Analysis of Patient Falls in a Rehabilitation Department Report
VerifiedAdded on 2021/05/31
|10
|2783
|77
Report
AI Summary
This report presents an analysis of patient falls in a hospital rehabilitation department, examining the causes, circumstances, and contributing factors of these incidents. The study, conducted over five years, reviewed 80 fall incidents among patients, particularly stroke victims, with a focus on identifying risk factors and suggesting preventive strategies. The analysis highlights the importance of considering patient conditions, behaviors, and environmental factors in fall prevention. The study also emphasizes the need for multifactorial fall risk assessments, building safety awareness among clinical teams, and implementing routine diligence to reduce fall incidents. The report recommends continuous quality improvement (CQI) and the use of various interventions like secure wheelchairs, bedside rails, and patient education to minimize the risk of falls and associated injuries. It concludes that while fall avoidance initiatives are important, attention to modifiable risk factors and the proper use of devices are crucial in preventing falls in hospitals.

People fall accidentally in
Hospital
Hospital
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Background..................................................................................................................................................2
Case:............................................................................................................................................................3
Analysis:.......................................................................................................................................................3
Discussion and Recommendation................................................................................................................5
Conclusion...................................................................................................................................................7
References:..................................................................................................................................................8
Background..................................................................................................................................................2
Case:............................................................................................................................................................3
Analysis:.......................................................................................................................................................3
Discussion and Recommendation................................................................................................................5
Conclusion...................................................................................................................................................7
References:..................................................................................................................................................8
Background
Causes in the rehabilitation department are typical and provide both the falling individual and the
health care community with serious problems. Falls can cause discomfort, damage to the soft
tissue, fracture of the bone or brain. Participation of recovery programmes, which may create a
dangerous environment, regularly promotes versatility. Thereby, it appears urgent for those who
are vulnerable to frequent drops to find means of preventing dropping. High-risk patients are an
essential part of preventive programmes, and risk factors have also been investigated to a certain
degree in various patient groups. The cumulative influence of several risk factors will be more
significant than the possible effects of each factor alone. Cases can induce more movement
restrictions and can have a detrimental effect on physiotherapy (Fernando et al., 2017)..
Several cognitive and physical deficits also arise in people with stroke cortical lesions, or other
brain disorders that are completing recovery and are at high risk of declines. In the case of stroke
victims admitted for recovery, confusion, unsafe gait and wheelchair containment were major
risk factors. Fallers also have signs of deprivation and dyspraxia in the visuo-space that may lead
to their dysfunction. In 32 patients admitted in a rehabilitative centre, 40 cases have been
reported. The sensory motor and cognitive disorder induced "intrinsic falls" resulted in 35% of
cases, and the environmental causes caused extrinsic falls, in 12.5% of cases. 'Extrinsic causes'
may be slipping from a position in a wheelchair or some other form of furniture (Guirguis-Blake
et sl., 2018).
Cases are frequent cases in the hospitals and are a significant recovery health issue. A specific
situation in the recovery department is that entry is directed at preserving function and freedom.
An estimation of the fall probability will help to plan the extent of functional autonomy.
Identified that crashes after recovery of the stroke may have led to a prolonged hospital stay.
The purpose of the present research was to find, and analysis features of patients fallen during
their recovery: the condition, disability and the time, location and circumstances of their dropout,
and the causes contributing to the patient in the rehabilitation department. Patient decline is one
of the quality criteria for patient treatment. During hospitalisation, it is an avoidable adverse
occurrence. In addition to the provision of acute physical wounds, long-standing physical injuries
and psychiatric conditions, the healing of injured elderly patients includes additional medical and
nursing services. Almost 4,000 cases of fall injuries during hospitalisation have been registered
in Hong Kong (Naseri et al., 2018). A new reduction prevention approach at the ward level is
needed to strengthen existing procedures and decrease hospital drop with ageing population and
predictable escalation statistics (Moncada et al., 2017).
Causes in the rehabilitation department are typical and provide both the falling individual and the
health care community with serious problems. Falls can cause discomfort, damage to the soft
tissue, fracture of the bone or brain. Participation of recovery programmes, which may create a
dangerous environment, regularly promotes versatility. Thereby, it appears urgent for those who
are vulnerable to frequent drops to find means of preventing dropping. High-risk patients are an
essential part of preventive programmes, and risk factors have also been investigated to a certain
degree in various patient groups. The cumulative influence of several risk factors will be more
significant than the possible effects of each factor alone. Cases can induce more movement
restrictions and can have a detrimental effect on physiotherapy (Fernando et al., 2017)..
Several cognitive and physical deficits also arise in people with stroke cortical lesions, or other
brain disorders that are completing recovery and are at high risk of declines. In the case of stroke
victims admitted for recovery, confusion, unsafe gait and wheelchair containment were major
risk factors. Fallers also have signs of deprivation and dyspraxia in the visuo-space that may lead
to their dysfunction. In 32 patients admitted in a rehabilitative centre, 40 cases have been
reported. The sensory motor and cognitive disorder induced "intrinsic falls" resulted in 35% of
cases, and the environmental causes caused extrinsic falls, in 12.5% of cases. 'Extrinsic causes'
may be slipping from a position in a wheelchair or some other form of furniture (Guirguis-Blake
et sl., 2018).
Cases are frequent cases in the hospitals and are a significant recovery health issue. A specific
situation in the recovery department is that entry is directed at preserving function and freedom.
An estimation of the fall probability will help to plan the extent of functional autonomy.
Identified that crashes after recovery of the stroke may have led to a prolonged hospital stay.
The purpose of the present research was to find, and analysis features of patients fallen during
their recovery: the condition, disability and the time, location and circumstances of their dropout,
and the causes contributing to the patient in the rehabilitation department. Patient decline is one
of the quality criteria for patient treatment. During hospitalisation, it is an avoidable adverse
occurrence. In addition to the provision of acute physical wounds, long-standing physical injuries
and psychiatric conditions, the healing of injured elderly patients includes additional medical and
nursing services. Almost 4,000 cases of fall injuries during hospitalisation have been registered
in Hong Kong (Naseri et al., 2018). A new reduction prevention approach at the ward level is
needed to strengthen existing procedures and decrease hospital drop with ageing population and
predictable escalation statistics (Moncada et al., 2017).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Case:
The study took place at a recovery hospital in a tertiary care facility with 24 beds. Following the
admission to Rehabilitation Department, the patients mentioned in this retrospect analysis
suffered a fall-accident. Between 2008 and 2012, the survey was conducted over five years.
After the acute period, all patients need additional recovery and hospitalisation. After choosing
from intensive care units, the patients were usually admitted several days to two weeks after
onset or after surgery. From induction to Recovery before discharge, they were recorded, and
medical histories included accurate information on the medical history of patients (Dai et al.,
2018).
All the studied patients recovered from brain injury, developmental deficiency spinal defects,
low limb amputation and lower limb injuries in our 24-bedded rehabilitation department. 80 falls
have been reported during the study period in 55 patients (38 men and 17 women). The average
age was 62.9+9.7 years for the patients. In Category 1 (called "participants") were 41 patients
who were once rejected (average age 63.2+10.4), and in Gruppe 2 (average age 62.3+7.9).
(average age 62.3+7.9) Of the 55 patients suffering from spinal, brain, or cerebellar lesions, 31
were admitted from the vascular root and 2 were admitted following cerebral tumour rejection.
(Bluetongue) (Bluetongue). Nine patients had orthopaedic surgery, eight patients had lower limb
amputation, and 5 patients had spinal disabilities of paraparesis. Fifty-eight out of 80 cases
(72.5%) affected cortical patients. Nobody was removed from the report on fall cases (Montero‐
Odasso et al., 2018).
Analysis:
An event was described as an occurrence recorded in a case study, in which unregulated
unintentional behaviour resulted in the body's movement to a knee level or below. The nursing
team shall record all incidents in the hospital in compliance with the hospital protocol. The
nursing staff checked all injury records and retrieved the following details. We contrasted the
safety risk evaluation carried out by the fall nurses Each fall in the department was routinely
reported in a standardised way by the nurses and asked where, how, and why the patient was
down. Questions regarding the time, location and circumstances of the fall and any injury or
other fall effects offered valuable detail. Various details analysed included: the disease or
condition that patients were treated for; the hour of the fall; the presence of disease or prior
accident that may have caused the fall; The action that caused the fall; when the Fall happened in
the hospital, if any damage caused by the fall. Health steps have been taken for the whole
population of patients as a departmental procedure to avoid crashes. Brakes were applied to both
The study took place at a recovery hospital in a tertiary care facility with 24 beds. Following the
admission to Rehabilitation Department, the patients mentioned in this retrospect analysis
suffered a fall-accident. Between 2008 and 2012, the survey was conducted over five years.
After the acute period, all patients need additional recovery and hospitalisation. After choosing
from intensive care units, the patients were usually admitted several days to two weeks after
onset or after surgery. From induction to Recovery before discharge, they were recorded, and
medical histories included accurate information on the medical history of patients (Dai et al.,
2018).
All the studied patients recovered from brain injury, developmental deficiency spinal defects,
low limb amputation and lower limb injuries in our 24-bedded rehabilitation department. 80 falls
have been reported during the study period in 55 patients (38 men and 17 women). The average
age was 62.9+9.7 years for the patients. In Category 1 (called "participants") were 41 patients
who were once rejected (average age 63.2+10.4), and in Gruppe 2 (average age 62.3+7.9).
(average age 62.3+7.9) Of the 55 patients suffering from spinal, brain, or cerebellar lesions, 31
were admitted from the vascular root and 2 were admitted following cerebral tumour rejection.
(Bluetongue) (Bluetongue). Nine patients had orthopaedic surgery, eight patients had lower limb
amputation, and 5 patients had spinal disabilities of paraparesis. Fifty-eight out of 80 cases
(72.5%) affected cortical patients. Nobody was removed from the report on fall cases (Montero‐
Odasso et al., 2018).
Analysis:
An event was described as an occurrence recorded in a case study, in which unregulated
unintentional behaviour resulted in the body's movement to a knee level or below. The nursing
team shall record all incidents in the hospital in compliance with the hospital protocol. The
nursing staff checked all injury records and retrieved the following details. We contrasted the
safety risk evaluation carried out by the fall nurses Each fall in the department was routinely
reported in a standardised way by the nurses and asked where, how, and why the patient was
down. Questions regarding the time, location and circumstances of the fall and any injury or
other fall effects offered valuable detail. Various details analysed included: the disease or
condition that patients were treated for; the hour of the fall; the presence of disease or prior
accident that may have caused the fall; The action that caused the fall; when the Fall happened in
the hospital, if any damage caused by the fall. Health steps have been taken for the whole
population of patients as a departmental procedure to avoid crashes. Brakes were applied to both
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
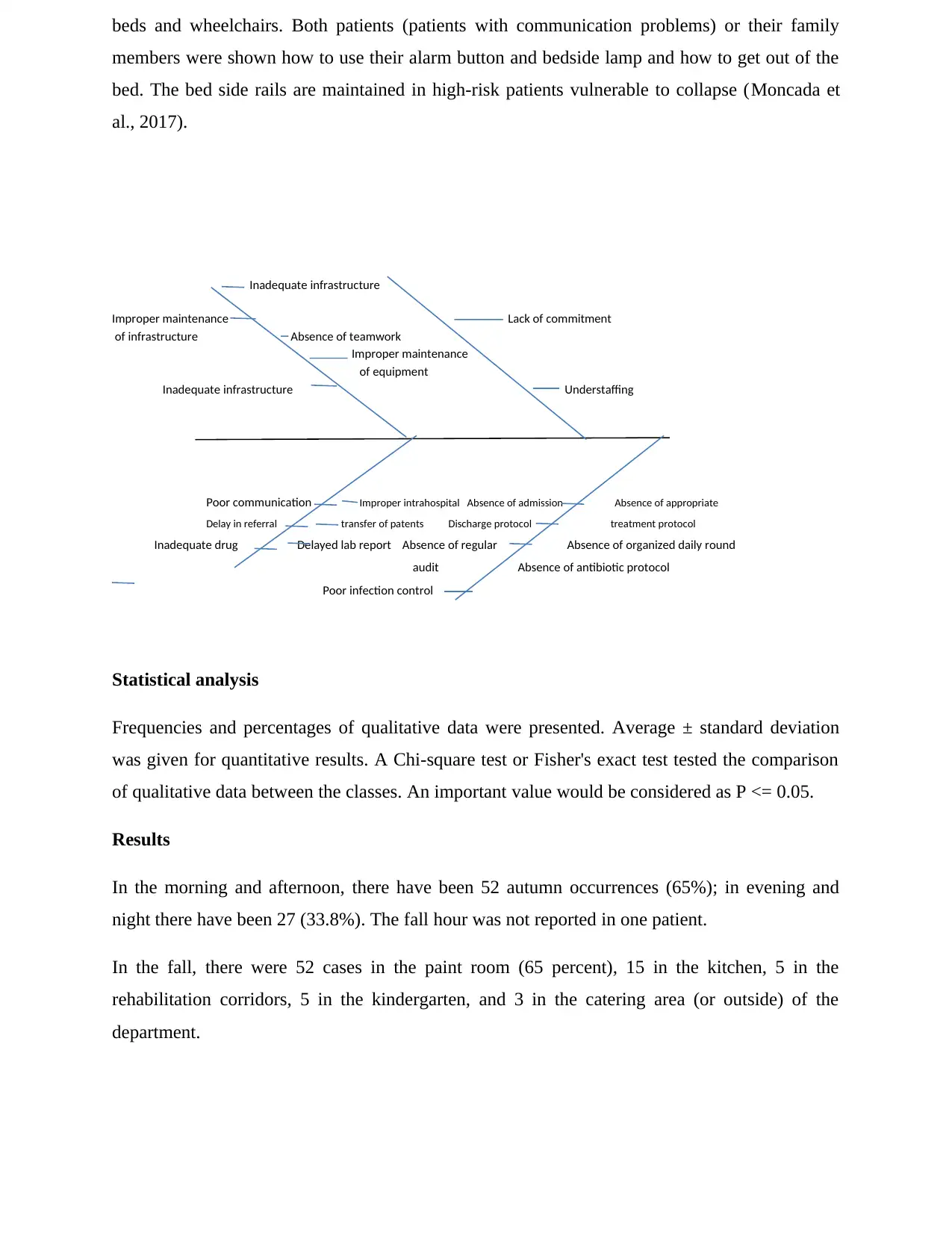
beds and wheelchairs. Both patients (patients with communication problems) or their family
members were shown how to use their alarm button and bedside lamp and how to get out of the
bed. The bed side rails are maintained in high-risk patients vulnerable to collapse (Moncada et
al., 2017).
Inadequate infrastructure
Improper maintenance Lack of commitment
of infrastructure Absence of teamwork
Improper maintenance
of equipment
Inadequate infrastructure Understaffing
Poor communication Improper intrahospital Absence of admission Absence of appropriate
Delay in referral transfer of patents Discharge protocol treatment protocol
Inadequate drug Delayed lab report Absence of regular Absence of organized daily round
audit Absence of antibiotic protocol
Poor infection control
Statistical analysis
Frequencies and percentages of qualitative data were presented. Average ± standard deviation
was given for quantitative results. A Chi-square test or Fisher's exact test tested the comparison
of qualitative data between the classes. An important value would be considered as P <= 0.05.
Results
In the morning and afternoon, there have been 52 autumn occurrences (65%); in evening and
night there have been 27 (33.8%). The fall hour was not reported in one patient.
In the fall, there were 52 cases in the paint room (65 percent), 15 in the kitchen, 5 in the
rehabilitation corridors, 5 in the kindergarten, and 3 in the catering area (or outside) of the
department.
members were shown how to use their alarm button and bedside lamp and how to get out of the
bed. The bed side rails are maintained in high-risk patients vulnerable to collapse (Moncada et
al., 2017).
Inadequate infrastructure
Improper maintenance Lack of commitment
of infrastructure Absence of teamwork
Improper maintenance
of equipment
Inadequate infrastructure Understaffing
Poor communication Improper intrahospital Absence of admission Absence of appropriate
Delay in referral transfer of patents Discharge protocol treatment protocol
Inadequate drug Delayed lab report Absence of regular Absence of organized daily round
audit Absence of antibiotic protocol
Poor infection control
Statistical analysis
Frequencies and percentages of qualitative data were presented. Average ± standard deviation
was given for quantitative results. A Chi-square test or Fisher's exact test tested the comparison
of qualitative data between the classes. An important value would be considered as P <= 0.05.
Results
In the morning and afternoon, there have been 52 autumn occurrences (65%); in evening and
night there have been 27 (33.8%). The fall hour was not reported in one patient.
In the fall, there were 52 cases in the paint room (65 percent), 15 in the kitchen, 5 in the
rehabilitation corridors, 5 in the kindergarten, and 3 in the catering area (or outside) of the
department.
During transfers, the peak frequencies of 44 drops (55 percent), 16 drops from slipping, 5 drops
from patients ascending the bed and 3 patients from the floor, causing them to be unknown, were
reported. Another 12 falls happened because of multiple causes, such as an obstacle, leaning,
falling away from wheelchairs, chaps, rising, etc (Sharif et al., 2018).
In the recovery department, there is an association between the number of people falling and the
cause for hospitalization. Group 1 patients have been hospitalized following a temporal, brain
stem or cerebellar lesion, amputated lower limb, broken lower limb or colorectal dysfunction
(Fischer's Exact Test, p=0,003 2-sided) (Chi Square Test, p=0,038 on one side)) Testing of group
1 patients (Chi Square Test). The event usually occurs in Category 1 patients as they were moved
from one venue to another (Table 2). In group 2 patients, the incident often happened as a result
of walking or standing slipping (Chi Square Exam, p=0,005) (Table 3).
Discussion and Recommendation
Hospital declines in recovery settings are a chronic concern. This research indicates that these
falls may be affected by multiple complex patient traits, conditions, and behaviours. Some
patients in hospitals attempt to carry out unassisted activities which account for a large
proportion of dropping conditions.
Therefore, it is recommended to conduct a multifactorial fall risk assessment of all patients
hospitalised and over age of 65 (and those over 54 years judged to be risk-specific). Risk
assessment and proactive steps will reduce the fall to 20-30% as much as possible. The
successful harm reduction schemes include building safety awareness in clinical teams and
implementing routine diligence. However, the National Event Audit showed that many trusts
lose the chance to reduce hospital falls.
In the hospital, prevention is the business of all, from the trust board to the clinical interface of
all staff. The best practices tend to consist of empowering multidisciplinary teams to test and
optimize interventions aimed at minimizing the risk factors that have been identified as relevant
across study management systems that seek to explain the causes of stationary events.
Continuous quality improvement (CQI)/total quality management can improve clinical results,
enrich program effects across management channels. We describe CQI as 'a continuous
mechanism in which senior management takes the necessary steps to enable everyone within the
company to set and meet standards that match or surpass customer's needs and requirements in
the course of all duties. In the case of fall prevention, the purpose of this paper is to test the value
of a quality improvement approach.
from patients ascending the bed and 3 patients from the floor, causing them to be unknown, were
reported. Another 12 falls happened because of multiple causes, such as an obstacle, leaning,
falling away from wheelchairs, chaps, rising, etc (Sharif et al., 2018).
In the recovery department, there is an association between the number of people falling and the
cause for hospitalization. Group 1 patients have been hospitalized following a temporal, brain
stem or cerebellar lesion, amputated lower limb, broken lower limb or colorectal dysfunction
(Fischer's Exact Test, p=0,003 2-sided) (Chi Square Test, p=0,038 on one side)) Testing of group
1 patients (Chi Square Test). The event usually occurs in Category 1 patients as they were moved
from one venue to another (Table 2). In group 2 patients, the incident often happened as a result
of walking or standing slipping (Chi Square Exam, p=0,005) (Table 3).
Discussion and Recommendation
Hospital declines in recovery settings are a chronic concern. This research indicates that these
falls may be affected by multiple complex patient traits, conditions, and behaviours. Some
patients in hospitals attempt to carry out unassisted activities which account for a large
proportion of dropping conditions.
Therefore, it is recommended to conduct a multifactorial fall risk assessment of all patients
hospitalised and over age of 65 (and those over 54 years judged to be risk-specific). Risk
assessment and proactive steps will reduce the fall to 20-30% as much as possible. The
successful harm reduction schemes include building safety awareness in clinical teams and
implementing routine diligence. However, the National Event Audit showed that many trusts
lose the chance to reduce hospital falls.
In the hospital, prevention is the business of all, from the trust board to the clinical interface of
all staff. The best practices tend to consist of empowering multidisciplinary teams to test and
optimize interventions aimed at minimizing the risk factors that have been identified as relevant
across study management systems that seek to explain the causes of stationary events.
Continuous quality improvement (CQI)/total quality management can improve clinical results,
enrich program effects across management channels. We describe CQI as 'a continuous
mechanism in which senior management takes the necessary steps to enable everyone within the
company to set and meet standards that match or surpass customer's needs and requirements in
the course of all duties. In the case of fall prevention, the purpose of this paper is to test the value
of a quality improvement approach.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Cases and accidents associated with fall are a major clinical concern in the older demographic
and several active preventive measures are available. Reduced knowledge of oneself and under-
estimation of the risk for dropping have also been described as a possible cause of risk to the
elderly hospitalising community. As the chance of falls increases with the number of present risk
factors, intervention must consider any potential risk factor and include the entire
multidisciplinary team. For example, instruction for workers on the avoidance of falls and fall
accidents should be given. Our facility has an ongoing fall avoidance programme as common in
other hospitals to avoid fall accidents. Interventions in our recovery departments are considered.
Secure wheelchairs with all the appropriate equipment to avoid patients who are vulnerable to
falling out of the chair or jumping on their feet without examination.
Check the patients' room for bed stoppers, bed side panels, alarm clock and night light.
In the shower, check the alarm bell and the illumination quality.
Use a symbol to warn the wet floor.
Extraction from the patient's space of superfluous furniture.
To teach the patient to use the bathroom/toilet safety rail.
Move patients from bed to wheelchair and back to advise family members.
Identification of patients susceptible to drops to get as close to the nursing station as possible.
Executive functions are cognitive skills that enable people to communicate efficiently and
effectively with their surroundings. Executive function tests provide incremental prediction
information in the recovery system for hospital crashes. It would appear it decreases most often
in people with worse brain functions in patients with similar postural control.
We prescribe that patients at risk for drop be identified and efficient procedures be implemented
to avoid falls and reduce injury due to falling.
and several active preventive measures are available. Reduced knowledge of oneself and under-
estimation of the risk for dropping have also been described as a possible cause of risk to the
elderly hospitalising community. As the chance of falls increases with the number of present risk
factors, intervention must consider any potential risk factor and include the entire
multidisciplinary team. For example, instruction for workers on the avoidance of falls and fall
accidents should be given. Our facility has an ongoing fall avoidance programme as common in
other hospitals to avoid fall accidents. Interventions in our recovery departments are considered.
Secure wheelchairs with all the appropriate equipment to avoid patients who are vulnerable to
falling out of the chair or jumping on their feet without examination.
Check the patients' room for bed stoppers, bed side panels, alarm clock and night light.
In the shower, check the alarm bell and the illumination quality.
Use a symbol to warn the wet floor.
Extraction from the patient's space of superfluous furniture.
To teach the patient to use the bathroom/toilet safety rail.
Move patients from bed to wheelchair and back to advise family members.
Identification of patients susceptible to drops to get as close to the nursing station as possible.
Executive functions are cognitive skills that enable people to communicate efficiently and
effectively with their surroundings. Executive function tests provide incremental prediction
information in the recovery system for hospital crashes. It would appear it decreases most often
in people with worse brain functions in patients with similar postural control.
We prescribe that patients at risk for drop be identified and efficient procedures be implemented
to avoid falls and reduce injury due to falling.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
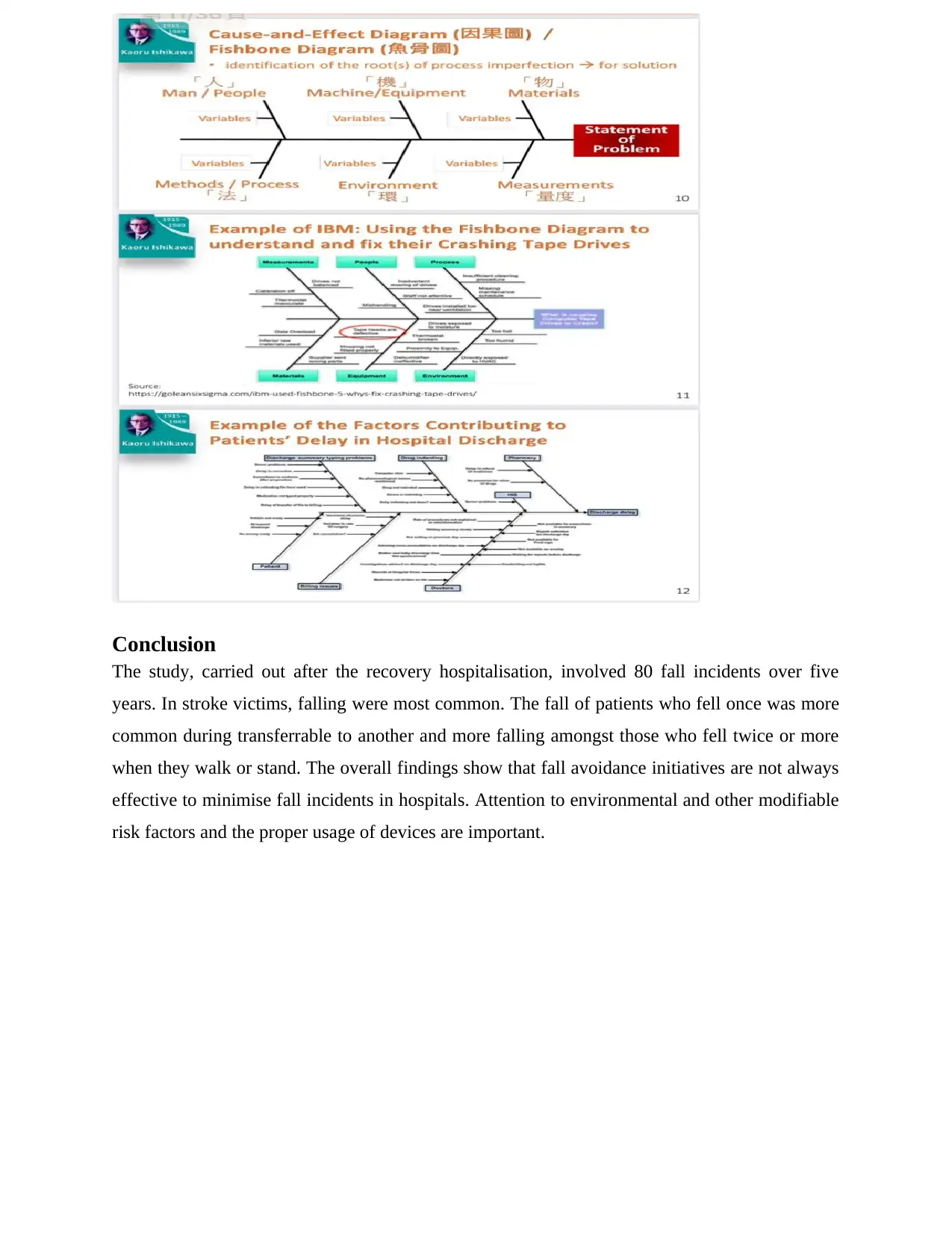
Conclusion
The study, carried out after the recovery hospitalisation, involved 80 fall incidents over five
years. In stroke victims, falling were most common. The fall of patients who fell once was more
common during transferrable to another and more falling amongst those who fell twice or more
when they walk or stand. The overall findings show that fall avoidance initiatives are not always
effective to minimise fall incidents in hospitals. Attention to environmental and other modifiable
risk factors and the proper usage of devices are important.
The study, carried out after the recovery hospitalisation, involved 80 fall incidents over five
years. In stroke victims, falling were most common. The fall of patients who fell once was more
common during transferrable to another and more falling amongst those who fell twice or more
when they walk or stand. The overall findings show that fall avoidance initiatives are not always
effective to minimise fall incidents in hospitals. Attention to environmental and other modifiable
risk factors and the proper usage of devices are important.
References:
Fernando, E., Fraser, M., Hendriksen, J., Kim, C. H., & Muir-Hunter, S. W. (2017). Risk factors
associated with falls in older adults with dementia: a systematic review. Physiotherapy
Canada, 69(2), 161-170.
Dai, B., Yang, D., Ai, L., & Zhang, P. (2018, October). A novel video-surveillance-based algorithm of fall
detection. In 2018 11th International Congress on Image and Signal Processing, BioMedical Engineering
and Informatics (CISP-BMEI) (pp. 1-6). IEEE.
Guirguis-Blake, J. M., Michael, Y. L., Perdue, L. A., Coppola, E. L., & Beil, T. L. (2018).
Interventions to prevent falls in older adults: updated evidence report and systematic review for
the US Preventive Services Task Force. Jama, 319(16), 1705-1716.
Moncada, L. V. V., & Mire, L. G. (2017). Preventing falls in older persons. American family
physician, 96(4), 240-247.
Montero‐Odasso, M., & Speechley, M. (2018). Falls in cognitively impaired older adults:
implications for risk assessment and prevention. Journal of the american geriatrics
society, 66(2), 367-375.
Naseri, C., Haines, T. P., Etherton-Beer, C., McPhail, S., Morris, M. E., Flicker, L., ... & Hill, A.
M. (2018). Reducing falls in older adults recently discharged from hospital: a systematic review
and meta-analysis. Age and ageing, 47(4), 512-519.
Rimland, J. M., Abraha, I., Dell’Aquila, G., Cruz-Jentoft, A., Soiza, R. L., Gudmundsson, A., ...
& Cherubini, A. (2017). Non-pharmacological interventions to prevent falls in older patients:
Clinical practice recommendations–the SENATOR ONTOP Series. European Geriatric
Medicine, 8(5-6), 413-418.
Sharif, S. I., Al-Harbi, A. B., Al-Shihabi, A. M., Al-Daour, D. S., & Sharif, R. S. (2018). Falls in
the elderly: assessment of prevalence and risk factors. Pharmacy Practice (Granada), 16(3).
Stout, N. L., Santa Mina, D., Lyons, K. D., Robb, K., & Silver, J. K. (2021). A systematic review
of rehabilitation and exercise recommendations in oncology guidelines. CA: A Cancer Journal
for Clinicians, 71(2), 149-175.
Fernando, E., Fraser, M., Hendriksen, J., Kim, C. H., & Muir-Hunter, S. W. (2017). Risk factors
associated with falls in older adults with dementia: a systematic review. Physiotherapy
Canada, 69(2), 161-170.
Dai, B., Yang, D., Ai, L., & Zhang, P. (2018, October). A novel video-surveillance-based algorithm of fall
detection. In 2018 11th International Congress on Image and Signal Processing, BioMedical Engineering
and Informatics (CISP-BMEI) (pp. 1-6). IEEE.
Guirguis-Blake, J. M., Michael, Y. L., Perdue, L. A., Coppola, E. L., & Beil, T. L. (2018).
Interventions to prevent falls in older adults: updated evidence report and systematic review for
the US Preventive Services Task Force. Jama, 319(16), 1705-1716.
Moncada, L. V. V., & Mire, L. G. (2017). Preventing falls in older persons. American family
physician, 96(4), 240-247.
Montero‐Odasso, M., & Speechley, M. (2018). Falls in cognitively impaired older adults:
implications for risk assessment and prevention. Journal of the american geriatrics
society, 66(2), 367-375.
Naseri, C., Haines, T. P., Etherton-Beer, C., McPhail, S., Morris, M. E., Flicker, L., ... & Hill, A.
M. (2018). Reducing falls in older adults recently discharged from hospital: a systematic review
and meta-analysis. Age and ageing, 47(4), 512-519.
Rimland, J. M., Abraha, I., Dell’Aquila, G., Cruz-Jentoft, A., Soiza, R. L., Gudmundsson, A., ...
& Cherubini, A. (2017). Non-pharmacological interventions to prevent falls in older patients:
Clinical practice recommendations–the SENATOR ONTOP Series. European Geriatric
Medicine, 8(5-6), 413-418.
Sharif, S. I., Al-Harbi, A. B., Al-Shihabi, A. M., Al-Daour, D. S., & Sharif, R. S. (2018). Falls in
the elderly: assessment of prevalence and risk factors. Pharmacy Practice (Granada), 16(3).
Stout, N. L., Santa Mina, D., Lyons, K. D., Robb, K., & Silver, J. K. (2021). A systematic review
of rehabilitation and exercise recommendations in oncology guidelines. CA: A Cancer Journal
for Clinicians, 71(2), 149-175.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Tricco, A. C., Thomas, S. M., Veroniki, A. A., Hamid, J. S., Cogo, E., Strifler, L., ... & Straus, S.
E. (2017). Comparisons of interventions for preventing falls in older adults: a systematic review
and meta-analysis. Jama, 318(17), 1687-1699.
Zhao, H. M., Xie, Y. X., & Wang, C. (2020). Recommendations for respiratory rehabilitation in
adults with coronavirus disease 2019. Chinese medical journal, 133(13), 1595-1602.
E. (2017). Comparisons of interventions for preventing falls in older adults: a systematic review
and meta-analysis. Jama, 318(17), 1687-1699.
Zhao, H. M., Xie, Y. X., & Wang, C. (2020). Recommendations for respiratory rehabilitation in
adults with coronavirus disease 2019. Chinese medical journal, 133(13), 1595-1602.
1 out of 10
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.