A Health Workforce Plan for Bangladesh: Addressing Shortages
VerifiedAdded on 2023/06/11
|21
|4629
|493
Report
AI Summary
This report provides a comprehensive health workforce plan for Bangladesh, addressing critical challenges such as shortages of qualified healthcare professionals, inequitable distribution of personnel, and inadequate skill mix. It begins with an environmental scan, highlighting the double burden of communicable and non-communicable diseases, environmental sanitation issues, and malnutrition. The report analyzes health workforce data, revealing disparities in the distribution of doctors, nurses, and dentists across different regions. The proposed health workforce plan focuses on job creation, education and training, gender equality, healthcare service delivery, technology integration, financial resources, crisis management, international migration, cooperation, and data accountability. The plan aims to improve healthcare access and quality for all citizens, regardless of socioeconomic status, and to strengthen the overall healthcare system in Bangladesh. Desklib provides similar solved assignments and resources for students.

Running head: HEALTH WORKFORCE PLANNING
Health Workforce in Bangladesh
Name of the Student
Name of the University
Author Note
Health Workforce in Bangladesh
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1HEALTH WORKFORCE PLANNING
Executive summary
The report will illustrate the importance of a health workforce for the development of a country.
Delivery of optimal healthcare services is crucial for good health outcomes of a population and
can only be achieved through an appropriate formulation of policies and distribution of health
services. Recruitment of skilled and qualified health care personnel forms an integral part of the
building a health workforce. Thus, the government must be recruit health personnel who meet
the health preferences and needs of the entire population, regardless of the socioeconomic
conditions or other biases. However, in low income countries, there is a major shortage of
qualified healthcare providers. According to the World Health Statistics Report, 2015,
Bangladesh is a low income country that faces several challenges in its healthcare workforce due
to inequitable access, gender disparities, skill mixing and imbalances in demand and supply.
There are shortages of doctors, nurses, clinicians, midwives, and pharmacists. Therefore, this
report will produce a health workforce plan to mitigate the challenges faced by Bangladesh.
Executive summary
The report will illustrate the importance of a health workforce for the development of a country.
Delivery of optimal healthcare services is crucial for good health outcomes of a population and
can only be achieved through an appropriate formulation of policies and distribution of health
services. Recruitment of skilled and qualified health care personnel forms an integral part of the
building a health workforce. Thus, the government must be recruit health personnel who meet
the health preferences and needs of the entire population, regardless of the socioeconomic
conditions or other biases. However, in low income countries, there is a major shortage of
qualified healthcare providers. According to the World Health Statistics Report, 2015,
Bangladesh is a low income country that faces several challenges in its healthcare workforce due
to inequitable access, gender disparities, skill mixing and imbalances in demand and supply.
There are shortages of doctors, nurses, clinicians, midwives, and pharmacists. Therefore, this
report will produce a health workforce plan to mitigate the challenges faced by Bangladesh.
2HEALTH WORKFORCE PLANNING
Table of Contents
Introduction......................................................................................................................................3
Nature and extent of issue............................................................................................................3
Environmental scan.................................................................................................................3
Health workforce data profile..................................................................................................5
Health workforce plan.................................................................................................................8
1. Job creation....................................................................................................................9
2. Education, training and skills........................................................................................9
3. Women and gender right.............................................................................................10
4. Healthcare Service Delivery........................................................................................10
5. Technology..................................................................................................................11
6. Finance and fiscal space..............................................................................................11
7. Crisis and humanitarian settings..................................................................................11
8. International migration................................................................................................12
9. Cooperation and partnership.......................................................................................12
10. Data information and accountability...........................................................................12
Conclusion.................................................................................................................................12
References......................................................................................................................................14
Appendix........................................................................................................................................18
Table of Contents
Introduction......................................................................................................................................3
Nature and extent of issue............................................................................................................3
Environmental scan.................................................................................................................3
Health workforce data profile..................................................................................................5
Health workforce plan.................................................................................................................8
1. Job creation....................................................................................................................9
2. Education, training and skills........................................................................................9
3. Women and gender right.............................................................................................10
4. Healthcare Service Delivery........................................................................................10
5. Technology..................................................................................................................11
6. Finance and fiscal space..............................................................................................11
7. Crisis and humanitarian settings..................................................................................11
8. International migration................................................................................................12
9. Cooperation and partnership.......................................................................................12
10. Data information and accountability...........................................................................12
Conclusion.................................................................................................................................12
References......................................................................................................................................14
Appendix........................................................................................................................................18
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3HEALTH WORKFORCE PLANNING
Introduction
Health workforce or health human resources are defined as all individuals who are
engaged in actions, the primary intent of which is to enhance the overall health and well-being of
all citizens. Health workforce has been identified as one of the integral building blocks for an
efficient health system. The field of health workforce deals with several issues such as,
formulation, development, management, information, retention, and research on human
resources that are essential for the healthcare sector, thereby improving the population health
outcomes. An analysis of the reports suggests that health levels are relatively low in Bangladesh,
which has been categorised as a low income country (Crisp & Chen, 2014). Due to huge
population, Bangladesh faces a double burden of communicable and non-communicable
diseases. In addition to these, some of the other health problems also involve environmental
sanitation problem, and prevalence of malnutrition. This formed the rationale for choosing
Bangladesh as the country (Alam et al., 2013). Bangladesh has also been identified as one of the
major countries with severe shortage in health workers. Owing to the fact that healthcare workers
form the backbone of an appropriate healthcare system, the following report will analyse the
health workforce profile present in Bangladesh and the challenges faced by it, followed by a
recommendation to mitigate the shortage of healthcare professionals in the country, using the
WHO framework.
Nature and extent of issue
Environmental scan
Human health resources have been identified as an integral limiting factor that determines
the health of a population, besides range of behavioral, socio-economic and environmental
factors. Close correlation exists between the concentration of efficient and qualified health
Introduction
Health workforce or health human resources are defined as all individuals who are
engaged in actions, the primary intent of which is to enhance the overall health and well-being of
all citizens. Health workforce has been identified as one of the integral building blocks for an
efficient health system. The field of health workforce deals with several issues such as,
formulation, development, management, information, retention, and research on human
resources that are essential for the healthcare sector, thereby improving the population health
outcomes. An analysis of the reports suggests that health levels are relatively low in Bangladesh,
which has been categorised as a low income country (Crisp & Chen, 2014). Due to huge
population, Bangladesh faces a double burden of communicable and non-communicable
diseases. In addition to these, some of the other health problems also involve environmental
sanitation problem, and prevalence of malnutrition. This formed the rationale for choosing
Bangladesh as the country (Alam et al., 2013). Bangladesh has also been identified as one of the
major countries with severe shortage in health workers. Owing to the fact that healthcare workers
form the backbone of an appropriate healthcare system, the following report will analyse the
health workforce profile present in Bangladesh and the challenges faced by it, followed by a
recommendation to mitigate the shortage of healthcare professionals in the country, using the
WHO framework.
Nature and extent of issue
Environmental scan
Human health resources have been identified as an integral limiting factor that determines
the health of a population, besides range of behavioral, socio-economic and environmental
factors. Close correlation exists between the concentration of efficient and qualified health
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4HEALTH WORKFORCE PLANNING
workers such as, nurses, dentists, doctors, and midwives, with the major health outcomes such
as, coverage of immunization, outreach of primary health care services, and maternal and child
welfare (Truth, 2013). The Dhaka declaration recognises the critical importance of effective
healthcare workforce for functioning of the health systems, to achieve the targeted goals. It also
identified misdistribution, with respect to geography, gender, inappropriate levels of
competency, and lack of dedication, amongst the healthcare workers, directly responsible for
poor health outcomes in Bangladesh (Mahtab et al., 2015). In this regard Bangladesh has been
recognised as one of the countries with severe shortage of healthcare workers. The current
demographic scenario in the country is also characterized by a continuous increase of the
population (Chowdhury et al., 2013). Presence of ethnic minorities, who do not have access to
appropriate healthcare resources, also contributes to poor health outcomes among the population.
Evidences exist about the causal relationship between low socioeconomic status and lack of
health literacy among the vulnerable population.
Rates of morbidity and mortality are found to be significantly lower among people living
in Bangladesh, due to their poor nutrition, harmful lifestyle practices, social exclusion, and lack
of access to appropriate healthcare. Due to lack of health literacy, the overall consumption of
healthcare services in Bangladesh is comparatively low than other developing countries (Hoyler
et al., 2014). Evidences also exist that focus on increasing the overall per capita consumption
levels, in order to achieve average levels of health outcomes. Recent reports state that
Bangladesh has succeeded in lowering rates of under-five mortality, by approximately 60%,
from 146 deaths/1,000 live births (1991) to 65 (2007). The nation has also shown remarkable
progress in health and population over the past 30 years, in terms of reducing child mortality (El
Arifeen et al., 2013).
workers such as, nurses, dentists, doctors, and midwives, with the major health outcomes such
as, coverage of immunization, outreach of primary health care services, and maternal and child
welfare (Truth, 2013). The Dhaka declaration recognises the critical importance of effective
healthcare workforce for functioning of the health systems, to achieve the targeted goals. It also
identified misdistribution, with respect to geography, gender, inappropriate levels of
competency, and lack of dedication, amongst the healthcare workers, directly responsible for
poor health outcomes in Bangladesh (Mahtab et al., 2015). In this regard Bangladesh has been
recognised as one of the countries with severe shortage of healthcare workers. The current
demographic scenario in the country is also characterized by a continuous increase of the
population (Chowdhury et al., 2013). Presence of ethnic minorities, who do not have access to
appropriate healthcare resources, also contributes to poor health outcomes among the population.
Evidences exist about the causal relationship between low socioeconomic status and lack of
health literacy among the vulnerable population.
Rates of morbidity and mortality are found to be significantly lower among people living
in Bangladesh, due to their poor nutrition, harmful lifestyle practices, social exclusion, and lack
of access to appropriate healthcare. Due to lack of health literacy, the overall consumption of
healthcare services in Bangladesh is comparatively low than other developing countries (Hoyler
et al., 2014). Evidences also exist that focus on increasing the overall per capita consumption
levels, in order to achieve average levels of health outcomes. Recent reports state that
Bangladesh has succeeded in lowering rates of under-five mortality, by approximately 60%,
from 146 deaths/1,000 live births (1991) to 65 (2007). The nation has also shown remarkable
progress in health and population over the past 30 years, in terms of reducing child mortality (El
Arifeen et al., 2013).
5HEALTH WORKFORCE PLANNING
Research studies also emphasize on the fact that the burden of non-communicable
diseases has reached approximately 26% of the population, who are found to be undernourished.
46% children suffer from severe underweight problems as well (Adams et al., 2013). Bangladesh
ranks first among countries where children suffer from malnutrition. The National Health Policy
was published in the year 2011, with the aim of ensuring basic rights to adequate healthcare
services to every citizen. The policy also wants to ensure presence of an effective healthcare
system, which responds appropriately to the health needs of the nation (Prince et al., 2015).
Moreover, pursuit of the policy will also help in fulfilling demands of the citizens, in addition to
empowering and inspiring the healthcare providers.
Health workforce data profile
The human resources for health country profile are considered essential by the Ministry
Of Health And Family Welfare. This profile is generally used as a source of data for the human
resources of the country, which in turn helps to measure its progress towards achievement of the
Millennium Development Goals. It has been estimated that one third of the total healthcare
workforce is accounted for by public health personnel that is represented by doctors and nurses.
Approximately 38% of the staff are unskilled and work in Administrative Services, either as
menial stuff or support personnel. Approximately 155,000 healthcare workers are available
within the system, against the sanction the number of posts 187,500 (Ahmed et al., 2013).
Moreover, estimates also suggest that 38% of allopathic doctors work in the public healthcare
sector, while approximately 35% are under the jurisdiction of the MOHFW (refer to appendix).
Research studies also emphasize on the fact that the burden of non-communicable
diseases has reached approximately 26% of the population, who are found to be undernourished.
46% children suffer from severe underweight problems as well (Adams et al., 2013). Bangladesh
ranks first among countries where children suffer from malnutrition. The National Health Policy
was published in the year 2011, with the aim of ensuring basic rights to adequate healthcare
services to every citizen. The policy also wants to ensure presence of an effective healthcare
system, which responds appropriately to the health needs of the nation (Prince et al., 2015).
Moreover, pursuit of the policy will also help in fulfilling demands of the citizens, in addition to
empowering and inspiring the healthcare providers.
Health workforce data profile
The human resources for health country profile are considered essential by the Ministry
Of Health And Family Welfare. This profile is generally used as a source of data for the human
resources of the country, which in turn helps to measure its progress towards achievement of the
Millennium Development Goals. It has been estimated that one third of the total healthcare
workforce is accounted for by public health personnel that is represented by doctors and nurses.
Approximately 38% of the staff are unskilled and work in Administrative Services, either as
menial stuff or support personnel. Approximately 155,000 healthcare workers are available
within the system, against the sanction the number of posts 187,500 (Ahmed et al., 2013).
Moreover, estimates also suggest that 38% of allopathic doctors work in the public healthcare
sector, while approximately 35% are under the jurisdiction of the MOHFW (refer to appendix).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6HEALTH WORKFORCE PLANNING
Division Doctors Nurses Dentist
s
All Nurse per
Doctor
ratio
Barisal 1.7 0.9 0.3 3.08 0.5
Chittagong 4.8 3.6 0.3 8.8 0.7
Dhaka 10.8 2.8 0.5 14.2 0.2
Khulna 1.3 1.9 0.05 3.3 1.4
Rajshahi 2.1 1.1 0.0 3.2 0.5
Sylhet 2.2 0.4 0.0 3.2 0.1
Location
Rural 1.1 0.8 0.08 2.1 0.7
Urban 18.2 5.8 0.8 24.9 0.3
Sex
Male 4.5 0.2 0.2 5.0 0.05
Female 0.8 1.8 0.03 2.7 2.1
All 5.4 2.1 0.3 7.7 0.4
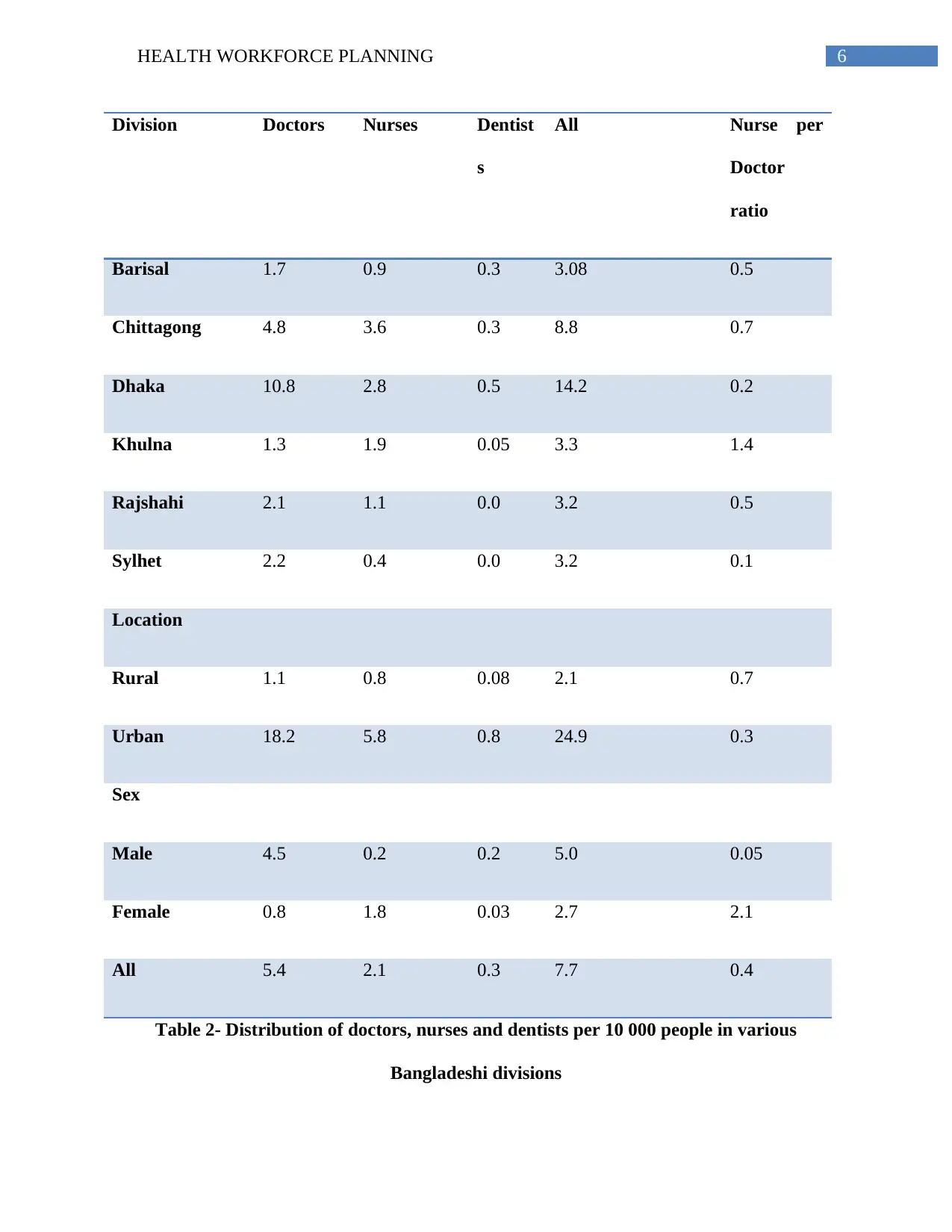
Table 2- Distribution of doctors, nurses and dentists per 10 000 people in various
Bangladeshi divisions
Division Doctors Nurses Dentist
s
All Nurse per
Doctor
ratio
Barisal 1.7 0.9 0.3 3.08 0.5
Chittagong 4.8 3.6 0.3 8.8 0.7
Dhaka 10.8 2.8 0.5 14.2 0.2
Khulna 1.3 1.9 0.05 3.3 1.4
Rajshahi 2.1 1.1 0.0 3.2 0.5
Sylhet 2.2 0.4 0.0 3.2 0.1
Location
Rural 1.1 0.8 0.08 2.1 0.7
Urban 18.2 5.8 0.8 24.9 0.3
Sex
Male 4.5 0.2 0.2 5.0 0.05
Female 0.8 1.8 0.03 2.7 2.1
All 5.4 2.1 0.3 7.7 0.4
Table 2- Distribution of doctors, nurses and dentists per 10 000 people in various
Bangladeshi divisions
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7HEALTH WORKFORCE PLANNING
(Source- Ahmed et al., 2011)
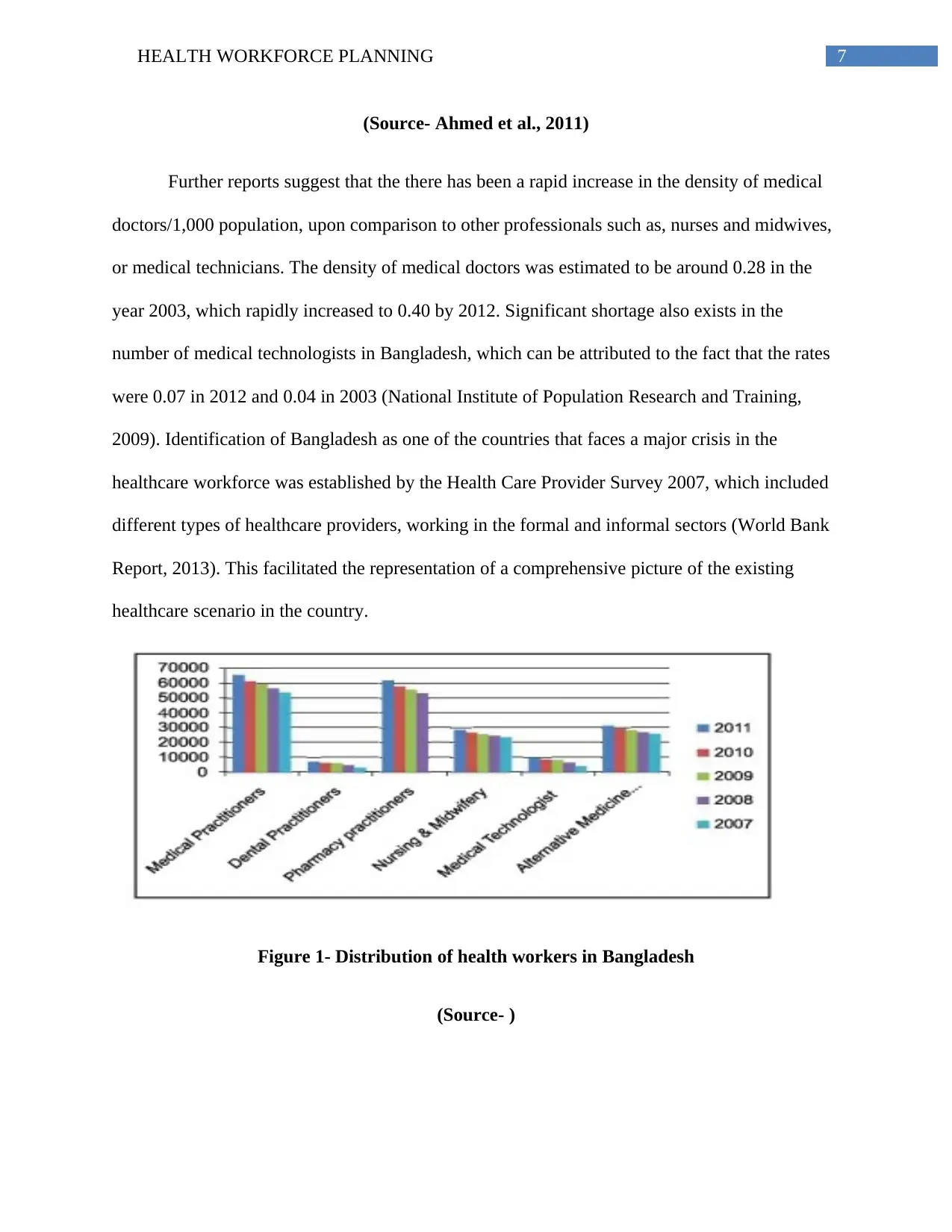
Further reports suggest that the there has been a rapid increase in the density of medical
doctors/1,000 population, upon comparison to other professionals such as, nurses and midwives,
or medical technicians. The density of medical doctors was estimated to be around 0.28 in the
year 2003, which rapidly increased to 0.40 by 2012. Significant shortage also exists in the
number of medical technologists in Bangladesh, which can be attributed to the fact that the rates
were 0.07 in 2012 and 0.04 in 2003 (National Institute of Population Research and Training,
2009). Identification of Bangladesh as one of the countries that faces a major crisis in the
healthcare workforce was established by the Health Care Provider Survey 2007, which included
different types of healthcare providers, working in the formal and informal sectors (World Bank
Report, 2013). This facilitated the representation of a comprehensive picture of the existing
healthcare scenario in the country.
Figure 1- Distribution of health workers in Bangladesh
(Source- )
(Source- Ahmed et al., 2011)
Further reports suggest that the there has been a rapid increase in the density of medical
doctors/1,000 population, upon comparison to other professionals such as, nurses and midwives,
or medical technicians. The density of medical doctors was estimated to be around 0.28 in the
year 2003, which rapidly increased to 0.40 by 2012. Significant shortage also exists in the
number of medical technologists in Bangladesh, which can be attributed to the fact that the rates
were 0.07 in 2012 and 0.04 in 2003 (National Institute of Population Research and Training,
2009). Identification of Bangladesh as one of the countries that faces a major crisis in the
healthcare workforce was established by the Health Care Provider Survey 2007, which included
different types of healthcare providers, working in the formal and informal sectors (World Bank
Report, 2013). This facilitated the representation of a comprehensive picture of the existing
healthcare scenario in the country.
Figure 1- Distribution of health workers in Bangladesh
(Source- )
8HEALTH WORKFORCE PLANNING
Findings from the survey suggested that the density of physicians and nurses had
increased over the last decades, from 1.1 nurses and 1.9 physicians in 1998 to 2.1 nurses and 5.4
physicians in 2007. However, the increase was quite lower than the average health workforce,
estimated from low income countries (WHO, 2014). A slight increase was also observed in the
density of dentists as well. However, significant disparities exist between the density of qualified
healthcare professionals such as, physicians, nurse, and dentists, when compared to other South
Asian Countries (Human Resources Management Unit, 2013). This falls significantly short of the
projected estimates by the WHO, which is crucial for achieving the MDG targets. The data
presented above and in the appendix also indicate that there exists an overwhelming urban bias
related to the distribution of formerly qualified healthcare providers. This inequitable distribution
shows more concentration of the professionals in regions of Dhaka and Chittagong. The
community health workers associated with non-governmental sectors are found to be
concentrated in rural areas. Inequitable distribution of drug retail outlets also demonstrates their
unhindered expansion across the nation.
Health workforce plan
The health workforce plan of Bangladesh has the primary objective of addressing the
challenges that are associated with shortage of qualified healthcare professionals, inappropriate
skill mix of the nurse to doctor ratio, inequitable distribution of healthcare personnel, and poor
health literacy. This health workforce plans to improve the existing conditions in both urban and
rural regions of the nation. It intends to implement an approach that will focus on delivery of
optimal quality healthcare services to all citizens, regardless of their socioeconomic status. This
plan will also help in eliminating the imbalances that threaten the potential capacity of the
existing health care system in Bangladesh. Some of the major challenges that will be eliminated
Findings from the survey suggested that the density of physicians and nurses had
increased over the last decades, from 1.1 nurses and 1.9 physicians in 1998 to 2.1 nurses and 5.4
physicians in 2007. However, the increase was quite lower than the average health workforce,
estimated from low income countries (WHO, 2014). A slight increase was also observed in the
density of dentists as well. However, significant disparities exist between the density of qualified
healthcare professionals such as, physicians, nurse, and dentists, when compared to other South
Asian Countries (Human Resources Management Unit, 2013). This falls significantly short of the
projected estimates by the WHO, which is crucial for achieving the MDG targets. The data
presented above and in the appendix also indicate that there exists an overwhelming urban bias
related to the distribution of formerly qualified healthcare providers. This inequitable distribution
shows more concentration of the professionals in regions of Dhaka and Chittagong. The
community health workers associated with non-governmental sectors are found to be
concentrated in rural areas. Inequitable distribution of drug retail outlets also demonstrates their
unhindered expansion across the nation.
Health workforce plan
The health workforce plan of Bangladesh has the primary objective of addressing the
challenges that are associated with shortage of qualified healthcare professionals, inappropriate
skill mix of the nurse to doctor ratio, inequitable distribution of healthcare personnel, and poor
health literacy. This health workforce plans to improve the existing conditions in both urban and
rural regions of the nation. It intends to implement an approach that will focus on delivery of
optimal quality healthcare services to all citizens, regardless of their socioeconomic status. This
plan will also help in eliminating the imbalances that threaten the potential capacity of the
existing health care system in Bangladesh. Some of the major challenges that will be eliminated
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9HEALTH WORKFORCE PLANNING
by the plan encompass the problems faced by rural communities, in recruiting qualified
healthcare professionals and providing training and education opportunities to the existing staff.
The plan will also help in identification of the need for an improved educational partnership
between medical and academic institutions to improve commitment of healthcare workers to
workplace diversity in the nation.
1. Job creation
There is a need to stimulate investments in the development of decent jobs in the healthcare
sector in Bangladesh, particularly for the women, owing to the fact that only 20-30% healthcare
personnel are females. Urgent action must be taken for the development of policies related to the
existing labour market in Bangladesh, which in turn would foster the need of enforcing a
sustainable and qualified health care workforce in the nation. The existing government policies
related to health should also be addressed for identifying the systemic issues, which in turn
would result in subsequent changes in the health labour market and would reduce rates of public
failure (Gaziano et al., 2015). Motivating the youth, who form a large proportion of the entire
population, and creating provisions for their training and education would empower them and
facilitate their engagement in jobs related to the healthcare human resources. This can be
achieved by gathering funds and sponsors that would help the youth to enroll them in the
educational and training institutes present across Bangladesh.
2. Education, training and skills
Efforts must be taken by the governmental policies of the country to prioritise their
investment in all kinds of education and training. The policies should focus on shifting away
educational models from narrow subject specialisations and should build in locally relevant
competencies in near future. This can be achieved by scaling up high quality education, which
by the plan encompass the problems faced by rural communities, in recruiting qualified
healthcare professionals and providing training and education opportunities to the existing staff.
The plan will also help in identification of the need for an improved educational partnership
between medical and academic institutions to improve commitment of healthcare workers to
workplace diversity in the nation.
1. Job creation
There is a need to stimulate investments in the development of decent jobs in the healthcare
sector in Bangladesh, particularly for the women, owing to the fact that only 20-30% healthcare
personnel are females. Urgent action must be taken for the development of policies related to the
existing labour market in Bangladesh, which in turn would foster the need of enforcing a
sustainable and qualified health care workforce in the nation. The existing government policies
related to health should also be addressed for identifying the systemic issues, which in turn
would result in subsequent changes in the health labour market and would reduce rates of public
failure (Gaziano et al., 2015). Motivating the youth, who form a large proportion of the entire
population, and creating provisions for their training and education would empower them and
facilitate their engagement in jobs related to the healthcare human resources. This can be
achieved by gathering funds and sponsors that would help the youth to enroll them in the
educational and training institutes present across Bangladesh.
2. Education, training and skills
Efforts must be taken by the governmental policies of the country to prioritise their
investment in all kinds of education and training. The policies should focus on shifting away
educational models from narrow subject specialisations and should build in locally relevant
competencies in near future. This can be achieved by scaling up high quality education, which
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10HEALTH WORKFORCE PLANNING
will assist all healthcare workers to acquire skills that are required in their profession, which in
turn would help them match and the meet the healthcare preferences and demands of the entire
population. Appropriate training and education will also allow the healthcare professionals to
work according to their full potential. This in turn can be facilitated by addressing all kinds of
geographical inequities that exist in the country. Removing such inequities between the rural and
urban areas would help in strengthening youth education and facilitate their employment in the
healthcare sector.
3. Women and gender right
Disparities exist between men and women in their ability to gain adequate access to
healthcare services or be a part of the healthcare workforce in Bangladesh. Status of women in
the country has been identified as a major obstacle to their development in the healthcare work
force. Therefore, they must be provided opportunities to gain better excess of healthcare services
and should also be allowed to work in partnership with men at different levels of the healthcare
sector, including policymaking stages (Khera et al., 2014). Economic participation of females
should be maximized, which in turn will lead to their empowerment by reinforcing skills of
leadership and addressing all forms of inequity and gender bias that exists in health labour
market and education system.
4. Healthcare Service Delivery
Integrated patient centred healthcare services are imperative for reaching universal health
coverage (Reich et al., 2016). Optimal health care services should focus around the health needs
and preferences of people and the community, rather than on the prevalence of diseases. The
country should focus on implementing reforms service models that emphasize on hospital care,
instead of preventing rates of diseases (Quayyum et al., 2013). Efforts must also be taken to
will assist all healthcare workers to acquire skills that are required in their profession, which in
turn would help them match and the meet the healthcare preferences and demands of the entire
population. Appropriate training and education will also allow the healthcare professionals to
work according to their full potential. This in turn can be facilitated by addressing all kinds of
geographical inequities that exist in the country. Removing such inequities between the rural and
urban areas would help in strengthening youth education and facilitate their employment in the
healthcare sector.
3. Women and gender right
Disparities exist between men and women in their ability to gain adequate access to
healthcare services or be a part of the healthcare workforce in Bangladesh. Status of women in
the country has been identified as a major obstacle to their development in the healthcare work
force. Therefore, they must be provided opportunities to gain better excess of healthcare services
and should also be allowed to work in partnership with men at different levels of the healthcare
sector, including policymaking stages (Khera et al., 2014). Economic participation of females
should be maximized, which in turn will lead to their empowerment by reinforcing skills of
leadership and addressing all forms of inequity and gender bias that exists in health labour
market and education system.
4. Healthcare Service Delivery
Integrated patient centred healthcare services are imperative for reaching universal health
coverage (Reich et al., 2016). Optimal health care services should focus around the health needs
and preferences of people and the community, rather than on the prevalence of diseases. The
country should focus on implementing reforms service models that emphasize on hospital care,
instead of preventing rates of diseases (Quayyum et al., 2013). Efforts must also be taken to
11HEALTH WORKFORCE PLANNING
deliver integrated community based and affordable ambulatory and primary care to all people,
with a special attention to those living in underserved areas. This can be facilitated by adoption
of appropriate policy and social business models that will help in serving the disadvantaged
people.
5. Technology
The governmental policies should try to harness powers of communication technologies
and cost-effective information technologies for enhancing health education and literacy among
all sections of the society (Ahmed et al., 2014). Use of appropriate mobile and wireless
technology will also help in a better communication between patients and physicians, in addition
to constant monitoring of patients living in remote regions of the country (Agarwal et al., 2015).
Digital technologies will also help in enhancing access of all people to necessary healthcare
services, and will improve responsiveness of the existing systems thereby enhancing delivery of
primary health care.
6. Finance and fiscal space
Effects must be taken by the government to gather adequate funding from international and
domestic bodies, in addition to private and public organizations, for the enforcement and
implementation of appropriate health financing reforms that will help in investing in the correct
skills and working conditions for all health workers. Sustainable health financing can be secured
through public revenues (Balabanova et al., 2013). Political commitment and societal dialogue
will play an important role in bringing about macroeconomic reforms in the country that will
also attract co-investment from the private sector.
deliver integrated community based and affordable ambulatory and primary care to all people,
with a special attention to those living in underserved areas. This can be facilitated by adoption
of appropriate policy and social business models that will help in serving the disadvantaged
people.
5. Technology
The governmental policies should try to harness powers of communication technologies
and cost-effective information technologies for enhancing health education and literacy among
all sections of the society (Ahmed et al., 2014). Use of appropriate mobile and wireless
technology will also help in a better communication between patients and physicians, in addition
to constant monitoring of patients living in remote regions of the country (Agarwal et al., 2015).
Digital technologies will also help in enhancing access of all people to necessary healthcare
services, and will improve responsiveness of the existing systems thereby enhancing delivery of
primary health care.
6. Finance and fiscal space
Effects must be taken by the government to gather adequate funding from international and
domestic bodies, in addition to private and public organizations, for the enforcement and
implementation of appropriate health financing reforms that will help in investing in the correct
skills and working conditions for all health workers. Sustainable health financing can be secured
through public revenues (Balabanova et al., 2013). Political commitment and societal dialogue
will play an important role in bringing about macroeconomic reforms in the country that will
also attract co-investment from the private sector.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 21
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.