Muscles Involved in Reaching for a Glass in an Overhead Cabinet
VerifiedAdded on 2021/04/24
|8
|1008
|32
Report
AI Summary
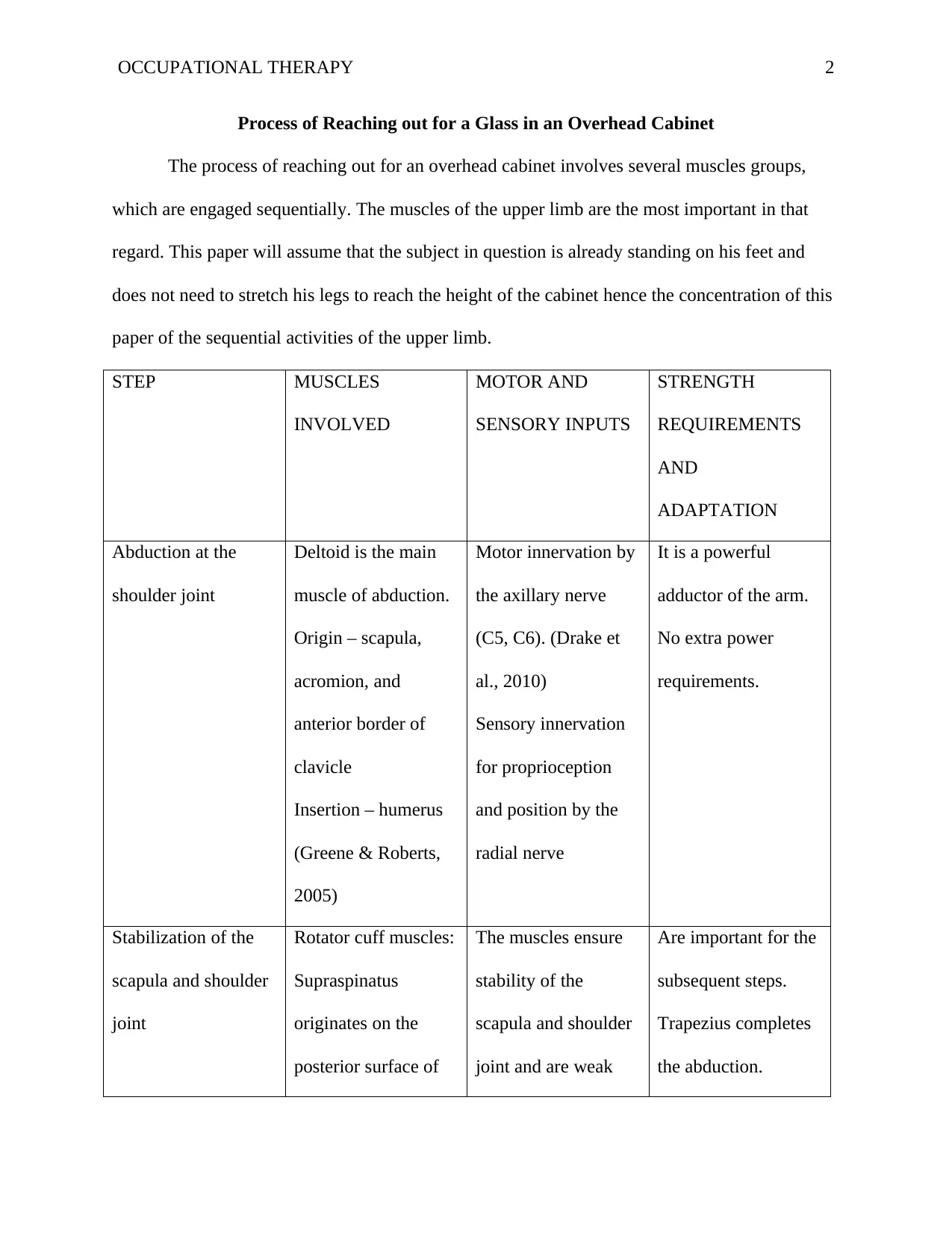
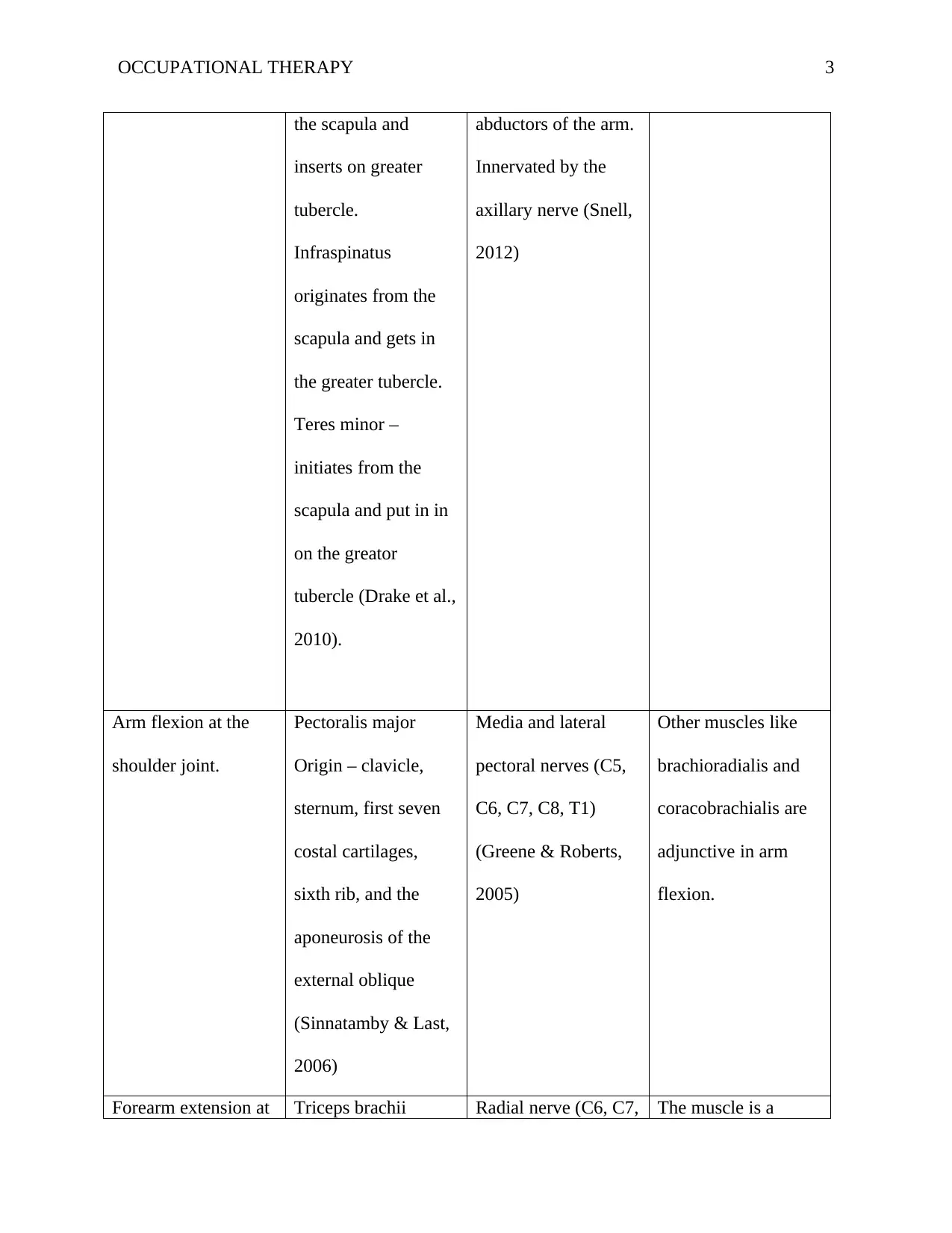
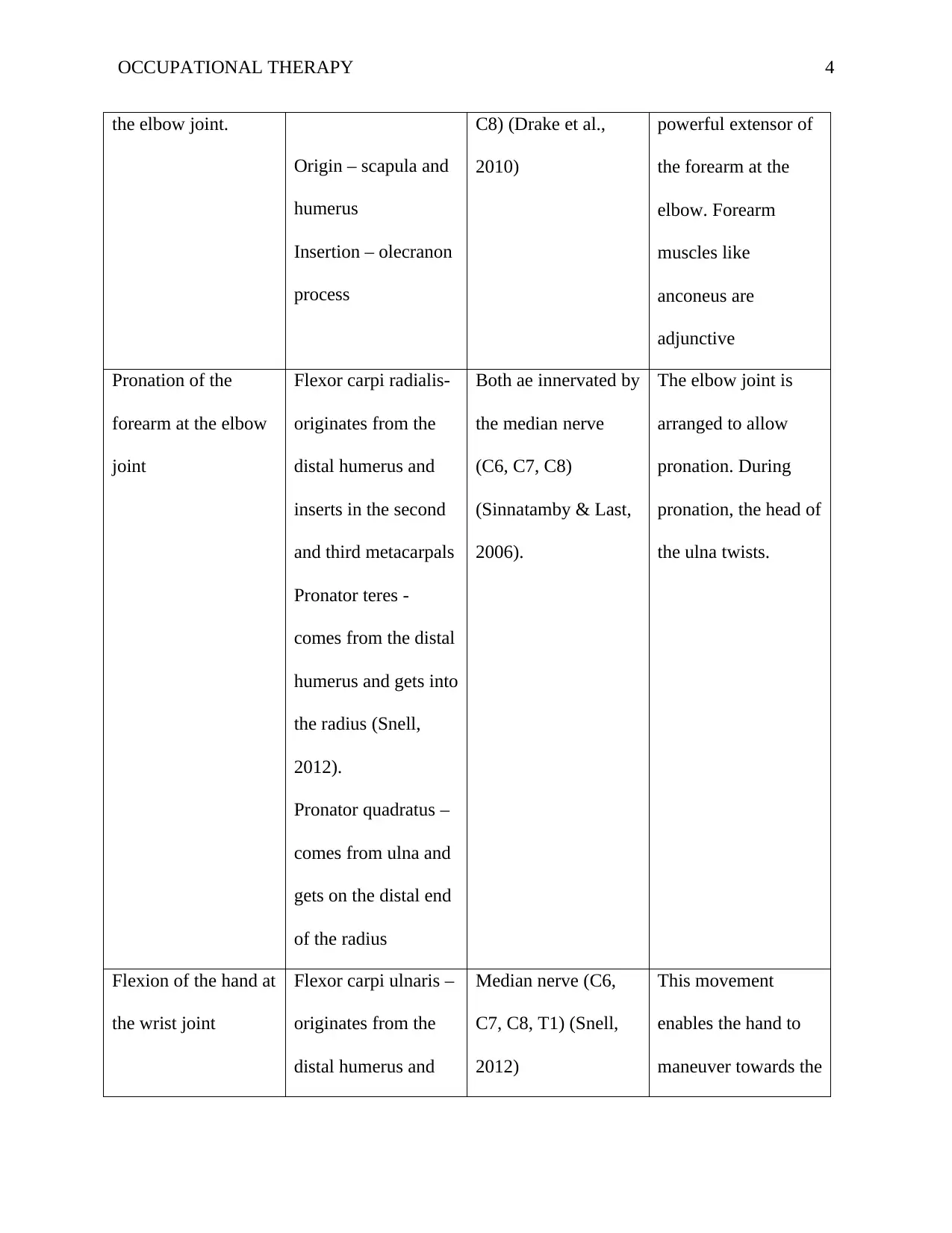
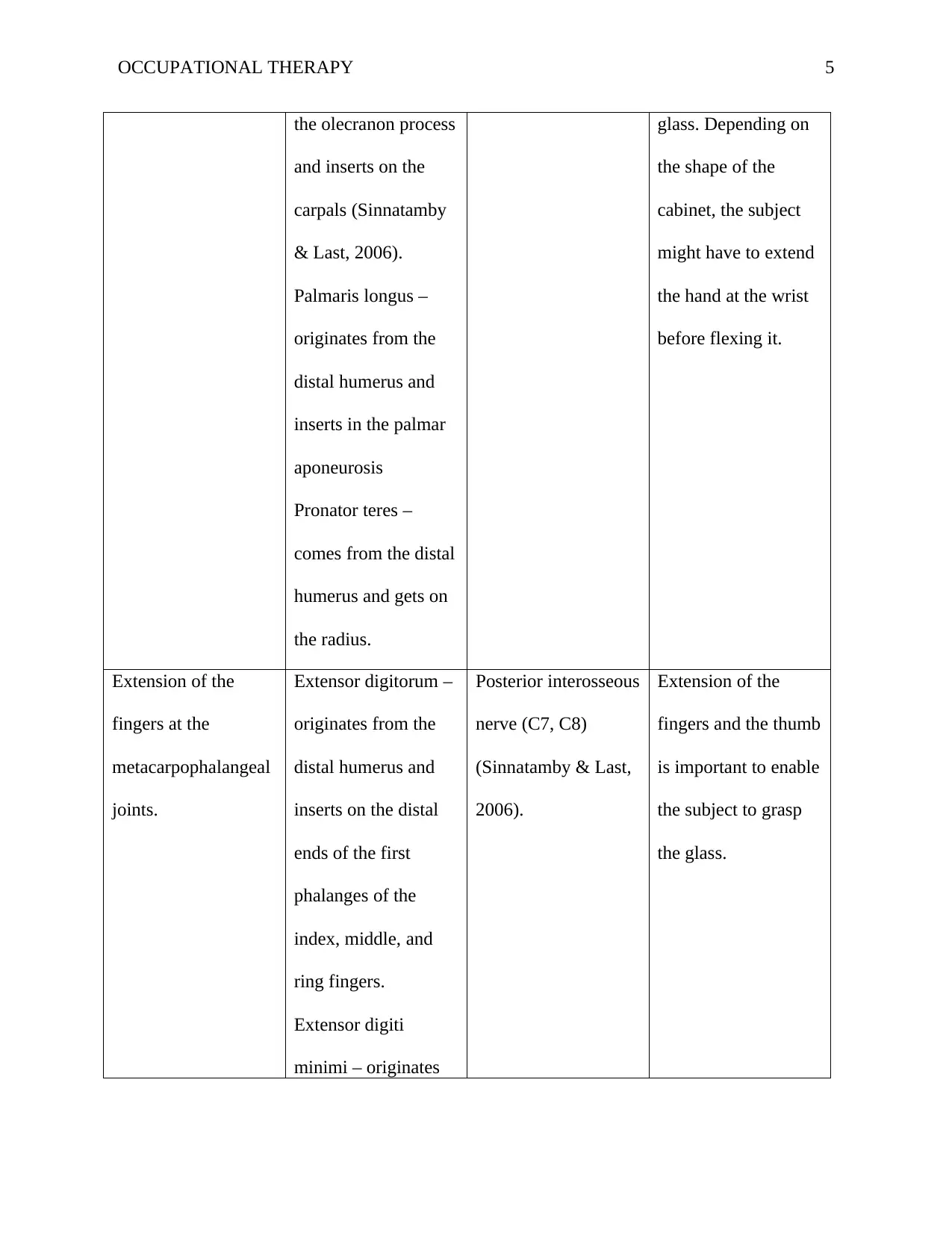
This report details the sequential muscle activations required to reach for a glass in an overhead cabinet, focusing on the upper limb. It begins with the assumption that the subject is standing and examines each step, from shoulder abduction (deltoid) and stabilization (rotator cuff, trapezius) to arm flexion (pectoralis major), forearm extension (triceps brachii), pronation (flexor carpi radialis, pronator teres, pronator quadratus), hand flexion (flexor carpi ulnaris, palmaris longus), finger extension (extensor digitorum, extensor digiti minimi, extensor policis brevis, extensor policis longus, extensor indicis), and finally, finger flexion (flexor digitorum profundus, flexor policis longus) to grasp the glass. The report outlines the muscles involved, their origins, insertions, motor and sensory inputs, and strength requirements, referencing key anatomical texts. The elbow joint's pronation capabilities and the metacarpophalangeal joints' extension role are also highlighted. The analysis provides a comprehensive understanding of the biomechanics of this common daily task.

1 out of 8

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.