Critical Analysis of Parkinson's Disease Management Strategies
VerifiedAdded on 2022/08/26
|22
|5303
|83
Report
AI Summary
This report provides a critical examination of evidence concerning the management of Parkinson's disease. It begins with an introduction to the disease, its symptoms, and ethical considerations in patient care. The report then delves into a quantitative study, analyzing the outcomes of interventions like physiotherapy and cognitive training, supported by a clinical trial. The study involved randomizing participants into motor and cognitive motor groups, assessing them using various scales and tests. The results indicate that cognitive training combined with physiotherapy can improve quality of life and cognitive function. The report also includes a qualitative analysis, discussing the psychological concerns of patients. This research aims to understand the patient's experiences and the impact of the disease on their lives, emphasizing the importance of addressing both physical and psychological aspects of Parkinson's disease management. The report further discusses the ethical guidelines followed in the study and the statistical analysis performed to interpret the data.

Running head: PARKINSON’S DISEASE
A critical examination of evidence concerning ways of managing the Parkinson disease
Name of the Student:
Name of the University:
Author Note:
A critical examination of evidence concerning ways of managing the Parkinson disease
Name of the Student:
Name of the University:
Author Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1PARKINSON’S DISEASE
Introduction
Parkinson's disease is a chronic condition of the nervous system which affects motion
of an Individual. Symptoms begin slowly, beginning at times with an unnoticeable tremor in
just one hand. Tremors are normal but the disorder often causes movement weakness or
slowdown. Individual's face can show little or no attitude at the initial stages of Parkinson's
disease. Even it may not move the arms while walking. The voice could get soft or mumbled.
The signs of Parkinson's disease intensify as the condition progresses through period. While
it is not possible to find a remedy for Parkinson's disease, medicines could gradually improve
the noticeable symptoms. The physician may periodically recommend surgical procedure to
monitor and control certain brain regions and improve the illnesses (Postuma et al., 2015).
Symptoms
The symptoms of the disease of Parkinson's disorder can be specific for every
individual. Early indications could be mild and stay overlooked. Symptoms often start on one
side of the body, and eventually get worse on that side; even afterwards, symptoms start to
affect both sides. Symptoms usually comes up with: Tremors, bradukinesia, stiffness of
muscles, Difficulty with proper balance while walking or normal posture, Loss of automatic
movement, Fumbling speech and changes in writing pattern.
A tremor, or trembling, typically starts in the arm, often impacting with hand or
fingers. One will rub their back-and-forth of the thumb and forefinger, known as a pill-rolling
tremor. Even the hand might be shivering when it is at ease. Over time, Parkinson’s disease,
make basic activities challenging and time consuming, which may impair the mobility. When
one walk, even their steps might become shorter. Getting out of a chair can be challenging.
Individuals need to drag their feet when trying to walk. Muscle rigidity can happen in any
body part. The stiff muscles can also be painful and unpleasant and the range of movement
Introduction
Parkinson's disease is a chronic condition of the nervous system which affects motion
of an Individual. Symptoms begin slowly, beginning at times with an unnoticeable tremor in
just one hand. Tremors are normal but the disorder often causes movement weakness or
slowdown. Individual's face can show little or no attitude at the initial stages of Parkinson's
disease. Even it may not move the arms while walking. The voice could get soft or mumbled.
The signs of Parkinson's disease intensify as the condition progresses through period. While
it is not possible to find a remedy for Parkinson's disease, medicines could gradually improve
the noticeable symptoms. The physician may periodically recommend surgical procedure to
monitor and control certain brain regions and improve the illnesses (Postuma et al., 2015).
Symptoms
The symptoms of the disease of Parkinson's disorder can be specific for every
individual. Early indications could be mild and stay overlooked. Symptoms often start on one
side of the body, and eventually get worse on that side; even afterwards, symptoms start to
affect both sides. Symptoms usually comes up with: Tremors, bradukinesia, stiffness of
muscles, Difficulty with proper balance while walking or normal posture, Loss of automatic
movement, Fumbling speech and changes in writing pattern.
A tremor, or trembling, typically starts in the arm, often impacting with hand or
fingers. One will rub their back-and-forth of the thumb and forefinger, known as a pill-rolling
tremor. Even the hand might be shivering when it is at ease. Over time, Parkinson’s disease,
make basic activities challenging and time consuming, which may impair the mobility. When
one walk, even their steps might become shorter. Getting out of a chair can be challenging.
Individuals need to drag their feet when trying to walk. Muscle rigidity can happen in any
body part. The stiff muscles can also be painful and unpleasant and the range of movement
2PARKINSON’S DISEASE
can be restricted (Sveinbjornsdottir., 2016). The posture could get deteriorated, as a result of
Parkinson's disease, individuals may have issues with their balance. Including when they
walk, they may have a reduced capacity to perform unconscious motions, such as blinking of
eyes, making faces, laughing or swinging their arms. Individuals should be able to speak
softly, rapidly, whisper or pause until they communicate. Even their voice can be more of a
monotonous than the normal speech patterns. Writing can also turn out to get difficult, and
thus writing may seem low.
Ethical Guidelines While taking care of Parkinson’s disease
It always had been a matter of concern to abide by the ethical guidelines and hence four
open-ended question has been putted on into consideration whose answers were the key to
these ethical guidelines. These questions are: Receiving treatment and diagnosis about
Parkinson’s Syndrome for an individual, the effectiveness of the receiving treatment, Change
in life due to acquired Parkinson and challenges faced while living such conditions and plans
regarding the future treatments (Shaw, & Vivekananda-Schmidt., 2017).
Quantitative Study
Use of statistical and mathematical modelling to interpret and quantify the behavioral
outcomes after the decision making process is the quantitative analysis. The analysis is made
to study the outcome of the subjects who are independent of each other and thus answers a
numeric value of a framework. The study over Parkinson’s Disease was made and hence
further analysis was made based on the symptoms shown, interventions used and progress
shown by each individual.
There were attempts to perform pharmaceutical and non-pharmacological research.
Non-pharmacological alternatives are an increasing area of concern that include neuron-
stimulation, aerobic workouts, physical therapy, mental exercises, music, art, and cognitive
can be restricted (Sveinbjornsdottir., 2016). The posture could get deteriorated, as a result of
Parkinson's disease, individuals may have issues with their balance. Including when they
walk, they may have a reduced capacity to perform unconscious motions, such as blinking of
eyes, making faces, laughing or swinging their arms. Individuals should be able to speak
softly, rapidly, whisper or pause until they communicate. Even their voice can be more of a
monotonous than the normal speech patterns. Writing can also turn out to get difficult, and
thus writing may seem low.
Ethical Guidelines While taking care of Parkinson’s disease
It always had been a matter of concern to abide by the ethical guidelines and hence four
open-ended question has been putted on into consideration whose answers were the key to
these ethical guidelines. These questions are: Receiving treatment and diagnosis about
Parkinson’s Syndrome for an individual, the effectiveness of the receiving treatment, Change
in life due to acquired Parkinson and challenges faced while living such conditions and plans
regarding the future treatments (Shaw, & Vivekananda-Schmidt., 2017).
Quantitative Study
Use of statistical and mathematical modelling to interpret and quantify the behavioral
outcomes after the decision making process is the quantitative analysis. The analysis is made
to study the outcome of the subjects who are independent of each other and thus answers a
numeric value of a framework. The study over Parkinson’s Disease was made and hence
further analysis was made based on the symptoms shown, interventions used and progress
shown by each individual.
There were attempts to perform pharmaceutical and non-pharmacological research.
Non-pharmacological alternatives are an increasing area of concern that include neuron-
stimulation, aerobic workouts, physical therapy, mental exercises, music, art, and cognitive
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3PARKINSON’S DISEASE
education. In present, although certain reports have dealt with the topic, they pose analytical
shortcomings in the implementation of cognitive performance and assessment methods, such
as the lack of treatment groups, a small sample, and heterogeneity.
Cognitive conditioning may be an alternative for medical care, involving organized,
technically oriented learning of methods or controlled practice of duties that target specific
cognitive areas. In a recent meta-analysis and statistical study, it was noted that cognitive
stimulation is successful in enhancing memory in stable older individuals and in adults with
mild cognitive impairment, respectively. A recent meta-analysis of Parkinson Disease
concluded that cognitive training contributes to significant changes in cognitive function but
indicates the need for additional randomized trials in order to better examine the feasibility
for this outcome in case for Parkinson's disease. Nonetheless, the current body of evidence
suggests that cognitive training for this group suffering from PD is secure and modestly
successful.
Evidience based on Physiotherapy Versus Physiotherapy Plus Cognitive Training
on Cognition and Quality of Life in Parkinson Disease.
Natália Mariano Barboza, MSc, Marcelle Brandão Terra, MSc, Maria Eduarda
Brandão Bueno, MSc, Gustavo Christofoletti, PhD, and Suhaila Mahmoud
Smaili, PhD
Methods Undertaken
A clinical trial was randomized and was conducted among a certain population of
individuals affected with Parkinson’s disease. Based on the method of CONSORT the
randomized trial was conducted, in which the first step was finding the candidates who
required treatment regarding the disease. Upon finding the sample size with the candidates
education. In present, although certain reports have dealt with the topic, they pose analytical
shortcomings in the implementation of cognitive performance and assessment methods, such
as the lack of treatment groups, a small sample, and heterogeneity.
Cognitive conditioning may be an alternative for medical care, involving organized,
technically oriented learning of methods or controlled practice of duties that target specific
cognitive areas. In a recent meta-analysis and statistical study, it was noted that cognitive
stimulation is successful in enhancing memory in stable older individuals and in adults with
mild cognitive impairment, respectively. A recent meta-analysis of Parkinson Disease
concluded that cognitive training contributes to significant changes in cognitive function but
indicates the need for additional randomized trials in order to better examine the feasibility
for this outcome in case for Parkinson's disease. Nonetheless, the current body of evidence
suggests that cognitive training for this group suffering from PD is secure and modestly
successful.
Evidience based on Physiotherapy Versus Physiotherapy Plus Cognitive Training
on Cognition and Quality of Life in Parkinson Disease.
Natália Mariano Barboza, MSc, Marcelle Brandão Terra, MSc, Maria Eduarda
Brandão Bueno, MSc, Gustavo Christofoletti, PhD, and Suhaila Mahmoud
Smaili, PhD
Methods Undertaken
A clinical trial was randomized and was conducted among a certain population of
individuals affected with Parkinson’s disease. Based on the method of CONSORT the
randomized trial was conducted, in which the first step was finding the candidates who
required treatment regarding the disease. Upon finding the sample size with the candidates
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4PARKINSON’S DISEASE
affected with Parkinson’s syndrome some were allocated to intervention and the count stood
58. These candidates were randomized for the clinical trials (Santos et al., 2017).
Randomization and followed by Blinding
An independent researcher had a basic randomisation to conduct Persons with PD
randomized by blind randomization by means of a random number generator,
utilizing similar, opaque, sealed envelopes, and identified into "Motor Group (MG)" or
"Cognitive Motor Group (CMG)." In the case of PD, the number generator was randomized.
In the presence of the patients, the envelopes (containing only the acronyms MG or CMG)
were released to be assigned to the respective categories.
At first researchers performed a telephone trial of structured questions about the
validity of the PD diagnosis, the time of diagnosis, available medications, existing
treatment programs through rehabilitation, mobility for walking and daily living tasks,
personal background and physiotherapy desires. The patients tested were assessed in order to
determine whether they met the criteria for participation. The study included patients
diagnosed with idiopathic PD according to the guidelines of the London Brain Bank, graded
in stages 1.5 to 3 over 50yrs adjusted and independent for walking were also considered. The
test procedures were carried out not by physiotherapists participating in the research
(treatment) and accountable for each intervention. An independent blind investigator, skilled
in Parkinson's disease, conducted the assessments. Additionally, professionally trained
physiotherapists conducted the operation.
Outcome and Intervention
The first day included demographic information: age, body weight, height, body
mass, education, testing times, the daily dose alternative of Levodopa; cognitive analysis by
using the Mini mental-state tests for measuring overall cognitive function; seriousness of
affected with Parkinson’s syndrome some were allocated to intervention and the count stood
58. These candidates were randomized for the clinical trials (Santos et al., 2017).
Randomization and followed by Blinding
An independent researcher had a basic randomisation to conduct Persons with PD
randomized by blind randomization by means of a random number generator,
utilizing similar, opaque, sealed envelopes, and identified into "Motor Group (MG)" or
"Cognitive Motor Group (CMG)." In the case of PD, the number generator was randomized.
In the presence of the patients, the envelopes (containing only the acronyms MG or CMG)
were released to be assigned to the respective categories.
At first researchers performed a telephone trial of structured questions about the
validity of the PD diagnosis, the time of diagnosis, available medications, existing
treatment programs through rehabilitation, mobility for walking and daily living tasks,
personal background and physiotherapy desires. The patients tested were assessed in order to
determine whether they met the criteria for participation. The study included patients
diagnosed with idiopathic PD according to the guidelines of the London Brain Bank, graded
in stages 1.5 to 3 over 50yrs adjusted and independent for walking were also considered. The
test procedures were carried out not by physiotherapists participating in the research
(treatment) and accountable for each intervention. An independent blind investigator, skilled
in Parkinson's disease, conducted the assessments. Additionally, professionally trained
physiotherapists conducted the operation.
Outcome and Intervention
The first day included demographic information: age, body weight, height, body
mass, education, testing times, the daily dose alternative of Levodopa; cognitive analysis by
using the Mini mental-state tests for measuring overall cognitive function; seriousness of
5PARKINSON’S DISEASE
disease using the Unified Parkinson Rating Scale and the Revised Hoehn and Yahr S.
Disorder evaluations were conducted (Karssemeijer et al., 2017). The second day saw the
following tests: Montreal cognitive test for general cognitive performance, Semantic Verbal
Fluid testing for memory, knowledge retrieval and impulse control, Rey Auditory Verbal
Learning Test (RAVLT), Cognitive and Percetual examination for sensory and visuospacious
functions; Trail making test for immediate and lateness of memory (Folstein, Folstein, &
McHugh., 1975). The following evaluations were conducted in particular for answering the
quality of life assessment delivery to the patient.
The Physiotherapeutic Treatment plan, which comprises of 32 interventions (4 mos)
which have taken place twice a week, began after the training of groups and the assessment
procedures. The motor group (MG) was treated for 60 minutes, while the cognitive motor
group (CMG) was treated for about 90 minutes (60 minutes of idle and 30 minutes of
cognitive training). A physiotherapist who has expertise in physiotherapy for Parkinson's
disease established the protocols. While this physical therapist was responsible for the
session, for each patient another specialist was assigned, thus it was in the ratio of one
therapist for each patient. While it was a group therapy, a certified physiotherapist supervised
each patient individually.
Statistical Analysis
Explanatory data, examined using the Shapiro-Wilk test, were presented as standard
or medians and interquartile ranges in accordance with normality distribution. Comparison of
the demographics of the individual has been analyzed for continuous variables and for the sex
variable by using the t test for separate samples or the Mann-Whitney U test, in accordance
with the normality of the data. The Wilcoxon test was used in comparing pre-intervention and
post-intervention Montreal Cognitive Assessment and Geriatric Depression Scale data.
disease using the Unified Parkinson Rating Scale and the Revised Hoehn and Yahr S.
Disorder evaluations were conducted (Karssemeijer et al., 2017). The second day saw the
following tests: Montreal cognitive test for general cognitive performance, Semantic Verbal
Fluid testing for memory, knowledge retrieval and impulse control, Rey Auditory Verbal
Learning Test (RAVLT), Cognitive and Percetual examination for sensory and visuospacious
functions; Trail making test for immediate and lateness of memory (Folstein, Folstein, &
McHugh., 1975). The following evaluations were conducted in particular for answering the
quality of life assessment delivery to the patient.
The Physiotherapeutic Treatment plan, which comprises of 32 interventions (4 mos)
which have taken place twice a week, began after the training of groups and the assessment
procedures. The motor group (MG) was treated for 60 minutes, while the cognitive motor
group (CMG) was treated for about 90 minutes (60 minutes of idle and 30 minutes of
cognitive training). A physiotherapist who has expertise in physiotherapy for Parkinson's
disease established the protocols. While this physical therapist was responsible for the
session, for each patient another specialist was assigned, thus it was in the ratio of one
therapist for each patient. While it was a group therapy, a certified physiotherapist supervised
each patient individually.
Statistical Analysis
Explanatory data, examined using the Shapiro-Wilk test, were presented as standard
or medians and interquartile ranges in accordance with normality distribution. Comparison of
the demographics of the individual has been analyzed for continuous variables and for the sex
variable by using the t test for separate samples or the Mann-Whitney U test, in accordance
with the normality of the data. The Wilcoxon test was used in comparing pre-intervention and
post-intervention Montreal Cognitive Assessment and Geriatric Depression Scale data.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6PARKINSON’S DISEASE
Result
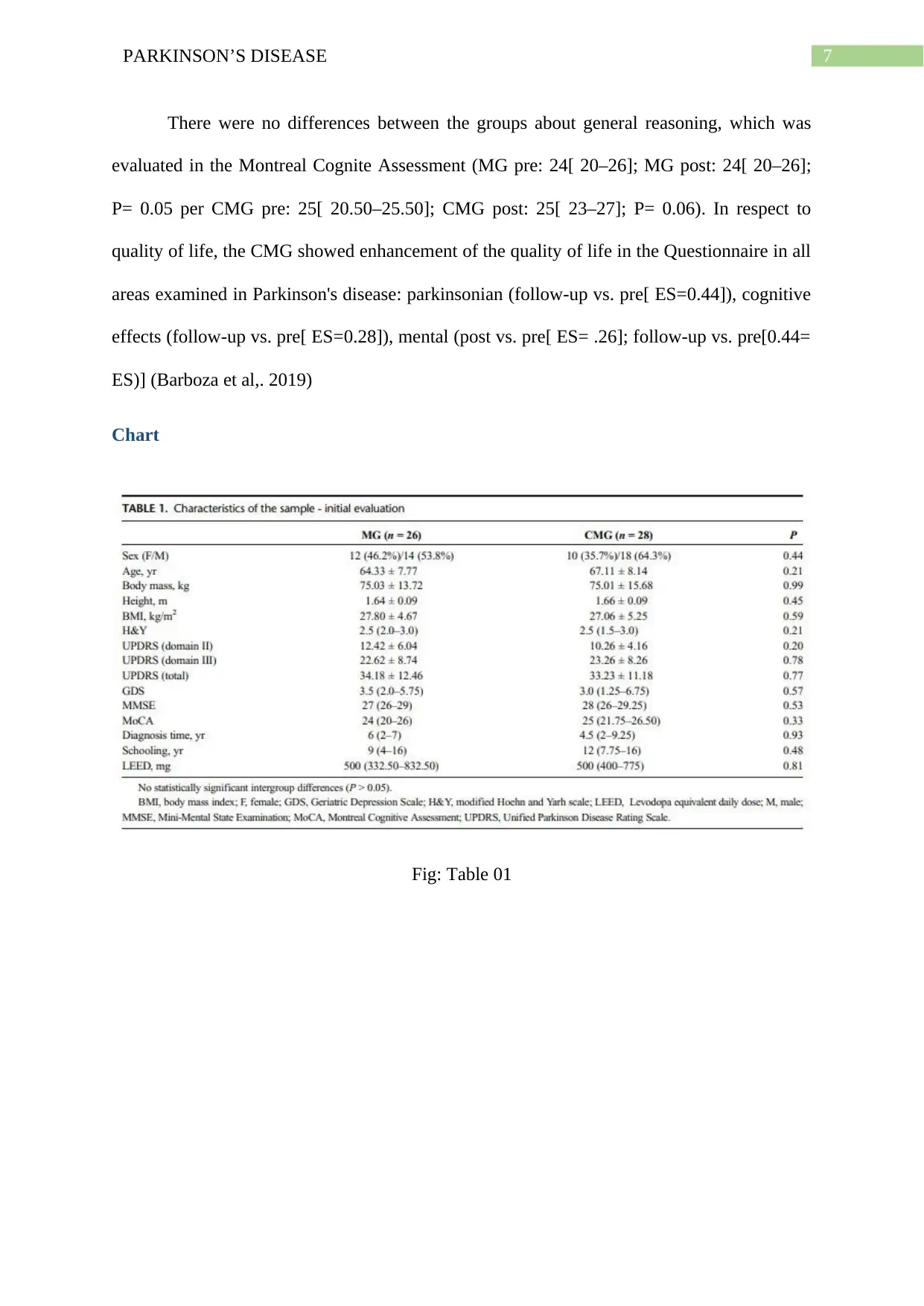
Table 1 displays the main characteristics of the grades. Mean and daily
deviance or inter-quartile distribution as per the normality of the data is expressed. At the
outset of the analysis, all participants were homogeneous with respect to age, gender, height,
body mass index, H and Y scale, Unified Rating Scale, GDS Scale, Montreal Cognitive
Assessment ratings, years of diagnosis, school years and levodopa related daily dose
variables (Barboza et al,. 2019).
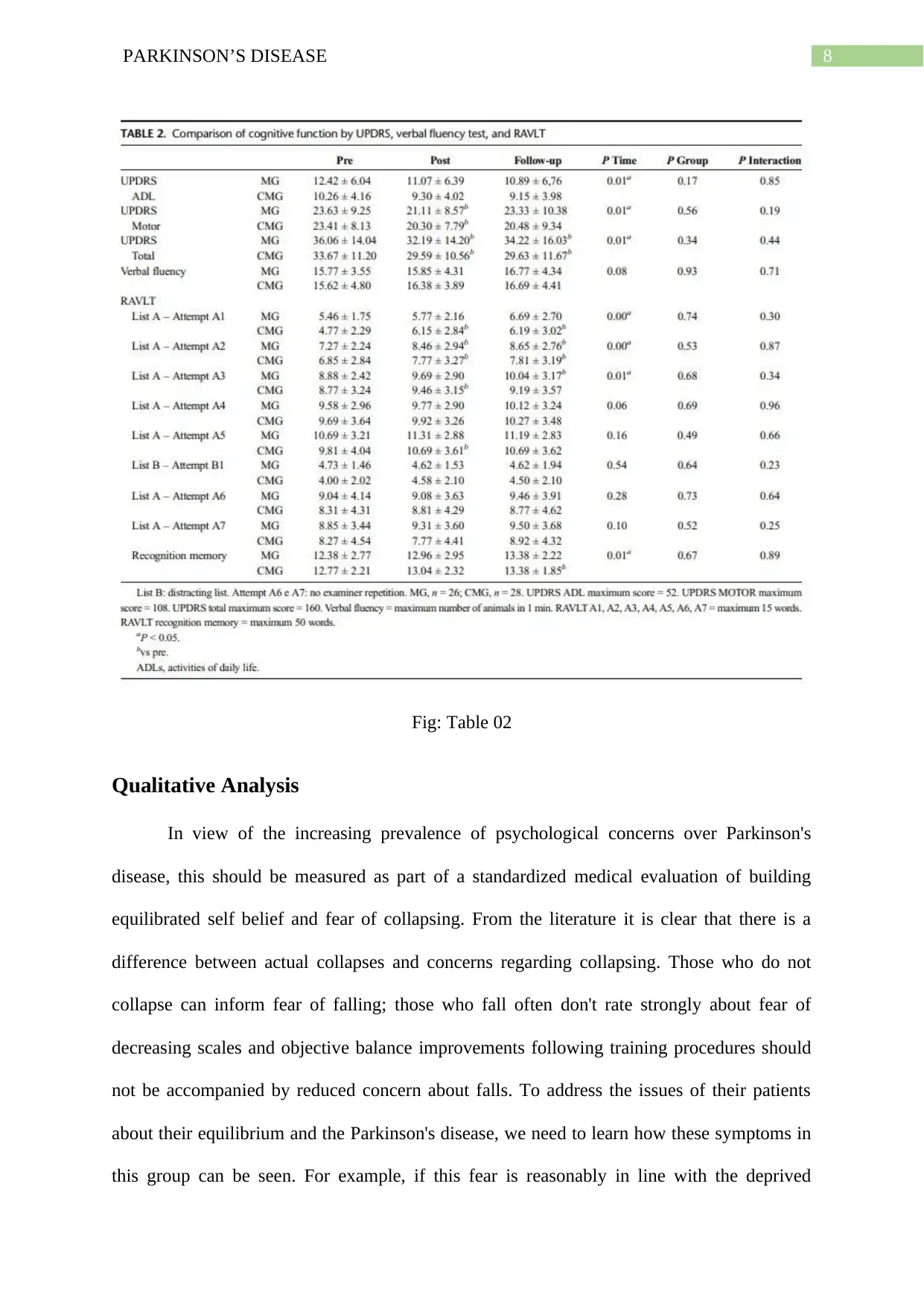
In Table 2 the comparable qualities (daily life behavior, motor function and overall
score) and the cognitive function of verbal and RAVLT measures are shown. In fact, the
qualities are shown in Column 2. Our results show that the engine region and total score of
the Unified Parkinson Disease Rating Scale has changed from pretreatment to non-treatment
with a time-effect. The score for pre- and post- and cumulative measures was statistically
significant. The MG and the CMG groups were found to be improving only when taking the
time effects (post intervention versus pre-intervention and follow-up versus pre) in phases
A1, A2, and A3 and the recognition memory (number of hits). The model was statistically
significant with regard to time for those subgroups, medium to large ESs (ESs ranged from
0.32 to 0.62), but intergroup and time interactive differences between groups were not present
(Barboza et al,. 2019).
Table 3 shows coefficients of contrast between the category and community in visual
measures, clock drawing executive and trail producing trials for cognitive and perceptual
assessment. The improvement of the cognitive-and-perceptual assessment was observed only
with the picture tests of the intragroup comparisons (figure 1: follow-up versus previous (ES=
0.39), follow-up versus post (ES= 0.45), and in CMG (figure 1: follow-up versus pre[ ES=
0.15]; Fig. 2: post versus pre (ES))). (fig. 1: follow-up versus pre (ES= 0.15)). There were no
variations between intergroups and time x groups (Barboza et al,. 2019).
Result
Table 1 displays the main characteristics of the grades. Mean and daily
deviance or inter-quartile distribution as per the normality of the data is expressed. At the
outset of the analysis, all participants were homogeneous with respect to age, gender, height,
body mass index, H and Y scale, Unified Rating Scale, GDS Scale, Montreal Cognitive
Assessment ratings, years of diagnosis, school years and levodopa related daily dose
variables (Barboza et al,. 2019).
In Table 2 the comparable qualities (daily life behavior, motor function and overall
score) and the cognitive function of verbal and RAVLT measures are shown. In fact, the
qualities are shown in Column 2. Our results show that the engine region and total score of
the Unified Parkinson Disease Rating Scale has changed from pretreatment to non-treatment
with a time-effect. The score for pre- and post- and cumulative measures was statistically
significant. The MG and the CMG groups were found to be improving only when taking the
time effects (post intervention versus pre-intervention and follow-up versus pre) in phases
A1, A2, and A3 and the recognition memory (number of hits). The model was statistically
significant with regard to time for those subgroups, medium to large ESs (ESs ranged from
0.32 to 0.62), but intergroup and time interactive differences between groups were not present
(Barboza et al,. 2019).
Table 3 shows coefficients of contrast between the category and community in visual
measures, clock drawing executive and trail producing trials for cognitive and perceptual
assessment. The improvement of the cognitive-and-perceptual assessment was observed only
with the picture tests of the intragroup comparisons (figure 1: follow-up versus previous (ES=
0.39), follow-up versus post (ES= 0.45), and in CMG (figure 1: follow-up versus pre[ ES=
0.15]; Fig. 2: post versus pre (ES))). (fig. 1: follow-up versus pre (ES= 0.15)). There were no
variations between intergroups and time x groups (Barboza et al,. 2019).
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7PARKINSON’S DISEASE
There were no differences between the groups about general reasoning, which was
evaluated in the Montreal Cognite Assessment (MG pre: 24[ 20–26]; MG post: 24[ 20–26];
P= 0.05 per CMG pre: 25[ 20.50–25.50]; CMG post: 25[ 23–27]; P= 0.06). In respect to
quality of life, the CMG showed enhancement of the quality of life in the Questionnaire in all
areas examined in Parkinson's disease: parkinsonian (follow-up vs. pre[ ES=0.44]), cognitive
effects (follow-up vs. pre[ ES=0.28]), mental (post vs. pre[ ES= .26]; follow-up vs. pre[0.44=
ES)] (Barboza et al,. 2019)
Chart
Fig: Table 01
There were no differences between the groups about general reasoning, which was
evaluated in the Montreal Cognite Assessment (MG pre: 24[ 20–26]; MG post: 24[ 20–26];
P= 0.05 per CMG pre: 25[ 20.50–25.50]; CMG post: 25[ 23–27]; P= 0.06). In respect to
quality of life, the CMG showed enhancement of the quality of life in the Questionnaire in all
areas examined in Parkinson's disease: parkinsonian (follow-up vs. pre[ ES=0.44]), cognitive
effects (follow-up vs. pre[ ES=0.28]), mental (post vs. pre[ ES= .26]; follow-up vs. pre[0.44=
ES)] (Barboza et al,. 2019)
Chart
Fig: Table 01
8PARKINSON’S DISEASE
Fig: Table 02
Qualitative Analysis
In view of the increasing prevalence of psychological concerns over Parkinson's
disease, this should be measured as part of a standardized medical evaluation of building
equilibrated self belief and fear of collapsing. From the literature it is clear that there is a
difference between actual collapses and concerns regarding collapsing. Those who do not
collapse can inform fear of falling; those who fall often don't rate strongly about fear of
decreasing scales and objective balance improvements following training procedures should
not be accompanied by reduced concern about falls. To address the issues of their patients
about their equilibrium and the Parkinson's disease, we need to learn how these symptoms in
this group can be seen. For example, if this fear is reasonably in line with the deprived
Fig: Table 02
Qualitative Analysis
In view of the increasing prevalence of psychological concerns over Parkinson's
disease, this should be measured as part of a standardized medical evaluation of building
equilibrated self belief and fear of collapsing. From the literature it is clear that there is a
difference between actual collapses and concerns regarding collapsing. Those who do not
collapse can inform fear of falling; those who fall often don't rate strongly about fear of
decreasing scales and objective balance improvements following training procedures should
not be accompanied by reduced concern about falls. To address the issues of their patients
about their equilibrium and the Parkinson's disease, we need to learn how these symptoms in
this group can be seen. For example, if this fear is reasonably in line with the deprived
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9PARKINSON’S DISEASE
balance and is thus used to decrease the risk of a person, it may not always be an appropriate
rehabilitation goal to decrease the fear of detoriation.
Observational research is a powerful way to understand people's experiences in depth. A
greater understanding into the equilibrium and decline of individuals with Parkinson's disease
will better inform the successful evaluation and treatment of the psychiatric issues that come
in this category. The collection of appropriate fall-related findings for future studies in this
population may also be provided with such information. Surprisingly there is a scarcity of
research in observational studies exploring balance and expectations of deterioration in
people with Parkinson's disease. Although the experiences of equilibrium and decline in
generally older people are more commonly studied, it is doubtful that these findings are
transferable to those with Parkinson's disease because not only of illness-specific movement
symptoms such as gastrip impairment but also because they are at risk for neuropsychiatric
indications such as anxiety and depression. This research was therefore directed at
researching and explaining experiences of balance and came within 3 to 12 months of taking
part in the controlled equilibrium training program for people with mild to severe Parkinson's
disease.
Evidience Based study on Perceptions of balance and falls following a supervised
training intervention – a qualitative study of people with Parkinson’s disease
Breiffni Leavy, Johan Berntsson, Erika Franzén & Kirsti Skavborg Roaldson
DataCollection
Information from 3 to 12 months after interest in a guided balance system was
obtained between October and December 2013. The founder, has extensive experience in
quality research and has no prior participation in the evaluation or preparation of subjects.
Specific semi-structured interviews were conducted. An interview guide (supplementary
balance and is thus used to decrease the risk of a person, it may not always be an appropriate
rehabilitation goal to decrease the fear of detoriation.
Observational research is a powerful way to understand people's experiences in depth. A
greater understanding into the equilibrium and decline of individuals with Parkinson's disease
will better inform the successful evaluation and treatment of the psychiatric issues that come
in this category. The collection of appropriate fall-related findings for future studies in this
population may also be provided with such information. Surprisingly there is a scarcity of
research in observational studies exploring balance and expectations of deterioration in
people with Parkinson's disease. Although the experiences of equilibrium and decline in
generally older people are more commonly studied, it is doubtful that these findings are
transferable to those with Parkinson's disease because not only of illness-specific movement
symptoms such as gastrip impairment but also because they are at risk for neuropsychiatric
indications such as anxiety and depression. This research was therefore directed at
researching and explaining experiences of balance and came within 3 to 12 months of taking
part in the controlled equilibrium training program for people with mild to severe Parkinson's
disease.
Evidience Based study on Perceptions of balance and falls following a supervised
training intervention – a qualitative study of people with Parkinson’s disease
Breiffni Leavy, Johan Berntsson, Erika Franzén & Kirsti Skavborg Roaldson
DataCollection
Information from 3 to 12 months after interest in a guided balance system was
obtained between October and December 2013. The founder, has extensive experience in
quality research and has no prior participation in the evaluation or preparation of subjects.
Specific semi-structured interviews were conducted. An interview guide (supplementary
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10PARKINSON’S DISEASE
material) led the interviews. It was organized with the following open end questions in
keeping with predefined themes. The interviews lasted 70 to 95 minutes, were documented
and transcribed simply on the digital voice recorder (Olympus WS-550 M). Throughout
different phases of interviews, the researcher orally outlined her understanding of the
perceptions of the subjects throughout order for them to clarify misinterpretations.
Transcripts of the discussion were analyzed using a replicable and accurate method to
analyze the text using qualitative content analysis. An inductive method requiring systemic
comprehension of the document contributed to the research process, first at realized and then
latent stages, involving text interpretation in greater abstraction (Conradsson et al., 2015).
Meaning units were defined and organized in all interviews to determine the part of the text
that highlights the research purpose. The units of interest were then condensed, abstracted
and labeled with an initial name.
The different codes were compared and categorized in sub-themes, which were then
individually grouped into the major themes. The writer holds the key codes of all interviews
were modified and optimized constantly during a sequence of briefing sessions covering all
the participants in order to ensure the truthfulness of the study.
Result
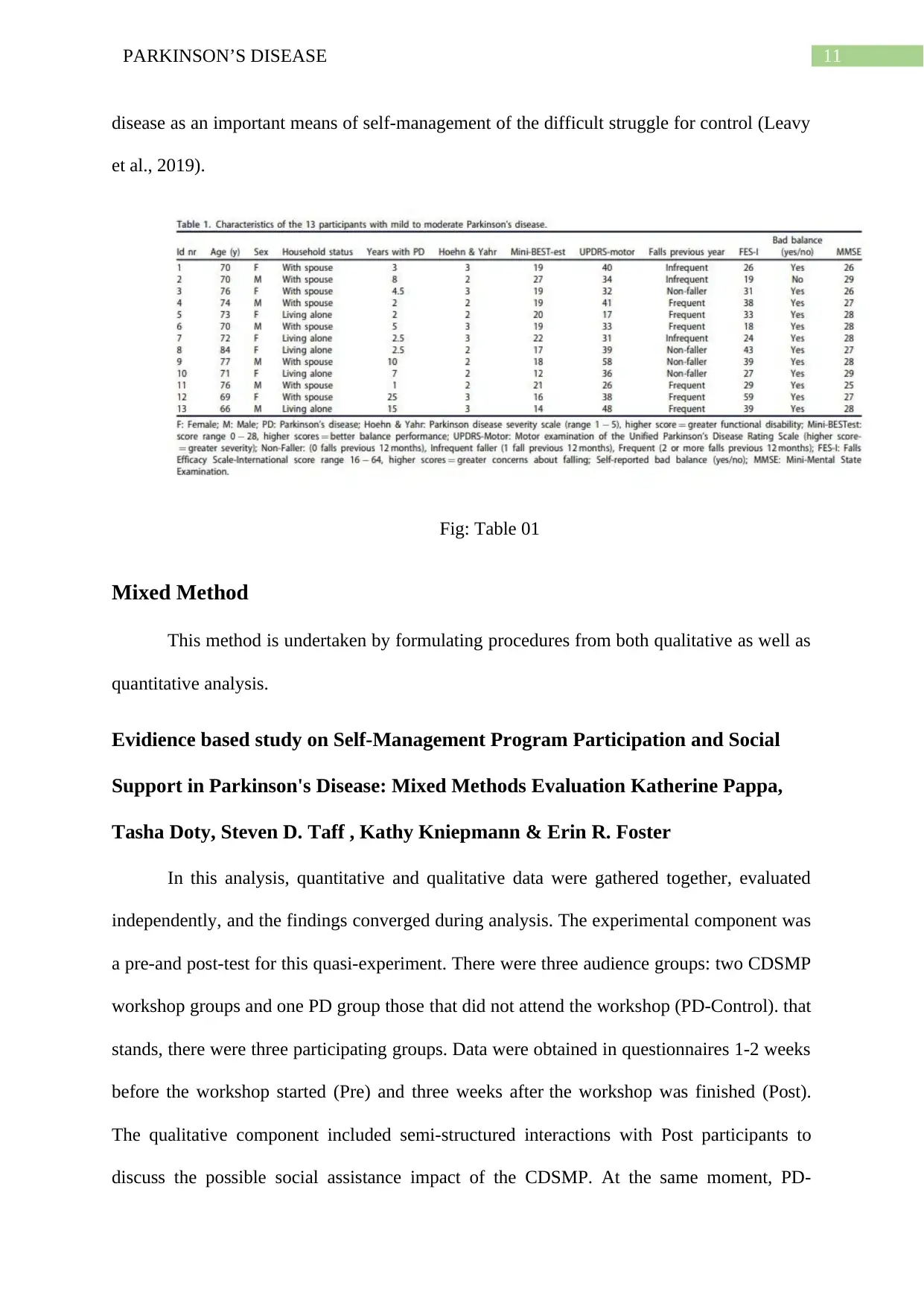
Table 1 details the characteristics of the participants. Age mean was 72.9 (SD 4.6)
years; the mean diagnostic time was 6.7 years (SD 6.7); balance capacity ranged from 14 to
27 points. The resulting balance capacity ranges between 14 and 27 points. Four citizens
felled in the intervening year, three never fell, and six dropped two or more times.
Eight sub-themes were developed through qualitative content analysis, containing
three major topics and an underlying subject. The main subject integrates key issues with
subthemes and explores how rehabilitation became viewed through people with Parkinson's
material) led the interviews. It was organized with the following open end questions in
keeping with predefined themes. The interviews lasted 70 to 95 minutes, were documented
and transcribed simply on the digital voice recorder (Olympus WS-550 M). Throughout
different phases of interviews, the researcher orally outlined her understanding of the
perceptions of the subjects throughout order for them to clarify misinterpretations.
Transcripts of the discussion were analyzed using a replicable and accurate method to
analyze the text using qualitative content analysis. An inductive method requiring systemic
comprehension of the document contributed to the research process, first at realized and then
latent stages, involving text interpretation in greater abstraction (Conradsson et al., 2015).
Meaning units were defined and organized in all interviews to determine the part of the text
that highlights the research purpose. The units of interest were then condensed, abstracted
and labeled with an initial name.
The different codes were compared and categorized in sub-themes, which were then
individually grouped into the major themes. The writer holds the key codes of all interviews
were modified and optimized constantly during a sequence of briefing sessions covering all
the participants in order to ensure the truthfulness of the study.
Result
Table 1 details the characteristics of the participants. Age mean was 72.9 (SD 4.6)
years; the mean diagnostic time was 6.7 years (SD 6.7); balance capacity ranged from 14 to
27 points. The resulting balance capacity ranges between 14 and 27 points. Four citizens
felled in the intervening year, three never fell, and six dropped two or more times.
Eight sub-themes were developed through qualitative content analysis, containing
three major topics and an underlying subject. The main subject integrates key issues with
subthemes and explores how rehabilitation became viewed through people with Parkinson's
11PARKINSON’S DISEASE
disease as an important means of self-management of the difficult struggle for control (Leavy
et al., 2019).
Fig: Table 01
Mixed Method
This method is undertaken by formulating procedures from both qualitative as well as
quantitative analysis.
Evidience based study on Self-Management Program Participation and Social
Support in Parkinson's Disease: Mixed Methods Evaluation Katherine Pappa,
Tasha Doty, Steven D. Taff , Kathy Kniepmann & Erin R. Foster
In this analysis, quantitative and qualitative data were gathered together, evaluated
independently, and the findings converged during analysis. The experimental component was
a pre-and post-test for this quasi-experiment. There were three audience groups: two CDSMP
workshop groups and one PD group those that did not attend the workshop (PD-Control). that
stands, there were three participating groups. Data were obtained in questionnaires 1-2 weeks
before the workshop started (Pre) and three weeks after the workshop was finished (Post).
The qualitative component included semi-structured interactions with Post participants to
discuss the possible social assistance impact of the CDSMP. At the same moment, PD-
disease as an important means of self-management of the difficult struggle for control (Leavy
et al., 2019).
Fig: Table 01
Mixed Method
This method is undertaken by formulating procedures from both qualitative as well as
quantitative analysis.
Evidience based study on Self-Management Program Participation and Social
Support in Parkinson's Disease: Mixed Methods Evaluation Katherine Pappa,
Tasha Doty, Steven D. Taff , Kathy Kniepmann & Erin R. Foster
In this analysis, quantitative and qualitative data were gathered together, evaluated
independently, and the findings converged during analysis. The experimental component was
a pre-and post-test for this quasi-experiment. There were three audience groups: two CDSMP
workshop groups and one PD group those that did not attend the workshop (PD-Control). that
stands, there were three participating groups. Data were obtained in questionnaires 1-2 weeks
before the workshop started (Pre) and three weeks after the workshop was finished (Post).
The qualitative component included semi-structured interactions with Post participants to
discuss the possible social assistance impact of the CDSMP. At the same moment, PD-
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 22
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.