Health Promotion Assignment: Obesity, Determinants, and Local Plans
VerifiedAdded on 2023/01/18
|12
|2890
|68
Report
AI Summary
This report addresses obesity as a significant health concern, particularly among individuals with low socioeconomic status, examining its prevalence, causes, and consequences. It explores the determinants of health contributing to obesity, including lack of access to nutritious food, limited physical activity, and inadequate education and healthcare. The report analyzes the Living Well Latrobe Council Municipal Public Health and Wellbeing Plan 2017-2021, assessing its strategies to address obesity by promoting healthy eating, increasing physical activity, and improving community health and wellbeing. It identifies gaps in the plan, such as the lack of health education regarding physical activities, and highlights the plan's strengths in promoting physical activity and access to nutritious foods. The report concludes by emphasizing the urgent need for action to combat obesity through interventions addressing the identified determinants, with a focus on improving access to resources and education for vulnerable populations.

Running head: HEALTH PROMOTION 1
Health Promotion
Students Name
Institutional Affiliation
Health Promotion
Students Name
Institutional Affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH PROMOTION 2
Introduction
Obesity is a growing health concern that needs urgent attention due to the severe health
effects it has on both individuals and the community. Obesity leads to increased morbidity and
mortality from cardiovascular diseases. Secondly, it is one of the leading causes of hypertension
which can result in heart failure, stroke, congestive heart failure, and coronary heart diseases.
Lastly, obesity can lead to certain types of cancers and respiratory disorders. Obesity is more
prevalent among people with low socio-economic status. This is attributed to limited access to
quality foods, lack of education, lack of access to healthcare and lack of physical activities. The
Living Well Latrobe Council Municipal Public Health and Wellbeing Plan 2017-2021 is keen on
ensuring that there are reduced cased of obesity and that people live healthy lives. For instance, it
is keen on increasing access to quality food and ensuring increased physical activities by creating
more affordable physical activity and sporting options.
Obesity
Obesity is a medical condition where an individual carries excess body fat or weight that
can have an adverse effect on one’s health (Bogart 2013, pp.31–69). Globally, there has been an
increased prevalence of obesity to the extent that it has now become a global health challenge.
According to the WHO, the number of people with obesity has tripled between 1975 and 2016.
This is attributed to the lack of physical activities, genetics, and consumption of unhealthy foods.
In 2016, an estimated 1.9billion adults who were 18 years and older were overweight while
650million of these adults were obese. In 2016, 13% of adults aged 18 years and above were
obese while 39% were overweight (World Health Organization, 2016).
Introduction
Obesity is a growing health concern that needs urgent attention due to the severe health
effects it has on both individuals and the community. Obesity leads to increased morbidity and
mortality from cardiovascular diseases. Secondly, it is one of the leading causes of hypertension
which can result in heart failure, stroke, congestive heart failure, and coronary heart diseases.
Lastly, obesity can lead to certain types of cancers and respiratory disorders. Obesity is more
prevalent among people with low socio-economic status. This is attributed to limited access to
quality foods, lack of education, lack of access to healthcare and lack of physical activities. The
Living Well Latrobe Council Municipal Public Health and Wellbeing Plan 2017-2021 is keen on
ensuring that there are reduced cased of obesity and that people live healthy lives. For instance, it
is keen on increasing access to quality food and ensuring increased physical activities by creating
more affordable physical activity and sporting options.
Obesity
Obesity is a medical condition where an individual carries excess body fat or weight that
can have an adverse effect on one’s health (Bogart 2013, pp.31–69). Globally, there has been an
increased prevalence of obesity to the extent that it has now become a global health challenge.
According to the WHO, the number of people with obesity has tripled between 1975 and 2016.
This is attributed to the lack of physical activities, genetics, and consumption of unhealthy foods.
In 2016, an estimated 1.9billion adults who were 18 years and older were overweight while
650million of these adults were obese. In 2016, 13% of adults aged 18 years and above were
obese while 39% were overweight (World Health Organization, 2016).
HEALTH PROMOTION 3
Although obesity was once considered to be a problem only in high-income countries, it
is now more prevalent in low and middle-income countries. In Africa for instance, the number of
obese children under the age of 5 has increased by approximately 50% since 2000. In 2016, an
estimated 41million children aged below 5 were obese or overweight (World Health
Organization, 2016). In 2016, more than 340 million adolescents and children aged 5-19 were
either obese or overweight. Among these, 18% were girls while 19% were boys. The prevalence
of obesity and overweight among adolescents and children has increased from 4% to 18%
between 1975 and 2016 (Seidell and Halberstadt 2015, pp.7-12).
In Australia, approximately 67.0% of the adults aged 18 and over were obese or
overweight in 2017-2018. This is an estimated two-thirds of the whole population. Among these,
35.6% were overweight while 31.3% were obese. Since 2014-2015, the number of adults aged 18
years and above with obesity has increased from 63.4% to 67.0%. Since 1995, the number of
adults with obesity has increased from 56.2% to 67.0%. In 2017-2018, the proportion of men
who were obese or overweight was 74.5% while that of women was 59.7%. Since 2014-2015,
the number of obese men and women has increased. The number of obese men changed from
28.4% to 32.5% while that of women increased from 27.4% to 30.2% (Australian Bureau of
Statistics 2015).
In 2014-2015, an estimated 63.4% of Australians aged 18 years and above were
overweight or obese which translates to 11.2 million people. 35.5% of the 6.3 million people
were overweight while 27.9% were obese. 35.0% had a normal weight while 1.6% were
underweight. Research indicates that the number of obese people in Australia is likely to increase
in the future. It is expected that by 2025, the number of men and women aged 20 years and
Although obesity was once considered to be a problem only in high-income countries, it
is now more prevalent in low and middle-income countries. In Africa for instance, the number of
obese children under the age of 5 has increased by approximately 50% since 2000. In 2016, an
estimated 41million children aged below 5 were obese or overweight (World Health
Organization, 2016). In 2016, more than 340 million adolescents and children aged 5-19 were
either obese or overweight. Among these, 18% were girls while 19% were boys. The prevalence
of obesity and overweight among adolescents and children has increased from 4% to 18%
between 1975 and 2016 (Seidell and Halberstadt 2015, pp.7-12).
In Australia, approximately 67.0% of the adults aged 18 and over were obese or
overweight in 2017-2018. This is an estimated two-thirds of the whole population. Among these,
35.6% were overweight while 31.3% were obese. Since 2014-2015, the number of adults aged 18
years and above with obesity has increased from 63.4% to 67.0%. Since 1995, the number of
adults with obesity has increased from 56.2% to 67.0%. In 2017-2018, the proportion of men
who were obese or overweight was 74.5% while that of women was 59.7%. Since 2014-2015,
the number of obese men and women has increased. The number of obese men changed from
28.4% to 32.5% while that of women increased from 27.4% to 30.2% (Australian Bureau of
Statistics 2015).
In 2014-2015, an estimated 63.4% of Australians aged 18 years and above were
overweight or obese which translates to 11.2 million people. 35.5% of the 6.3 million people
were overweight while 27.9% were obese. 35.0% had a normal weight while 1.6% were
underweight. Research indicates that the number of obese people in Australia is likely to increase
in the future. It is expected that by 2025, the number of men and women aged 20 years and
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH PROMOTION 4
above will increase by 83% and 75% respectively. It is also projected that there will be 16.9
million obese and overweight Australians by 2025 (Australian Bureau of Statistics 2015).
In Victoria, there has been an increase in the number of people who are either obese or
overweight. An estimated one in four adults is now obese in Victoria. In 2017-2018, the number
of obese or overweight people increased from 63.3% to 68.3%. In 2014-2015, 37.1%
(1.7million) of the adults aged 18 years and above were overweight. In the same year, 26.4%
(1.2million) adults were obese. 63.3% (2.9 million) people were obese or overweight. In 2014-
2015, 21.9% (248,400) children aged between 2-17 years were overweight. 7.3% (82,900)
children were obese. 28.6% (324,500) children were obese or overweight (Department of Health
and Human Services Victoria 2015, pp.1–63).
Obesity is a serious health concern that has led to increased morbidity and mortality from
obesity-related illnesses. According to the World Health Organization, globally an estimated 2.8
million people die annually as a result of being obese or overweight. Approximately 2.3% of
global DALYs are due to overweight or obesity. In 2011, 5% of the burden of disease was due to
overweight or obesity. In Victoria, obesity is one of the leading causes of poor health and
preventable deaths (World Health Organization 2016).
Obesity has a significant impact on the health of an individual and population. A high
body mass index is associated with increased cardiovascular risk as well as high cardiovascular
morbidity. Secondly, obesity can also result to hypertension which can then increase the risks of
kidney disease, heart failure, stroke, coronary heart diseases and congestive heart failure (De
Schutter Lavie and Milani 2014, pp.401-408). Thirdly, obesity can also lead to heart disease
which is one of the leading cause of mortality. Studies indicate that the risk of heart disease
above will increase by 83% and 75% respectively. It is also projected that there will be 16.9
million obese and overweight Australians by 2025 (Australian Bureau of Statistics 2015).
In Victoria, there has been an increase in the number of people who are either obese or
overweight. An estimated one in four adults is now obese in Victoria. In 2017-2018, the number
of obese or overweight people increased from 63.3% to 68.3%. In 2014-2015, 37.1%
(1.7million) of the adults aged 18 years and above were overweight. In the same year, 26.4%
(1.2million) adults were obese. 63.3% (2.9 million) people were obese or overweight. In 2014-
2015, 21.9% (248,400) children aged between 2-17 years were overweight. 7.3% (82,900)
children were obese. 28.6% (324,500) children were obese or overweight (Department of Health
and Human Services Victoria 2015, pp.1–63).
Obesity is a serious health concern that has led to increased morbidity and mortality from
obesity-related illnesses. According to the World Health Organization, globally an estimated 2.8
million people die annually as a result of being obese or overweight. Approximately 2.3% of
global DALYs are due to overweight or obesity. In 2011, 5% of the burden of disease was due to
overweight or obesity. In Victoria, obesity is one of the leading causes of poor health and
preventable deaths (World Health Organization 2016).
Obesity has a significant impact on the health of an individual and population. A high
body mass index is associated with increased cardiovascular risk as well as high cardiovascular
morbidity. Secondly, obesity can also result to hypertension which can then increase the risks of
kidney disease, heart failure, stroke, coronary heart diseases and congestive heart failure (De
Schutter Lavie and Milani 2014, pp.401-408). Thirdly, obesity can also lead to heart disease
which is one of the leading cause of mortality. Studies indicate that the risk of heart disease
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH PROMOTION 5
increases with obesity. Individuals with severe obesity have a high risk of developing coronary
artery disease which means that they also have an increased risk of heart attack. Fourthly, obesity
can lead to certain types of cancers. Studies indicate that obesity can cause up to an estimated
90,000 cancer deaths annually. Lastly, obesity can lead to respiratory disorders (GBD 2015
Obesity Collaborators, 2017, pp.13-27).
The individual costs of obesity include poor physical functioning as well as limitations in
daily life. They may also face job and insurance discrimination due to the stigma and disabilities
associated with the condition. The economic costs include loss of productivity and a high cost of
diagnosis and treatment of the illnesses related to obesity (Goldberg 2011, p.788).
Obesity among people with low socioeconomic status
The vulnerable population most affected by obesity are the people with low
socioeconomic status (How Obesity Relates to Socioeconomic Status 2016). This because people
with low socio-economic status lack enough income to buy healthy foods and poor diets. It is
well known that proper nutrition and feeding is vital for proper growth and good health.
Previously, obesity was associated with people with high income. However recently, obesity has
become a challenge among the low-income people due to lack of quality food as well as poor
diets. This is because the poor lack enough resources to have access to quality and healthy foods
(Gordon-Larsen 2014, pp.809-817).
People from low socio-economic backgrounds lack enough resources to go to the fitness
centers as compared to those with high incomes (Chin, Kahathuduwa & Binks 2016, pp.1226–
1244). Most of the people from low-income families are less educated. This means that they lack
enough knowledge to adopt healthy eating habits. Proper education is associated with eating
increases with obesity. Individuals with severe obesity have a high risk of developing coronary
artery disease which means that they also have an increased risk of heart attack. Fourthly, obesity
can lead to certain types of cancers. Studies indicate that obesity can cause up to an estimated
90,000 cancer deaths annually. Lastly, obesity can lead to respiratory disorders (GBD 2015
Obesity Collaborators, 2017, pp.13-27).
The individual costs of obesity include poor physical functioning as well as limitations in
daily life. They may also face job and insurance discrimination due to the stigma and disabilities
associated with the condition. The economic costs include loss of productivity and a high cost of
diagnosis and treatment of the illnesses related to obesity (Goldberg 2011, p.788).
Obesity among people with low socioeconomic status
The vulnerable population most affected by obesity are the people with low
socioeconomic status (How Obesity Relates to Socioeconomic Status 2016). This because people
with low socio-economic status lack enough income to buy healthy foods and poor diets. It is
well known that proper nutrition and feeding is vital for proper growth and good health.
Previously, obesity was associated with people with high income. However recently, obesity has
become a challenge among the low-income people due to lack of quality food as well as poor
diets. This is because the poor lack enough resources to have access to quality and healthy foods
(Gordon-Larsen 2014, pp.809-817).
People from low socio-economic backgrounds lack enough resources to go to the fitness
centers as compared to those with high incomes (Chin, Kahathuduwa & Binks 2016, pp.1226–
1244). Most of the people from low-income families are less educated. This means that they lack
enough knowledge to adopt healthy eating habits. Proper education is associated with eating
HEALTH PROMOTION 6
healthy foods and engaging in physical activities. Lack of access to health care has also increased
the rate of obesity among the poor. This is because they fail to get health education regarding the
types of foods they should take as well. They also lack timely treatment for the condition
(Eisenberg and Burgess 2015, pp.854-860).
The environmental factors that lead to increased obesity among people from low-income
families include the fact that they lack enough space and land to engage in physical activities.
This is because they live in squeezed areas where land is limited (Evans Wells & Schamberg,
2010, pp.713–725). The political factors that lead to increased obesity among people with low
income include the lack of political goodwill to improve access to quality and nutritious foods
among the poor. It also includes lack of political goodwill to create public spaces where the
community may engage in physical activities (Zukiewicz-Sobczak et al. 2014).
healthy foods and engaging in physical activities. Lack of access to health care has also increased
the rate of obesity among the poor. This is because they fail to get health education regarding the
types of foods they should take as well. They also lack timely treatment for the condition
(Eisenberg and Burgess 2015, pp.854-860).
The environmental factors that lead to increased obesity among people from low-income
families include the fact that they lack enough space and land to engage in physical activities.
This is because they live in squeezed areas where land is limited (Evans Wells & Schamberg,
2010, pp.713–725). The political factors that lead to increased obesity among people with low
income include the lack of political goodwill to improve access to quality and nutritious foods
among the poor. It also includes lack of political goodwill to create public spaces where the
community may engage in physical activities (Zukiewicz-Sobczak et al. 2014).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH PROMOTION 7
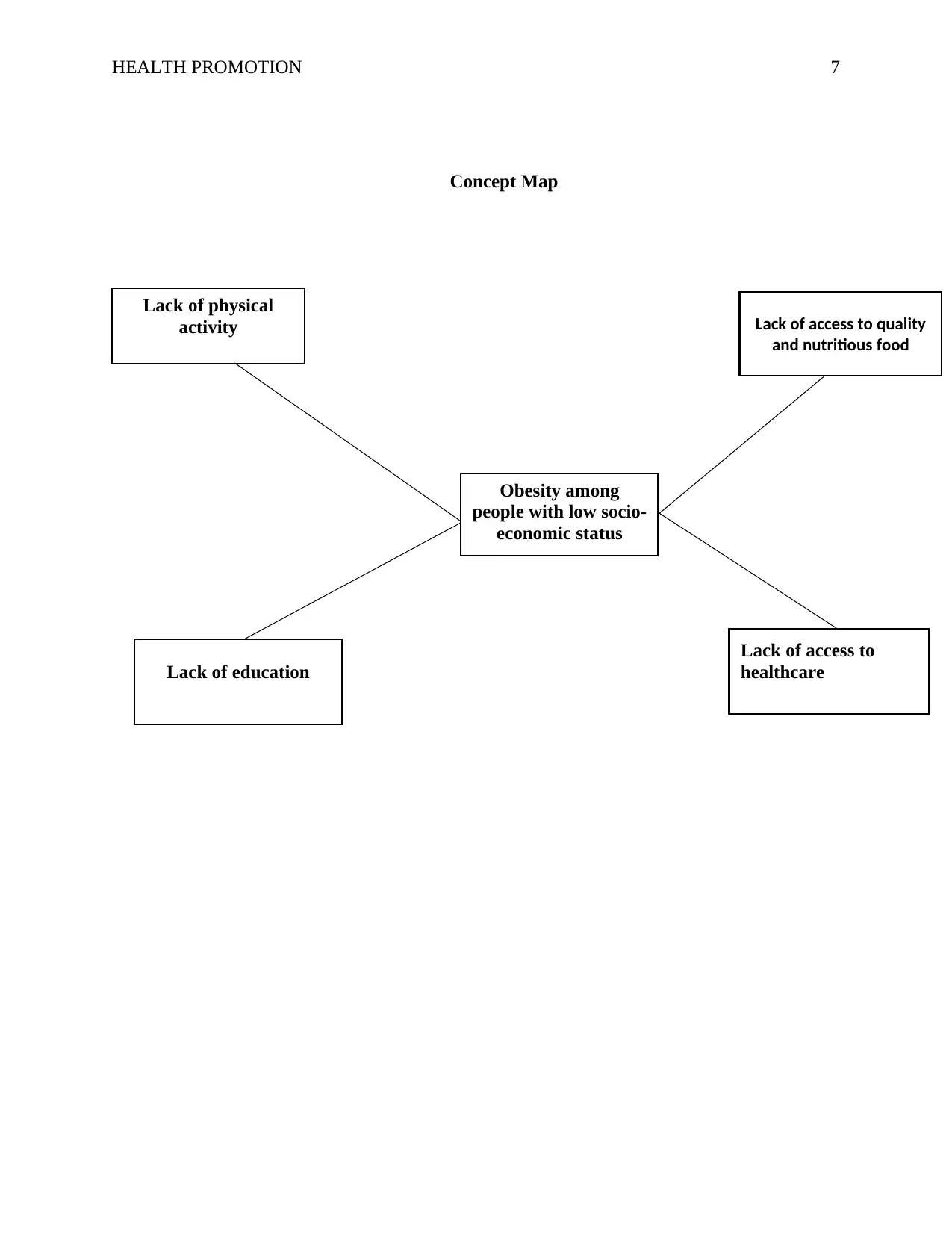
Concept Map
Lack of access to quality
and nutritious food
Lack of physical
activity
Lack of education
Lack of access to
healthcare
Obesity among
people with low socio-
economic status
Concept Map
Lack of access to quality
and nutritious food
Lack of physical
activity
Lack of education
Lack of access to
healthcare
Obesity among
people with low socio-
economic status
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH PROMOTION 8
The Living Well Latrobe council Municipal Public Health and Wellbeing Plan 2017-
2021
The Living Well Latrobe council Municipal Public Health and Wellbeing Plan 2017-
2021 is keen on ensuring a healthy, safe and connected community. The issue of obesity among
the people from low socio-economic status backgrounds has been integrated into the plan where
it is indicated that their focus is active living, improving the health and wellbeing of the people
and increasing lifelong learning and opportunities (Living Well Latrobe 2017, pp.3–23).
The MPHWP addresses the determinants of health that increase obesity cases among
people with low income. For instance, it has focused on ways to be active at school and work.
Secondly, it has focused on the built environments that encourage more physical activities such
as walking. Thirdly, it is keen on investing in infrastructure that gives low-cost physical activities
that can be used by everyone in the community to increase physical activity (Ren 2016).
Fourthly, it has focused on many affordable physical activity and sporting options with various
sporting organizations and clubs. It is keen on encouraging participation in physical activity
among the multicultural community, women, Aboriginal and Torres Island people, the seniors
and people living with a disability. Lastly, it has concentrated on ensuring that there are cheaper
physical activity facilities to encourage people to cycle and walk (Living Well Latrobe 2017,
pp.3–23).
The MPHWP is also keen on encouraging the health and wellbeing of the people by
focusing on increasing availability, access and consumption of healthy foods and drinks. This is
an important step in reducing the cases of obesity. Secondly, it has focused on supporting
community food initiatives which include encouraging the use of food swaps and community
The Living Well Latrobe council Municipal Public Health and Wellbeing Plan 2017-
2021
The Living Well Latrobe council Municipal Public Health and Wellbeing Plan 2017-
2021 is keen on ensuring a healthy, safe and connected community. The issue of obesity among
the people from low socio-economic status backgrounds has been integrated into the plan where
it is indicated that their focus is active living, improving the health and wellbeing of the people
and increasing lifelong learning and opportunities (Living Well Latrobe 2017, pp.3–23).
The MPHWP addresses the determinants of health that increase obesity cases among
people with low income. For instance, it has focused on ways to be active at school and work.
Secondly, it has focused on the built environments that encourage more physical activities such
as walking. Thirdly, it is keen on investing in infrastructure that gives low-cost physical activities
that can be used by everyone in the community to increase physical activity (Ren 2016).
Fourthly, it has focused on many affordable physical activity and sporting options with various
sporting organizations and clubs. It is keen on encouraging participation in physical activity
among the multicultural community, women, Aboriginal and Torres Island people, the seniors
and people living with a disability. Lastly, it has concentrated on ensuring that there are cheaper
physical activity facilities to encourage people to cycle and walk (Living Well Latrobe 2017,
pp.3–23).
The MPHWP is also keen on encouraging the health and wellbeing of the people by
focusing on increasing availability, access and consumption of healthy foods and drinks. This is
an important step in reducing the cases of obesity. Secondly, it has focused on supporting
community food initiatives which include encouraging the use of food swaps and community
HEALTH PROMOTION 9
gardens. Lastly, it has developed partnerships that can help address the causes of food insecurity
with the main focus on improving access to healthy food, supporting local producers and
improving health education concerning healthy eating (Living Well Latrobe 2017, pp.3–23).
The MPHWP has focused on increasing lifelong learning and opportunities to help
reduce poverty and unemployment rates. For instance, it has focused on growing, promoting and
supporting program and services that increase digital and financial literacy. Secondly, it has
focused on recognizing that employment is key to ensuring the health and wellbeing of a
community. Thirdly, it has supported the community in ensuring that they build enough skills
that they can use in the job market. Lastly, it has created and promoted clear local pathways from
education and skills training to employment opportunities (Living Well Latrobe 2017, pp.3–23).
The gaps present in the MPHWP include the fact that it has not incorporated the aspect of
offering health education concerning physical activities to reduce obesity. It has also not focused
on access to health care services. The strengths of the MPHWP is that it has focused mainly on
improving physical activities and access to nutritious foods. It has focused on creating built
environments that increase physical activities. It has also established cheaper physical activity
facilities (Living Well Latrobe 2017, pp.3–23).
gardens. Lastly, it has developed partnerships that can help address the causes of food insecurity
with the main focus on improving access to healthy food, supporting local producers and
improving health education concerning healthy eating (Living Well Latrobe 2017, pp.3–23).
The MPHWP has focused on increasing lifelong learning and opportunities to help
reduce poverty and unemployment rates. For instance, it has focused on growing, promoting and
supporting program and services that increase digital and financial literacy. Secondly, it has
focused on recognizing that employment is key to ensuring the health and wellbeing of a
community. Thirdly, it has supported the community in ensuring that they build enough skills
that they can use in the job market. Lastly, it has created and promoted clear local pathways from
education and skills training to employment opportunities (Living Well Latrobe 2017, pp.3–23).
The gaps present in the MPHWP include the fact that it has not incorporated the aspect of
offering health education concerning physical activities to reduce obesity. It has also not focused
on access to health care services. The strengths of the MPHWP is that it has focused mainly on
improving physical activities and access to nutritious foods. It has focused on creating built
environments that increase physical activities. It has also established cheaper physical activity
facilities (Living Well Latrobe 2017, pp.3–23).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH PROMOTION 10
Conclusion
In conclusion, obesity among people from low socio-economic families is a worldwide
growing concern that needs urgent action. The factors that have increased the number of people
with obesity among the low-income people include lack of physical activities which is due to
congestion and lack of public spaces where they can walk, cycle, run or exercise. Secondly, they
lack access to quality and nutritious food due to lack of enough income. Thirdly they are also
less educated, and hence they lack knowledge on the importance of physical activities and
consuming healthy foods. The determinants of health that increase obesity among the low-
income people have been well addressed in The Living Well Latrobe council Municipal Public
Health and Wellbeing Plan 2017-2021. For instance, the plan has outlined how it intends to
improve access to healthy foods and encourage physical activities. It has also outlined how it
plans to empower people and enhance employment opportunities to fight poverty.
References
Conclusion
In conclusion, obesity among people from low socio-economic families is a worldwide
growing concern that needs urgent action. The factors that have increased the number of people
with obesity among the low-income people include lack of physical activities which is due to
congestion and lack of public spaces where they can walk, cycle, run or exercise. Secondly, they
lack access to quality and nutritious food due to lack of enough income. Thirdly they are also
less educated, and hence they lack knowledge on the importance of physical activities and
consuming healthy foods. The determinants of health that increase obesity among the low-
income people have been well addressed in The Living Well Latrobe council Municipal Public
Health and Wellbeing Plan 2017-2021. For instance, the plan has outlined how it intends to
improve access to healthy foods and encourage physical activities. It has also outlined how it
plans to empower people and enhance employment opportunities to fight poverty.
References
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH PROMOTION 11
Australian Bureau of Statistics, 2015 Australian Government- Victoria. Available at:
https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by Subject/4364.0.55.001~2014-
15~Main Features~Victoria~10003 [Accessed April 14, 2019].
Australian Bureau of Statistics, 2015. National health survey: First results, 2014–15. ABS Cat.
No. 4364.0. 55.001).
Bogart, W.A., 2013. How Is Obesity a Problem? Regulating Obesity?, pp.31–69.
Chin, S.-H., Kahathuduwa, C.N. & Binks, M., 2016. Physical activity and obesity: what we
know and what we need to know*. Obesity Reviews, 17(12), pp.1226–1244.
De Schutter, A., Lavie, C.J. and Milani, R.V., 2014. The impact of obesity on risk factors and
prevalence and prognosis of coronary heart disease—the obesity paradox. Progress in
cardiovascular diseases, 56(4), pp.401-408.
Department of Health and Human Services Victoria, 2015. Victorian public health and wellbeing
plan 2015–2019. , pp.1–63. Available at: https://www2.health.vic.gov.au/about/health-
strategies/public-health-wellbeing-plan/action-plan-update.
Eisenberg, D.M. and Burgess, J.D., 2015. Nutrition education in an era of global obesity and
diabetes: thinking outside the box. Academic Medicine, 90(7), pp.854-860.
Evans, G.W., Wells, N.M. & Schamberg, M.A., 2010. The Role of the Environment in Socio-
Economic Status and Obesity. Obesity Prevention, pp.713–725.
GBD 2015 Obesity Collaborator., 2017. Health effects of overweight and obesity in 195
countries over 25 years. New England Journal of Medicine, 377(1), pp.13-27.
Australian Bureau of Statistics, 2015 Australian Government- Victoria. Available at:
https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by Subject/4364.0.55.001~2014-
15~Main Features~Victoria~10003 [Accessed April 14, 2019].
Australian Bureau of Statistics, 2015. National health survey: First results, 2014–15. ABS Cat.
No. 4364.0. 55.001).
Bogart, W.A., 2013. How Is Obesity a Problem? Regulating Obesity?, pp.31–69.
Chin, S.-H., Kahathuduwa, C.N. & Binks, M., 2016. Physical activity and obesity: what we
know and what we need to know*. Obesity Reviews, 17(12), pp.1226–1244.
De Schutter, A., Lavie, C.J. and Milani, R.V., 2014. The impact of obesity on risk factors and
prevalence and prognosis of coronary heart disease—the obesity paradox. Progress in
cardiovascular diseases, 56(4), pp.401-408.
Department of Health and Human Services Victoria, 2015. Victorian public health and wellbeing
plan 2015–2019. , pp.1–63. Available at: https://www2.health.vic.gov.au/about/health-
strategies/public-health-wellbeing-plan/action-plan-update.
Eisenberg, D.M. and Burgess, J.D., 2015. Nutrition education in an era of global obesity and
diabetes: thinking outside the box. Academic Medicine, 90(7), pp.854-860.
Evans, G.W., Wells, N.M. & Schamberg, M.A., 2010. The Role of the Environment in Socio-
Economic Status and Obesity. Obesity Prevention, pp.713–725.
GBD 2015 Obesity Collaborator., 2017. Health effects of overweight and obesity in 195
countries over 25 years. New England Journal of Medicine, 377(1), pp.13-27.
HEALTH PROMOTION 12
Goldberg, D.S., 2011. What Kind of People: Obesity Stigma and Inequities. The American
Journal of Medicine, 124(8), p.788.
Gordon-Larsen, P., 2014. Food availability/convenience and obesity. Advances in nutrition, 5(6),
pp.809-817.
How Obesity Relates to Socioeconomic Status, 2016. Population Reference Bureau. Available
at: https://www.prb.org/obesity-socioeconomic-status/ [Accessed April 14, 2019].
Living Well Latrobe, 2017. MUNICIPAL PUBLIC HEALTH AND WELLBEING PLAN 2017-
2021, pp.3–23. Available at:
http://www.latrobe.vic.gov.au/Our_Community/Living_Well_Latrobe/Living_Well_Latr
obe_Health_and_Wellbeing_Plan.
Ren, P., 2016. ShuttleKickers: Exploring Social Persuasions to Encourage Physical Activities.
Seidell, J.C. and Halberstadt, J., 2015. The global burden of obesity and the challenges of
prevention. Annals of Nutrition and Metabolism, 66(Suppl. 2), pp.7-12.
World Health Organization, 2016. Obesity and overweight. Available at:
https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight [Accessed
April 14, 2019].
Zukiewicz-Sobczak, W., Wróblewska, P., Zwolinski, J., Chmielewska-Badora, J., Adamczuk, P.,
Krasowska, E., Zagórski, J., Oniszczuk, A., Piatek, J. and Silny, W., 2014. Obesity and
poverty paradox in developed countries. Annals of Agricultural and Environmental
Medicine, 21(3).
Goldberg, D.S., 2011. What Kind of People: Obesity Stigma and Inequities. The American
Journal of Medicine, 124(8), p.788.
Gordon-Larsen, P., 2014. Food availability/convenience and obesity. Advances in nutrition, 5(6),
pp.809-817.
How Obesity Relates to Socioeconomic Status, 2016. Population Reference Bureau. Available
at: https://www.prb.org/obesity-socioeconomic-status/ [Accessed April 14, 2019].
Living Well Latrobe, 2017. MUNICIPAL PUBLIC HEALTH AND WELLBEING PLAN 2017-
2021, pp.3–23. Available at:
http://www.latrobe.vic.gov.au/Our_Community/Living_Well_Latrobe/Living_Well_Latr
obe_Health_and_Wellbeing_Plan.
Ren, P., 2016. ShuttleKickers: Exploring Social Persuasions to Encourage Physical Activities.
Seidell, J.C. and Halberstadt, J., 2015. The global burden of obesity and the challenges of
prevention. Annals of Nutrition and Metabolism, 66(Suppl. 2), pp.7-12.
World Health Organization, 2016. Obesity and overweight. Available at:
https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight [Accessed
April 14, 2019].
Zukiewicz-Sobczak, W., Wróblewska, P., Zwolinski, J., Chmielewska-Badora, J., Adamczuk, P.,
Krasowska, E., Zagórski, J., Oniszczuk, A., Piatek, J. and Silny, W., 2014. Obesity and
poverty paradox in developed countries. Annals of Agricultural and Environmental
Medicine, 21(3).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.