Obesity Guidelines: Global, Oman Prevalence, Clinical Management
VerifiedAdded on 2022/08/14
|15
|2771
|19
Report
AI Summary
This report provides a comprehensive overview of obesity, a metabolic illness with epidemic levels globally, and its significant health consequences. It explores the rationales behind the rise in obesity, emphasizing economic and biological factors influencing eating behaviors. The report delves into the global prevalence of obesity, highlighting the situation in Oman, including its high rates of obesity and related health issues. It defines obesity and its classifications based on BMI and waist circumference, outlining clinical evaluation and assessment procedures. The report also covers comprehensive obesity management strategies, including treatment aims, weight loss promotion, prevention of weight regain, and the management of co-morbidities. The report emphasizes lifestyle modifications, dietary interventions, and the importance of addressing psychological factors in obesity management, aiming to reduce health risks and improve patients' quality of life.

Obesity Guidelines
Name, email, postal address and telephone of corresponding author
Full name, deprt, institution, city and country of co-authors
Word count: 2200
Name, email, postal address and telephone of corresponding author
Full name, deprt, institution, city and country of co-authors
Word count: 2200
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1
Obesity Guidelines
Introduction
Obesity remains a metabolic illness (ICD-10 code E66) which has hit epidemic levels.
The WHO has since declared it as the biggest worldwide chronic health concern amongst adults
that is growingly converting into an increasingly severe problem as compared to malnutrition. It
remains an ill-health gateway. Obesity has since turned out to be among the foremost causes of
death and disabilities, which affects both children and adults alongside adolescents globally. In
the year 2014, over 1.90B adults (18+ years) remained overweight. Amongst them, more than
600M stood obese while in 2013, 42M were children below 15 years who were either obese or
overweight. The global health figures report by released by WHO in the year 2015 showed that
in the region of Europe only, the general rate of obesity amongst adults remained 21.50% in men
and 24.5% in women (as shown in figure 1 below).
Obesity Guidelines
Introduction
Obesity remains a metabolic illness (ICD-10 code E66) which has hit epidemic levels.
The WHO has since declared it as the biggest worldwide chronic health concern amongst adults
that is growingly converting into an increasingly severe problem as compared to malnutrition. It
remains an ill-health gateway. Obesity has since turned out to be among the foremost causes of
death and disabilities, which affects both children and adults alongside adolescents globally. In
the year 2014, over 1.90B adults (18+ years) remained overweight. Amongst them, more than
600M stood obese while in 2013, 42M were children below 15 years who were either obese or
overweight. The global health figures report by released by WHO in the year 2015 showed that
in the region of Europe only, the general rate of obesity amongst adults remained 21.50% in men
and 24.5% in women (as shown in figure 1 below).
2
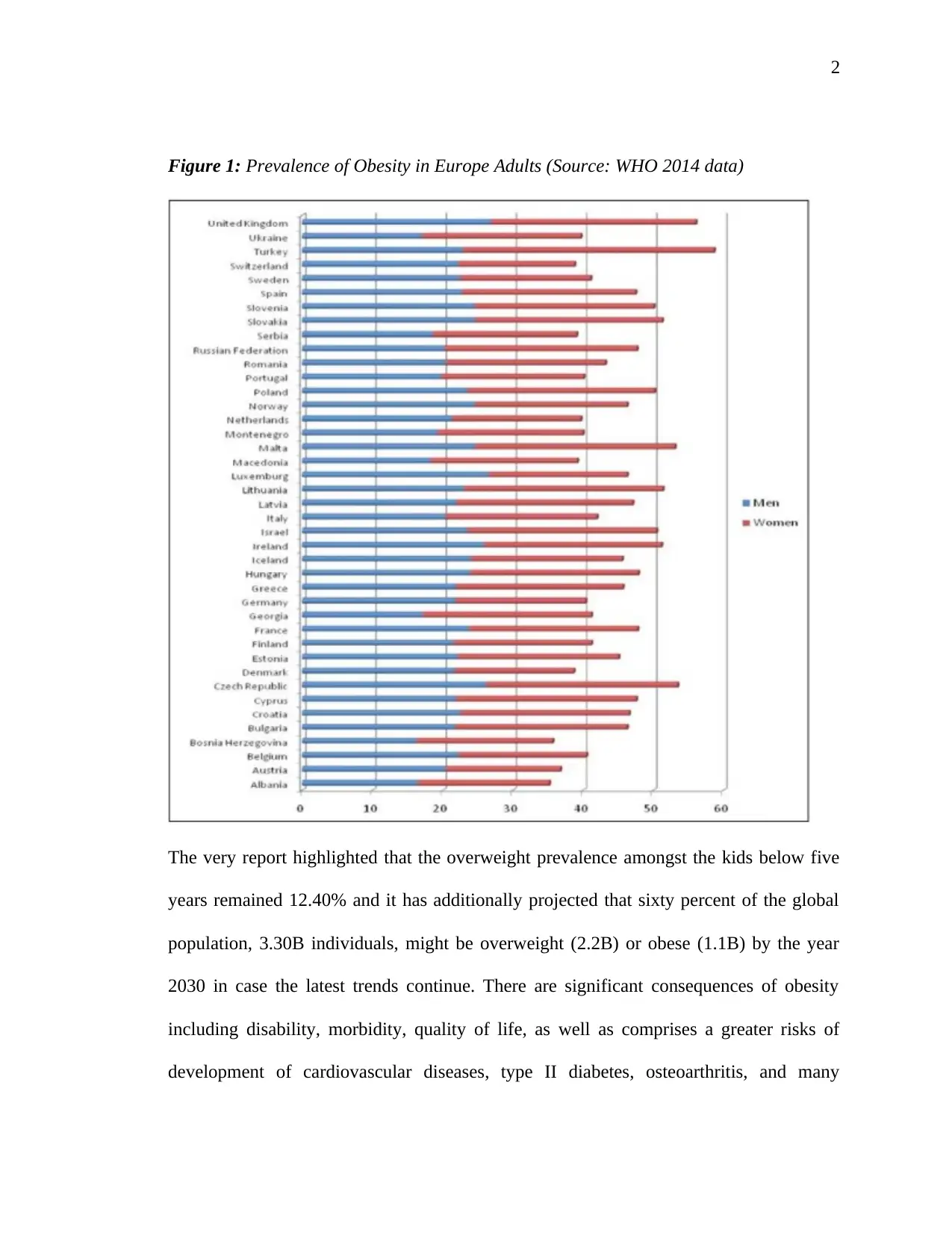
Figure 1: Prevalence of Obesity in Europe Adults (Source: WHO 2014 data)
The very report highlighted that the overweight prevalence amongst the kids below five
years remained 12.40% and it has additionally projected that sixty percent of the global
population, 3.30B individuals, might be overweight (2.2B) or obese (1.1B) by the year
2030 in case the latest trends continue. There are significant consequences of obesity
including disability, morbidity, quality of life, as well as comprises a greater risks of
development of cardiovascular diseases, type II diabetes, osteoarthritis, and many
Figure 1: Prevalence of Obesity in Europe Adults (Source: WHO 2014 data)
The very report highlighted that the overweight prevalence amongst the kids below five
years remained 12.40% and it has additionally projected that sixty percent of the global
population, 3.30B individuals, might be overweight (2.2B) or obese (1.1B) by the year
2030 in case the latest trends continue. There are significant consequences of obesity
including disability, morbidity, quality of life, as well as comprises a greater risks of
development of cardiovascular diseases, type II diabetes, osteoarthritis, and many
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
communal types of cancer alongside additional health concerns. In the year 2010, obesity
and overweight stood estimated to trigger 3.4M deaths, 4.0% of years of life lost
alongside 4.0% of disabilities-adjusted life years (DALYs).
Rational
The rise in Obesity remains a major concern for public health. Almost one in every three
individuals stood obese in early twenties, up from 1 in 7 a quarter-century ago. If the current
patterns continue, the rate of obesity shall rise to more than 40% by this year. Obesity is
connected to illnesses like diabetes, asthma, hypertension and premature mortalities-if left
unattended, the surge in obesity increasingly threatening to erode conventional gains in
expectancies of life. The surge in this illness is further as significant driver of the healthcare cost
in the country [2]. To comprehend the surge in obesity, it is imperative to comprehend how
people are deciding about eating alongside additional behaviors affecting their body weight. In
comprehending overeating and obesity, two eating models alongside regulation of weight and
examination of empirical data for testing the most consistent model with behavior of persons is
necessary. The rational economic model shows that people are trading off utility/contentment
from presently eating meals against both expenditure and disutility of future benefit. People are
making superlative decisions possible provided the accessible info alongside restraints on time
and income. Decision stay optimum (utility-maximizing) at certain conditions when made, even
where arrival of novel info makes such decisions appear mistakes in retrospect. Factors like
declining food prices remain most probable explications for obesity rise. People’s eating
decisions manifest economics and biology as humans are programmed genetically many years to
always feed, with main goalmouth of attaining sufficient survival calories. In a surrounding
whereby foodstuff stays inexpensive, and obtainable freely, biological programming might
communal types of cancer alongside additional health concerns. In the year 2010, obesity
and overweight stood estimated to trigger 3.4M deaths, 4.0% of years of life lost
alongside 4.0% of disabilities-adjusted life years (DALYs).
Rational
The rise in Obesity remains a major concern for public health. Almost one in every three
individuals stood obese in early twenties, up from 1 in 7 a quarter-century ago. If the current
patterns continue, the rate of obesity shall rise to more than 40% by this year. Obesity is
connected to illnesses like diabetes, asthma, hypertension and premature mortalities-if left
unattended, the surge in obesity increasingly threatening to erode conventional gains in
expectancies of life. The surge in this illness is further as significant driver of the healthcare cost
in the country [2]. To comprehend the surge in obesity, it is imperative to comprehend how
people are deciding about eating alongside additional behaviors affecting their body weight. In
comprehending overeating and obesity, two eating models alongside regulation of weight and
examination of empirical data for testing the most consistent model with behavior of persons is
necessary. The rational economic model shows that people are trading off utility/contentment
from presently eating meals against both expenditure and disutility of future benefit. People are
making superlative decisions possible provided the accessible info alongside restraints on time
and income. Decision stay optimum (utility-maximizing) at certain conditions when made, even
where arrival of novel info makes such decisions appear mistakes in retrospect. Factors like
declining food prices remain most probable explications for obesity rise. People’s eating
decisions manifest economics and biology as humans are programmed genetically many years to
always feed, with main goalmouth of attaining sufficient survival calories. In a surrounding
whereby foodstuff stays inexpensive, and obtainable freely, biological programming might
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
culminate in eating too much. Thus, “dual decision” model comes in with fundamental insight
that decisions on eating stay subject to 2-parts of brain which include the affective alongside
deliberative systems. The former system is for sensory inputs’ coordination to yield emotional
sates such as happiness and rage and reacts to clues and stimuli. For instance, food presence
might trigger endorphin alongside dopamine reactions. The latter system integrates greater
cognitive process like thinking abstractly along with planning thereby accounting for long-run
actions’ outcomes. Here, eating habits manifest combined influence of utility-maximizing
deliberative system alongside affective system which reacts rapidly as well as impulsively to
outdoor stimuli, without accounting for long-run consequences. Thus, dual decision model has
various implication for body weight alongside eating habits like predicting that several
individuals shall stay weightier than corresponding utility-maximizing weight and shall try
losing weight. Thus, evidence regarding weight loss, body weight, and consumption of food
stays aligned with “mistakes” of eating related to dual decision model and it is difficult to reunite
with standard utility-maximizing framework. Such findings have significant implications for
obesity policy and guidelines. Where affective system is playing an imperative role in eating
decisions, it shall tend to decrease the anti-obesity policies’ effectiveness which depend on
rational decision making like taxing foods with high fat, salt or sugar content or giving detailed
info on food content.
Prevalence (Global situation and Oman situation)
Globally, the global obesity has virtually trebled beginning 1975. In 2016, over 1.9B
adults, 18+ years, stood overweight and among them, over 650M stood obese. Thirty-nine
percent of adults 18+ years stood overweight in the year 2016, and thirteen percent stood obese.
Moist of the global populace live in economies whereby overweight alongside obesity is killing
culminate in eating too much. Thus, “dual decision” model comes in with fundamental insight
that decisions on eating stay subject to 2-parts of brain which include the affective alongside
deliberative systems. The former system is for sensory inputs’ coordination to yield emotional
sates such as happiness and rage and reacts to clues and stimuli. For instance, food presence
might trigger endorphin alongside dopamine reactions. The latter system integrates greater
cognitive process like thinking abstractly along with planning thereby accounting for long-run
actions’ outcomes. Here, eating habits manifest combined influence of utility-maximizing
deliberative system alongside affective system which reacts rapidly as well as impulsively to
outdoor stimuli, without accounting for long-run consequences. Thus, dual decision model has
various implication for body weight alongside eating habits like predicting that several
individuals shall stay weightier than corresponding utility-maximizing weight and shall try
losing weight. Thus, evidence regarding weight loss, body weight, and consumption of food
stays aligned with “mistakes” of eating related to dual decision model and it is difficult to reunite
with standard utility-maximizing framework. Such findings have significant implications for
obesity policy and guidelines. Where affective system is playing an imperative role in eating
decisions, it shall tend to decrease the anti-obesity policies’ effectiveness which depend on
rational decision making like taxing foods with high fat, salt or sugar content or giving detailed
info on food content.
Prevalence (Global situation and Oman situation)
Globally, the global obesity has virtually trebled beginning 1975. In 2016, over 1.9B
adults, 18+ years, stood overweight and among them, over 650M stood obese. Thirty-nine
percent of adults 18+ years stood overweight in the year 2016, and thirteen percent stood obese.
Moist of the global populace live in economies whereby overweight alongside obesity is killing
5
more individuals as opposed to underweight. Forty-one million kids below the age of five stood
obese/ overweight in 2016 while more than 340M kids alongside adolescents between five and
nineteen years stood obese/ overweight in 2016. Obesity, however, remains preventable.
In Oman situation, as accomplishment go, it is never one which Oman shall trumpet as
one of its finest moments. Sitting at fourteenth place in the league table of utmost obese
countries globally in the latest published survey remains absolutely never something to stay
proud of. Maybe, one consolation remains that Oman is never alone. Every single one of the 6
GCC member states make the list published news and info website HealthGrove, with 5 in the
top 8 fattest economies. Qatar, Kuwait and UAE occupy the 2nd, 3rd and 4th positions, disturbing
news for their health ministries. Oman’s health crises come as no dismay to medical practitioners
who remain well aware of the challenges, described as a “ticking time bomb” that is probable to
explode something near 2030 when the figures of diabetes in Sultanate is projected to surge to a
whopping 124%, according to International Diabetes Federation (IDF).Oman is increasingly
getting bigger, though not in terms of populace, but in terms of growing and soaring rates of
obesity and diabetes besides heart disease and high BPs. The vital statistics of Oman make for
uncomfortable readings since a projected 30.90% of the nation’s populace is already classified as
obese. Over 37.70% of Oman’s women population tip obesity gauges whereas males remain
never much behind at 27.70%. The outcome is 1400 demises from CVDs every year and another
one thousand lives being lost as a result of diabetes-linked diseases. Kids growing up on fast-
food diet remain being classed as obese as early as 5 years old while the high cholesterol
alongside heart disease remain observed in individuals in barely twenties.
Definition and classifications
more individuals as opposed to underweight. Forty-one million kids below the age of five stood
obese/ overweight in 2016 while more than 340M kids alongside adolescents between five and
nineteen years stood obese/ overweight in 2016. Obesity, however, remains preventable.
In Oman situation, as accomplishment go, it is never one which Oman shall trumpet as
one of its finest moments. Sitting at fourteenth place in the league table of utmost obese
countries globally in the latest published survey remains absolutely never something to stay
proud of. Maybe, one consolation remains that Oman is never alone. Every single one of the 6
GCC member states make the list published news and info website HealthGrove, with 5 in the
top 8 fattest economies. Qatar, Kuwait and UAE occupy the 2nd, 3rd and 4th positions, disturbing
news for their health ministries. Oman’s health crises come as no dismay to medical practitioners
who remain well aware of the challenges, described as a “ticking time bomb” that is probable to
explode something near 2030 when the figures of diabetes in Sultanate is projected to surge to a
whopping 124%, according to International Diabetes Federation (IDF).Oman is increasingly
getting bigger, though not in terms of populace, but in terms of growing and soaring rates of
obesity and diabetes besides heart disease and high BPs. The vital statistics of Oman make for
uncomfortable readings since a projected 30.90% of the nation’s populace is already classified as
obese. Over 37.70% of Oman’s women population tip obesity gauges whereas males remain
never much behind at 27.70%. The outcome is 1400 demises from CVDs every year and another
one thousand lives being lost as a result of diabetes-linked diseases. Kids growing up on fast-
food diet remain being classed as obese as early as 5 years old while the high cholesterol
alongside heart disease remain observed in individuals in barely twenties.
Definition and classifications
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

6
Obesity remains a long-lasting illness which is characterized by a surge in store of
fats in the body. Clinically, fatness of the body is often estimated by Body Mass Index (BMI).
This is computed as measured body weight in kilograms divided by measured height squared
(M2). Among adults, (18+), obesity remains well-defined by the BMI of 30kg/m2 alongside
overweight (pre-obesity) by the BMI between 25.0 and 29.90kg/m2. Lower cut-off points of BMI
remain applicable to certain ethnicities including Southeast Asians as shown in table1, level 1
below.
Table 1: BMI Categories (Source WHO 1997)
The intra-abdominal fat accumulation stays linked to higher metabolic alongside
cardiovascular disease risks as shown in level 1 in the above table 1. The abdominal fat amount
might be evaluated by waist circumference (WC) that extremely links with content of intra-
abdominal fat. WC gets measured in horizontal plane halfway in distance of superior ilia crest as
well as lower last rib margin. The utmost latest IDF agreement defines central/visceral/apple,
android-shaped/upper body-obesity in Europids as the WC of ≥ 94 centimeters in males and ≥ 80
in non-expectant females. Its lower cut-off points remain projected for diverse ethnicities as
shown in level 4.
Clinical Evaluation and Assessment
A detailed history, physical exams as well as lab assessment appropriate to the obesity of
the patient need to be obtained.
Obesity remains a long-lasting illness which is characterized by a surge in store of
fats in the body. Clinically, fatness of the body is often estimated by Body Mass Index (BMI).
This is computed as measured body weight in kilograms divided by measured height squared
(M2). Among adults, (18+), obesity remains well-defined by the BMI of 30kg/m2 alongside
overweight (pre-obesity) by the BMI between 25.0 and 29.90kg/m2. Lower cut-off points of BMI
remain applicable to certain ethnicities including Southeast Asians as shown in table1, level 1
below.
Table 1: BMI Categories (Source WHO 1997)
The intra-abdominal fat accumulation stays linked to higher metabolic alongside
cardiovascular disease risks as shown in level 1 in the above table 1. The abdominal fat amount
might be evaluated by waist circumference (WC) that extremely links with content of intra-
abdominal fat. WC gets measured in horizontal plane halfway in distance of superior ilia crest as
well as lower last rib margin. The utmost latest IDF agreement defines central/visceral/apple,
android-shaped/upper body-obesity in Europids as the WC of ≥ 94 centimeters in males and ≥ 80
in non-expectant females. Its lower cut-off points remain projected for diverse ethnicities as
shown in level 4.
Clinical Evaluation and Assessment
A detailed history, physical exams as well as lab assessment appropriate to the obesity of
the patient need to be obtained.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
Taking History:
Additional determinants including drugs, genetics, endocrine abnormalities, smoking
cessation, chronic stress and psychological factors
Dietary behaviors
Eating patterns and potential existence of eating disorder like night eating syndrome,
binge eating disorder or bulimia
Ethnicity
Expectations of patients and their motivation for change
Family history
Past obesity treatment
Physical exercise nature and frequency
Presence of depression alongside additional mood disorders
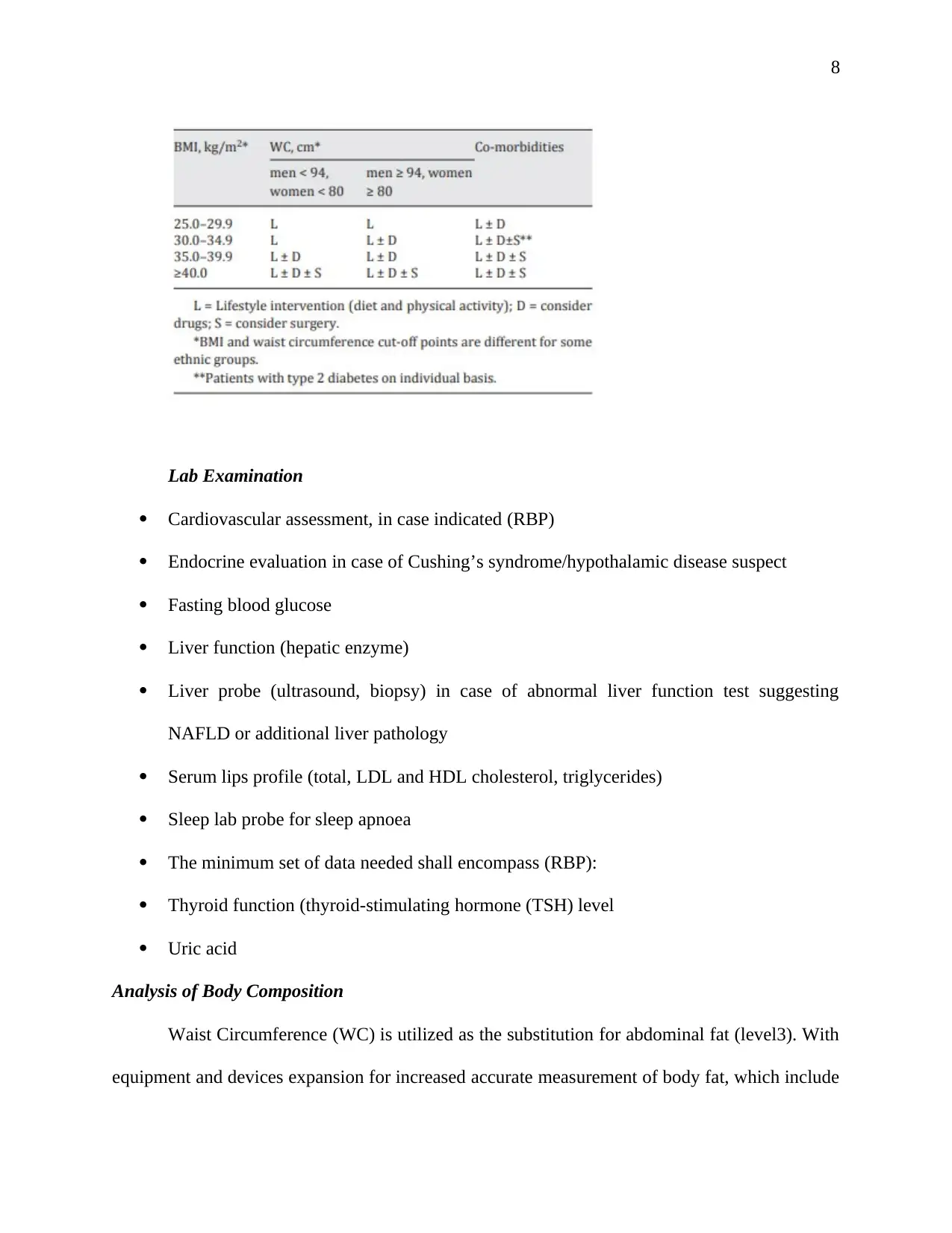
Obesity health consequences (table 2 below)
Table 2: A guide for decision on initial level of intervention level for patient-practitioner
discussion
Taking History:
Additional determinants including drugs, genetics, endocrine abnormalities, smoking
cessation, chronic stress and psychological factors
Dietary behaviors
Eating patterns and potential existence of eating disorder like night eating syndrome,
binge eating disorder or bulimia
Ethnicity
Expectations of patients and their motivation for change
Family history
Past obesity treatment
Physical exercise nature and frequency
Presence of depression alongside additional mood disorders
Obesity health consequences (table 2 below)
Table 2: A guide for decision on initial level of intervention level for patient-practitioner
discussion
8
Lab Examination
Cardiovascular assessment, in case indicated (RBP)
Endocrine evaluation in case of Cushing’s syndrome/hypothalamic disease suspect
Fasting blood glucose
Liver function (hepatic enzyme)
Liver probe (ultrasound, biopsy) in case of abnormal liver function test suggesting
NAFLD or additional liver pathology
Serum lips profile (total, LDL and HDL cholesterol, triglycerides)
Sleep lab probe for sleep apnoea
The minimum set of data needed shall encompass (RBP):
Thyroid function (thyroid-stimulating hormone (TSH) level
Uric acid
Analysis of Body Composition
Waist Circumference (WC) is utilized as the substitution for abdominal fat (level3). With
equipment and devices expansion for increased accurate measurement of body fat, which include
Lab Examination
Cardiovascular assessment, in case indicated (RBP)
Endocrine evaluation in case of Cushing’s syndrome/hypothalamic disease suspect
Fasting blood glucose
Liver function (hepatic enzyme)
Liver probe (ultrasound, biopsy) in case of abnormal liver function test suggesting
NAFLD or additional liver pathology
Serum lips profile (total, LDL and HDL cholesterol, triglycerides)
Sleep lab probe for sleep apnoea
The minimum set of data needed shall encompass (RBP):
Thyroid function (thyroid-stimulating hormone (TSH) level
Uric acid
Analysis of Body Composition
Waist Circumference (WC) is utilized as the substitution for abdominal fat (level3). With
equipment and devices expansion for increased accurate measurement of body fat, which include
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
dual energy X-ray, bioimpedance analysis (BIA), absorptiometry (DEXA), air-displacement
plethysmography (BodPod) along with procedure for body scanning-substituting burdensome
weighing of underwater-, it has been feasible to effortlessly classify a person based on body fat
degree, autonomously of BMI. Such a mechanism has further drawn significant courtesy to non-
adipose tissue function- i.e. fat-free mass (FFM) or lean mass-as well as the FFM’s contribution
to pathology, physiological functioning alongside wellbeing. Assessment body composition is
never indispensable for management of obesity in monotonous clinical run-through, however, it
might be helpful technique in fat alongside FFM measurement prior to and in the course of
treatment [3].
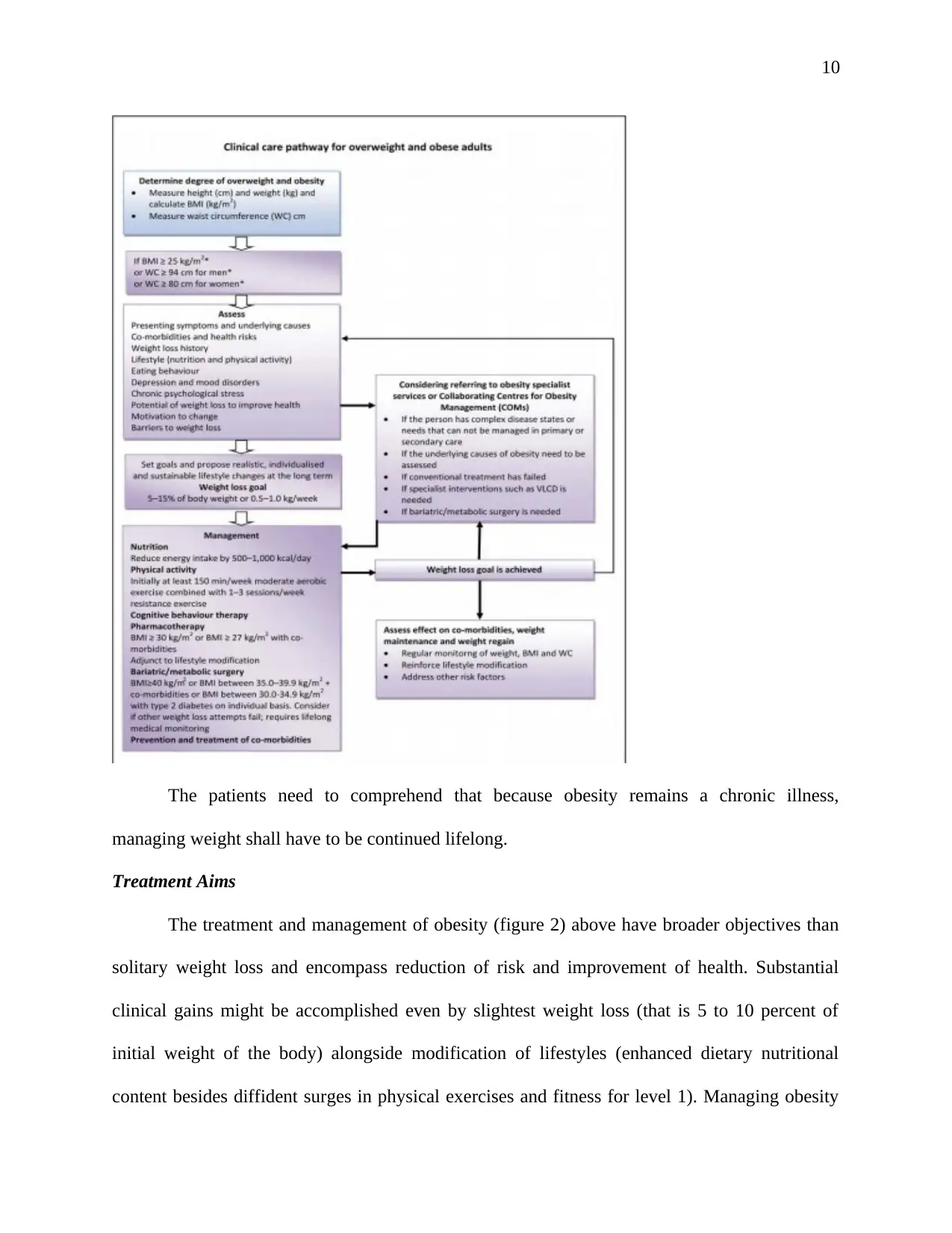
Comprehensive Obesity Management
Relevant goalmouths of managing weight stresses truthful weight loss to accomplish a
decrease in risk to health alongside need to encompass weight loss promotion, weight regain
maintenance and prevention as shown in figure 2 below.
Fig2: Algorithm for assessing and stepwise obese and overweight adults’ management. * BMI &
WC cut-off points remain dissimilar for certain ethnicities.
dual energy X-ray, bioimpedance analysis (BIA), absorptiometry (DEXA), air-displacement
plethysmography (BodPod) along with procedure for body scanning-substituting burdensome
weighing of underwater-, it has been feasible to effortlessly classify a person based on body fat
degree, autonomously of BMI. Such a mechanism has further drawn significant courtesy to non-
adipose tissue function- i.e. fat-free mass (FFM) or lean mass-as well as the FFM’s contribution
to pathology, physiological functioning alongside wellbeing. Assessment body composition is
never indispensable for management of obesity in monotonous clinical run-through, however, it
might be helpful technique in fat alongside FFM measurement prior to and in the course of
treatment [3].
Comprehensive Obesity Management
Relevant goalmouths of managing weight stresses truthful weight loss to accomplish a
decrease in risk to health alongside need to encompass weight loss promotion, weight regain
maintenance and prevention as shown in figure 2 below.
Fig2: Algorithm for assessing and stepwise obese and overweight adults’ management. * BMI &
WC cut-off points remain dissimilar for certain ethnicities.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
The patients need to comprehend that because obesity remains a chronic illness,
managing weight shall have to be continued lifelong.
Treatment Aims
The treatment and management of obesity (figure 2) above have broader objectives than
solitary weight loss and encompass reduction of risk and improvement of health. Substantial
clinical gains might be accomplished even by slightest weight loss (that is 5 to 10 percent of
initial weight of the body) alongside modification of lifestyles (enhanced dietary nutritional
content besides diffident surges in physical exercises and fitness for level 1). Managing obesity
The patients need to comprehend that because obesity remains a chronic illness,
managing weight shall have to be continued lifelong.
Treatment Aims
The treatment and management of obesity (figure 2) above have broader objectives than
solitary weight loss and encompass reduction of risk and improvement of health. Substantial
clinical gains might be accomplished even by slightest weight loss (that is 5 to 10 percent of
initial weight of the body) alongside modification of lifestyles (enhanced dietary nutritional
content besides diffident surges in physical exercises and fitness for level 1). Managing obesity

11
can never emphasize solely on weight alongside BMI decrease. Additional consideration must be
paid to waist circumference and body composition improvement that is emphasizing on
maintaining or ameliorating FFM and lowering fat mass. Managing co-morbidities, obese
patients’ quality of life and well-being improvement are further encompassed in aims of
treatment. Suitable management of overweight and obesity complication besides weight
management need to entail managing dyslipidemia, optimization of glycaemic control in type II
diabetic individuals, normalization of BP in hypertension, pulmonary disorders management like
sleep apnoea syndrome (SAS), attention to pain control alongside osteoarthritis’ mobility needs,
managing psychological instabilities which include eating disorders, affective disorders, low
self-esteem as well as disturbance of body image. Management of obesity might decrease the
need for treating co-morbidities by medication for level 1, grade A.
Further Weight Gain Prevention
Amongst overweight individuals (BMI 25.00–29.90 kg/m 2) with no overt co-
morbidities, preventing additional weight gain (via dietary advice alongside surge in physical
exercise) instead of weight loss per se might remain a suitable target. Objectives of weight loss
objectives need to stay realistic, individualized as well as aimed at long run (see table 3 below).
can never emphasize solely on weight alongside BMI decrease. Additional consideration must be
paid to waist circumference and body composition improvement that is emphasizing on
maintaining or ameliorating FFM and lowering fat mass. Managing co-morbidities, obese
patients’ quality of life and well-being improvement are further encompassed in aims of
treatment. Suitable management of overweight and obesity complication besides weight
management need to entail managing dyslipidemia, optimization of glycaemic control in type II
diabetic individuals, normalization of BP in hypertension, pulmonary disorders management like
sleep apnoea syndrome (SAS), attention to pain control alongside osteoarthritis’ mobility needs,
managing psychological instabilities which include eating disorders, affective disorders, low
self-esteem as well as disturbance of body image. Management of obesity might decrease the
need for treating co-morbidities by medication for level 1, grade A.
Further Weight Gain Prevention
Amongst overweight individuals (BMI 25.00–29.90 kg/m 2) with no overt co-
morbidities, preventing additional weight gain (via dietary advice alongside surge in physical
exercise) instead of weight loss per se might remain a suitable target. Objectives of weight loss
objectives need to stay realistic, individualized as well as aimed at long run (see table 3 below).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 15
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.