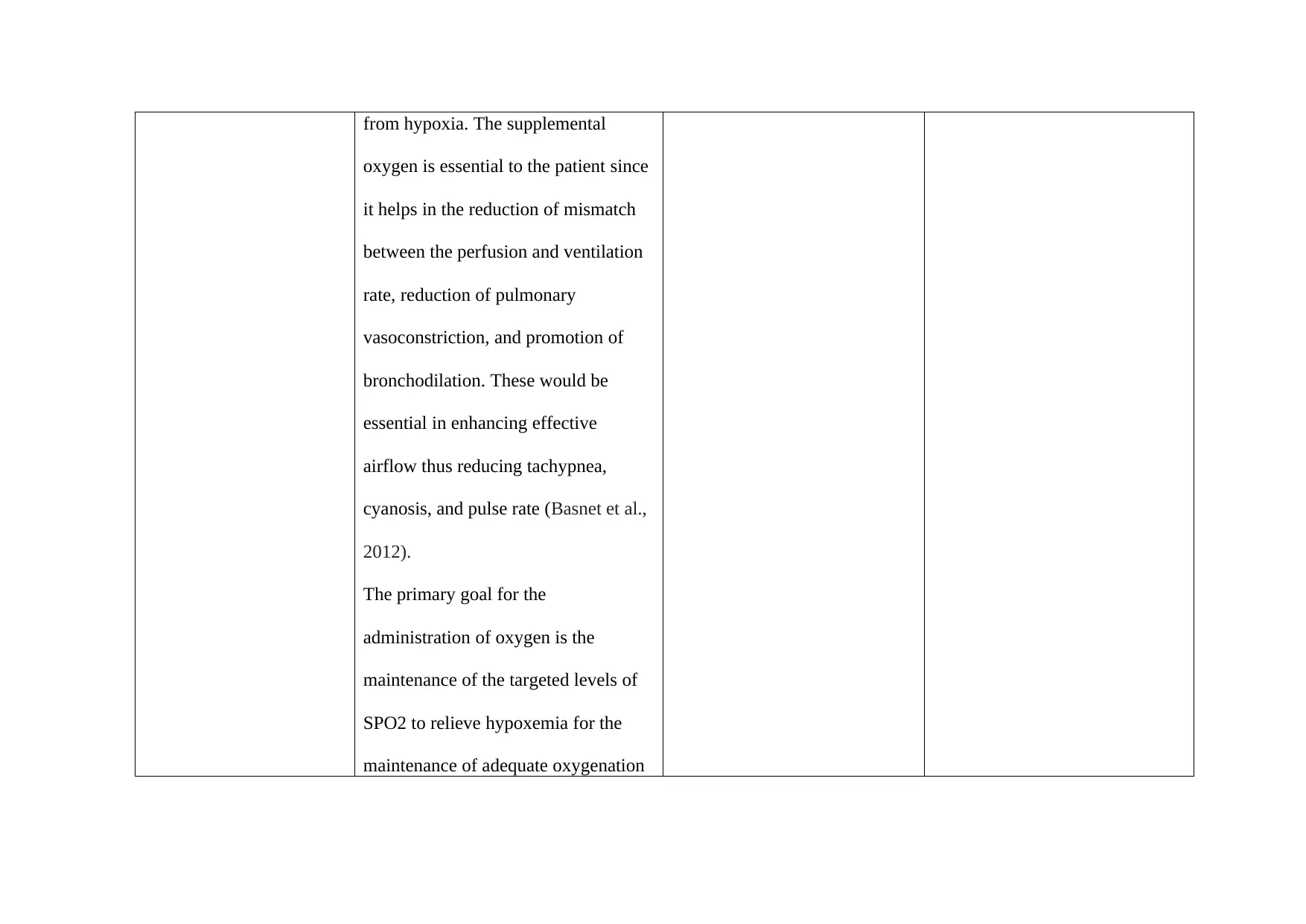
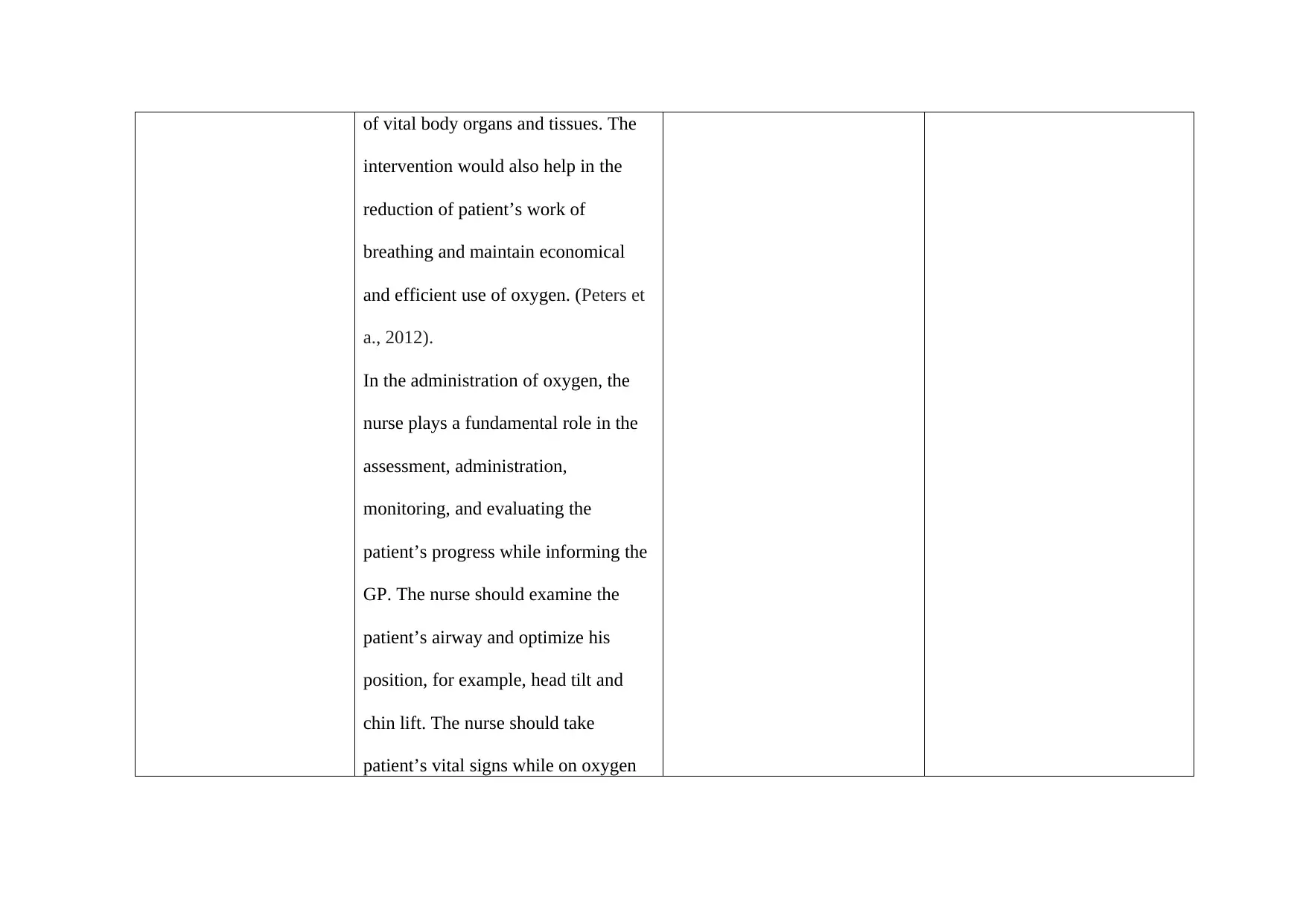
This essay provides a comprehensive analysis of nursing priorities in the case of a 14-year-old patient, Simon, experiencing status asthmaticus. It begins with an introduction to the condition, its pathophysiology, and the role of the nurse in patient care. The essay identifies and discusses two critical priority problems: ineffective breathing pattern and ineffective airway clearance. For each problem, it outlines specific assessment data, the underlying pathophysiology, and two major interventions, including both independent and collaborative approaches. The independent interventions include oxygen administration and controlled breathing exercises/patient positioning and education, while the collaborative interventions involve the administration of medications like Albuterol and Hydrocortisone, detailing their actions, dosages, precautions, and the nurse's responsibilities. The essay emphasizes the importance of a holistic approach, integrating both pharmacological and non-pharmacological interventions to improve patient outcomes and prevent complications associated with severe asthma exacerbations.

1 out of 23
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.