Knowledge Identification Regarding Organ Donation Barriers
VerifiedAdded on 2023/06/10
|10
|9886
|426
Report
AI Summary
This report examines the public's knowledge of organ donation, identifying key misconceptions and barriers that hinder donation rates. The study, involving undergraduate students, MBA students, and community members, assessed factual knowledge through a true/false questionnaire. Results revealed significant gaps in understanding, particularly regarding religious support, brain death, separation of physician teams, and the validity of donor cards. The report highlights the relationship between knowledge and attitudes towards organ donation, willingness to donate, and the likelihood of carrying a donor card. The findings suggest that improving public knowledge can positively influence attitudes and behaviors related to organ donation. Desklib provides access to similar solved assignments and resources for students.
Sot.Sci.Med. Vol.31,No.7.pp.791-800.1990 0277-953690 S3.00+0.00
Printed in Great Britain. All rights reserved Copyright S 1990 Pergamon Press plc
KNOWLEDGE REGARDING ORGAN DONATION:
IDENTIFYING AND OVERCOMING BARRIERS TO
ORGAN DONATION
RAYMOND L. HORTON and PATRICIAJ.HORTON
College of Business & Economics, Lehigh University, Drown Hall 35, Bethlehem, PA 18015, U.S.A.
Abstract-Four-hundred and fifty-five undergraduate students, 26 MBA students, and 465 people from
the surrounding community responded to 21 true/false questions regarding factual knowledge about organ
donation. The mean number of correct answers was 74.6%. The correct response rate, however, varied
widely over questions. Four questions with very large error rates suggest possible ‘barriers to donation’.
Specifically, these questions concerned religious support for organ donation, the concept of brain death.
the normally rigid separation of physician teams who are primarily responsible for the welfare of the donor
and donee, and a mistaken belief that to be valid an organ donor card must be filed with the U.S.
Department of Health and Human Services. Knowledge of organ donation facts was found to be related
to whether subjects carried or requested an organ donor card, their attitude towards organ donation and
their willingness to donate their own organs or the organs of a deceased loved one. These findings suggest
strategies for raising public support for organ donation.
Key words-organ donation, knowledge, education
INTRODUCI-ION
“Despite major advances in organ transplantation
technology, approximately one third of patients
accepted for transplantation die while awaiting a
matched donor” [I, p. 547, emphasis added]. These
deaths occur despite estimates that the pool of
potential donors is more than adequate to meet the
current demand for transplantable organs [2]. Unfor-
tunately, only a small fraction, perhaps as low as
15%, of these organs actually become available [l].
Understanding and overcoming the potential
‘barriers to donation’ that are so clearly apparent in
the discrepancy between demand and supply for
organs for transplantation is now recognized as a top
priority for organ donation research [3].
The focus of our research is on the decision to sign
and carry an organ donor card. A major assumption
underlying this research is that the decision process
involved in such decisions is constructed upon a
strong cognitive base. This assumption has a long and
productive history in psychology [cf. 41. While atti-
tudes, emotions, and behaviors that do not rest upon
a strong cognitive base are now generally acknowl-
edged to exist [e.g. $61, decisions that are important
to the person and that are made without great time
and external pressures are generally believed to fol-
low a model that proceeds from cognition to affect to
behavior and is generally referred to as a learning
hierarchy model of decision making [e.g. 5, 71. Atti-
tudes and decisions involving donor cards, as
opposed to actual donation decisions, are believed to
follow such a learning hierarchy model of decision
making.
The actual donation decision will be made by
family members under extremely difficult circum-
stances. This raises the question of the relationship
between signing a donor card and the family’s
decision to donate. Formal studies and impression-
istic evidence suggest important links between these
two very different types of decisions. Prottas [8] and
Manninen and Evans [9] show that knowledge that
the deceased carried a donor card is an important
factor in families’ decisions to donate. Recently,
Prottas and Batten [lo] reported in a large scale
survey “that medical/health professionals often hesi-
tate to cooperate because they fear contacting
families of donors” (p. 643). Callender [I I], a trans-
plant surgeon, reports that such requests are often
met with negative emotions of hostility, frustration,
anger, and despair. Callender also states that the
most important role for organ donor cards is in
stimulating family discussion. We believe that to
the extent physicians and other medical personnel
encounter positive reactions to requests for donation
they will be more willing to make such requests in the
future. We also believe that the likelihood of such
positive encounters will increase as more people sign
and carry donor cards.
Although many studies have shown high levels
of public awareness of organ donation [e.g. 91, there
has been little investigation of public knowledge of
specific facts regarding organ donation and what
effect such knowledge may have on the decision to
sign and carry an organ donor card. These same
studies indicate that only 14-19% of people polled
have actually signed donor cards. Clearly, awareness
alone has not been sufficient to turn general support
for the concept of organ transplantation into per-
sonal commitment to donate by signing donor cards.
The data reported here come from (1) a pilot for
a larger study of the relationships among knowledge,
values, attitudes, and behavior regarding organ
donation and the act of becoming a potential organ
donor, (2) a subsequent experiment which included
additional explanatory variables and an opportunity
Printed in Great Britain. All rights reserved Copyright S 1990 Pergamon Press plc
KNOWLEDGE REGARDING ORGAN DONATION:
IDENTIFYING AND OVERCOMING BARRIERS TO
ORGAN DONATION
RAYMOND L. HORTON and PATRICIAJ.HORTON
College of Business & Economics, Lehigh University, Drown Hall 35, Bethlehem, PA 18015, U.S.A.
Abstract-Four-hundred and fifty-five undergraduate students, 26 MBA students, and 465 people from
the surrounding community responded to 21 true/false questions regarding factual knowledge about organ
donation. The mean number of correct answers was 74.6%. The correct response rate, however, varied
widely over questions. Four questions with very large error rates suggest possible ‘barriers to donation’.
Specifically, these questions concerned religious support for organ donation, the concept of brain death.
the normally rigid separation of physician teams who are primarily responsible for the welfare of the donor
and donee, and a mistaken belief that to be valid an organ donor card must be filed with the U.S.
Department of Health and Human Services. Knowledge of organ donation facts was found to be related
to whether subjects carried or requested an organ donor card, their attitude towards organ donation and
their willingness to donate their own organs or the organs of a deceased loved one. These findings suggest
strategies for raising public support for organ donation.
Key words-organ donation, knowledge, education
INTRODUCI-ION
“Despite major advances in organ transplantation
technology, approximately one third of patients
accepted for transplantation die while awaiting a
matched donor” [I, p. 547, emphasis added]. These
deaths occur despite estimates that the pool of
potential donors is more than adequate to meet the
current demand for transplantable organs [2]. Unfor-
tunately, only a small fraction, perhaps as low as
15%, of these organs actually become available [l].
Understanding and overcoming the potential
‘barriers to donation’ that are so clearly apparent in
the discrepancy between demand and supply for
organs for transplantation is now recognized as a top
priority for organ donation research [3].
The focus of our research is on the decision to sign
and carry an organ donor card. A major assumption
underlying this research is that the decision process
involved in such decisions is constructed upon a
strong cognitive base. This assumption has a long and
productive history in psychology [cf. 41. While atti-
tudes, emotions, and behaviors that do not rest upon
a strong cognitive base are now generally acknowl-
edged to exist [e.g. $61, decisions that are important
to the person and that are made without great time
and external pressures are generally believed to fol-
low a model that proceeds from cognition to affect to
behavior and is generally referred to as a learning
hierarchy model of decision making [e.g. 5, 71. Atti-
tudes and decisions involving donor cards, as
opposed to actual donation decisions, are believed to
follow such a learning hierarchy model of decision
making.
The actual donation decision will be made by
family members under extremely difficult circum-
stances. This raises the question of the relationship
between signing a donor card and the family’s
decision to donate. Formal studies and impression-
istic evidence suggest important links between these
two very different types of decisions. Prottas [8] and
Manninen and Evans [9] show that knowledge that
the deceased carried a donor card is an important
factor in families’ decisions to donate. Recently,
Prottas and Batten [lo] reported in a large scale
survey “that medical/health professionals often hesi-
tate to cooperate because they fear contacting
families of donors” (p. 643). Callender [I I], a trans-
plant surgeon, reports that such requests are often
met with negative emotions of hostility, frustration,
anger, and despair. Callender also states that the
most important role for organ donor cards is in
stimulating family discussion. We believe that to
the extent physicians and other medical personnel
encounter positive reactions to requests for donation
they will be more willing to make such requests in the
future. We also believe that the likelihood of such
positive encounters will increase as more people sign
and carry donor cards.
Although many studies have shown high levels
of public awareness of organ donation [e.g. 91, there
has been little investigation of public knowledge of
specific facts regarding organ donation and what
effect such knowledge may have on the decision to
sign and carry an organ donor card. These same
studies indicate that only 14-19% of people polled
have actually signed donor cards. Clearly, awareness
alone has not been sufficient to turn general support
for the concept of organ transplantation into per-
sonal commitment to donate by signing donor cards.
The data reported here come from (1) a pilot for
a larger study of the relationships among knowledge,
values, attitudes, and behavior regarding organ
donation and the act of becoming a potential organ
donor, (2) a subsequent experiment which included
additional explanatory variables and an opportunity
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
792 RAYMOND L. HORTONand PATRICIAJ. HORTON
for subjects to request an organ donor card, and (3) a
followup study of the community surrounding the
university. The focus of the present report is on the
knowledge portion of the study.
The results of the survey reveal some major gaps
and errors in knowledge about organ donation. Posi-
tive relationships between knowledge and various
attitudinal and behavioral measures suggest that in-
creasing knowledge regarding organ donation may
improve attitudes towards organ donation, increase
expressed willingness to become a potential organ
donor or to donate the organs of a deceased loved
one, and increase the likelihood of requesting an
organ donor card when given the chance to do so.
METHODOLOGY
Subjects in the first study were 26 MBA students
and 455 undergraduates at an eastern private univer-
sity. These subjects were drawn from the subject pool
maintained by the psychology department and sev-
eral courses in the colleges of arts and sciences and
business and all subjects were participating as a
course requirement. While subjects represented a
cross section of the university, the student sample
must be regarded as a convenience sample. Subjects
in the second study were 465 adults drawn from the
local community. The subjects were recruited as a
Kth sample from the local telephone directory. There
were three phases to the data collection process and
five distinct subject groups:
A preexperimental group of (1) 115 undergraduates and (2)
26 MBA students who completed four questionnaires in the
following sequence: (a) Rokeach’s[ 121Terminal and Instru-
mental value scales, (b) Goodmonson and Glaudin’s 113)
Attitude Toward Organ Donation scale, (c) the organ
donation knowledge instrument developed and reported
here, and (d) an instrument that collected data on subjects’
age, sex, previous experience with organ donation, whether
subjects carried a donor card, and willingness to donate the
organs of a loved one and willingness to donate theirown
organs.
(3) A true experimental group of 185 undergraduates who
answered the above questionnaires plus a Belief in a Just
World Scale ll41 and an Attitude Towards Death Scale I151
which were piaced immediately following the Rokeach v&.rd
scales. These subjects were not asked questions about their
experiences with organ donation or their willingness to
donate. They were asked their class standing and college
affiliation. Approximately one month after completing these
questionnaires, subjects received a letter from Mr Howard
Nathan, Executive Director of the Delaware Valley Trans-
plant Program, explaining the need for donated- organs.
Enclosed with Mr Nathan’s letter was a Dow nublication
called ‘Make a Miracle’ that explains organ donation in a
simple question and answer format and an addressed,
stamped postcard the subject could use to request an organ
donor card. The Delaware Valley Transplant Program
prepared a coded list of subjects who requested a donor
card.
As part of the experiment there was also (4) a control
group of 155 undergraduates. The control group completed
the questionnaires approximately one month a/rer receiving
*The authors greatly appreciate the assistance of Howard
Nathan, Executive Director of the Delaware Valley
Transplant Program, in reviewing the knowledge ques-
tionnaire.
the letter and accompanying material from Mr Nathan
described above and ufier the cutoff date for recording
requested organ donor cards. These subjects also completed
all demographic and donor questions described for groups
one and two.
The second study used telephone contacts, which were
made by 78 undergraduate students in the first author’s
marketing research class, to request adult members of the
local community to complete a mail survey on organ
donation. Of 968 who agreed to participate, useable re-
sponses were received from 465 persons. Five questionnaires
were returned uncompleted; two with notes explaining that
after seeing the questionnaire they had decided not to
participate. Although the overall content of the question-
naires was similar, a number of changes were made to make
the questionnaire more appropriate for a mail survey. The
knowledge questions, however, were unchanged. The last
question on the survey was whether the respondent would
like to be sent an organ donor card.
Data for the student sample was collected in
groups of approx. IO-20 persons. In a brief intro-
duction student subjects were told only that the study
concerned the relationships among knowledge,
values, attitudes, and behavior. The format of the
questionnaires to be answered was explained and
subjects were asked if they had any questions, few
did, and then told to begin. The entire process took
approx. 20-25 min. While the Organ Donation Atti-
tude questionnaire alerted most subjects to the object
of study, it provided subjects with no factual infor-
mation. Subjects in the second study were told in the
initial telephone request that the survey concerned
organ donation. Approximately half of the persons
contacted by telephone agreed to participate. These
persons were mailed the self-administered question-
naire along with a postage paid business reply
envelop. Subjects were invited to telephone the first
author if they had any questions or concerns about
the survey. None did.
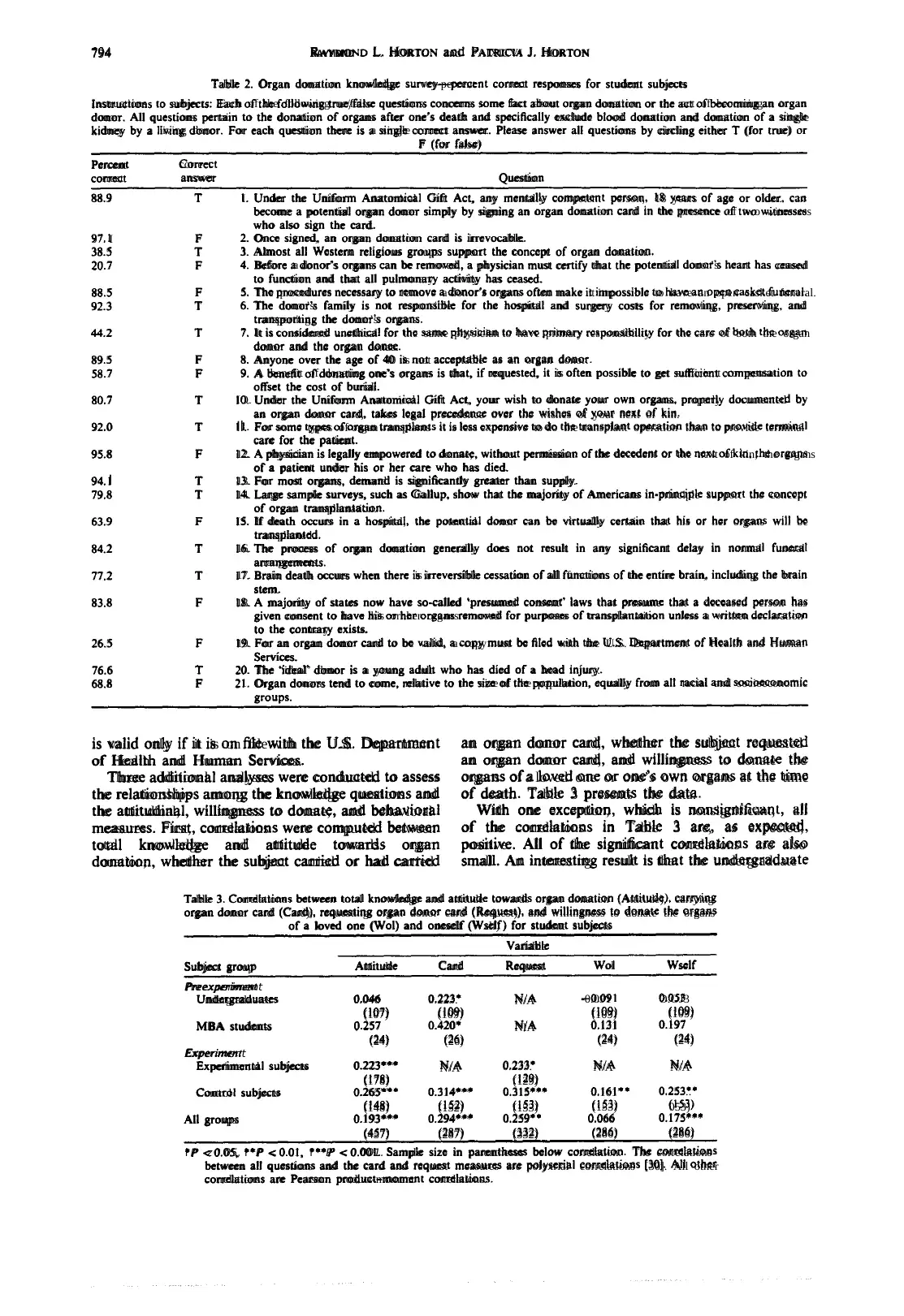
The instructions regarding the knowledge ques-
tionnaire given to all subject groups are reproduced
in Table 2 below. The 21 knowledge questions were
developed from a variety of sources including infor-
mation accompanying organ donor cards, national
surveys such as Gallup, and articles from the journal
literature. Each question was designed to have an
unequivocal true or false answer.*
RESULTSFOR STUDE5-t’SURJECTS
Data for the student subjects was collected and
completely analyzed prior to data collection for the
community sample. For this reason, we first present
results for the student subjects; treating the com-
munity sample as a partial replication and major
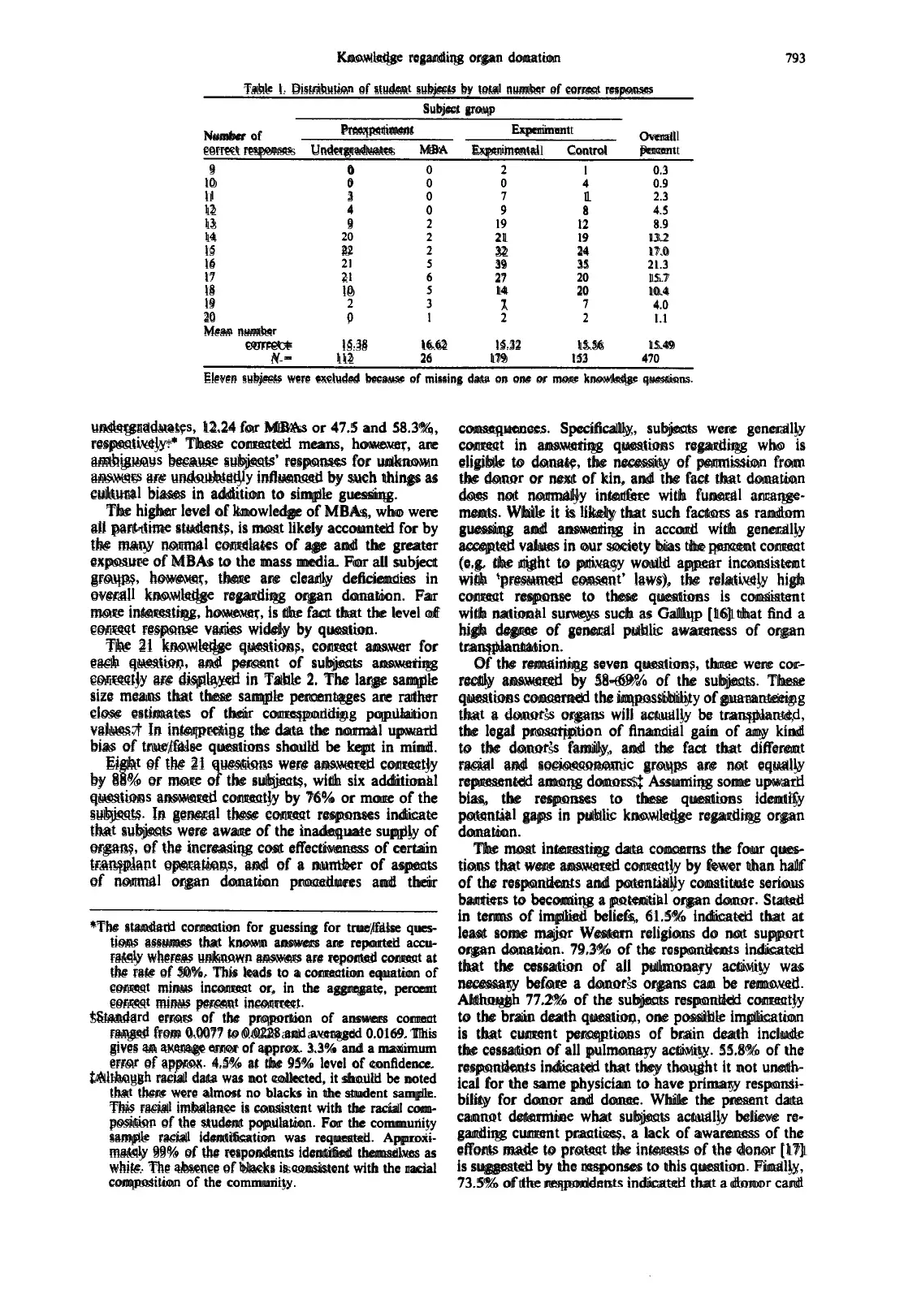
extension. Table 1 presents the distribution of correct
answers for the four identifiable student subject
groups. The number of correct answers ranged from
9 to 20 with a mean of 15.49 or 73.8%. MBAs
answered 1.2 more questions correctly than under-
graduates (P = 0.002). There were no significant
differences in knowledge among the three under-
graduate groups. The mean number of correct
answers should be considered an upper limit on true
knowledge because true/false questions are subject to
inflation from guessing. The standard correction
for guessing yields a corrected mean of 9.98 for
for subjects to request an organ donor card, and (3) a
followup study of the community surrounding the
university. The focus of the present report is on the
knowledge portion of the study.
The results of the survey reveal some major gaps
and errors in knowledge about organ donation. Posi-
tive relationships between knowledge and various
attitudinal and behavioral measures suggest that in-
creasing knowledge regarding organ donation may
improve attitudes towards organ donation, increase
expressed willingness to become a potential organ
donor or to donate the organs of a deceased loved
one, and increase the likelihood of requesting an
organ donor card when given the chance to do so.
METHODOLOGY
Subjects in the first study were 26 MBA students
and 455 undergraduates at an eastern private univer-
sity. These subjects were drawn from the subject pool
maintained by the psychology department and sev-
eral courses in the colleges of arts and sciences and
business and all subjects were participating as a
course requirement. While subjects represented a
cross section of the university, the student sample
must be regarded as a convenience sample. Subjects
in the second study were 465 adults drawn from the
local community. The subjects were recruited as a
Kth sample from the local telephone directory. There
were three phases to the data collection process and
five distinct subject groups:
A preexperimental group of (1) 115 undergraduates and (2)
26 MBA students who completed four questionnaires in the
following sequence: (a) Rokeach’s[ 121Terminal and Instru-
mental value scales, (b) Goodmonson and Glaudin’s 113)
Attitude Toward Organ Donation scale, (c) the organ
donation knowledge instrument developed and reported
here, and (d) an instrument that collected data on subjects’
age, sex, previous experience with organ donation, whether
subjects carried a donor card, and willingness to donate the
organs of a loved one and willingness to donate theirown
organs.
(3) A true experimental group of 185 undergraduates who
answered the above questionnaires plus a Belief in a Just
World Scale ll41 and an Attitude Towards Death Scale I151
which were piaced immediately following the Rokeach v&.rd
scales. These subjects were not asked questions about their
experiences with organ donation or their willingness to
donate. They were asked their class standing and college
affiliation. Approximately one month after completing these
questionnaires, subjects received a letter from Mr Howard
Nathan, Executive Director of the Delaware Valley Trans-
plant Program, explaining the need for donated- organs.
Enclosed with Mr Nathan’s letter was a Dow nublication
called ‘Make a Miracle’ that explains organ donation in a
simple question and answer format and an addressed,
stamped postcard the subject could use to request an organ
donor card. The Delaware Valley Transplant Program
prepared a coded list of subjects who requested a donor
card.
As part of the experiment there was also (4) a control
group of 155 undergraduates. The control group completed
the questionnaires approximately one month a/rer receiving
*The authors greatly appreciate the assistance of Howard
Nathan, Executive Director of the Delaware Valley
Transplant Program, in reviewing the knowledge ques-
tionnaire.
the letter and accompanying material from Mr Nathan
described above and ufier the cutoff date for recording
requested organ donor cards. These subjects also completed
all demographic and donor questions described for groups
one and two.
The second study used telephone contacts, which were
made by 78 undergraduate students in the first author’s
marketing research class, to request adult members of the
local community to complete a mail survey on organ
donation. Of 968 who agreed to participate, useable re-
sponses were received from 465 persons. Five questionnaires
were returned uncompleted; two with notes explaining that
after seeing the questionnaire they had decided not to
participate. Although the overall content of the question-
naires was similar, a number of changes were made to make
the questionnaire more appropriate for a mail survey. The
knowledge questions, however, were unchanged. The last
question on the survey was whether the respondent would
like to be sent an organ donor card.
Data for the student sample was collected in
groups of approx. IO-20 persons. In a brief intro-
duction student subjects were told only that the study
concerned the relationships among knowledge,
values, attitudes, and behavior. The format of the
questionnaires to be answered was explained and
subjects were asked if they had any questions, few
did, and then told to begin. The entire process took
approx. 20-25 min. While the Organ Donation Atti-
tude questionnaire alerted most subjects to the object
of study, it provided subjects with no factual infor-
mation. Subjects in the second study were told in the
initial telephone request that the survey concerned
organ donation. Approximately half of the persons
contacted by telephone agreed to participate. These
persons were mailed the self-administered question-
naire along with a postage paid business reply
envelop. Subjects were invited to telephone the first
author if they had any questions or concerns about
the survey. None did.
The instructions regarding the knowledge ques-
tionnaire given to all subject groups are reproduced
in Table 2 below. The 21 knowledge questions were
developed from a variety of sources including infor-
mation accompanying organ donor cards, national
surveys such as Gallup, and articles from the journal
literature. Each question was designed to have an
unequivocal true or false answer.*
RESULTSFOR STUDE5-t’SURJECTS
Data for the student subjects was collected and
completely analyzed prior to data collection for the
community sample. For this reason, we first present
results for the student subjects; treating the com-
munity sample as a partial replication and major
extension. Table 1 presents the distribution of correct
answers for the four identifiable student subject
groups. The number of correct answers ranged from
9 to 20 with a mean of 15.49 or 73.8%. MBAs
answered 1.2 more questions correctly than under-
graduates (P = 0.002). There were no significant
differences in knowledge among the three under-
graduate groups. The mean number of correct
answers should be considered an upper limit on true
knowledge because true/false questions are subject to
inflation from guessing. The standard correction
for guessing yields a corrected mean of 9.98 for
Knowledge regarding organ donation
Table I. Distribution of student subjects by total number of correct responses
Subject group
793
Number of Pmxperiment Experiment Overall
correct responses Undergraduates MBA Experimental Control Percent
9
IO
II
12
13
14
I5
I6
I7
I8
I9
20
Mean number
0
0
3
4
9
f9
::
IO
;
21
32
39
27
14
1
^
4
1
8
I2
I9
24
35
20
20
0.3
0.9
2.3
4.5
8.9
13.2
17.0
21.3
15.7
10.4
4.0
I.1
correct= IS.38 16.62 IS.32 15.56 15.49
N- 112 26 179 I53 470
Eleven subjects were excluded because of missing data on one or more knowledge questions.
undergraduates, 12.24 for MBAs or 47.5 and 58.3%,
respectively.* These corrected means. however, are
ambiguous because subjects’ responses for unknown
answers are undoubtedly influenced by such things as
cultural biases in addition to simple guessing.
The higher level of knowledge of MBAs, who were
all part-time students, is most likely accounted for by
the many normal correlates of age and the greater
exposure of MBAs to the mass media. For all subject
groups, however, there are clearly deficiencies in
overall knowledge regarding organ donation. Far
more interesting, however, is the fact that the level of
correct response varies widely by question.
The 21 knowledge questions, correct answer for
each question, and percent of subjects answering
correctly are displayed in Table 2. The large sample
size means that these sample percentages are rather
close estimates of their corresponding population
values.7 In interpreting the data the normal upward
bias of true/false questions should be kept in mind.
Eight of the 21 questions were answered correctly
by 88% or more of the subjects, with six additional
questions answered correctly by 76% or more of the
subjects. In general these correct responses indicate
that subjects were aware of the inadequate supply of
organs, of the increasing cost effectiveness of certain
transplant operations, and of a number of aspects
of normal organ donation procedures and their
*The standard correction for guessing for true/false ques-
tions assumes that known answers are reported accu-
rately whereas unknown answers are reported correct at
the rate of 50%. This leads to a correction eauation of.
correct minus incorrect or, in the aggregate, percent
correct minus percent incorrrect.
Standard errors of the proportion of answers correct
ranged from 0.0077 to 0.0228 and averaged 0.0169. This
gives an average error of approx. 3.3% and a maximum
error of approx. 4.5% at the 95% level of confidence.
iAlthough racial data was not collected, it should be noted
that there were almost no blacks in the student sample.
This racial imbalance is consistent with the racial com-
position of the student population. For the community
sample racial identification was requested. Approxi-
mately 99% of the respondents identified themselves as
white. The absence of blacks is consistent with the racial
composition of the community.
consequences. Specifically, subjects were generally
correct in answering questions regarding who is
eligible to donate, the necessity of permission from
the donor or next of kin, and the fact that donation
does not normally interfere with funeral arrange-
ments. While it is likely that such factors as random
guessing and answering in accord with generally
accepted values in our society bias the percent correct
(e.g. the right to privacy would appear inconsistent
with ‘presumed consent’ laws), the relatively high
correct response to these questions is consistent
with national surveys such as Gallup [ 161 that find a
high degree of general public awareness of organ
transplantation.
Of the remaining seven questions, three were cor-
rectly answered by 58-69% of the subjects. These
questions concerned the impossibility of guaranteeing
that a donor’s organs will actually be transplanted,
the legal proscription of financial gain of any kind
to the donor’s family, and the fact that different
racial and socioeconomic groups are not equally
represented among donors.$ Assuming some upward
bias, the responses to these questions identify
potential gaps in public knowledge regarding organ
donation.
The most interesting data concerns the four ques-
tions that were answered correctly by fewer than half
of the respondents and potentially constitute serious
barriers to becoming a potential organ donor. Stated
in terms of implied beliefs, 61.5% indicated that at
least some major Western religions do not support
organ donation. 79.3% of the respondents indicated
that the cessation of all pulmonary activity was
necessary before a donor’s organs can be removed.
Although 77.2% of the subjects responded correctly
to the brain death question, one possible implication
is that current perceptions of brain death include
the cessation of all pulmonary activity. 55.8% of the
respondents indicated that they thought it not uneth-
ical for the same physician to have primary responsi-
bility for donor and donee. While the present data
cannot determine what subjects actually believe re-
garding current practices, a lack of awareness of the
efforts made to protect the interests of the donor [ 171
is suggested by the responses to this question. Finally,
73.5% of the respondents indicated that a donor card
Table I. Distribution of student subjects by total number of correct responses
Subject group
793
Number of Pmxperiment Experiment Overall
correct responses Undergraduates MBA Experimental Control Percent
9
IO
II
12
13
14
I5
I6
I7
I8
I9
20
Mean number
0
0
3
4
9
f9
::
IO
;
21
32
39
27
14
1
^
4
1
8
I2
I9
24
35
20
20
0.3
0.9
2.3
4.5
8.9
13.2
17.0
21.3
15.7
10.4
4.0
I.1
correct= IS.38 16.62 IS.32 15.56 15.49
N- 112 26 179 I53 470
Eleven subjects were excluded because of missing data on one or more knowledge questions.
undergraduates, 12.24 for MBAs or 47.5 and 58.3%,
respectively.* These corrected means. however, are
ambiguous because subjects’ responses for unknown
answers are undoubtedly influenced by such things as
cultural biases in addition to simple guessing.
The higher level of knowledge of MBAs, who were
all part-time students, is most likely accounted for by
the many normal correlates of age and the greater
exposure of MBAs to the mass media. For all subject
groups, however, there are clearly deficiencies in
overall knowledge regarding organ donation. Far
more interesting, however, is the fact that the level of
correct response varies widely by question.
The 21 knowledge questions, correct answer for
each question, and percent of subjects answering
correctly are displayed in Table 2. The large sample
size means that these sample percentages are rather
close estimates of their corresponding population
values.7 In interpreting the data the normal upward
bias of true/false questions should be kept in mind.
Eight of the 21 questions were answered correctly
by 88% or more of the subjects, with six additional
questions answered correctly by 76% or more of the
subjects. In general these correct responses indicate
that subjects were aware of the inadequate supply of
organs, of the increasing cost effectiveness of certain
transplant operations, and of a number of aspects
of normal organ donation procedures and their
*The standard correction for guessing for true/false ques-
tions assumes that known answers are reported accu-
rately whereas unknown answers are reported correct at
the rate of 50%. This leads to a correction eauation of.
correct minus incorrect or, in the aggregate, percent
correct minus percent incorrrect.
Standard errors of the proportion of answers correct
ranged from 0.0077 to 0.0228 and averaged 0.0169. This
gives an average error of approx. 3.3% and a maximum
error of approx. 4.5% at the 95% level of confidence.
iAlthough racial data was not collected, it should be noted
that there were almost no blacks in the student sample.
This racial imbalance is consistent with the racial com-
position of the student population. For the community
sample racial identification was requested. Approxi-
mately 99% of the respondents identified themselves as
white. The absence of blacks is consistent with the racial
composition of the community.
consequences. Specifically, subjects were generally
correct in answering questions regarding who is
eligible to donate, the necessity of permission from
the donor or next of kin, and the fact that donation
does not normally interfere with funeral arrange-
ments. While it is likely that such factors as random
guessing and answering in accord with generally
accepted values in our society bias the percent correct
(e.g. the right to privacy would appear inconsistent
with ‘presumed consent’ laws), the relatively high
correct response to these questions is consistent
with national surveys such as Gallup [ 161 that find a
high degree of general public awareness of organ
transplantation.
Of the remaining seven questions, three were cor-
rectly answered by 58-69% of the subjects. These
questions concerned the impossibility of guaranteeing
that a donor’s organs will actually be transplanted,
the legal proscription of financial gain of any kind
to the donor’s family, and the fact that different
racial and socioeconomic groups are not equally
represented among donors.$ Assuming some upward
bias, the responses to these questions identify
potential gaps in public knowledge regarding organ
donation.
The most interesting data concerns the four ques-
tions that were answered correctly by fewer than half
of the respondents and potentially constitute serious
barriers to becoming a potential organ donor. Stated
in terms of implied beliefs, 61.5% indicated that at
least some major Western religions do not support
organ donation. 79.3% of the respondents indicated
that the cessation of all pulmonary activity was
necessary before a donor’s organs can be removed.
Although 77.2% of the subjects responded correctly
to the brain death question, one possible implication
is that current perceptions of brain death include
the cessation of all pulmonary activity. 55.8% of the
respondents indicated that they thought it not uneth-
ical for the same physician to have primary responsi-
bility for donor and donee. While the present data
cannot determine what subjects actually believe re-
garding current practices, a lack of awareness of the
efforts made to protect the interests of the donor [ 171
is suggested by the responses to this question. Finally,
73.5% of the respondents indicated that a donor card
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
794 RAYMOND L. HORTON and PAIXICVI J. HORTON
Table 2. Organ donation knowledge survey-percent correct responses for student subjects
Instructions to subjects: Each of the followingtrue/false questions concerns some fact about organ donation or the act of becomingan organ
donor. All questions pertain to the donation of organs after one’s death and specifically exclude blood donation and donation of a single
kidney by a living donor. For each question there is a single correct answer. Please answer all questions by circling either T (for true) or
F (for false)
Percent
correct
correct
answer Ouestion
88.9 T
97. I F
38.5 T
20.7 F
88.5 F
92.3 T
44.2 T
89.5 F
58.7 F
80.7 T
92.0 T
95.8 F
94. I T
79.8 T
63.9 F
84.2 T
77.2 T
83.8 F
26.5 F
76.6 T
68.8 F
I. Under the Uniform Anatomical Gift Act, any mentally competent person, 18 years of age or older. can
become a potential organ donor simply by signing an organ donation card in the presence of two witnesses
who also sign the card.
2. Once signed, an organ donation card is irrevocable.
3. Almost all Western religious groups support the concept of organ donation.
4. Before a donor’s organs can be removed, a physician must certify that the potential donor’s heart has ceased
to function and that all pulmonary activity has ceased.
5. The procedures necessary to remove a donor’s organs often make it impossible to have an open casket funeral.
6. The donor’s family is not responsible for the hospital and surgery costs for removing, preserving, and
transporting the donor’s organs.
7. It is considered unethical for the same physician to have primary responsibility for the care of both the organ
donor and the organ donee.
8. Anyone over the age of 40 is not acceptable as an organ donor.
9. A benefit of donating one’s organs is that, if requested, it is often possible to get sufficient compensation to
offset the cost of burial.
IO. Under the Uniform Anatomical Gift Act, your wish to donate your own organs. properly documented by
an organ donor card, takes legal precedence over the wishes of your next of kin.
Il. For some types of organ transplants it is less expensive to do the transplant operation than to provide terminal
care for the patient.
12. A physician is legally empowered to donate, without permission of the decedent or the next of kin, the organs
of a patient under his or her care who has died.
13. For most organs, demand is significantly greater than supply.
14. Large sample surveys, such as Gallup. show that the majority of Americans in-principle support the concept
of organ transplantation.
IS. If death occurs in a hospital, the potential donor can be virtually certain that his or her organs will be
transplanted.
16. The process of organ donation generally does not result in any significant delay in normal funeral
arrangements.
17. Brain death occurs when there is irreversible cessation of all functions of the entire brain, including the brain
stem.
18. A majority of states now have so-called ‘presumed consent’ laws that presume that a deceased person has
given consent to have his or her organsremoved for purposes of transplantation unless a written declaration
to the contrary exists.
19. For an organ donor card to be valid, a copy must be filed with the U.S. Department of Health and Human
Services.
20. The ‘ideal’ donor is a young adult who has died of a head injury.
21. Organ donors tend to come, relative to the size of the population, equally from all racial and socioeconomic
is valid only if it is on file with the U.S. Department
of Health and Human Services.
Three additional analyses were conducted to assess
the relationships among the knowledge questions and
the attitudinal, willingness to donate, and behavioral
measures. First, correlations were computed between
total knowledge and attitude towards organ
donation, whether the subject carried or had carried
an organ donor card, whether the subject requested
an organ donor card, and willingness to donate the
organs of a loved one or one’s own organs at the time
of death. Table 3 presents the data.
With one exception, which is nonsignificant, all
of the correlations in Table 3 are, as expected,
positive. All of the significant correlations are also
small. An interesting result is that the undergraduate
Table 3. Correlations between total knowledge and attitude towards organ donation (Attitude), carrying
organ donor card (Card), requesting organ donor card (Request), and willingness to donate the organs
of a loved one (Wol) and oneself (Wxlf) for student subjects
Variable
Subject group Attitude Card Request Wol Wself
Preexperiment
Undergraduates 0.046 0.223. N/A -0.091 O.OJ3
(107) (109) (109) (109)
MBA students 0.257 0.420’ NIA 0.131 0.197
(24) (26) (24) (24)
Experiment
Experimental subjects 0.223*** N/A 0.233. N/A N/A
(178) (129)
Control subjects 0.265”’ 0.314*** 0.315*** 0.161” 0.253..
(148) (152) (153) (153) 053)
All groups 0.193*** 0.294*** 0.259” 0.066 0.175***
(457) (287) (332) (286) (286)
l P -z 0.05, l *P < 0.01, l **P < 0.001. Sample size in parentheses below correlation. The correlations
between all questions and the card and request measures are polyxrial correlations [30]. All other
correlations are Pearson product-moment correlations.
Table 2. Organ donation knowledge survey-percent correct responses for student subjects
Instructions to subjects: Each of the followingtrue/false questions concerns some fact about organ donation or the act of becomingan organ
donor. All questions pertain to the donation of organs after one’s death and specifically exclude blood donation and donation of a single
kidney by a living donor. For each question there is a single correct answer. Please answer all questions by circling either T (for true) or
F (for false)
Percent
correct
correct
answer Ouestion
88.9 T
97. I F
38.5 T
20.7 F
88.5 F
92.3 T
44.2 T
89.5 F
58.7 F
80.7 T
92.0 T
95.8 F
94. I T
79.8 T
63.9 F
84.2 T
77.2 T
83.8 F
26.5 F
76.6 T
68.8 F
I. Under the Uniform Anatomical Gift Act, any mentally competent person, 18 years of age or older. can
become a potential organ donor simply by signing an organ donation card in the presence of two witnesses
who also sign the card.
2. Once signed, an organ donation card is irrevocable.
3. Almost all Western religious groups support the concept of organ donation.
4. Before a donor’s organs can be removed, a physician must certify that the potential donor’s heart has ceased
to function and that all pulmonary activity has ceased.
5. The procedures necessary to remove a donor’s organs often make it impossible to have an open casket funeral.
6. The donor’s family is not responsible for the hospital and surgery costs for removing, preserving, and
transporting the donor’s organs.
7. It is considered unethical for the same physician to have primary responsibility for the care of both the organ
donor and the organ donee.
8. Anyone over the age of 40 is not acceptable as an organ donor.
9. A benefit of donating one’s organs is that, if requested, it is often possible to get sufficient compensation to
offset the cost of burial.
IO. Under the Uniform Anatomical Gift Act, your wish to donate your own organs. properly documented by
an organ donor card, takes legal precedence over the wishes of your next of kin.
Il. For some types of organ transplants it is less expensive to do the transplant operation than to provide terminal
care for the patient.
12. A physician is legally empowered to donate, without permission of the decedent or the next of kin, the organs
of a patient under his or her care who has died.
13. For most organs, demand is significantly greater than supply.
14. Large sample surveys, such as Gallup. show that the majority of Americans in-principle support the concept
of organ transplantation.
IS. If death occurs in a hospital, the potential donor can be virtually certain that his or her organs will be
transplanted.
16. The process of organ donation generally does not result in any significant delay in normal funeral
arrangements.
17. Brain death occurs when there is irreversible cessation of all functions of the entire brain, including the brain
stem.
18. A majority of states now have so-called ‘presumed consent’ laws that presume that a deceased person has
given consent to have his or her organsremoved for purposes of transplantation unless a written declaration
to the contrary exists.
19. For an organ donor card to be valid, a copy must be filed with the U.S. Department of Health and Human
Services.
20. The ‘ideal’ donor is a young adult who has died of a head injury.
21. Organ donors tend to come, relative to the size of the population, equally from all racial and socioeconomic
is valid only if it is on file with the U.S. Department
of Health and Human Services.
Three additional analyses were conducted to assess
the relationships among the knowledge questions and
the attitudinal, willingness to donate, and behavioral
measures. First, correlations were computed between
total knowledge and attitude towards organ
donation, whether the subject carried or had carried
an organ donor card, whether the subject requested
an organ donor card, and willingness to donate the
organs of a loved one or one’s own organs at the time
of death. Table 3 presents the data.
With one exception, which is nonsignificant, all
of the correlations in Table 3 are, as expected,
positive. All of the significant correlations are also
small. An interesting result is that the undergraduate
Table 3. Correlations between total knowledge and attitude towards organ donation (Attitude), carrying
organ donor card (Card), requesting organ donor card (Request), and willingness to donate the organs
of a loved one (Wol) and oneself (Wxlf) for student subjects
Variable
Subject group Attitude Card Request Wol Wself
Preexperiment
Undergraduates 0.046 0.223. N/A -0.091 O.OJ3
(107) (109) (109) (109)
MBA students 0.257 0.420’ NIA 0.131 0.197
(24) (26) (24) (24)
Experiment
Experimental subjects 0.223*** N/A 0.233. N/A N/A
(178) (129)
Control subjects 0.265”’ 0.314*** 0.315*** 0.161” 0.253..
(148) (152) (153) (153) 053)
All groups 0.193*** 0.294*** 0.259” 0.066 0.175***
(457) (287) (332) (286) (286)
l P -z 0.05, l *P < 0.01, l **P < 0.001. Sample size in parentheses below correlation. The correlations
between all questions and the card and request measures are polyxrial correlations [30]. All other
correlations are Pearson product-moment correlations.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Knowledge regarding organ donation
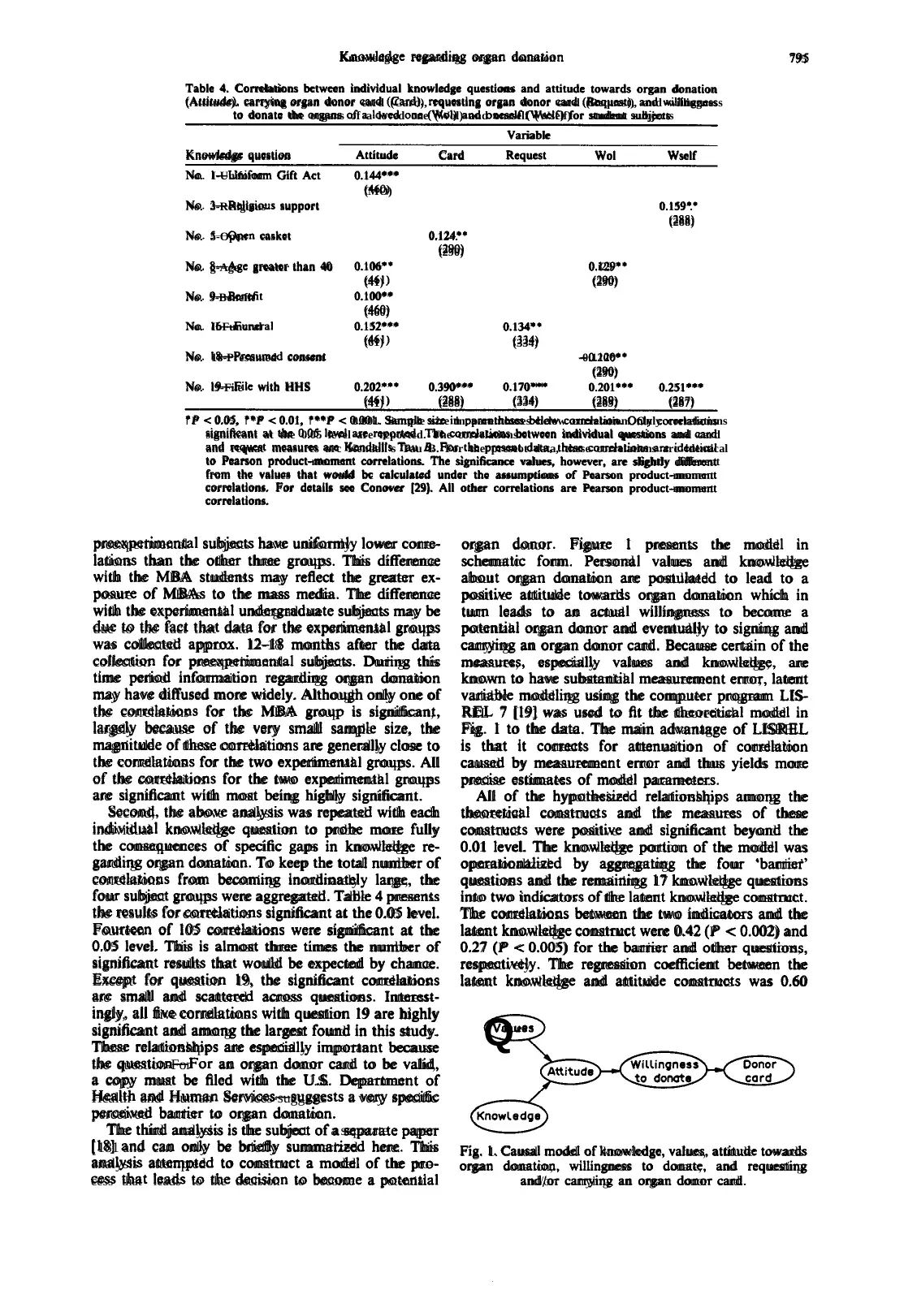
Table 4. Correlations bctwcen individual knowledge questions and attitude towards organ donation
(Attitude). carrying organ donor card (Card), rquesting organ donor card (Request), and willingness
to donate the organs of a loved one (Wol) and oneself (Wself)for student subjects
Variable
Knowledge question Attitude Card Request Wol Wself
No. I-Uniform Gift Act 0.144***
(MO)
No. 3-Religious support 0.159’.
(288)
No. 5-Open casket 0.124.’
(290)
No. g-Age greater than 40 0.106” 0.i29”
(41) (290)
No. 9-Benefit 0.100**
(460)
No. IbFuncral 0.152*** 0.134”
(61) (334)
No. 18-Presumed consent -0.120**
(290)
No. l9-File with HHS 0.202”’ 0.390*** 0.170’** 0.201*** 0.251***
(41) (288) (334) (289) (287)
l P < 0.05, l *P < 0.01, l **P < 0.001. Sample size in parentheses below correlation. Only correlations
significant at the 0.05 level are rcportcd. The correlationsbetween individual questions and card
and rcquat measures arc Kendall’s Tau B. For the prcseot data, these correlations arc identical
to Pearson product-moment correlations. The significance values, however, are slightly different
from the values that would bc calculated under the assumptions of Pearson product-moment
correlations. For details see Conover [29). All other correlations are Pearson product-moment
795
correlations.
preexperimental subjects have uniformly lower corre-
lations than the other three groups. This difference
with the MBA students may reflect the greater ex-
posure of MBAs to the mass media. The difference
with the experimental undergraduate subjects may be
due to the fact that data for the experimental groups
was collected approx. 12-18 months after the data
collection for preexperimental subjects. During this
time period information regarding organ donation
may have diffused more widely. Although only one of
the correlations for the MBA group is significant,
largely because of the very small sample size, the
magnitude of these correlations are generally close to
the correlations for the two experimental groups. All
of the correlations for the two experimental groups
are significant with most being highly significant.
Second, the above analysis was repeated with each
individual knowledge question to probe more fully
the consequences of specific gaps in knowledge re-
garding organ donation. To keep the total number of
correlations from becoming inordinately large, the
four subject groups were aggregated. Table 4 presents
the results for correlations significant at the 0.05 level.
Fourteen of I05 correlations were significant at the
0.05 level. This is almost three times the number of
significant results that would be expected by chance.
Except for question 19, the significant correlations
are small and scattered across questions. Interest-
ingly, all five correlations with question I9 are highly
significant and among the largest found in this study.
These relationships are especially important because
the question-For an organ donor card to be valid,
a copy must be filed with the U.S. Department of
Health and Human Services-suggests a very specific
perceived barrier to organ donation.
The third analysis is the subject of a separate paper
[ 181 and can only be briefly summarized here. This
analysis attempted to construct a model of the pro-
cess that leads to the decision to become a potential
organ donor. Figure I presents the model in
schematic form. Personal values and knowledge
about organ donation are postulated to lead to a
positive attitude towards organ donation which in
turn leads to an actual willingness to become a
potential organ donor and eventually to signing and
carrying an organ donor card. Because certain of the
measures, especially values and knowledge, are
known to have substantial measurement error, latent
variable modeling using the computer program LIS-
REL 7 [I91 was used to fit the theoretical model in
Fig. I to the data. The main advantage of LISREL
is that it corrects for attenuation of correlation
caused by measurement error and thus yields more
precise estimates of model parameters.
All of the hypothesized relationships among the
theoretical constructs and the measures of these
constructs were positive and significant beyond the
0.01 level. The knowledge portion of the model was
operationalized by aggregating the four ‘barrier’
questions and the remaining 17 knowledge questions
into two indicators of the latent knowledge construct.
The correlations between the two indicators and the
latent knowledge construct were 0.42 (P < 0.002) and
0.27 (P < 0.005) for the barrier and other questions,
respectively. The regression coefficient between the
latent knowledge and attitude constructs was 0.60
QValues
Fig. 1. Causal model of knowledge, values, attitude towards
organ donation, willingness to donate, and requesting
and/or carrying an organ donor card.
Table 4. Correlations bctwcen individual knowledge questions and attitude towards organ donation
(Attitude). carrying organ donor card (Card), rquesting organ donor card (Request), and willingness
to donate the organs of a loved one (Wol) and oneself (Wself)for student subjects
Variable
Knowledge question Attitude Card Request Wol Wself
No. I-Uniform Gift Act 0.144***
(MO)
No. 3-Religious support 0.159’.
(288)
No. 5-Open casket 0.124.’
(290)
No. g-Age greater than 40 0.106” 0.i29”
(41) (290)
No. 9-Benefit 0.100**
(460)
No. IbFuncral 0.152*** 0.134”
(61) (334)
No. 18-Presumed consent -0.120**
(290)
No. l9-File with HHS 0.202”’ 0.390*** 0.170’** 0.201*** 0.251***
(41) (288) (334) (289) (287)
l P < 0.05, l *P < 0.01, l **P < 0.001. Sample size in parentheses below correlation. Only correlations
significant at the 0.05 level are rcportcd. The correlationsbetween individual questions and card
and rcquat measures arc Kendall’s Tau B. For the prcseot data, these correlations arc identical
to Pearson product-moment correlations. The significance values, however, are slightly different
from the values that would bc calculated under the assumptions of Pearson product-moment
correlations. For details see Conover [29). All other correlations are Pearson product-moment
795
correlations.
preexperimental subjects have uniformly lower corre-
lations than the other three groups. This difference
with the MBA students may reflect the greater ex-
posure of MBAs to the mass media. The difference
with the experimental undergraduate subjects may be
due to the fact that data for the experimental groups
was collected approx. 12-18 months after the data
collection for preexperimental subjects. During this
time period information regarding organ donation
may have diffused more widely. Although only one of
the correlations for the MBA group is significant,
largely because of the very small sample size, the
magnitude of these correlations are generally close to
the correlations for the two experimental groups. All
of the correlations for the two experimental groups
are significant with most being highly significant.
Second, the above analysis was repeated with each
individual knowledge question to probe more fully
the consequences of specific gaps in knowledge re-
garding organ donation. To keep the total number of
correlations from becoming inordinately large, the
four subject groups were aggregated. Table 4 presents
the results for correlations significant at the 0.05 level.
Fourteen of I05 correlations were significant at the
0.05 level. This is almost three times the number of
significant results that would be expected by chance.
Except for question 19, the significant correlations
are small and scattered across questions. Interest-
ingly, all five correlations with question I9 are highly
significant and among the largest found in this study.
These relationships are especially important because
the question-For an organ donor card to be valid,
a copy must be filed with the U.S. Department of
Health and Human Services-suggests a very specific
perceived barrier to organ donation.
The third analysis is the subject of a separate paper
[ 181 and can only be briefly summarized here. This
analysis attempted to construct a model of the pro-
cess that leads to the decision to become a potential
organ donor. Figure I presents the model in
schematic form. Personal values and knowledge
about organ donation are postulated to lead to a
positive attitude towards organ donation which in
turn leads to an actual willingness to become a
potential organ donor and eventually to signing and
carrying an organ donor card. Because certain of the
measures, especially values and knowledge, are
known to have substantial measurement error, latent
variable modeling using the computer program LIS-
REL 7 [I91 was used to fit the theoretical model in
Fig. I to the data. The main advantage of LISREL
is that it corrects for attenuation of correlation
caused by measurement error and thus yields more
precise estimates of model parameters.
All of the hypothesized relationships among the
theoretical constructs and the measures of these
constructs were positive and significant beyond the
0.01 level. The knowledge portion of the model was
operationalized by aggregating the four ‘barrier’
questions and the remaining 17 knowledge questions
into two indicators of the latent knowledge construct.
The correlations between the two indicators and the
latent knowledge construct were 0.42 (P < 0.002) and
0.27 (P < 0.005) for the barrier and other questions,
respectively. The regression coefficient between the
latent knowledge and attitude constructs was 0.60
QValues
Fig. 1. Causal model of knowledge, values, attitude towards
organ donation, willingness to donate, and requesting
and/or carrying an organ donor card.
796 RAYMOND L. HORTON and PATRICIA J. HORTON
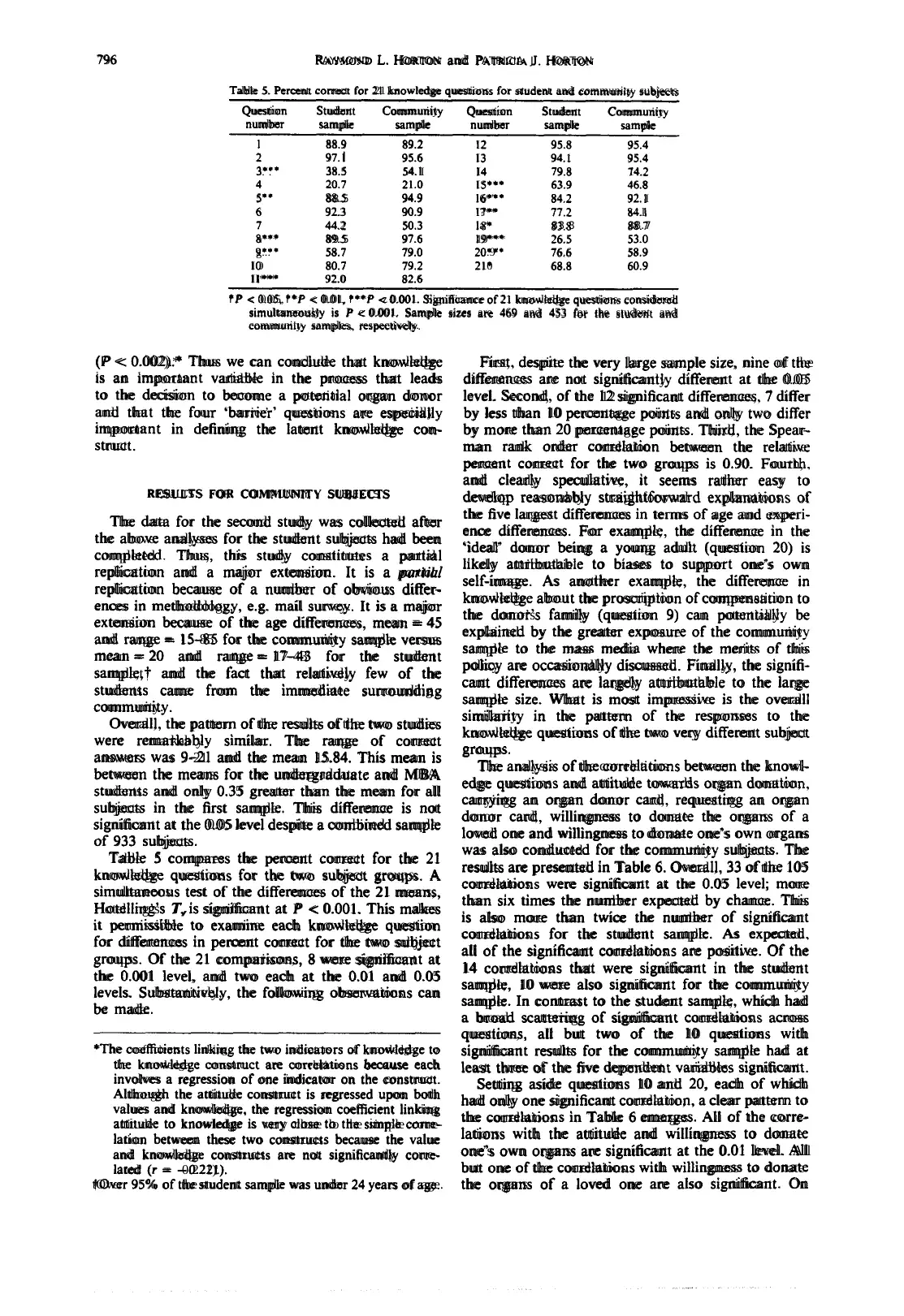
Table 5. Percent correct for 21 knowledge questions for student and community subjects
Question Student Community Question Student Community
number sample sample number sample samulc
I 88.9 89.2 I2 95.8 95.4
2 97. I 95.6 I3 94.1 95.4
3.‘. 38.5 54. I I4 79.8 14.2
4 20.7 21.0 IS*** 63.9 46.8
5” 88.5 94.9 l6*” 84.2 92. I
6 92.3 90.9 I?** 77.2 a4.l
7 44.2 50.3 la* 83.8 88.7
a*** 89.5 97.6 19*** 26.5 53.0
g... 58.7 79.0 20.9’ 76.6 58.9
IO 80.7 79.2 210 68.8 60.9
II*** 92.0 82.6
l P < 0.05, l *f < 0.01, l **f -z 0.001. Significance of 21 knowledge questions considered
simultaneously is P c 0.001. Sample sizes are 469 and 453 for the student and
community samples, respectively.
(P < 0.002).* Thus we can conclude that knowledge
is an important variable in the process that leads
to the decision to become a potential organ donor
and that the four ‘barrier’ questions are especially
important in defining the latent knowledge con-
struct.
RESULTS FOR COIMMUNITY SUBJECTS
The data for the second study was collected after
the above analyses for the student subjects had been
completed. Thus, this study constitutes a partial
replication and a major extension. It is a partial
replication because of a number of obvious differ-
ences in methodology, e.g. mail survey. It is a major
extension because of the age differences, mean = 45
and range = 15-85 for the community sample versus
mean = 20 and range = 17-43 for the student
sample,t and the fact that relatively few of the
students came from the immediate surrounding
community.
Overall, the pattern of the results of the two studies
were remarkably similar. The range of correct
answers was 9-21 and the mean 15.84. This mean is
between the means for the undergraduate and MBA
students and only 0.35 greater than the mean for all
subjects in the first sample. This difference is not
significant at the 0.05 level despite a combined sample
of 933 subjects.
Table 5 compares the percent correct for the 21
knowledge questions for the two subject groups. A
simultaneous test of the differences of the 21 means,
Hotelling’s T,is significant at P < 0.001. This makes
it permissible to examine each knowledge question
for differences in percent correct for the two subject
groups. Of the 21 comparisons, 8 were significant at
the 0.001 level, and two each at the 0.01 and 0.05
levels. Substantively, the following observations can
be made.
*The coefficients linking the two indicators of knowledge to
the knowledge construct are correlations because each
involves a regression of one indicator on the construct.
Although the attitude construct is regressed upon both
values and knowledge, the regression coefficient linking
attitude to knowledge is very close lo the simple cotre-
lation between these two constructs because the value
and knowledge constructs are not significantly corre-
lated (r = -0.221).
tOver 95% of the student sample was under 24 years of age.
First, despite the very large sample size, nine of the
differences are not significantly different at the 0.05
level. Second, of the 12 significant differences, 7 differ
by less than 10 percentage points and only two differ
by more than 20 percentage points. Third, the Spear-
man rank order correlation between the relative
percent correct for the two groups is 0.90. Fourth,
and clearly speculative, it seems rather easy to
develop reasonably straightforward explanations of
the five largest differences in terms of age and experi-
ence differences. For example, the difference in the
‘ideal’ donor being a young adult (question 20) is
likely attributabie to biases to support one’s own
self-image. As another example, the difference in
knowledge about the proscription of compensation to
the donor’s family (question 9) can potentially be
explained by the greater exposure of the community
sample to the mass media where the merits of this
policy are occasionally discussed. Finally, the signifi-
cant differences are largely attributable to the large
sample size. What is most impressive is the overall
similarity in the pattern of the responses to the
knowledge questions of the two very different subject
groups.
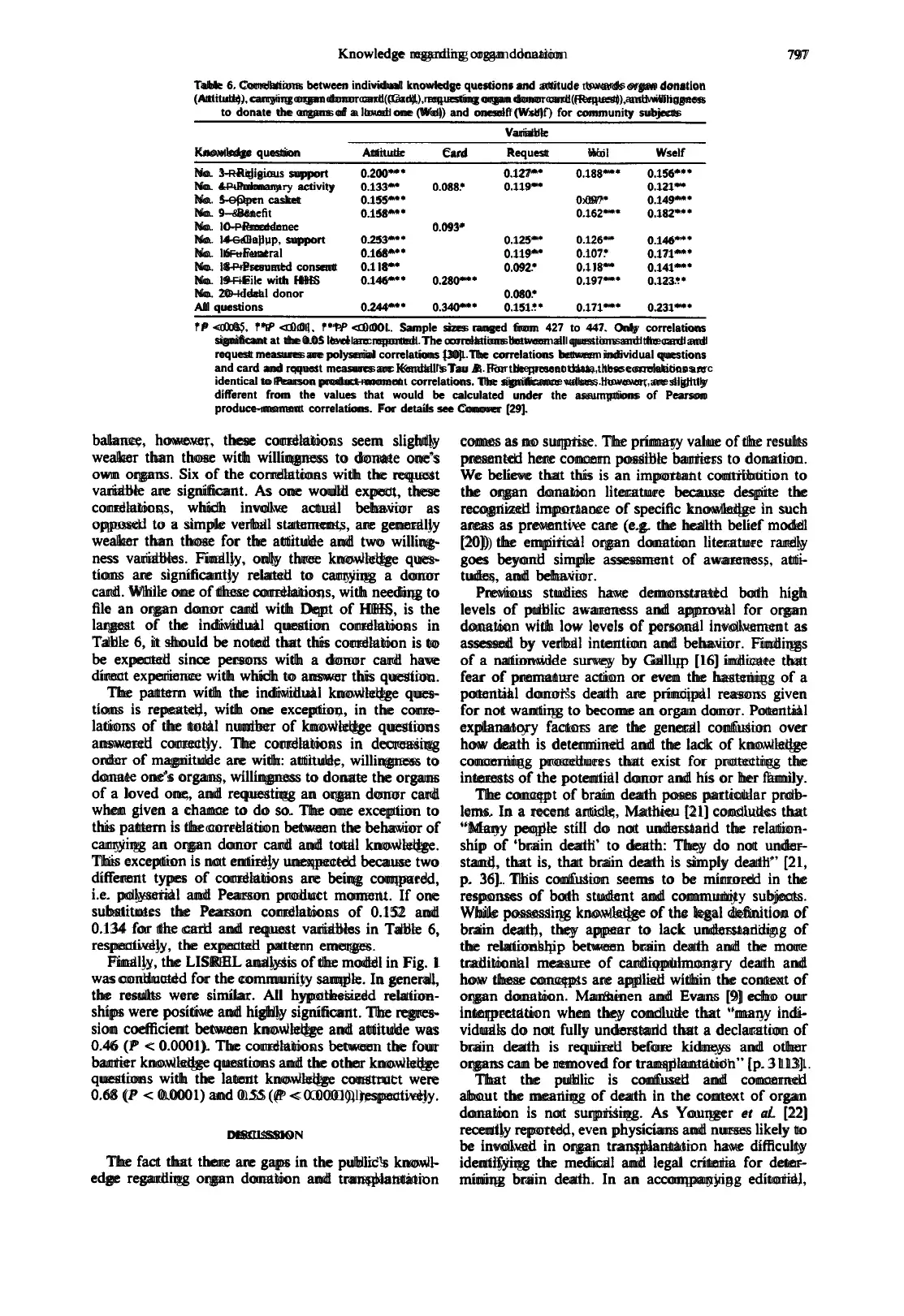
The analysis of the correlations between the knowl-
edge questions and attitude towards organ donation,
carrying an organ donor card, requesting an organ
donor card, willingness to donate the organs of a
loved one and willingness to donate one’s own organs
was also conducted for the community subjects. The
results are presented in Table 6. Overall, 33 of the 105
correlations were significant at the 0.05 level; more
than six times the number expected by chance. This
is also more than twice the number of significant
correlations for the student sample. As expected.
all of the significant correlations are positive. Of the
14 correlations that were significant in the student
sample, 10 were also significant for the community
sample. In contrast to the student sample, which had
a broad scattering of significant correlations across
questions, all but two of the 10 questions with
significant results for the community sample had at
least three of the five dependent variables significant.
Setting aside questions 10 and 20, each of which
had only one significant correlation, a clear pattern to
the correlations in Table 6 emerges. All of the corre-
lations with the attitude and willingness to donate
one’s own organs are significant at the 0.01 level. All
but one of the correlations with willingness to donate
the organs of a loved one are also significant. On
Table 5. Percent correct for 21 knowledge questions for student and community subjects
Question Student Community Question Student Community
number sample sample number sample samulc
I 88.9 89.2 I2 95.8 95.4
2 97. I 95.6 I3 94.1 95.4
3.‘. 38.5 54. I I4 79.8 14.2
4 20.7 21.0 IS*** 63.9 46.8
5” 88.5 94.9 l6*” 84.2 92. I
6 92.3 90.9 I?** 77.2 a4.l
7 44.2 50.3 la* 83.8 88.7
a*** 89.5 97.6 19*** 26.5 53.0
g... 58.7 79.0 20.9’ 76.6 58.9
IO 80.7 79.2 210 68.8 60.9
II*** 92.0 82.6
l P < 0.05, l *f < 0.01, l **f -z 0.001. Significance of 21 knowledge questions considered
simultaneously is P c 0.001. Sample sizes are 469 and 453 for the student and
community samples, respectively.
(P < 0.002).* Thus we can conclude that knowledge
is an important variable in the process that leads
to the decision to become a potential organ donor
and that the four ‘barrier’ questions are especially
important in defining the latent knowledge con-
struct.
RESULTS FOR COIMMUNITY SUBJECTS
The data for the second study was collected after
the above analyses for the student subjects had been
completed. Thus, this study constitutes a partial
replication and a major extension. It is a partial
replication because of a number of obvious differ-
ences in methodology, e.g. mail survey. It is a major
extension because of the age differences, mean = 45
and range = 15-85 for the community sample versus
mean = 20 and range = 17-43 for the student
sample,t and the fact that relatively few of the
students came from the immediate surrounding
community.
Overall, the pattern of the results of the two studies
were remarkably similar. The range of correct
answers was 9-21 and the mean 15.84. This mean is
between the means for the undergraduate and MBA
students and only 0.35 greater than the mean for all
subjects in the first sample. This difference is not
significant at the 0.05 level despite a combined sample
of 933 subjects.
Table 5 compares the percent correct for the 21
knowledge questions for the two subject groups. A
simultaneous test of the differences of the 21 means,
Hotelling’s T,is significant at P < 0.001. This makes
it permissible to examine each knowledge question
for differences in percent correct for the two subject
groups. Of the 21 comparisons, 8 were significant at
the 0.001 level, and two each at the 0.01 and 0.05
levels. Substantively, the following observations can
be made.
*The coefficients linking the two indicators of knowledge to
the knowledge construct are correlations because each
involves a regression of one indicator on the construct.
Although the attitude construct is regressed upon both
values and knowledge, the regression coefficient linking
attitude to knowledge is very close lo the simple cotre-
lation between these two constructs because the value
and knowledge constructs are not significantly corre-
lated (r = -0.221).
tOver 95% of the student sample was under 24 years of age.
First, despite the very large sample size, nine of the
differences are not significantly different at the 0.05
level. Second, of the 12 significant differences, 7 differ
by less than 10 percentage points and only two differ
by more than 20 percentage points. Third, the Spear-
man rank order correlation between the relative
percent correct for the two groups is 0.90. Fourth,
and clearly speculative, it seems rather easy to
develop reasonably straightforward explanations of
the five largest differences in terms of age and experi-
ence differences. For example, the difference in the
‘ideal’ donor being a young adult (question 20) is
likely attributabie to biases to support one’s own
self-image. As another example, the difference in
knowledge about the proscription of compensation to
the donor’s family (question 9) can potentially be
explained by the greater exposure of the community
sample to the mass media where the merits of this
policy are occasionally discussed. Finally, the signifi-
cant differences are largely attributable to the large
sample size. What is most impressive is the overall
similarity in the pattern of the responses to the
knowledge questions of the two very different subject
groups.
The analysis of the correlations between the knowl-
edge questions and attitude towards organ donation,
carrying an organ donor card, requesting an organ
donor card, willingness to donate the organs of a
loved one and willingness to donate one’s own organs
was also conducted for the community subjects. The
results are presented in Table 6. Overall, 33 of the 105
correlations were significant at the 0.05 level; more
than six times the number expected by chance. This
is also more than twice the number of significant
correlations for the student sample. As expected.
all of the significant correlations are positive. Of the
14 correlations that were significant in the student
sample, 10 were also significant for the community
sample. In contrast to the student sample, which had
a broad scattering of significant correlations across
questions, all but two of the 10 questions with
significant results for the community sample had at
least three of the five dependent variables significant.
Setting aside questions 10 and 20, each of which
had only one significant correlation, a clear pattern to
the correlations in Table 6 emerges. All of the corre-
lations with the attitude and willingness to donate
one’s own organs are significant at the 0.01 level. All
but one of the correlations with willingness to donate
the organs of a loved one are also significant. On
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Knowledge regarding organ donation
Table 6. Correlations bctwcen individual knowledge questions and attitude towards organ donation
(Attitude), carrying organ donor card (Card), requesting organ donor card (Request), and willingness
to donate the organs of a loved one (Wol) and oneself (Wxlf) for community subjects
Variable
Knowledge question Attitude Card Request woi Wself
No. 3-Religious support 0.200”* 0.127** 0.188*** 0.156*‘*
No. &Pulmonary activity 0.133** 0.088. 0.119** 0.121**
No. 5-Open casket 0.155*** 0x97* 0.149***
No. 9--&r&t 0.158*** 0.162*** 0.182’**
No. IO-Precedence 0.093*
No. I4-Gallup, support 0.253*** 0.125** 0.126** 0.146’”
No. lbFuneral 0.168**’ 0.119** 0.107. 0.171***
No. l8-Presumed consent 0.1 l8** 0.092. 0.1 l8** 0.141***
No. l9-File with HHS 0.146**’ 0.280*** 0.197*** 0.123..
No. ZO-Ideal donor 0.080.
All questions 0.244*** 0.340*** 0.151.. 0.171*** 0.231***
l P ~0.05, l *P <O.Ol, l *‘P <O.OOl. Sample sizes ranged from 427 to 447. Only correlations
significant at the 0.05 level arc reported. The correlations between all questions and the card and
request measures are polyserial correlations 1301. The correlations between individual questions
and card and rquest mcasurcs arc Kendall’s Tau B. For the present data, these correlations arc
identical to Pearson product-moment correlations. The significance values. however, are slightly
different from the values that would be calculated under the assumptions of Pearson
produce-moment correlations. For details see Conover [29].
797
balance, however, these correlations seem slightly
weaker than those with willingness to donate one’s
own organs. Six of the correlations with the request
variable are significant. As one would expect, these
correlations, which involve actual behavior as
opposed to a simple verbal statements, are generally
weaker than those for the attitude and two willing-
ness variables. Finally, only three knowledge ques-
tions are significantly related to carrying a donor
card. While one of these correlations, with needing to
file an organ donor card with Dept of HHS, is the
largest of the individual question correlations in
Table 6, it should be noted that this correlation is to
be expected since persons with a donor card have
direct experience with which to answer this question.
The pattern with the individual knowledge ques-
tions is repeated, with one exception, in the corre-
lations of the total number of knowledge questions
answered correctly. The correlations in decreasing
order of magnitude are with: attitude, willingness to
donate one’s organs, willingness to donate the organs
of a loved one, and requesting an organ donor card
when given a chance to do so. The one exception to
this pattern is the correlation between the behavior of
carrying an organ donor card and total knowledge.
This exception is not entirely unexpected because two
different types of correlations are being compared,
i.e. polyserial and Pearson product moment. If one
substitutes the Pearson correlations of 0.152 and
0.134 for the card and request variables in Table 6,
respectively, the expected pattern emerges.
Finally, the LISREL analysis of the model in Fig. 1
was conducted for the community sample. In general,
the results were similar. All hypothesized relation-
ships were positive and highly significant. The regres-
sion coefficient between knowledge and attitude was
0.46 (P < 0.0001). The correlations between the four
barrier knowledge questions and the other knowledge
questions with the latent knowledge construct were
0.68 (P < 0.0001) and 0.55 (P < O.OOOl),respectively.
DISCUSSION
The fact that there are gaps in the public’s knowl-
edge regarding organ donation and transplantation
comes as no surprise. The primary value of the results
presented here concern possible barriers to donation.
We believe that this is an important contribution to
the organ donation literature because despite the
recognized importance of specific knowledge in such
areas as preventive care (e.g. the health belief model
(201) the empirical organ donation literature rarely
goes beyond simple assessment of awareness, atti-
tudes, and behavior.
Previous studies have demonstrated both high
levels of public awareness and approval for organ
donation with low levels of personal involvement as
assessed by verbal intention and behavior. Findings
of a nationwide survey by Gallup [16] indicate that
fear of premature action or even the hastening of a
potential donor’s death are principal reasons given
for not wanting to become an organ donor. Potential
explanatory factors are the general confusion over
how death is determined and the lack of knowledge
concerning procedures that exist for protecting the
interests of the potential donor and his or her family.
The concept of brain death poses particular prob-
lems. In a recent article, Mathieu [21] concludes that
“Many people still do not understand the relation-
ship of ‘brain death’ to death: They do not under-
stand, that is, that brain death is simply death” [21,
p. 361. This confusion seems to be mirrored in the
responses of both student and community subjects.
While possessing knowledge of the legal definition of
brain death, they appear to lack understanding of
the relationship between brain death and the more
traditional measure of cardiopulmonary death and
how these concepts are applied within the context of
organ donation. Man&en and Evans [9] echo our
interpretation when they conclude that “many indi-
viduals do not fully understand that a declaration of
brain death is required before kidneys and other
organs can be removed for transplantation” [p. 3 1131.
That the public is confused and concerned
about the meaning of death in the context of organ
donation is not surprising. As Younger et al. [22]
recently reported, even physicians and nurses likely to
be involved in organ transplantation have difficulty
identifying the medical and legal criteria for deter-
mining brain death. In an accompanying editorial,
Table 6. Correlations bctwcen individual knowledge questions and attitude towards organ donation
(Attitude), carrying organ donor card (Card), requesting organ donor card (Request), and willingness
to donate the organs of a loved one (Wol) and oneself (Wxlf) for community subjects
Variable
Knowledge question Attitude Card Request woi Wself
No. 3-Religious support 0.200”* 0.127** 0.188*** 0.156*‘*
No. &Pulmonary activity 0.133** 0.088. 0.119** 0.121**
No. 5-Open casket 0.155*** 0x97* 0.149***
No. 9--&r&t 0.158*** 0.162*** 0.182’**
No. IO-Precedence 0.093*
No. I4-Gallup, support 0.253*** 0.125** 0.126** 0.146’”
No. lbFuneral 0.168**’ 0.119** 0.107. 0.171***
No. l8-Presumed consent 0.1 l8** 0.092. 0.1 l8** 0.141***
No. l9-File with HHS 0.146**’ 0.280*** 0.197*** 0.123..
No. ZO-Ideal donor 0.080.
All questions 0.244*** 0.340*** 0.151.. 0.171*** 0.231***
l P ~0.05, l *P <O.Ol, l *‘P <O.OOl. Sample sizes ranged from 427 to 447. Only correlations
significant at the 0.05 level arc reported. The correlations between all questions and the card and
request measures are polyserial correlations 1301. The correlations between individual questions
and card and rquest mcasurcs arc Kendall’s Tau B. For the present data, these correlations arc
identical to Pearson product-moment correlations. The significance values. however, are slightly
different from the values that would be calculated under the assumptions of Pearson
produce-moment correlations. For details see Conover [29].
797
balance, however, these correlations seem slightly
weaker than those with willingness to donate one’s
own organs. Six of the correlations with the request
variable are significant. As one would expect, these
correlations, which involve actual behavior as
opposed to a simple verbal statements, are generally
weaker than those for the attitude and two willing-
ness variables. Finally, only three knowledge ques-
tions are significantly related to carrying a donor
card. While one of these correlations, with needing to
file an organ donor card with Dept of HHS, is the
largest of the individual question correlations in
Table 6, it should be noted that this correlation is to
be expected since persons with a donor card have
direct experience with which to answer this question.
The pattern with the individual knowledge ques-
tions is repeated, with one exception, in the corre-
lations of the total number of knowledge questions
answered correctly. The correlations in decreasing
order of magnitude are with: attitude, willingness to
donate one’s organs, willingness to donate the organs
of a loved one, and requesting an organ donor card
when given a chance to do so. The one exception to
this pattern is the correlation between the behavior of
carrying an organ donor card and total knowledge.
This exception is not entirely unexpected because two
different types of correlations are being compared,
i.e. polyserial and Pearson product moment. If one
substitutes the Pearson correlations of 0.152 and
0.134 for the card and request variables in Table 6,
respectively, the expected pattern emerges.
Finally, the LISREL analysis of the model in Fig. 1
was conducted for the community sample. In general,
the results were similar. All hypothesized relation-
ships were positive and highly significant. The regres-
sion coefficient between knowledge and attitude was
0.46 (P < 0.0001). The correlations between the four
barrier knowledge questions and the other knowledge
questions with the latent knowledge construct were
0.68 (P < 0.0001) and 0.55 (P < O.OOOl),respectively.
DISCUSSION
The fact that there are gaps in the public’s knowl-
edge regarding organ donation and transplantation
comes as no surprise. The primary value of the results
presented here concern possible barriers to donation.
We believe that this is an important contribution to
the organ donation literature because despite the
recognized importance of specific knowledge in such
areas as preventive care (e.g. the health belief model
(201) the empirical organ donation literature rarely
goes beyond simple assessment of awareness, atti-
tudes, and behavior.
Previous studies have demonstrated both high
levels of public awareness and approval for organ
donation with low levels of personal involvement as
assessed by verbal intention and behavior. Findings
of a nationwide survey by Gallup [16] indicate that
fear of premature action or even the hastening of a
potential donor’s death are principal reasons given
for not wanting to become an organ donor. Potential
explanatory factors are the general confusion over
how death is determined and the lack of knowledge
concerning procedures that exist for protecting the
interests of the potential donor and his or her family.
The concept of brain death poses particular prob-
lems. In a recent article, Mathieu [21] concludes that
“Many people still do not understand the relation-
ship of ‘brain death’ to death: They do not under-
stand, that is, that brain death is simply death” [21,
p. 361. This confusion seems to be mirrored in the
responses of both student and community subjects.
While possessing knowledge of the legal definition of
brain death, they appear to lack understanding of
the relationship between brain death and the more
traditional measure of cardiopulmonary death and
how these concepts are applied within the context of
organ donation. Man&en and Evans [9] echo our
interpretation when they conclude that “many indi-
viduals do not fully understand that a declaration of
brain death is required before kidneys and other
organs can be removed for transplantation” [p. 3 1131.
That the public is confused and concerned
about the meaning of death in the context of organ
donation is not surprising. As Younger et al. [22]
recently reported, even physicians and nurses likely to
be involved in organ transplantation have difficulty
identifying the medical and legal criteria for deter-
mining brain death. In an accompanying editorial,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
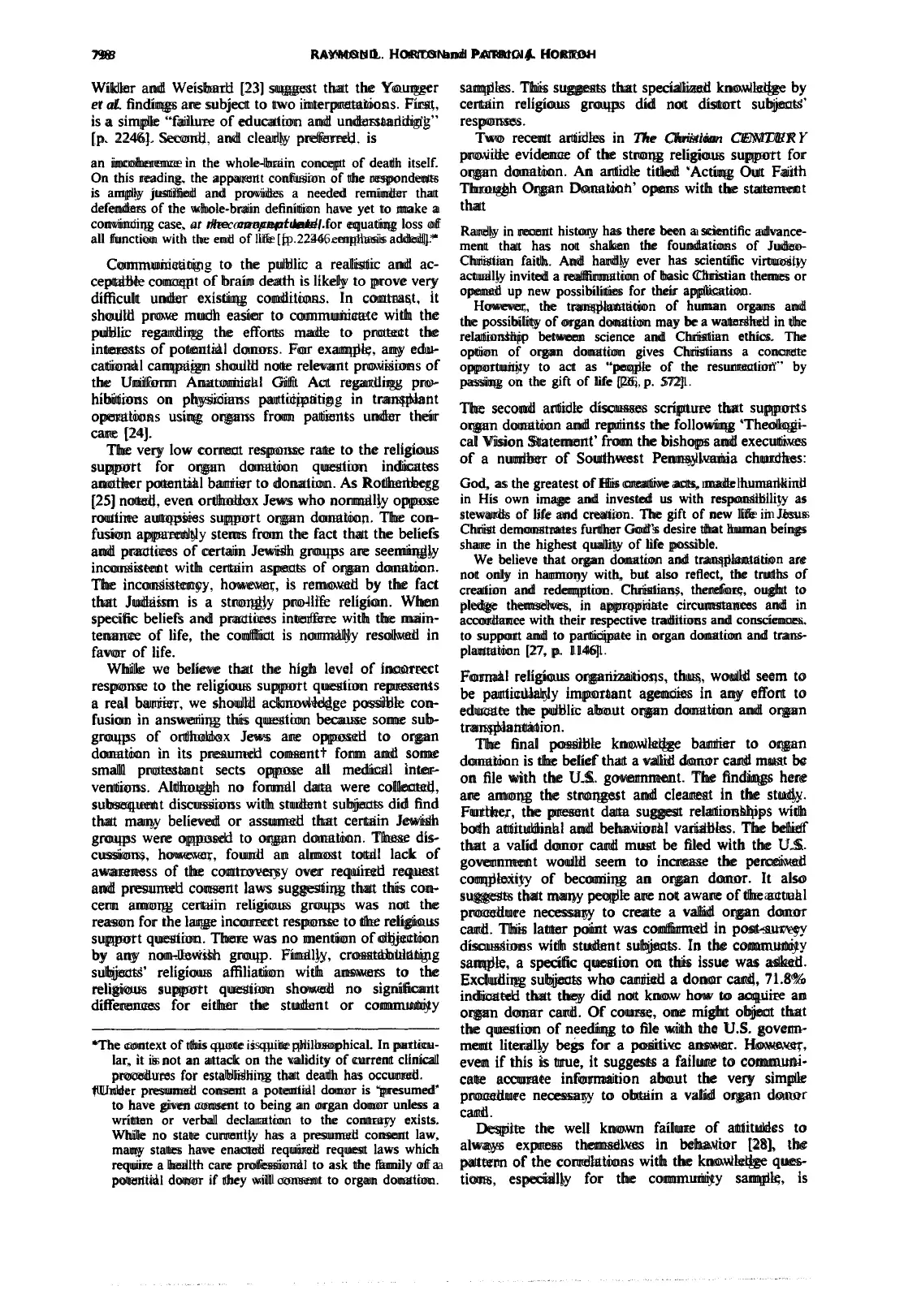
798 RAYMONDL. HORTONand PATRICIAJ. HORTOH
Wikler and Weisbard [23] suggest that the Younger
et al. findings are subject to two interpretations. First,
is a simple “failure of education and understanding”
[p. 22461. Second, and clearly preferred, is
an incoherence in the whole-brain concept of death itself.
On this reading. the apparent confusion of the respondents
is amply justified and provides a needed reminder that
defenders of the whole-brain definition have yet to make a
convincing case, ar rhe conceptuallerel.for equating loss of
all function with the end of life [p. 2246. emphasis added].*
Communicating to the public a realistic and ac-
ceptable concept of brain death is likely to prove very
difficult under existing conditions. In contrast, it
should prove much easier to communicate with the
public regarding the efforts made to protect the
interests of potential donors. For example, any edu-
cational campaign should note relevant provisions of
the Uniform Anatomical Gift Act regarding pro-
hibitions on physicians participating in transplant
operations using organs from patients under their
care [24].
The very low correct response rate to the religious
support for organ donation question indicates
another potential barrier to donation. As Rothenberg
[25] noted, even orthodox Jews who normally oppose
routine autopsies support organ donation, The con-
fusion apparently stems from the fact that the beliefs
and practices of certain Jewish groups are seemingly
inconsistent with certain aspects of organ donation.
The inconsistency, however, is removed by the fact
that Judaism is a strongly pro-life religion. When
specific beliefs and practices interfere with the main-
tenance of life, the conflict is normally resolved in
favor of life.
While we believe that the high level of incorrect
response to the religious support question represents
a real barrier, we should acknowledge possible con-
fusion in answering this question because some sub-
groups of orthodox Jews are opposed to organ
donation in its presumed consentt form and some
small protestant sects oppose all medical inter-
ventions. Although no formal data were collected,
subsequent discussions with student subjects did find
that many believed or assumed that certain Jewish
groups were opposed to organ donation. These dis-
cussions, however, found an almost total lack of
awareness of the controversy over required request
and presumed consent laws suggesting that this con-
cern among certain religious groups was not the
reason for the large incorrect response to the religious
support question. There was no mention of objection
by any non-Jewish group. Finally, crosstabulating
subjects’ religious affiliation with answers to the
religious support question showed no significant
differences for either the student or community
*The context of this quote is quite philosophical. In particu-
lar, it is not an attack on the validity of current clinical
procedures for establishing that death has occurred.
tUnder presumed consent a potential donor is ‘presumed’
to have given consent to being an organ donor unless a
written or verbal declaration to the contrary exists.
While no state currently has a presumed consent law,
many states have enacted required request laws which
require a health care professional to ask the family of a
potential donor if they will consent to organ donation.
samples. This suggests that specialized knowledge by
certain religious groups did not distort subjects’
responses.
Two recent articles in The Christian CENTURY
provide evidence of the strong religious support for
organ donation. An article titled ‘Acting Out Faith
Through Organ Donation’ opens with the statement
that
Rarely in recent history has there been a scientific advance-
ment that has not shaken the foundations of Judeo-
Christian faith. And hardly ever has scientific virtuosity
actually invited a reaffirmation of basic Christian themes or
opened up new possibilities for their application.
However, the transplantation of human organs and
the possibility of organ donation may be a watershed in the
relationship between science and Christian ethics. The
option of organ donation gives Christians a concrete
opportunity to act as “people of the resurrection” by
passing on the gift of life [26, p. 5721.
The second article discusses scripture that supports
organ donation and reprints the following ‘Theologi-
cal Vision Statement’ from the bishops and executives
of a number of Southwest Pennsylvania churches:
God, as the greatest of His creative acts, made humankind
in His own image and invested us with responsibility as
stewards of life and creation. The gift of new life in Jesus
Christ demonstrates further God’s desire that human beings
share in the highest quality of life possible.
We believe that organ donation and transplantation are
not only in harmony with, but also reflect, the truths of
creation and redemption. Christians, therefore, ought to
pledge themselves, in appropriate circumstances and in
accordance with their respective traditions and consciences.
to support and to participate in organ donation and trans-
plantation [27, p. 11461.
Formal religious organizations, thus, would seem to
be particularly important agencies in any effort to
educate the public about organ donation and organ
transplantation.
The final possible knowledge barrier to organ
donation is the belief that a valid donor card must be
on file with the U.S. government. The findings here
are among the strongest and clearest in the study.
Further, the present data suggest relationships with
both attitudinal and behavioral variables. The behef
that a valid donor card must be filed with the U.S.
government would seem to increase the perceived
complexity of becoming an organ donor. It also
suggests that many people are not aware of the actual
procedure necessary to create a valid organ donor
card. This latter point was confirmed in post-survey
discussions with student subjects. In the community
sample, a specific question on this issue was asked.
Excluding subjects who carried a donor card, 71.8%
indicated that they did not know how to acquire an
organ donar card. Of course, one might object that
the question of needing to file with the U.S. govem-
ment literally begs for a positive answer. However,
even if this is true, it suggests a failure to communi-
cate accurate information about the very simple
procedure necessary to obtain a valid organ donor
card.
Despite the well known failure of attitudes to
always express themselves in behavior [28], the
pattern of the correlations with the knowledge ques-
tions, especially for the community sample, is
Wikler and Weisbard [23] suggest that the Younger
et al. findings are subject to two interpretations. First,
is a simple “failure of education and understanding”
[p. 22461. Second, and clearly preferred, is
an incoherence in the whole-brain concept of death itself.
On this reading. the apparent confusion of the respondents
is amply justified and provides a needed reminder that
defenders of the whole-brain definition have yet to make a
convincing case, ar rhe conceptuallerel.for equating loss of
all function with the end of life [p. 2246. emphasis added].*
Communicating to the public a realistic and ac-
ceptable concept of brain death is likely to prove very
difficult under existing conditions. In contrast, it
should prove much easier to communicate with the
public regarding the efforts made to protect the
interests of potential donors. For example, any edu-
cational campaign should note relevant provisions of
the Uniform Anatomical Gift Act regarding pro-
hibitions on physicians participating in transplant
operations using organs from patients under their
care [24].
The very low correct response rate to the religious
support for organ donation question indicates
another potential barrier to donation. As Rothenberg
[25] noted, even orthodox Jews who normally oppose
routine autopsies support organ donation, The con-
fusion apparently stems from the fact that the beliefs
and practices of certain Jewish groups are seemingly
inconsistent with certain aspects of organ donation.
The inconsistency, however, is removed by the fact
that Judaism is a strongly pro-life religion. When
specific beliefs and practices interfere with the main-
tenance of life, the conflict is normally resolved in
favor of life.
While we believe that the high level of incorrect
response to the religious support question represents
a real barrier, we should acknowledge possible con-
fusion in answering this question because some sub-
groups of orthodox Jews are opposed to organ
donation in its presumed consentt form and some
small protestant sects oppose all medical inter-
ventions. Although no formal data were collected,
subsequent discussions with student subjects did find
that many believed or assumed that certain Jewish
groups were opposed to organ donation. These dis-
cussions, however, found an almost total lack of
awareness of the controversy over required request
and presumed consent laws suggesting that this con-
cern among certain religious groups was not the
reason for the large incorrect response to the religious
support question. There was no mention of objection
by any non-Jewish group. Finally, crosstabulating
subjects’ religious affiliation with answers to the
religious support question showed no significant
differences for either the student or community
*The context of this quote is quite philosophical. In particu-
lar, it is not an attack on the validity of current clinical
procedures for establishing that death has occurred.
tUnder presumed consent a potential donor is ‘presumed’
to have given consent to being an organ donor unless a
written or verbal declaration to the contrary exists.
While no state currently has a presumed consent law,
many states have enacted required request laws which
require a health care professional to ask the family of a
potential donor if they will consent to organ donation.
samples. This suggests that specialized knowledge by
certain religious groups did not distort subjects’
responses.
Two recent articles in The Christian CENTURY
provide evidence of the strong religious support for
organ donation. An article titled ‘Acting Out Faith
Through Organ Donation’ opens with the statement
that
Rarely in recent history has there been a scientific advance-
ment that has not shaken the foundations of Judeo-
Christian faith. And hardly ever has scientific virtuosity
actually invited a reaffirmation of basic Christian themes or
opened up new possibilities for their application.
However, the transplantation of human organs and
the possibility of organ donation may be a watershed in the
relationship between science and Christian ethics. The
option of organ donation gives Christians a concrete
opportunity to act as “people of the resurrection” by
passing on the gift of life [26, p. 5721.
The second article discusses scripture that supports
organ donation and reprints the following ‘Theologi-
cal Vision Statement’ from the bishops and executives
of a number of Southwest Pennsylvania churches:
God, as the greatest of His creative acts, made humankind
in His own image and invested us with responsibility as
stewards of life and creation. The gift of new life in Jesus
Christ demonstrates further God’s desire that human beings
share in the highest quality of life possible.
We believe that organ donation and transplantation are
not only in harmony with, but also reflect, the truths of
creation and redemption. Christians, therefore, ought to
pledge themselves, in appropriate circumstances and in
accordance with their respective traditions and consciences.
to support and to participate in organ donation and trans-
plantation [27, p. 11461.
Formal religious organizations, thus, would seem to
be particularly important agencies in any effort to
educate the public about organ donation and organ
transplantation.
The final possible knowledge barrier to organ
donation is the belief that a valid donor card must be
on file with the U.S. government. The findings here
are among the strongest and clearest in the study.
Further, the present data suggest relationships with
both attitudinal and behavioral variables. The behef
that a valid donor card must be filed with the U.S.
government would seem to increase the perceived
complexity of becoming an organ donor. It also
suggests that many people are not aware of the actual
procedure necessary to create a valid organ donor
card. This latter point was confirmed in post-survey
discussions with student subjects. In the community
sample, a specific question on this issue was asked.
Excluding subjects who carried a donor card, 71.8%
indicated that they did not know how to acquire an
organ donar card. Of course, one might object that
the question of needing to file with the U.S. govem-
ment literally begs for a positive answer. However,
even if this is true, it suggests a failure to communi-
cate accurate information about the very simple
procedure necessary to obtain a valid organ donor
card.
Despite the well known failure of attitudes to
always express themselves in behavior [28], the
pattern of the correlations with the knowledge ques-
tions, especially for the community sample, is
Knowledge regarding organ donation 799
consistent with a ‘learning hierarchy’ decision making
model in which knowledge causes attitude, which in
turn causes willingness to donate and which may
eventually lead to behaviors such as requesting an
organ donor card. That is, correlations between
knowledge and the other variables are progressively
smaller as the distance between knowledge and the
other variables in the model lengthens. This fact,
coupled with the small positive correlations between
knowledge and the five attitudinal and behavioral
variables in Tables 3, 4, and 6 raises the question of
what effect increased knowledge would have if it
could be imparted while subjects’ attention was more
fully engaged in the learning process. While this is a
question that can only be answered by future re-
search, the multivariate analyses using LISREL sug-
gest that the effects of increasing knowledge on both
attitudes and behavior may be much larger than
the simple bivariate correlations suggest because the
latter are suppressed by measurement errors.
At this point we need to raise the standard caveats
regarding the distinctions between cross-sectional
and longitudinal data and between correlational and
experimental studies. The present cross-sectional,
correlational data shows positive relationships
between knowledge and the different indices of will-
ingness to donate. The next logical step in the re-
search process is to address, via an appropriate
longitudinal study, the question as to whether an
increase in knowledge will lead to an increase in
attitudes, willingness to donate, and actually obtain-
ing an organ donor card. The present study suggests
specific types of knowledge that might be subjected to
experimental investigation to address this question.
CONCLUSION
While no claim is made that the sample is represen-
tative of the general population, there are reasons to
believe that a properly constructed sample of the
U.S., and possibly, in its general relationships among
variables, Western Europe, would produce results
similar to those reported here. First 14.4% of the
student respondents and 17.5% of the community
respondents reported having signed an organ donor
card. The present samples are clearly representative
on this important characteristic. Second, the fact that
two very different subject groups gave generally
similar responses, suggests that other groups might
also yield similar profiles. Third, and finally, is the
general plausibility of the results. Nothing in the
responses of the present sample seriously contradicts
existing facts or seems implausible.
While a number of studies have reported on aware-
ness and attitudes, to the best of our knowledge the
present study is the only one which has taken a close
look at public knowledge of the many specific facts
of organ donation. The data reported here point to
several possible knowledge barriers to becoming an
organ donor. Future research needs to address two
specific questions. First, the findings reported here
need to be confirmed with a representative sample.
Second, assuming confirmation, careful experimental
studies should address the question of whether in-
creasing public knowledge regarding organ donation,
especially with respect to the four ‘barrier’ questions,
will lead to more positive attitudes towards organ
donation, a greater willingness to carry an organ
donor card, a greater willingness to donate the organs
of a deceased loved one, and, ultimately, an increase
in the supply of organs available for transplant.
Acknowledgements-The authors thank Roy Herronkohl,
Judy Lasker, Marty Richter, all of Lehigh University, and
three anonymous reviewers for helpful comments on earlier
drafts of this article. We especially appreciate the help of
Howard Nathan, Executive Director, Annette Servis,
Administrative Assistant, and the staff of the Delaware
Valley Transplant Program for their assistance in designing
the knowledge questionnaire and collecting the data for this
study.
The authors gratefully acknowledge financial support
provided by the Marketing Department, the College of
Business and Economics, the Office of Research, and the
Provost’s Office at Lehigh University.
1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
REFERENCES
DeChesser A. D. Organ donation: the supply,demand
discrepancy. Heart &Lung 15, 547-551, &I;. 1986.
Darbv J. M.. Stein K.. Grenvik A. and Stuart S. A.
Approach to. management of the heartbeating ‘brain
dead’ organ donor. J. Am. med. Ass. 261,2222-2228,21
April, 1989.
Koop C. E. Increasing the supply of solid organs for
transplantation. Publ. Hith Rep. 98, 566-572, 1983.
Lazarus R. S. Thoughts on the relation between
emotion and cognition. Am. Psycho/. 37, 1019-1024,
1982.
Petty R. E., Cacioppo J. T. and Schumann A. Central
and peripheral routes to advertising effectiveness: the
moderating role of involvement. J. Consumer Res. 10,
135-146, Sept, 1983.
Zajonc R. B. Feeling and thinking: preferences need no
inferences. Am. Psychol. 35, 151-175, Febr. 1978.
Horton R. L. Buyer Behavior: A Decision-Making
Approach. Merrill, 1984.
Prottas J. M. Encouraging altruism: public attitudes
and the marketing of organ donation. Milbank Memf
Fund Q. 61, 278-306, 1983.
Manninen D. L. and Evans R. W. Public attitudes and
behavior regarding organ donation. J. Am. med. Ass.
253, 3111-3115, 7 June, 1985.
Prottas J. M. and Batten H. L. Health nrofessionals and
hospital administrators in organ procurement: attitudes,
reservation, and their resolutions. Am. J. publ. Hlrh 78,
642-645, June lY88.
1 I. Callender C. 0. Legal and ethical issues surrounding
transplantation: the transplant teams perspective. In
Human Organ Transplanration (Edited by Cowan D. H.
ef al.), pp. 42-52. Health Administration Press, Ann
Arbor, Mi, 1987.
12. Rokeach M. The Nature of Human Values. The Free
Press, New York, 1973.
13. Goodmonson C. and Glaudin V. The relationship of
commitment free behavior and commitment behavior:
a study of attitude toward organ transplantation. J. Sot.
Issues 27, 171-183, 1971.
14. Rubin Z. and Peplau A. Belief in a just world and
reactions to another’s lot: a study of participants in the
national draft lottery. 1. Sot. Issues 29. 73-93. 1973.
15. Lonetto R. and Templer D. L. The nature of death
anxiety. In Aahxznces in Personality Assessment (Edited
by Spielberger C. D. and Butcher J. N.), Vol. 3,
pp. 14-174. Erlbaum, Potomac, MD, 1983.
16. The Gallup Organization, Inc. The U.S. public’s atti-
tudes toward organ transplants/organ donation. Con-
ducted for The American Council of Transulantation’
1985.
consistent with a ‘learning hierarchy’ decision making
model in which knowledge causes attitude, which in
turn causes willingness to donate and which may
eventually lead to behaviors such as requesting an
organ donor card. That is, correlations between
knowledge and the other variables are progressively
smaller as the distance between knowledge and the
other variables in the model lengthens. This fact,
coupled with the small positive correlations between
knowledge and the five attitudinal and behavioral
variables in Tables 3, 4, and 6 raises the question of
what effect increased knowledge would have if it
could be imparted while subjects’ attention was more
fully engaged in the learning process. While this is a
question that can only be answered by future re-
search, the multivariate analyses using LISREL sug-
gest that the effects of increasing knowledge on both
attitudes and behavior may be much larger than
the simple bivariate correlations suggest because the
latter are suppressed by measurement errors.
At this point we need to raise the standard caveats
regarding the distinctions between cross-sectional
and longitudinal data and between correlational and
experimental studies. The present cross-sectional,
correlational data shows positive relationships
between knowledge and the different indices of will-
ingness to donate. The next logical step in the re-
search process is to address, via an appropriate
longitudinal study, the question as to whether an
increase in knowledge will lead to an increase in
attitudes, willingness to donate, and actually obtain-
ing an organ donor card. The present study suggests
specific types of knowledge that might be subjected to
experimental investigation to address this question.
CONCLUSION
While no claim is made that the sample is represen-
tative of the general population, there are reasons to
believe that a properly constructed sample of the
U.S., and possibly, in its general relationships among
variables, Western Europe, would produce results
similar to those reported here. First 14.4% of the
student respondents and 17.5% of the community
respondents reported having signed an organ donor
card. The present samples are clearly representative
on this important characteristic. Second, the fact that
two very different subject groups gave generally
similar responses, suggests that other groups might
also yield similar profiles. Third, and finally, is the
general plausibility of the results. Nothing in the
responses of the present sample seriously contradicts
existing facts or seems implausible.
While a number of studies have reported on aware-
ness and attitudes, to the best of our knowledge the
present study is the only one which has taken a close
look at public knowledge of the many specific facts
of organ donation. The data reported here point to
several possible knowledge barriers to becoming an
organ donor. Future research needs to address two
specific questions. First, the findings reported here
need to be confirmed with a representative sample.
Second, assuming confirmation, careful experimental
studies should address the question of whether in-
creasing public knowledge regarding organ donation,
especially with respect to the four ‘barrier’ questions,
will lead to more positive attitudes towards organ
donation, a greater willingness to carry an organ
donor card, a greater willingness to donate the organs
of a deceased loved one, and, ultimately, an increase
in the supply of organs available for transplant.
Acknowledgements-The authors thank Roy Herronkohl,
Judy Lasker, Marty Richter, all of Lehigh University, and
three anonymous reviewers for helpful comments on earlier
drafts of this article. We especially appreciate the help of
Howard Nathan, Executive Director, Annette Servis,
Administrative Assistant, and the staff of the Delaware
Valley Transplant Program for their assistance in designing
the knowledge questionnaire and collecting the data for this
study.
The authors gratefully acknowledge financial support
provided by the Marketing Department, the College of
Business and Economics, the Office of Research, and the
Provost’s Office at Lehigh University.
1.
2.
3.
4.
5.
6.
I.
8.
9.
10.
REFERENCES
DeChesser A. D. Organ donation: the supply,demand
discrepancy. Heart &Lung 15, 547-551, &I;. 1986.
Darbv J. M.. Stein K.. Grenvik A. and Stuart S. A.
Approach to. management of the heartbeating ‘brain
dead’ organ donor. J. Am. med. Ass. 261,2222-2228,21
April, 1989.
Koop C. E. Increasing the supply of solid organs for
transplantation. Publ. Hith Rep. 98, 566-572, 1983.
Lazarus R. S. Thoughts on the relation between
emotion and cognition. Am. Psycho/. 37, 1019-1024,
1982.
Petty R. E., Cacioppo J. T. and Schumann A. Central
and peripheral routes to advertising effectiveness: the
moderating role of involvement. J. Consumer Res. 10,
135-146, Sept, 1983.
Zajonc R. B. Feeling and thinking: preferences need no
inferences. Am. Psychol. 35, 151-175, Febr. 1978.
Horton R. L. Buyer Behavior: A Decision-Making
Approach. Merrill, 1984.
Prottas J. M. Encouraging altruism: public attitudes
and the marketing of organ donation. Milbank Memf
Fund Q. 61, 278-306, 1983.
Manninen D. L. and Evans R. W. Public attitudes and
behavior regarding organ donation. J. Am. med. Ass.
253, 3111-3115, 7 June, 1985.
Prottas J. M. and Batten H. L. Health nrofessionals and
hospital administrators in organ procurement: attitudes,
reservation, and their resolutions. Am. J. publ. Hlrh 78,
642-645, June lY88.
1 I. Callender C. 0. Legal and ethical issues surrounding
transplantation: the transplant teams perspective. In
Human Organ Transplanration (Edited by Cowan D. H.
ef al.), pp. 42-52. Health Administration Press, Ann
Arbor, Mi, 1987.
12. Rokeach M. The Nature of Human Values. The Free
Press, New York, 1973.
13. Goodmonson C. and Glaudin V. The relationship of
commitment free behavior and commitment behavior:
a study of attitude toward organ transplantation. J. Sot.
Issues 27, 171-183, 1971.
14. Rubin Z. and Peplau A. Belief in a just world and
reactions to another’s lot: a study of participants in the
national draft lottery. 1. Sot. Issues 29. 73-93. 1973.
15. Lonetto R. and Templer D. L. The nature of death
anxiety. In Aahxznces in Personality Assessment (Edited
by Spielberger C. D. and Butcher J. N.), Vol. 3,
pp. 14-174. Erlbaum, Potomac, MD, 1983.
16. The Gallup Organization, Inc. The U.S. public’s atti-
tudes toward organ transplants/organ donation. Con-
ducted for The American Council of Transulantation’
1985.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
800 RAYMOND L. HORTON and PATRICIAJ. HORTON
17.
18.
19.
20.
21.
22.
Best A. Jr and Franklin L. Transfers of bodies and body
parts under the uniform anatomical gift act. ReuI Prop-
erry, Probate. & Trasr J. 15, 806-836, Winter, 1980.
Horton R. L. and Horton P. J. A model of willingness
to become a potential organ donor. Working paper,
Lehigh University, 1989.
Joreskog K. G. and Sorbom D. LISREL 7. SPSS. Inc.,
1988a.
For a recent attempt to determine the direction of causal
relationships among the constructs that comprise the
health belief model see: Chen M. and Land K. C.
Testing the health belief model: LISREL analysis of
causal relationships between health beliefs and preven-
tive dental behavior. Sot. Psycho/. Q. 49,45-60, March
1986.
Mathieu D. (Ed.) Organ Subsrirurion Technology:
Ethical, Legal, and Public Policy Issues. Westview Press,
Boulder, CO, 1988.
Younger S. J., Landefeld C. S., Co&on C. J., Juknialis,
B. W. and Leary M. ‘Brain death’ and organ retrieval.
J. Am. med. Ass. 261, 2205-2210, 21 April, 1989.
23. Wikler D. and Weisbard A. J. Appropriate confusion
over ‘brain death’. J. Am. med. Ass. 261, 246, 21 April,
1989.
24. Lee P. P. and Kissner P. Organ donation and the
uniform anatomical gift act. Surgery 100, 867-875,
1986.
25. Rothenberg L. S. Ethical issues in transplantation:
procuring body parts from trauma patients. Trauma Q.
43-51, May, 1985.
26. Moran M. Acting out faith through organ donation.
The Chrisriun CENTURY 103, 572-573, 18 June, 1986.
27. Davison J. E. Organ donation: giving the gift of life.
The Christian CENTURY 104, 1146-1148, 16 Dec.,
1986.
28. Horton R. L. The attitude-behavior relationship. In
Beacham’s Marketing Reference, Vol. I. Research Press,
Champaign, IL, 1986.
29. Conover W. J. Practical Nonparamerric Statistics, 2nd
edn. Wiley, New York, 1980.
30. Joreskog K. G. and Sorbom D. PRELIS, 2nd edn.
Scientific Software, Mooresviile, IN. 1988b.
17.
18.
19.
20.
21.
22.
Best A. Jr and Franklin L. Transfers of bodies and body
parts under the uniform anatomical gift act. ReuI Prop-
erry, Probate. & Trasr J. 15, 806-836, Winter, 1980.
Horton R. L. and Horton P. J. A model of willingness
to become a potential organ donor. Working paper,
Lehigh University, 1989.
Joreskog K. G. and Sorbom D. LISREL 7. SPSS. Inc.,
1988a.
For a recent attempt to determine the direction of causal
relationships among the constructs that comprise the
health belief model see: Chen M. and Land K. C.
Testing the health belief model: LISREL analysis of
causal relationships between health beliefs and preven-
tive dental behavior. Sot. Psycho/. Q. 49,45-60, March
1986.
Mathieu D. (Ed.) Organ Subsrirurion Technology:
Ethical, Legal, and Public Policy Issues. Westview Press,
Boulder, CO, 1988.
Younger S. J., Landefeld C. S., Co&on C. J., Juknialis,
B. W. and Leary M. ‘Brain death’ and organ retrieval.
J. Am. med. Ass. 261, 2205-2210, 21 April, 1989.
23. Wikler D. and Weisbard A. J. Appropriate confusion
over ‘brain death’. J. Am. med. Ass. 261, 246, 21 April,
1989.
24. Lee P. P. and Kissner P. Organ donation and the
uniform anatomical gift act. Surgery 100, 867-875,
1986.
25. Rothenberg L. S. Ethical issues in transplantation:
procuring body parts from trauma patients. Trauma Q.
43-51, May, 1985.
26. Moran M. Acting out faith through organ donation.
The Chrisriun CENTURY 103, 572-573, 18 June, 1986.
27. Davison J. E. Organ donation: giving the gift of life.
The Christian CENTURY 104, 1146-1148, 16 Dec.,
1986.
28. Horton R. L. The attitude-behavior relationship. In
Beacham’s Marketing Reference, Vol. I. Research Press,
Champaign, IL, 1986.
29. Conover W. J. Practical Nonparamerric Statistics, 2nd
edn. Wiley, New York, 1980.
30. Joreskog K. G. and Sorbom D. PRELIS, 2nd edn.
Scientific Software, Mooresviile, IN. 1988b.
1 out of 10
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.