2804NRS: Pathophysiology and Pharmacology Case Study Report Analysis
VerifiedAdded on 2023/01/18
|8
|1996
|68
Report
AI Summary
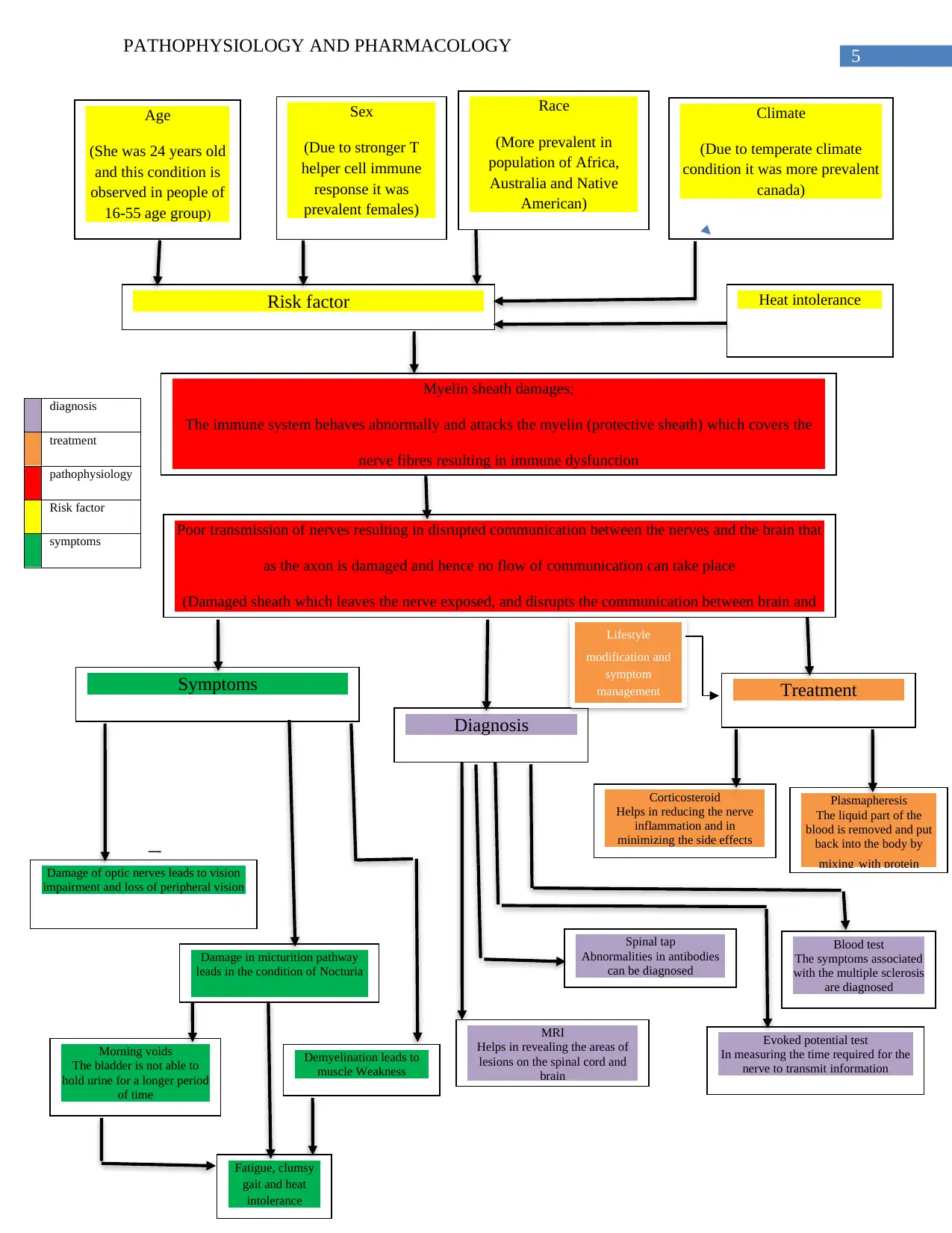
This report provides a detailed analysis of a multiple sclerosis (MS) case study involving a 24-year-old woman named Penny Hofsatder. The report begins by identifying Penny's risk factors, including age, sex, race, climate, smoking habits, and caffeine consumption, linking them to the development of MS. It then delves into the pathophysiology of MS, explaining the demyelination process and its impact on the central nervous system, leading to various clinical manifestations such as vision impairment, muscle weakness, and heat intolerance. The report further discusses the diagnostic examinations used to confirm MS, including blood tests, lumbar punctures, MRI, and evoked potential tests. Finally, it outlines the treatment modalities, including corticosteroids, plasmapheresis, and lifestyle modifications. The document references several scholarly articles to support the analysis.


1 out of 8
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.