Palliative Care: Origins, Core Principles and Delivery Methods
VerifiedAdded on 2024/06/05
|10
|2018
|72
Essay
AI Summary
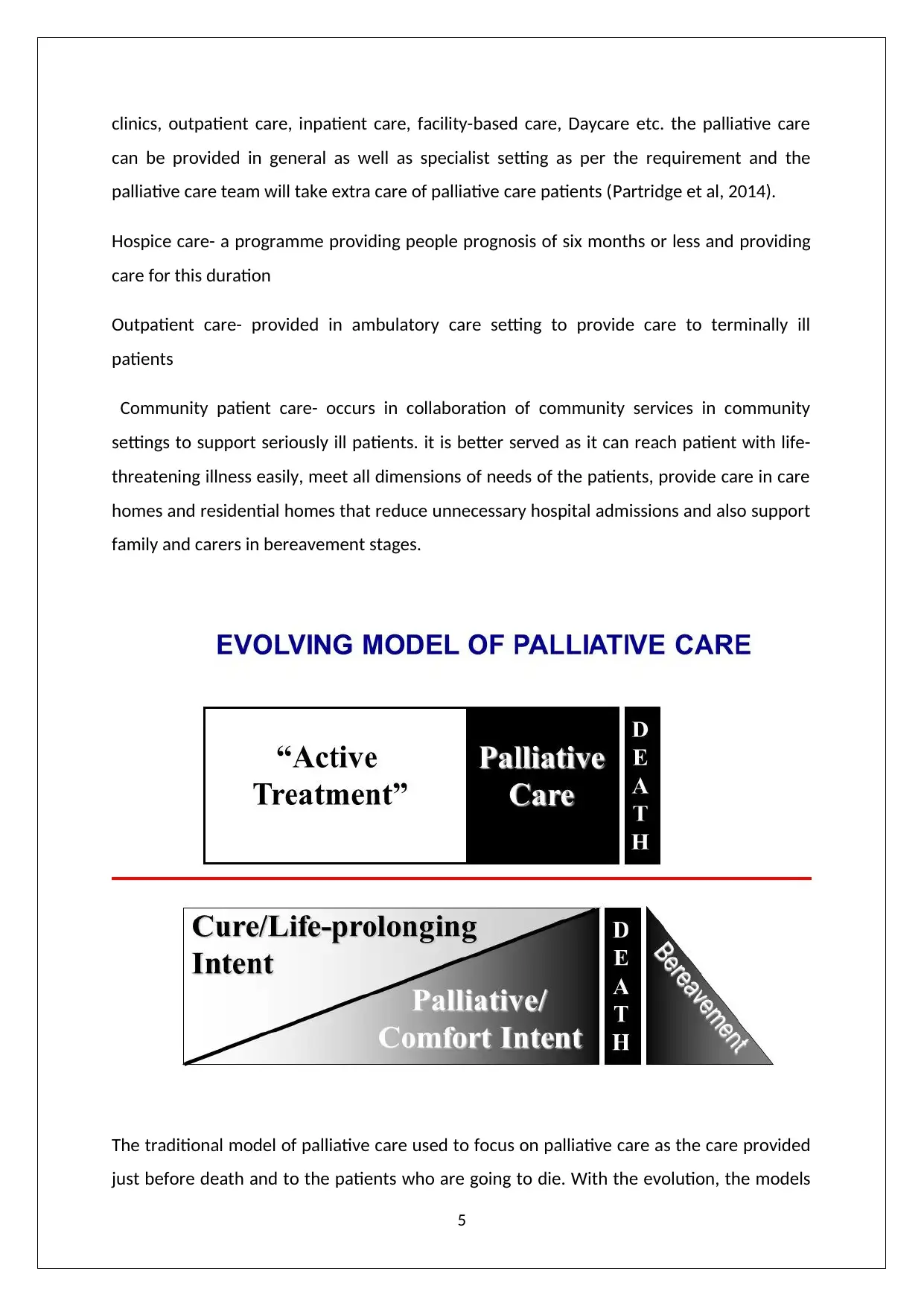
This essay provides a thorough understanding of palliative care, beginning with its origins and development, highlighting Cicely Sanders' role in the modern hospice movement and the evolution from traditional hospice care to a comprehensive approach addressing patient needs from diagnosis through end-of-life. It details the core principles of palliative care, including pain management, holistic assessment of physical, psychological, spiritual, and social needs, and support for both patients and their families. Furthermore, the essay critically examines various delivery models, such as home-based, outpatient, inpatient, and specialist settings, discussing their strengths and limitations, and emphasizing the shift towards specialist-level palliative care programs in the UK. The essay concludes by affirming the benefits of palliative care in enhancing the quality of life for terminally ill patients, relieving pain and distressing symptoms, and providing essential support to families during bereavement.



1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.