Respiratory System's Response to Altitude: A Physiological Analysis
VerifiedAdded on 2022/10/04
|13
|1358
|397
Report
AI Summary
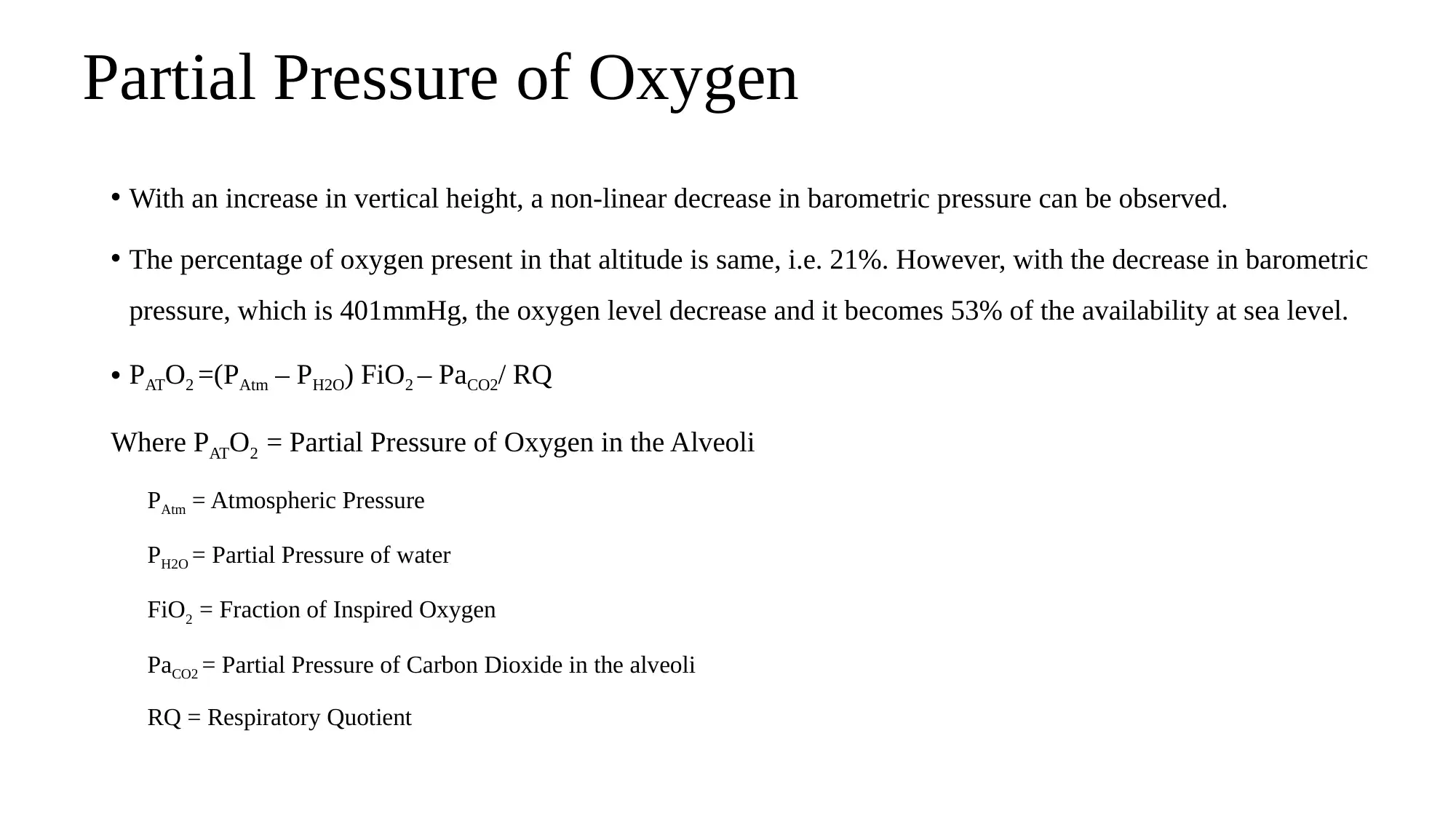
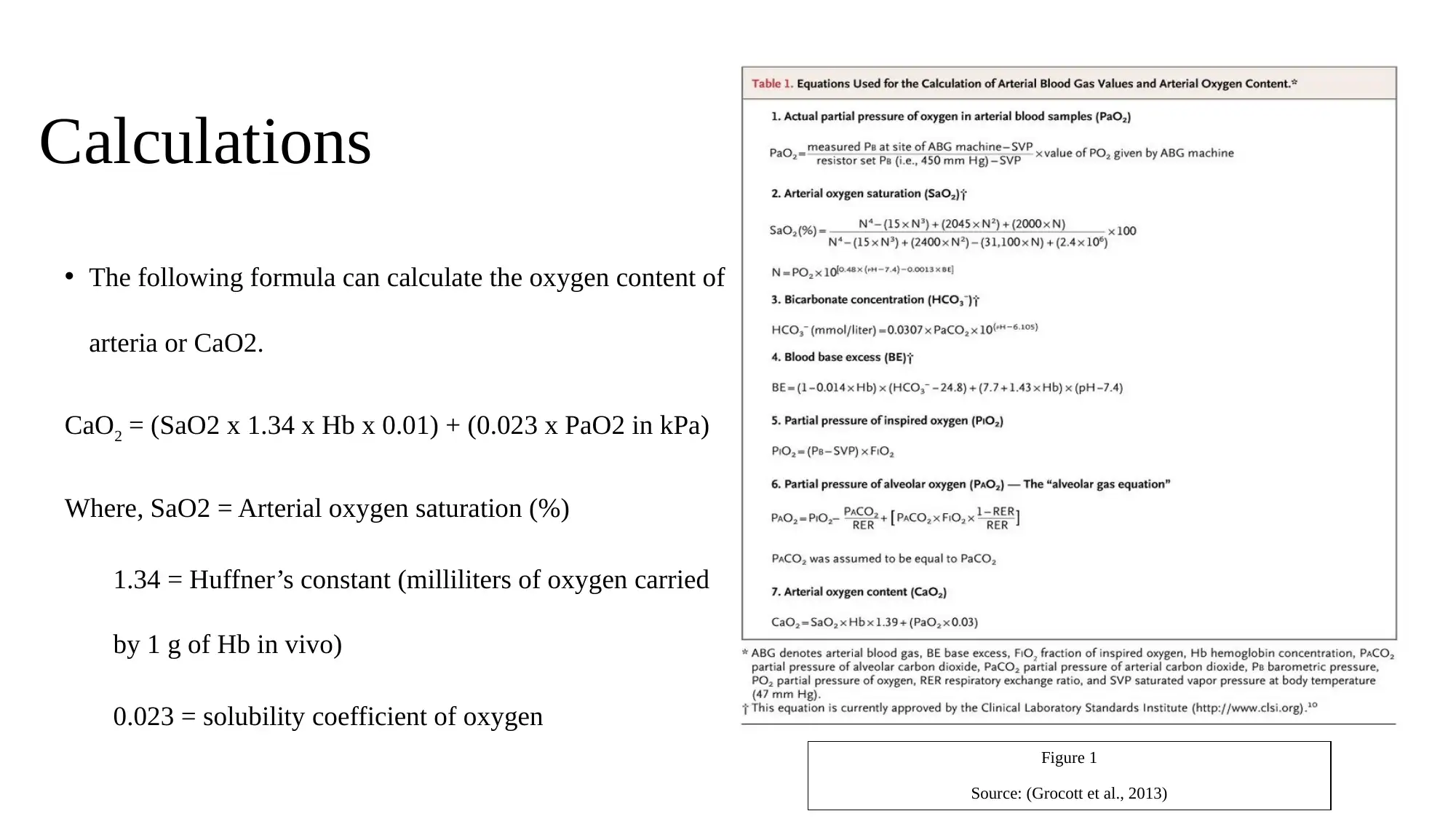
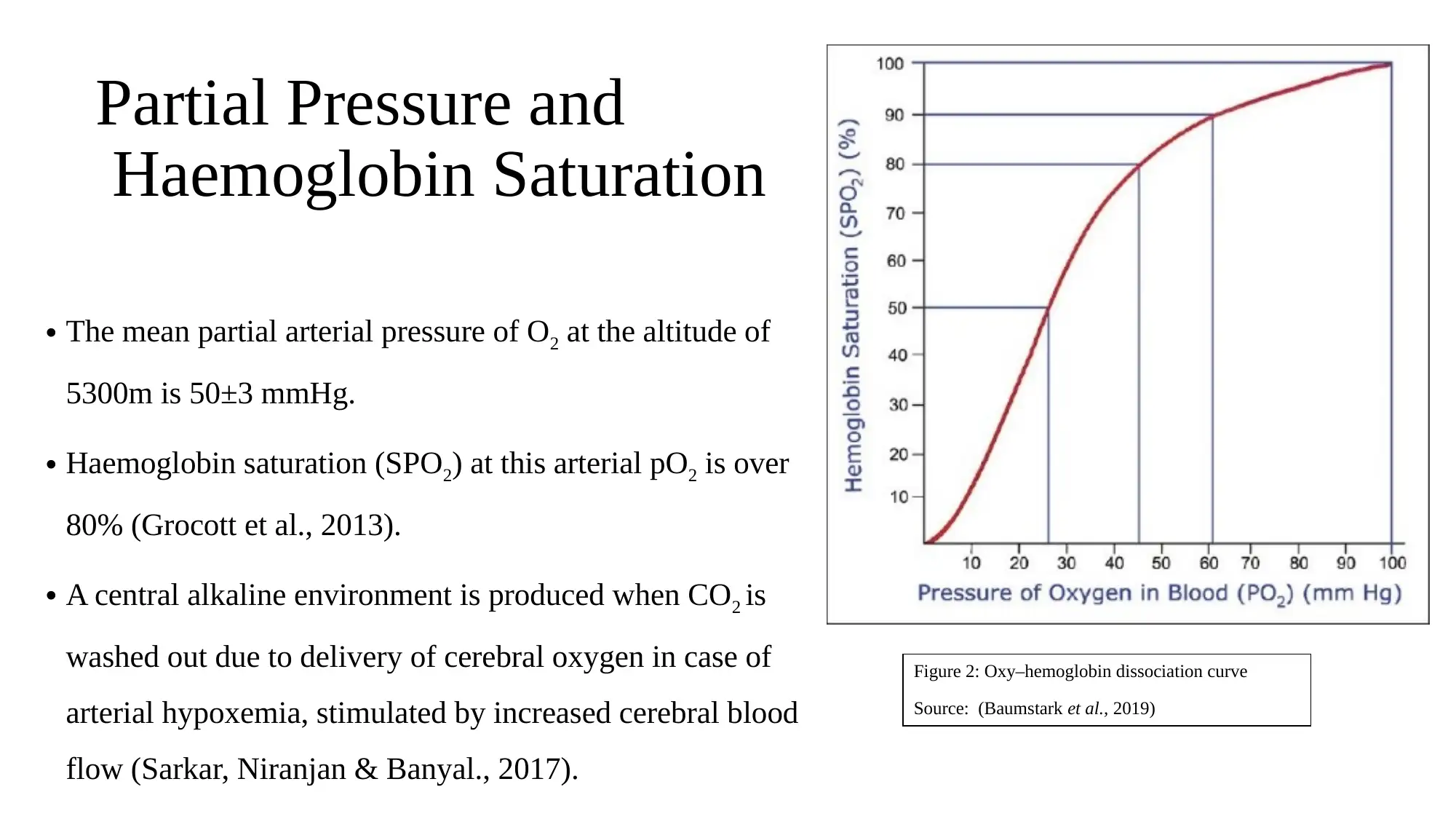
This report provides an in-depth analysis of the physiological effects of high altitude on the human respiratory system, focusing on the challenges faced at locations like Everest Base Camp. It details the decrease in oxygen partial pressure with increasing altitude and the body's acclimatization process. The report explains the calculations for oxygen content in arterial blood and the impact on hemoglobin saturation. It explores the causes and mechanisms of High Altitude Pulmonary Edema (HAPE), a severe condition resulting from inadequate acclimatization. The report also discusses the physiological responses to altitude changes, the factors contributing to HAPE, its signs, and preventive measures, including gradual ascent and medical treatments like nifedipine. The conclusion emphasizes the importance of proper acclimatization to prevent altitude-related illnesses and provides references to relevant research.
1 out of 13

Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.