Organizational Systems and Quality Leadership: RCA and FMEA Analysis
VerifiedAdded on 2023/04/21
|9
|2089
|226
Report
AI Summary
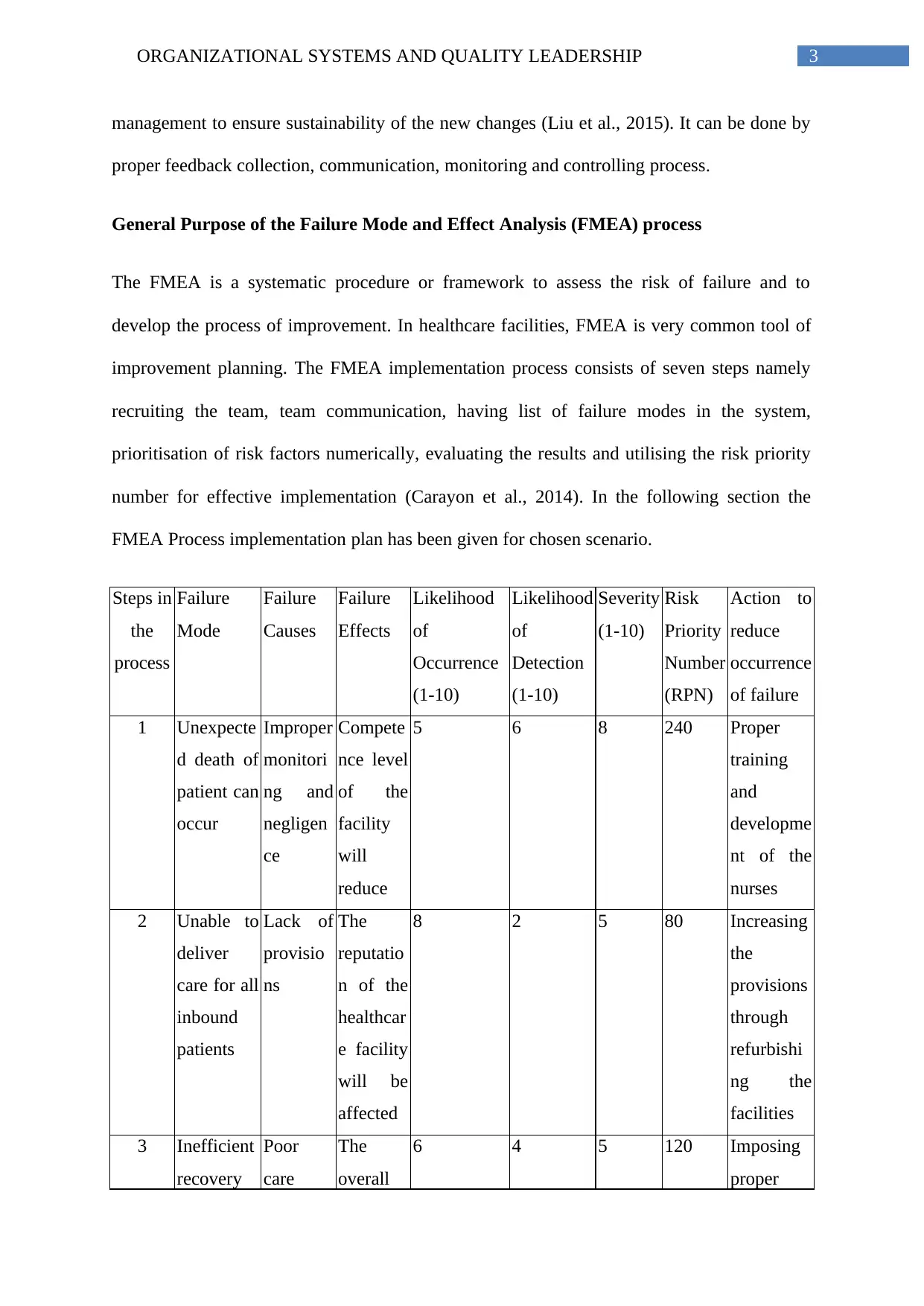
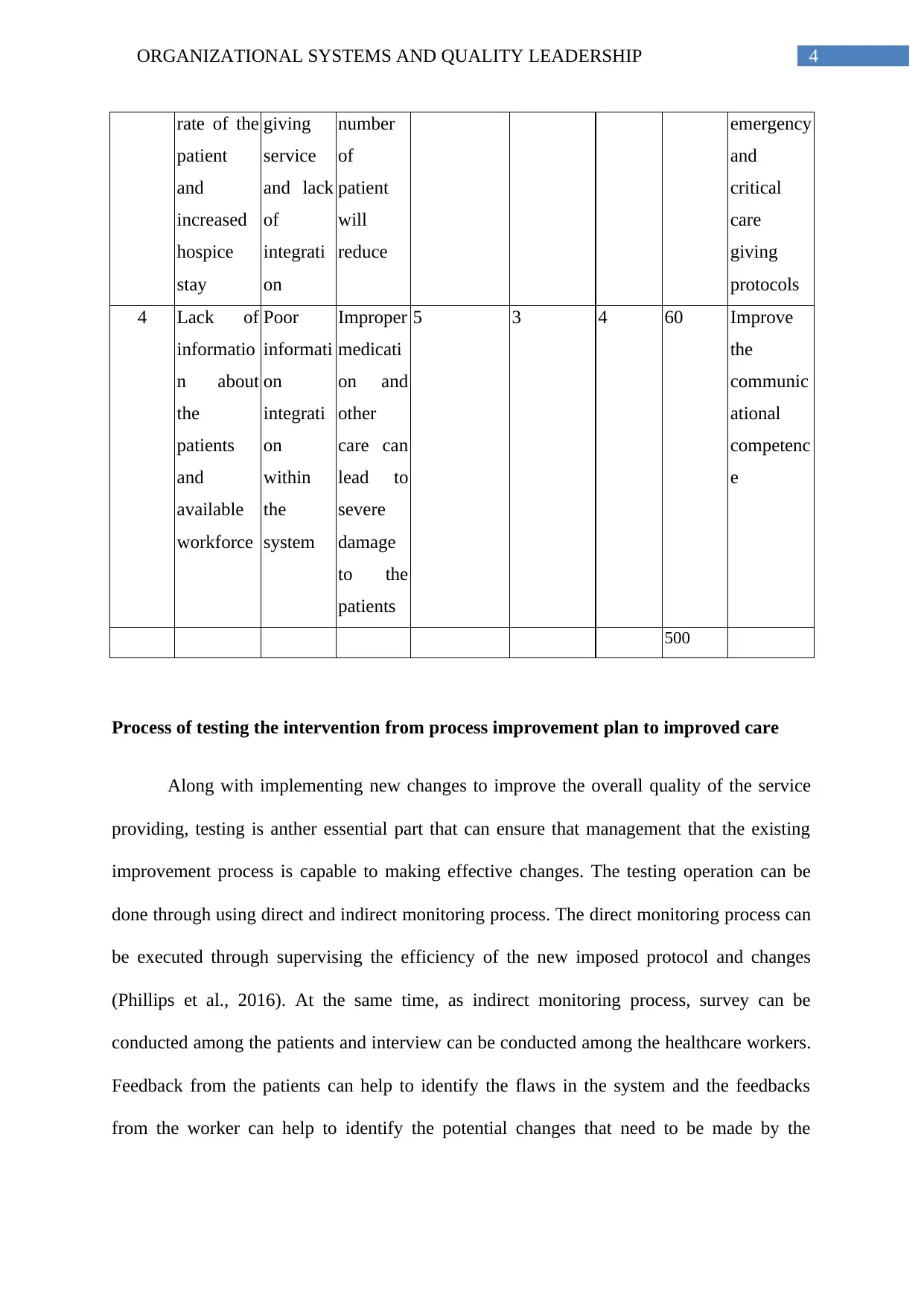
This report analyzes organizational systems and quality leadership within a healthcare context, focusing on Root Cause Analysis (RCA) and Failure Mode and Effects Analysis (FMEA). It begins by explaining the general purpose of RCA and outlines its six steps, using a case study involving a patient in an emergency department to illustrate causative and contributing factors. The report then details a process improvement plan based on Lewin's change management theory, including the 'Unfreeze, Change, and Refreeze' phases, and presents a Failure Mode and Effects Analysis (FMEA) implementation plan to assess and mitigate risks. It also discusses testing interventions, the role of professional nurses in demonstrating leadership through RCA and FMEA, and the importance of quality care and motivational programs for healthcare workers. The report concludes by emphasizing the systematic approach of RCA and FMEA in enhancing healthcare quality and patient safety, highlighting the role of leadership in promoting these improvements.


1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.