Nutrition Program and Proposal: Childhood Obesity Intervention
VerifiedAdded on 2022/09/08
|10
|2400
|55
Project
AI Summary
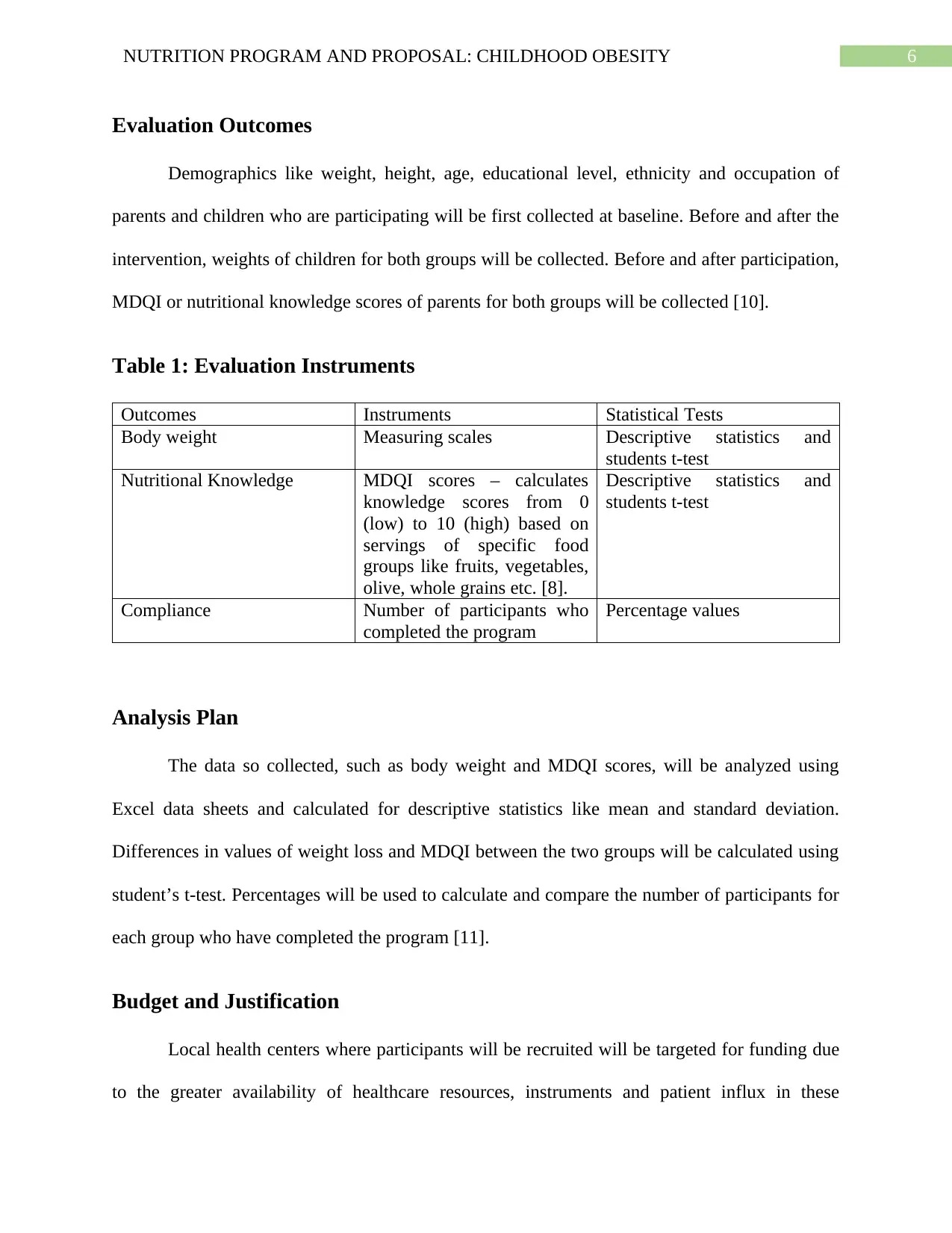
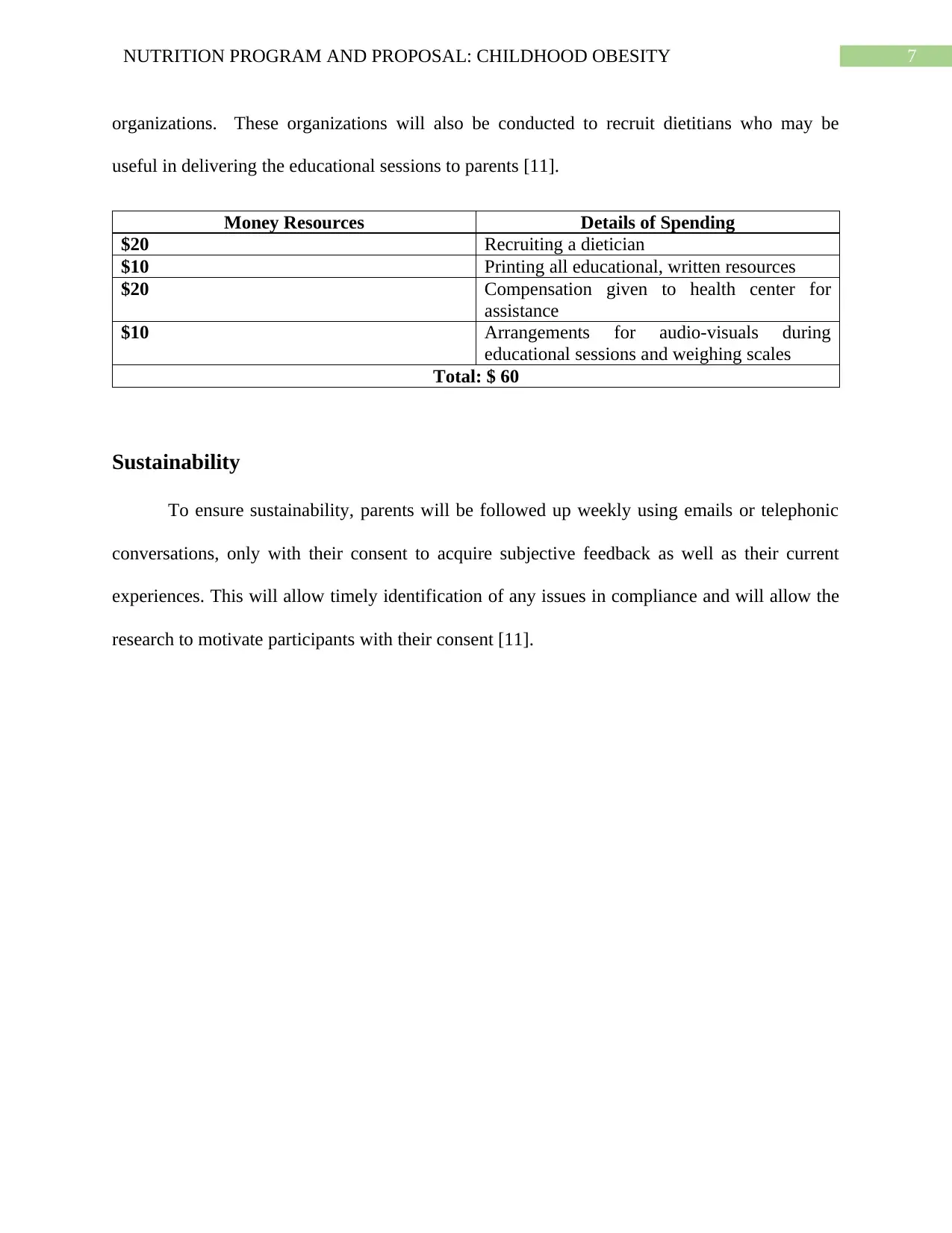
This program proposal outlines a comprehensive nutrition program designed to address childhood obesity through a randomized controlled trial. The program aims to involve both children and parents in educational and behavioral interventions, leveraging the trans-theoretical model of change. The study hypothesizes that a program involving both parents and children will lead to greater weight loss, improved nutritional knowledge, and better compliance compared to a program involving only children. The research design includes two groups: a control group receiving written nutritional guidelines and an experimental group participating in interactive educational sessions with pictorial and written resources. The study will evaluate weight loss, nutritional knowledge (using the MDQI), and program compliance over a three-month period. The sample size is estimated to be 68 participants, and recruitment will occur through weight loss centers, gyms, and diet clinics. The budget includes expenses for a dietician, educational resources, and incentives. Sustainability will be ensured through weekly follow-ups with parents to gather feedback and address any issues. The study references various research papers to support the program's rationale and methodology, with the overall goal of combating the rising rates of childhood obesity.


1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.