NURS8741 Patient Assessment: Case Study of a Critically Ill Patient
VerifiedAdded on 2022/09/16
|9
|2373
|22
Case Study
AI Summary
This case study presents a comprehensive assessment of a 68-year-old male patient admitted to the intensive care unit with septicemia secondary to a pressure sore infection. The assessment follows the ISBAR format, detailing the patient's condition, including airway, breathing, circulation, disability, and environment. System abnormalities identified include respiratory and integumentary issues, with the patient at risk of further deterioration. Interventions such as oxygen administration, systemic antibiotics, and wound care are prioritized. The assessment aligns with ACCCN practice standards, particularly in collaboration, critical thinking, and provision of care, with specific examples from the assessment process and findings. The study emphasizes the importance of critical care nurses' role in patient management, including respiratory, cardiovascular, and neurological assessments. The case study includes detailed information on interventions and the application of theoretical knowledge to clinical practice, reflecting on learning experiences and promoting improved patient outcomes. The case study also includes the patient's medical history and the nursing care provided, including medication and nutrition, to provide a holistic view of the patient's condition and care.

Nursing
Student name
Institution
Student name
Institution
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1. Patient case
The case study is a hypothetical case study of Mr X, who is a 68-year-old male who was brought
to the intensive care department on Monday 8:00 am. The patient was diagnosed with septicemia
secondary to pressure sore infection. The patient was connected to a cardiorespiratory monitor.
D = DANGER
All equipment to manage the patient was present and in good working condition, which included
a cardiorespiratory monitor. The patient is at risk of further infection.
R = RESPONSE
Mr X is a 68-year-old male who was brought to the intensive care department on Monday 8:00
am in a confused state.
A = AIRWAY
The airway was clear and open
No artificial airway
B = BREATHING
Shortness of breath and fast breathing
Use of accessory muscles and chest in drawing
Respiratory Rate of 34 breaths per minute
The patient was put on non-invasive ventilation parameters to the cardiopulmonary ventilator
SP02 of 82%
C = CIRCULATION
Central and peripheral pulses present skin clammy and sweaty
Capillary refill at 3 seconds
The heart rate of 120 bpm and irregular in rhythm
D = DISABILITY
Pupils equal in size and not dilated and reactive to light
The case study is a hypothetical case study of Mr X, who is a 68-year-old male who was brought
to the intensive care department on Monday 8:00 am. The patient was diagnosed with septicemia
secondary to pressure sore infection. The patient was connected to a cardiorespiratory monitor.
D = DANGER
All equipment to manage the patient was present and in good working condition, which included
a cardiorespiratory monitor. The patient is at risk of further infection.
R = RESPONSE
Mr X is a 68-year-old male who was brought to the intensive care department on Monday 8:00
am in a confused state.
A = AIRWAY
The airway was clear and open
No artificial airway
B = BREATHING
Shortness of breath and fast breathing
Use of accessory muscles and chest in drawing
Respiratory Rate of 34 breaths per minute
The patient was put on non-invasive ventilation parameters to the cardiopulmonary ventilator
SP02 of 82%
C = CIRCULATION
Central and peripheral pulses present skin clammy and sweaty
Capillary refill at 3 seconds
The heart rate of 120 bpm and irregular in rhythm
D = DISABILITY
Pupils equal in size and not dilated and reactive to light
On normal saline infusion via an intravenous line 500 mls
GCS of 12
The patient has a urinary catheter to drain urine and intravenous infusion line
Glucose
E = ENVIRONMENT & EXCRETION (Both internal - fluids and electrolyte and external
- clear surroundings related to danger)
A third-degree pressure sore on the right sacral area
Urine through a urinary catheter
Full blood count results within 14 days show an increase in sodium and hydrogen levels in the
blood.
The skin has red patches all over the body. Temperature 38.4 degrees Celsius
F = FULL SET OF VITAL SIGNS & FLUIDS
Fluids normal saline 500 mls
Was accompanied by his daughter to the hospital
Urine output of 150 mls within the last hour
Temperature 38.4 degrees Celsius, heart rate 120bpm, blood pressure 128/82 mmHg and RR 34
breaths per minute
This includes presenting problems, drugs and diagnostic tests, equipment and technological
devices and allergies. A full safety check of the patient and the patient environment
especially at the beginning of patient care is routine. Then a thorough head to toe, system
by system assessment process is performed including psychosocial assessment.
Airway and
Breathing
The patient was connected to a cardiorespiratory monitor with a supply of
oxygen 10 litres. On inspection, there was the use of accessory muscles
with the chest in drawing while breathing. There were no scars or bruises
on the chest area. On auscultation of the lungs, there was bilateral air entry
GCS of 12
The patient has a urinary catheter to drain urine and intravenous infusion line
Glucose
E = ENVIRONMENT & EXCRETION (Both internal - fluids and electrolyte and external
- clear surroundings related to danger)
A third-degree pressure sore on the right sacral area
Urine through a urinary catheter
Full blood count results within 14 days show an increase in sodium and hydrogen levels in the
blood.
The skin has red patches all over the body. Temperature 38.4 degrees Celsius
F = FULL SET OF VITAL SIGNS & FLUIDS
Fluids normal saline 500 mls
Was accompanied by his daughter to the hospital
Urine output of 150 mls within the last hour
Temperature 38.4 degrees Celsius, heart rate 120bpm, blood pressure 128/82 mmHg and RR 34
breaths per minute
This includes presenting problems, drugs and diagnostic tests, equipment and technological
devices and allergies. A full safety check of the patient and the patient environment
especially at the beginning of patient care is routine. Then a thorough head to toe, system
by system assessment process is performed including psychosocial assessment.
Airway and
Breathing
The patient was connected to a cardiorespiratory monitor with a supply of
oxygen 10 litres. On inspection, there was the use of accessory muscles
with the chest in drawing while breathing. There were no scars or bruises
on the chest area. On auscultation of the lungs, there was bilateral air entry
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
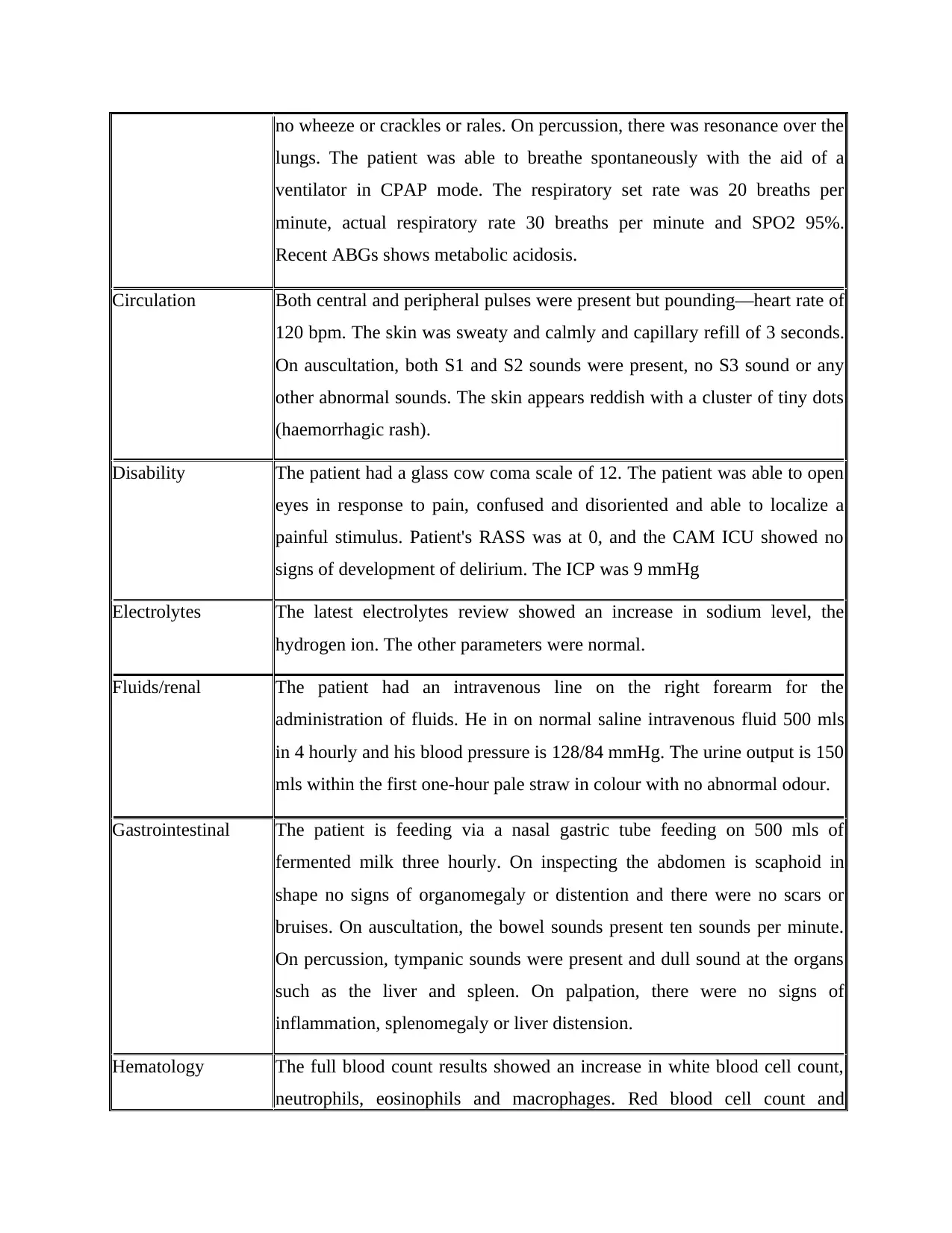
no wheeze or crackles or rales. On percussion, there was resonance over the
lungs. The patient was able to breathe spontaneously with the aid of a
ventilator in CPAP mode. The respiratory set rate was 20 breaths per
minute, actual respiratory rate 30 breaths per minute and SPO2 95%.
Recent ABGs shows metabolic acidosis.
Circulation Both central and peripheral pulses were present but pounding—heart rate of
120 bpm. The skin was sweaty and calmly and capillary refill of 3 seconds.
On auscultation, both S1 and S2 sounds were present, no S3 sound or any
other abnormal sounds. The skin appears reddish with a cluster of tiny dots
(haemorrhagic rash).
Disability The patient had a glass cow coma scale of 12. The patient was able to open
eyes in response to pain, confused and disoriented and able to localize a
painful stimulus. Patient's RASS was at 0, and the CAM ICU showed no
signs of development of delirium. The ICP was 9 mmHg
Electrolytes The latest electrolytes review showed an increase in sodium level, the
hydrogen ion. The other parameters were normal.
Fluids/renal The patient had an intravenous line on the right forearm for the
administration of fluids. He in on normal saline intravenous fluid 500 mls
in 4 hourly and his blood pressure is 128/84 mmHg. The urine output is 150
mls within the first one-hour pale straw in colour with no abnormal odour.
Gastrointestinal The patient is feeding via a nasal gastric tube feeding on 500 mls of
fermented milk three hourly. On inspecting the abdomen is scaphoid in
shape no signs of organomegaly or distention and there were no scars or
bruises. On auscultation, the bowel sounds present ten sounds per minute.
On percussion, tympanic sounds were present and dull sound at the organs
such as the liver and spleen. On palpation, there were no signs of
inflammation, splenomegaly or liver distension.
Hematology The full blood count results showed an increase in white blood cell count,
neutrophils, eosinophils and macrophages. Red blood cell count and
lungs. The patient was able to breathe spontaneously with the aid of a
ventilator in CPAP mode. The respiratory set rate was 20 breaths per
minute, actual respiratory rate 30 breaths per minute and SPO2 95%.
Recent ABGs shows metabolic acidosis.
Circulation Both central and peripheral pulses were present but pounding—heart rate of
120 bpm. The skin was sweaty and calmly and capillary refill of 3 seconds.
On auscultation, both S1 and S2 sounds were present, no S3 sound or any
other abnormal sounds. The skin appears reddish with a cluster of tiny dots
(haemorrhagic rash).
Disability The patient had a glass cow coma scale of 12. The patient was able to open
eyes in response to pain, confused and disoriented and able to localize a
painful stimulus. Patient's RASS was at 0, and the CAM ICU showed no
signs of development of delirium. The ICP was 9 mmHg
Electrolytes The latest electrolytes review showed an increase in sodium level, the
hydrogen ion. The other parameters were normal.
Fluids/renal The patient had an intravenous line on the right forearm for the
administration of fluids. He in on normal saline intravenous fluid 500 mls
in 4 hourly and his blood pressure is 128/84 mmHg. The urine output is 150
mls within the first one-hour pale straw in colour with no abnormal odour.
Gastrointestinal The patient is feeding via a nasal gastric tube feeding on 500 mls of
fermented milk three hourly. On inspecting the abdomen is scaphoid in
shape no signs of organomegaly or distention and there were no scars or
bruises. On auscultation, the bowel sounds present ten sounds per minute.
On percussion, tympanic sounds were present and dull sound at the organs
such as the liver and spleen. On palpation, there were no signs of
inflammation, splenomegaly or liver distension.
Hematology The full blood count results showed an increase in white blood cell count,
neutrophils, eosinophils and macrophages. Red blood cell count and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
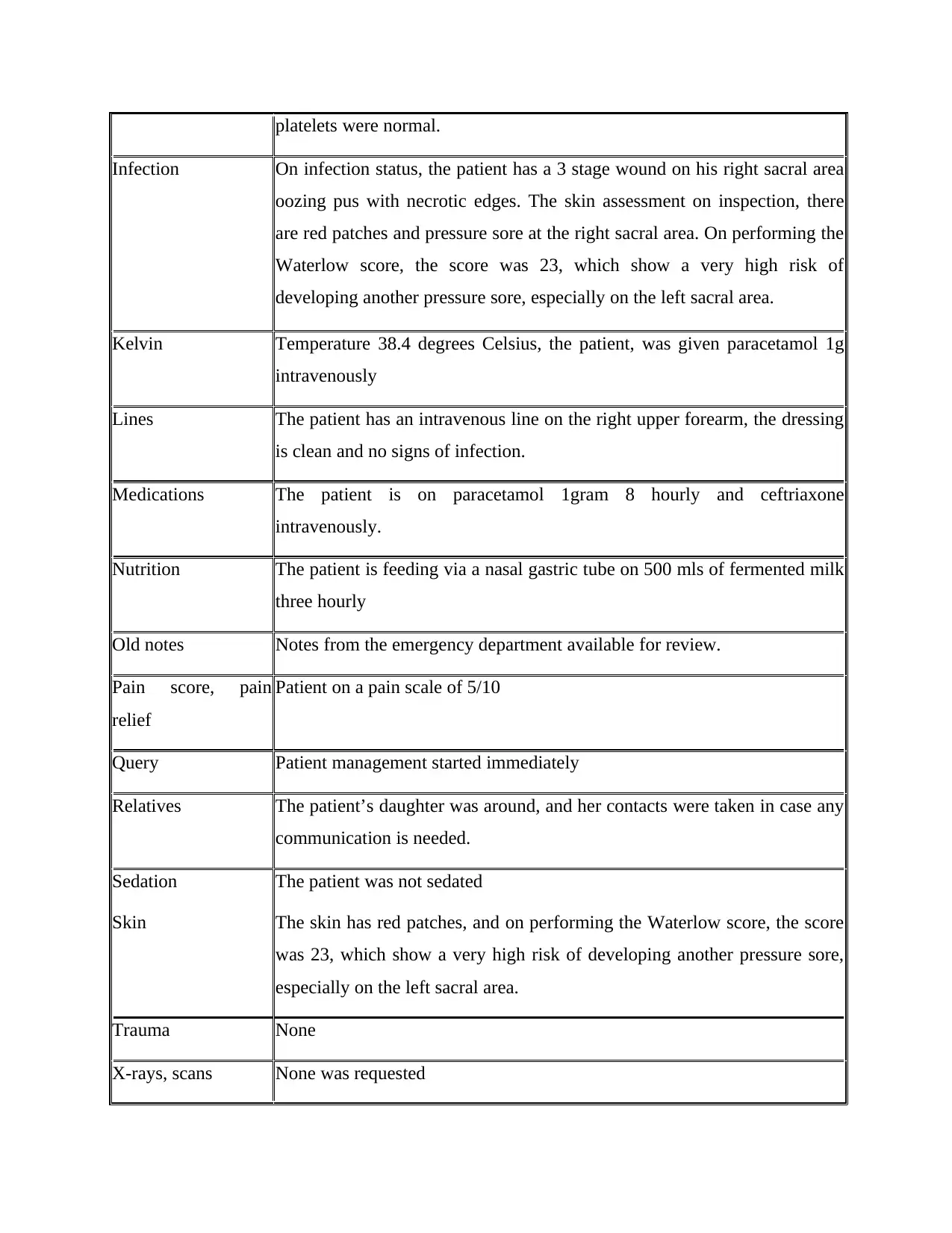
platelets were normal.
Infection On infection status, the patient has a 3 stage wound on his right sacral area
oozing pus with necrotic edges. The skin assessment on inspection, there
are red patches and pressure sore at the right sacral area. On performing the
Waterlow score, the score was 23, which show a very high risk of
developing another pressure sore, especially on the left sacral area.
Kelvin Temperature 38.4 degrees Celsius, the patient, was given paracetamol 1g
intravenously
Lines The patient has an intravenous line on the right upper forearm, the dressing
is clean and no signs of infection.
Medications The patient is on paracetamol 1gram 8 hourly and ceftriaxone
intravenously.
Nutrition The patient is feeding via a nasal gastric tube on 500 mls of fermented milk
three hourly
Old notes Notes from the emergency department available for review.
Pain score, pain
relief
Patient on a pain scale of 5/10
Query Patient management started immediately
Relatives The patient’s daughter was around, and her contacts were taken in case any
communication is needed.
Sedation
Skin
The patient was not sedated
The skin has red patches, and on performing the Waterlow score, the score
was 23, which show a very high risk of developing another pressure sore,
especially on the left sacral area.
Trauma None
X-rays, scans None was requested
Infection On infection status, the patient has a 3 stage wound on his right sacral area
oozing pus with necrotic edges. The skin assessment on inspection, there
are red patches and pressure sore at the right sacral area. On performing the
Waterlow score, the score was 23, which show a very high risk of
developing another pressure sore, especially on the left sacral area.
Kelvin Temperature 38.4 degrees Celsius, the patient, was given paracetamol 1g
intravenously
Lines The patient has an intravenous line on the right upper forearm, the dressing
is clean and no signs of infection.
Medications The patient is on paracetamol 1gram 8 hourly and ceftriaxone
intravenously.
Nutrition The patient is feeding via a nasal gastric tube on 500 mls of fermented milk
three hourly
Old notes Notes from the emergency department available for review.
Pain score, pain
relief
Patient on a pain scale of 5/10
Query Patient management started immediately
Relatives The patient’s daughter was around, and her contacts were taken in case any
communication is needed.
Sedation
Skin
The patient was not sedated
The skin has red patches, and on performing the Waterlow score, the score
was 23, which show a very high risk of developing another pressure sore,
especially on the left sacral area.
Trauma None
X-rays, scans None was requested
Zzzz: sleep The patient is still unconscious
2. Assessment state of the patient
From the patient's assessment, the patient is at risk of damage of vital organs such as the brain,
the kidney and the lungs. Tissue gangrene can also result, which can lead to amputation,
especially the right leg. It can even lead to septic shock or even death of the patient. From the
assessment, the patient has an integumentary system abnormalities and respiratory system
abnormalities. This is because the skin, which is the first defence mechanism against infection, is
already compromised. Therefore, there is an increased risk in infection and infections can easily
access the bloodstream due to the chronic pressure sore causing more complications. The patient
cannot breathe, and this affects the oxygen supply to the body tissues.
3. Interventions
The first intervention is the administration of oxygen to the patient to increase oxygen supply to
the lungs (Bell et al. 2017). Increase in oxygen supply to the blood and eventually to the body
tissue facilitates the elimination of accumulated carbon IV oxide in the tissues and blood.
Therefore an impulse is sent to the respiratory system to normalize the respiratory Rate and
avoid laboured breathing
The second intervention is the administration of systemic antibiotics to manage sepsis. Some of
the antibiotics include ceftriaxone, vancomycin, azithromycin and tazobactam. Most of these
drugs are broad-spectrum antibiotics and able to act on a wide range of bacterial microorganisms
as sepsis is commonly due to bacterial infection. Topical antibiotics can also be used at the site
of the pressure sore such as dermazine (Lewis et al. 2018).
Another intervention is cleaning the wound aseptically, using aseptic technique with normal
saline, metronidazole or any other solution depending on the state of the wound. The appropriate
dressing should be used preferred are dressing coated with an antibacterial or antiseptic agent
such as hydrocolloid dressings.
4. Assignment 2a Integument Assessment - Collaboration and Leadership Domain,
Standards 13 to 15
2. Assessment state of the patient
From the patient's assessment, the patient is at risk of damage of vital organs such as the brain,
the kidney and the lungs. Tissue gangrene can also result, which can lead to amputation,
especially the right leg. It can even lead to septic shock or even death of the patient. From the
assessment, the patient has an integumentary system abnormalities and respiratory system
abnormalities. This is because the skin, which is the first defence mechanism against infection, is
already compromised. Therefore, there is an increased risk in infection and infections can easily
access the bloodstream due to the chronic pressure sore causing more complications. The patient
cannot breathe, and this affects the oxygen supply to the body tissues.
3. Interventions
The first intervention is the administration of oxygen to the patient to increase oxygen supply to
the lungs (Bell et al. 2017). Increase in oxygen supply to the blood and eventually to the body
tissue facilitates the elimination of accumulated carbon IV oxide in the tissues and blood.
Therefore an impulse is sent to the respiratory system to normalize the respiratory Rate and
avoid laboured breathing
The second intervention is the administration of systemic antibiotics to manage sepsis. Some of
the antibiotics include ceftriaxone, vancomycin, azithromycin and tazobactam. Most of these
drugs are broad-spectrum antibiotics and able to act on a wide range of bacterial microorganisms
as sepsis is commonly due to bacterial infection. Topical antibiotics can also be used at the site
of the pressure sore such as dermazine (Lewis et al. 2018).
Another intervention is cleaning the wound aseptically, using aseptic technique with normal
saline, metronidazole or any other solution depending on the state of the wound. The appropriate
dressing should be used preferred are dressing coated with an antibacterial or antiseptic agent
such as hydrocolloid dressings.
4. Assignment 2a Integument Assessment - Collaboration and Leadership Domain,
Standards 13 to 15
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
The domain states that critical care team should collaborate with each other in order to achieve
the desired outcome. This can be achieved by learning from each other and appreciation other
team member's skills. Experienced nurses should give guidance to novice nurses and also
appreciate the experience of their superiors. The nurse can demonstrate to the novice nurses how
to clean the pressure sore aseptically or management of the patient to prevent the development of
pressure sore. Identifying learning needs and being a leader to identify how to solve it is also
important (Aitken et al. 2016).
Assignment 2b Cardiovascular Assessment- Critical Thinking and Analysis Domain, Standards
9 to 12
The critical care nurse has to apply critical thinking when faced with a problem or when the
patient changes condition either anticipated or not (Price, 2015). The nurse should, therefore,
continue monitoring the patient for vital signs to trace their progress. The heart rate should be
monitored for any changes and improvement and act accordingly. If the patient develops
tachycardia or bradycardia, appropriate action should be taken as fast as possible to avoid losing
the patient. Fluid overload should also be monitored and anticipated for especially when the
patient is on intravenous fluids all through.
Assignment 2c Fluid and Electrolyte Assessment - Provision and Coordination of Care Domain,
Standards 5 to 8
The nurse should provide holistic care to the patient. This involves not only taking care of the
patient's physical needs but also, social, psychological, physiological and spiritual needs. It also
involved taking care of family needs. Every patient has all the needs; therefore, appropriate
intervention and involvement of other professionals such as spiritual partner are important. The
family members and the patient should be educated on the patient’s condition, management and
even the expected outcome. The nurse should monitor the input and output of the patient, intake
ability and any abnormalities in output. Changes in electrolytes such as increased sodium or
hydrogen levels in the blood should be assessed, and appropriate intervention put into action.
The nurse should, therefore, take care of the patient as a whole.
Assignment 2d Respiratory & Airway Assessment - Critical Thinking and Analysis Domain,
Standards 9 to 12
the desired outcome. This can be achieved by learning from each other and appreciation other
team member's skills. Experienced nurses should give guidance to novice nurses and also
appreciate the experience of their superiors. The nurse can demonstrate to the novice nurses how
to clean the pressure sore aseptically or management of the patient to prevent the development of
pressure sore. Identifying learning needs and being a leader to identify how to solve it is also
important (Aitken et al. 2016).
Assignment 2b Cardiovascular Assessment- Critical Thinking and Analysis Domain, Standards
9 to 12
The critical care nurse has to apply critical thinking when faced with a problem or when the
patient changes condition either anticipated or not (Price, 2015). The nurse should, therefore,
continue monitoring the patient for vital signs to trace their progress. The heart rate should be
monitored for any changes and improvement and act accordingly. If the patient develops
tachycardia or bradycardia, appropriate action should be taken as fast as possible to avoid losing
the patient. Fluid overload should also be monitored and anticipated for especially when the
patient is on intravenous fluids all through.
Assignment 2c Fluid and Electrolyte Assessment - Provision and Coordination of Care Domain,
Standards 5 to 8
The nurse should provide holistic care to the patient. This involves not only taking care of the
patient's physical needs but also, social, psychological, physiological and spiritual needs. It also
involved taking care of family needs. Every patient has all the needs; therefore, appropriate
intervention and involvement of other professionals such as spiritual partner are important. The
family members and the patient should be educated on the patient’s condition, management and
even the expected outcome. The nurse should monitor the input and output of the patient, intake
ability and any abnormalities in output. Changes in electrolytes such as increased sodium or
hydrogen levels in the blood should be assessed, and appropriate intervention put into action.
The nurse should, therefore, take care of the patient as a whole.
Assignment 2d Respiratory & Airway Assessment - Critical Thinking and Analysis Domain,
Standards 9 to 12
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Airway and respiratory system is the first part of the patient to be assessed (Considine, & Currey,
2015). Any impairment in the respiratory system should be intervened first before carrying out
any other assessment. Oxygen was administered to the patient immediately signs of shortness of
breath and fas breathing were identified. Monitoring from the ventilator is also essential to detect
any change and decide on what to be done. The patient can develop respiratory alkalosis if too
much oxygen is delivered for an extended period of time. The nurse should also critically think
on the exact moment to change the ventilator settings or discontinue help the patient gain
independence.
Assignment 2e Neurological Assessment- Professional Practice Domain, Standards 1
The nurse was able to apply the standard one of ACCCN which starts that the nurse should
functions within the legal parameters of critical care nursing even when the patient has cognitive
disabilities or impairments, Mr X was brought in a confused state of mind, and therefore the
patient was not able to decide on their own health. The nurse, however, decided on what was best
for the patient and what would benefit the patient more. This is, therefore, acting according to
professional ethics in not causing harm but benefits to the patient.
5. Reflection of clinical practice and learning
From the assessment, I have learned how to prioritize patients' needs based on the primary
assessment. The interventions that should come first and at what moment are also identified. This
assessment is also a direct application to the clinical practice and the advanced knowledge gained
will be used in the clinical practice to take care of the patients for better outcomes.
2015). Any impairment in the respiratory system should be intervened first before carrying out
any other assessment. Oxygen was administered to the patient immediately signs of shortness of
breath and fas breathing were identified. Monitoring from the ventilator is also essential to detect
any change and decide on what to be done. The patient can develop respiratory alkalosis if too
much oxygen is delivered for an extended period of time. The nurse should also critically think
on the exact moment to change the ventilator settings or discontinue help the patient gain
independence.
Assignment 2e Neurological Assessment- Professional Practice Domain, Standards 1
The nurse was able to apply the standard one of ACCCN which starts that the nurse should
functions within the legal parameters of critical care nursing even when the patient has cognitive
disabilities or impairments, Mr X was brought in a confused state of mind, and therefore the
patient was not able to decide on their own health. The nurse, however, decided on what was best
for the patient and what would benefit the patient more. This is, therefore, acting according to
professional ethics in not causing harm but benefits to the patient.
5. Reflection of clinical practice and learning
From the assessment, I have learned how to prioritize patients' needs based on the primary
assessment. The interventions that should come first and at what moment are also identified. This
assessment is also a direct application to the clinical practice and the advanced knowledge gained
will be used in the clinical practice to take care of the patients for better outcomes.
References
Aitken, L., Marshall, A., & Chaboyer, W. (2016). ACCCN's Critical Care Nursing. Elsevier
Health Sciences.
Bell, E. C., Cox, N. S., Goh, N., Glaspole, I., Westall, G. P., Watson, A., & Holland, A. E.
(2017). Oxygen therapy for interstitial lung disease: a systematic review. European
Respiratory Review, 26(143), 160080.
Considine, J., & Currey, J. (2015). Ensuring a proactive, evidence‐based, patient safety approach
to patient assessment. Journal of Clinical Nursing, 24(1-2), 300-307.
Lewis, A. J., Griepentrog, J. E., Zhang, X., Angus, D. C., Seymour, C. W., & Rosengart, M. R.
(2018). Prompt administration of antibiotics and fluids in the treatment of sepsis: a
murine trial. Critical care medicine, 46(5), e426.
Price, B. (2015). Applying critical thinking to nursing. Nursing Standard (2014+), 29(51), 49.
Aitken, L., Marshall, A., & Chaboyer, W. (2016). ACCCN's Critical Care Nursing. Elsevier
Health Sciences.
Bell, E. C., Cox, N. S., Goh, N., Glaspole, I., Westall, G. P., Watson, A., & Holland, A. E.
(2017). Oxygen therapy for interstitial lung disease: a systematic review. European
Respiratory Review, 26(143), 160080.
Considine, J., & Currey, J. (2015). Ensuring a proactive, evidence‐based, patient safety approach
to patient assessment. Journal of Clinical Nursing, 24(1-2), 300-307.
Lewis, A. J., Griepentrog, J. E., Zhang, X., Angus, D. C., Seymour, C. W., & Rosengart, M. R.
(2018). Prompt administration of antibiotics and fluids in the treatment of sepsis: a
murine trial. Critical care medicine, 46(5), e426.
Price, B. (2015). Applying critical thinking to nursing. Nursing Standard (2014+), 29(51), 49.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.