Mr. Hunter's Pneumonia: Nursing Care, Pathophysiology, and Strategies
VerifiedAdded on 2020/01/23
|12
|3557
|45
Report
AI Summary
This report presents a comprehensive analysis of the nursing care provided to Mr. Edward Hunter, an 89-year-old widower admitted with pneumonia. It delves into the specific considerations for registered nurses regarding clinical manifestations in older adults, highlighting the importance of recognizing atypical presentations and the impact of Mr. Hunter's recent myocardial infarction. The report outlines the pathophysiology of altered ventilation and diffusion in pneumonia, including the impact on cellular and tissue responses. It differentiates between hospital-acquired, community-acquired, and aspiration pneumonia, including causative organisms. A detailed nursing care plan for Mr. Hunter is provided, with rationales for all elements, including airway clearance, fluid balance, nutrition, and infection control. The report also explains the rationale for monitoring specific parameters requested by the consultant, such as heart rate, oxygen saturation, and temperature. Furthermore, it explores strategies to ensure Mr. Hunter's understanding of his decisions and actions to manage his care, given his preference for self-direction. Finally, the report concludes with reflections on key learning points and implications for future nursing practice.
HEALTH ALTERATION AND CONTEXT OF
PRACTICE
1
PRACTICE
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENTS
Introduction......................................................................................................................................3
Question 1........................................................................................................................................3
What are the specific considerations a registered nurse should understand in relation to the
clinical manifestations of pneumonia in the older person?.........................................................3
Question 2........................................................................................................................................4
Outline the pathophysiology of altered ventilation and diffusion in relation to Mr Hunter’s
pneumonia. Include pathological response in cells and tissues...................................................4
Question 3........................................................................................................................................5
What are the differences between hospital acquired pneumonia, community acquired
pneumonia and aspiration pneumonia. Include causative organisms..........................................5
Question 4........................................................................................................................................6
Explain the nursing care required by the patient with pneumonia. Provide a rationale for all
elements of the care provided that reflects the particular needs of Mr Hunter............................6
Question 5........................................................................................................................................7
In the context of a patient with pneumonia, explain the rationales for monitoring the specific
parameters requested by the consultant.......................................................................................7
Question 6........................................................................................................................................8
(1) The strategies you would use to ensure Mr Hunters understands the implications of his
decisions......................................................................................................................................8
(2) The actions you would take to manage the situation.............................................................9
Question 7........................................................................................................................................9
What are the two most important things that you have learned from this scenario and why?
What actions will you take in your future practice because of what you have learned from this
scenario?......................................................................................................................................9
Conclusion.......................................................................................................................................9
2
Introduction......................................................................................................................................3
Question 1........................................................................................................................................3
What are the specific considerations a registered nurse should understand in relation to the
clinical manifestations of pneumonia in the older person?.........................................................3
Question 2........................................................................................................................................4
Outline the pathophysiology of altered ventilation and diffusion in relation to Mr Hunter’s
pneumonia. Include pathological response in cells and tissues...................................................4
Question 3........................................................................................................................................5
What are the differences between hospital acquired pneumonia, community acquired
pneumonia and aspiration pneumonia. Include causative organisms..........................................5
Question 4........................................................................................................................................6
Explain the nursing care required by the patient with pneumonia. Provide a rationale for all
elements of the care provided that reflects the particular needs of Mr Hunter............................6
Question 5........................................................................................................................................7
In the context of a patient with pneumonia, explain the rationales for monitoring the specific
parameters requested by the consultant.......................................................................................7
Question 6........................................................................................................................................8
(1) The strategies you would use to ensure Mr Hunters understands the implications of his
decisions......................................................................................................................................8
(2) The actions you would take to manage the situation.............................................................9
Question 7........................................................................................................................................9
What are the two most important things that you have learned from this scenario and why?
What actions will you take in your future practice because of what you have learned from this
scenario?......................................................................................................................................9
Conclusion.......................................................................................................................................9
2

References......................................................................................................................................10
3
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
INTRODUCTION
In the present case, discussion has been included regarding Mr. Edward Hunter who is an
89 year old widower and is was admitted in the medical ward because of the saturated oxygen
and viral influenza. From last 6 months, he has been receiving intensive home support from the
acute care home which also includes oxygen therapy. Hence, considering his situation,
discussion has been included altered pathophysiology of his health dimensions. In this respect,
research has also stated difference between hospital acquired pneumonia and community
acquired pneumonia. Along with this, suitable nursing care for the patient is also included in the
study with the strategies of controlling and monitoring.
QUESTION 1
What are the specific considerations a registered nurse should understand in relation to the
clinical manifestations of pneumonia in the older person?
It is important for a Registered Nurse to understand and interpret the differentiating
clinical manifestations of the older patient in comparison to younger patients. Clinical
manifestations can be objective as seen by a professional, or subjective as expressed by the
patient. In many cases, older individuals conditions develop and progress contrarily making
understanding by health professionals crucial for treatment and patient wellbeing (Söderström
and et. al., 2017). The elderly have a poorer immune system that means, it is more difficult for
their bodies to fight infections naturally. It is important for the RN to consider all clinical
manifestations presented by Mr Hunter. The clinical manifestations existing on Mr Hunters
arrival are concerning and show his condition is rapidly deteriorating. As Mr Hunter suffered a
myocardial infarction only one month ago, his chances of adapting pneumonia were increasingly
high.
As per the requirement of clinical manifestation, it is essential for the registered nurse to
emphasize on the immune system as through then only, the patient is able to cope up with the
diseases. It is also analysed that overnight Mr Hunter becomes restless and at the same time he
barely eats because of little appetite (Scannapieco and Shay, 2014). Thus, considering the same
aspect it is essential for the registered nurse to review the pleuritic pain on inspiration so as to
identify if the patient has the chances to develop pneumococcal pneumonia. Thus, registered
nurse is required to focus on all the diagnosis because that depicts the actual condition of the
4
In the present case, discussion has been included regarding Mr. Edward Hunter who is an
89 year old widower and is was admitted in the medical ward because of the saturated oxygen
and viral influenza. From last 6 months, he has been receiving intensive home support from the
acute care home which also includes oxygen therapy. Hence, considering his situation,
discussion has been included altered pathophysiology of his health dimensions. In this respect,
research has also stated difference between hospital acquired pneumonia and community
acquired pneumonia. Along with this, suitable nursing care for the patient is also included in the
study with the strategies of controlling and monitoring.
QUESTION 1
What are the specific considerations a registered nurse should understand in relation to the
clinical manifestations of pneumonia in the older person?
It is important for a Registered Nurse to understand and interpret the differentiating
clinical manifestations of the older patient in comparison to younger patients. Clinical
manifestations can be objective as seen by a professional, or subjective as expressed by the
patient. In many cases, older individuals conditions develop and progress contrarily making
understanding by health professionals crucial for treatment and patient wellbeing (Söderström
and et. al., 2017). The elderly have a poorer immune system that means, it is more difficult for
their bodies to fight infections naturally. It is important for the RN to consider all clinical
manifestations presented by Mr Hunter. The clinical manifestations existing on Mr Hunters
arrival are concerning and show his condition is rapidly deteriorating. As Mr Hunter suffered a
myocardial infarction only one month ago, his chances of adapting pneumonia were increasingly
high.
As per the requirement of clinical manifestation, it is essential for the registered nurse to
emphasize on the immune system as through then only, the patient is able to cope up with the
diseases. It is also analysed that overnight Mr Hunter becomes restless and at the same time he
barely eats because of little appetite (Scannapieco and Shay, 2014). Thus, considering the same
aspect it is essential for the registered nurse to review the pleuritic pain on inspiration so as to
identify if the patient has the chances to develop pneumococcal pneumonia. Thus, registered
nurse is required to focus on all the diagnosis because that depicts the actual condition of the
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
patient. At the same time, emphasis can also be laid towards the symptoms as that might affect
the health prospects of Mr Hunter.
QUESTION 2
Outline the pathophysiology of altered ventilation and diffusion in relation to Mr Hunter’s
pneumonia. Include pathological response in cells and tissues
Afterwards, reviewing the existing case of Mr Hunter, it is clear that the degree of
ventilation and diffusion has been changed because of pneumococcal pneumonia. Ventilatory
failure and hypoxemic respiratory are the major forms that exists in pneumococcal pneumonia. It
also brings changes in the lungs; hence it leads inflammatory exudate that affects the normal
functioning residual capacity (Rogus‐Pulia and et. al., 2016). At the same time, it also causes loss
of volume in the pulmonary infiltrate. It also consolidates the air space; hence it easily enhances
the transpulmonary pressure. At the same time, the loss of volume also diminishes the total lung
compliance which further enhances the level of oxygen saturation.
There is also an evidence that arterial hypoxemia exists in pneumococcal pneumonia and
that is also caused by pulmonary artery blood flow. This also fuses the lung in an intrapulmonary
diversion. This is also caused by intrapulmonary oxygen consumption that exist in the lung
because of ventilation perfusion (Quinn and et. al., 2014). It is also ascertained that the
persistence of pulmonary blood flow to lungs is caused by failure in the hypoxic pulmonary
vasoconstriction mechanism. There are a number of factors that change the distribution of
pulmonary blood flow. Similarly, it also increases consolidation in the lungs which
systematically changes the ratio of diffusion. Therefore, it brings certain changes in the
respiratory system; hence intensive supportive measures can be applied to treat Mr Hunter.
However, on the other hand, considering the present situation of Mr Hunter it is essential
for the registered nurse to adopt necessary measures so that his situation can be improved. Future
management is essential in this case because elderly patients are unable to tackle the changing
health conditions (Matsuda and et. al., 2016). During optimistic pressure on mechanical
ventilation, both the vessels are compressed which enhances the chances of lung inflation and
pulmonary vascular resistance. Nonetheless, hypoxic pulmonary vasoconstriction changes the
direction of blood because it exists on global basis. It is also ascertained that it greatly enhances
5
the health prospects of Mr Hunter.
QUESTION 2
Outline the pathophysiology of altered ventilation and diffusion in relation to Mr Hunter’s
pneumonia. Include pathological response in cells and tissues
Afterwards, reviewing the existing case of Mr Hunter, it is clear that the degree of
ventilation and diffusion has been changed because of pneumococcal pneumonia. Ventilatory
failure and hypoxemic respiratory are the major forms that exists in pneumococcal pneumonia. It
also brings changes in the lungs; hence it leads inflammatory exudate that affects the normal
functioning residual capacity (Rogus‐Pulia and et. al., 2016). At the same time, it also causes loss
of volume in the pulmonary infiltrate. It also consolidates the air space; hence it easily enhances
the transpulmonary pressure. At the same time, the loss of volume also diminishes the total lung
compliance which further enhances the level of oxygen saturation.
There is also an evidence that arterial hypoxemia exists in pneumococcal pneumonia and
that is also caused by pulmonary artery blood flow. This also fuses the lung in an intrapulmonary
diversion. This is also caused by intrapulmonary oxygen consumption that exist in the lung
because of ventilation perfusion (Quinn and et. al., 2014). It is also ascertained that the
persistence of pulmonary blood flow to lungs is caused by failure in the hypoxic pulmonary
vasoconstriction mechanism. There are a number of factors that change the distribution of
pulmonary blood flow. Similarly, it also increases consolidation in the lungs which
systematically changes the ratio of diffusion. Therefore, it brings certain changes in the
respiratory system; hence intensive supportive measures can be applied to treat Mr Hunter.
However, on the other hand, considering the present situation of Mr Hunter it is essential
for the registered nurse to adopt necessary measures so that his situation can be improved. Future
management is essential in this case because elderly patients are unable to tackle the changing
health conditions (Matsuda and et. al., 2016). During optimistic pressure on mechanical
ventilation, both the vessels are compressed which enhances the chances of lung inflation and
pulmonary vascular resistance. Nonetheless, hypoxic pulmonary vasoconstriction changes the
direction of blood because it exists on global basis. It is also ascertained that it greatly enhances
5

the load of the right ventricle which at the same time increases pulmonary artery pressure; hence
as a result it leads to pulmonary edema.
QUESTION 3
What are the differences between hospital acquired pneumonia, community acquired pneumonia
and aspiration pneumonia. Include causative organisms
There are many different types of pneumonia, and for the purpose of this question only
three will be discussed in further detail. These three are hospital acquired pneumonia (HAP),
community acquired pneumonia (CAP) and aspiration pneumonia. HAP is bacterial and occurs
more than 48 hours after a hospital admission with no signs or symptoms of infection during
their admission (Lumb, 2016). This particular type of pneumonia is bacterial and considered the
most lethal, one reason being the development in individuals with existing respiratory failure.
Majority of patients obtain multiple causative organisms which include pathogens Enterobacter
special, Escherichia coli, H. influenza, Klebsiella species, P. aerunginosa, Proteus, Serratia
marcescens, methicillin-sensitive or methicillin-resistant Staphylococcus aureus and S.
pneumonia.
Symptoms for the bacterial HAP are similar to the viral CAP and can often be hard to
differentiate. These include respiratory difficulty, fever, cough, sputum and malaise. Elderly
patient’s risks of contracting infection are particularly higher and are classified to be in the same
category as those with diabetes, alcoholism and chronic lung disease. CAP occurs in the
community setting and also within the first 48 hours of a patient being hospitalised due to the
contraction of pneumonia (Luks, 2015). Some causative organisms for patients with CAP are
Streptococcus pneumonia, mycoplasma pneumonia, and H. influenza. Aspiration pneumonia is
usually bacterial and can take place in the community and hospital setting. This is due to
endogenous or exogenous substances being located in the lower airway. Causative organisms for
aspiration pneumonia are H. influenza, S. pneumonia and S. aureus.
Thus, according to Mr Hunter’s current situation, it is essential for the registered nurse to
carry out all the diagnosis so that proper treatment can be delivered. Looking towards the exact
current situation, it is vital for the registered nurses to emphasize on proper observation and
monitoring. Registered nurses are also required to observe if the causative organisms are
increasing in the body of Mr Hunter. As per the age groups, organisms keep on changing; hence
6
as a result it leads to pulmonary edema.
QUESTION 3
What are the differences between hospital acquired pneumonia, community acquired pneumonia
and aspiration pneumonia. Include causative organisms
There are many different types of pneumonia, and for the purpose of this question only
three will be discussed in further detail. These three are hospital acquired pneumonia (HAP),
community acquired pneumonia (CAP) and aspiration pneumonia. HAP is bacterial and occurs
more than 48 hours after a hospital admission with no signs or symptoms of infection during
their admission (Lumb, 2016). This particular type of pneumonia is bacterial and considered the
most lethal, one reason being the development in individuals with existing respiratory failure.
Majority of patients obtain multiple causative organisms which include pathogens Enterobacter
special, Escherichia coli, H. influenza, Klebsiella species, P. aerunginosa, Proteus, Serratia
marcescens, methicillin-sensitive or methicillin-resistant Staphylococcus aureus and S.
pneumonia.
Symptoms for the bacterial HAP are similar to the viral CAP and can often be hard to
differentiate. These include respiratory difficulty, fever, cough, sputum and malaise. Elderly
patient’s risks of contracting infection are particularly higher and are classified to be in the same
category as those with diabetes, alcoholism and chronic lung disease. CAP occurs in the
community setting and also within the first 48 hours of a patient being hospitalised due to the
contraction of pneumonia (Luks, 2015). Some causative organisms for patients with CAP are
Streptococcus pneumonia, mycoplasma pneumonia, and H. influenza. Aspiration pneumonia is
usually bacterial and can take place in the community and hospital setting. This is due to
endogenous or exogenous substances being located in the lower airway. Causative organisms for
aspiration pneumonia are H. influenza, S. pneumonia and S. aureus.
Thus, according to Mr Hunter’s current situation, it is essential for the registered nurse to
carry out all the diagnosis so that proper treatment can be delivered. Looking towards the exact
current situation, it is vital for the registered nurses to emphasize on proper observation and
monitoring. Registered nurses are also required to observe if the causative organisms are
increasing in the body of Mr Hunter. As per the age groups, organisms keep on changing; hence
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
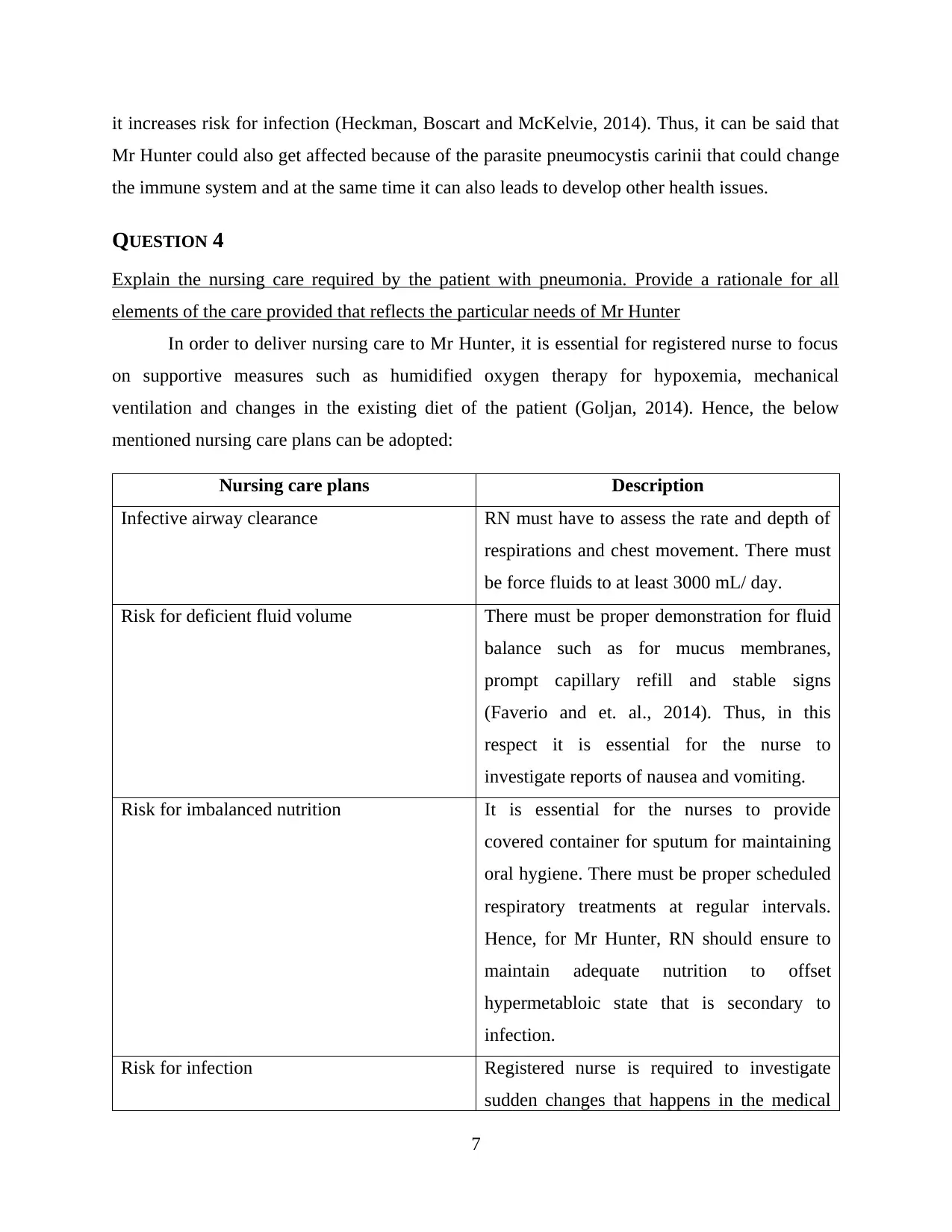
it increases risk for infection (Heckman, Boscart and McKelvie, 2014). Thus, it can be said that
Mr Hunter could also get affected because of the parasite pneumocystis carinii that could change
the immune system and at the same time it can also leads to develop other health issues.
QUESTION 4
Explain the nursing care required by the patient with pneumonia. Provide a rationale for all
elements of the care provided that reflects the particular needs of Mr Hunter
In order to deliver nursing care to Mr Hunter, it is essential for registered nurse to focus
on supportive measures such as humidified oxygen therapy for hypoxemia, mechanical
ventilation and changes in the existing diet of the patient (Goljan, 2014). Hence, the below
mentioned nursing care plans can be adopted:
Nursing care plans Description
Infective airway clearance RN must have to assess the rate and depth of
respirations and chest movement. There must
be force fluids to at least 3000 mL/ day.
Risk for deficient fluid volume There must be proper demonstration for fluid
balance such as for mucus membranes,
prompt capillary refill and stable signs
(Faverio and et. al., 2014). Thus, in this
respect it is essential for the nurse to
investigate reports of nausea and vomiting.
Risk for imbalanced nutrition It is essential for the nurses to provide
covered container for sputum for maintaining
oral hygiene. There must be proper scheduled
respiratory treatments at regular intervals.
Hence, for Mr Hunter, RN should ensure to
maintain adequate nutrition to offset
hypermetabloic state that is secondary to
infection.
Risk for infection Registered nurse is required to investigate
sudden changes that happens in the medical
7
Mr Hunter could also get affected because of the parasite pneumocystis carinii that could change
the immune system and at the same time it can also leads to develop other health issues.
QUESTION 4
Explain the nursing care required by the patient with pneumonia. Provide a rationale for all
elements of the care provided that reflects the particular needs of Mr Hunter
In order to deliver nursing care to Mr Hunter, it is essential for registered nurse to focus
on supportive measures such as humidified oxygen therapy for hypoxemia, mechanical
ventilation and changes in the existing diet of the patient (Goljan, 2014). Hence, the below
mentioned nursing care plans can be adopted:
Nursing care plans Description
Infective airway clearance RN must have to assess the rate and depth of
respirations and chest movement. There must
be force fluids to at least 3000 mL/ day.
Risk for deficient fluid volume There must be proper demonstration for fluid
balance such as for mucus membranes,
prompt capillary refill and stable signs
(Faverio and et. al., 2014). Thus, in this
respect it is essential for the nurse to
investigate reports of nausea and vomiting.
Risk for imbalanced nutrition It is essential for the nurses to provide
covered container for sputum for maintaining
oral hygiene. There must be proper scheduled
respiratory treatments at regular intervals.
Hence, for Mr Hunter, RN should ensure to
maintain adequate nutrition to offset
hypermetabloic state that is secondary to
infection.
Risk for infection Registered nurse is required to investigate
sudden changes that happens in the medical
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

condition such as increasing chest pain, heart
rate and altered sensorium. Further, nurses
can also monitor effectiveness of
antimicrobial therapy (Coker and et. al.,
2017).
QUESTION 5
In the context of a patient with pneumonia, explain the rationales for monitoring the specific
parameters requested by the consultant
Pneumonia being a respiratory disease is usually caused from some sort of bacteria that
leads to a state of inflammation and swelling in the lung tissues. For which, it is also known as a
form of infection in the chest that ultimately makes it hard for the sufferer to take a breath. The
adult people and the children are at a higher risk of getting contagious from it and need to take
some serious action for its treatment (Coulter and Collins, 2011). However, it is on referring to
yet another fact where this disease cannot be healed completely where it is often hard for the
patient who is too old or young to recover from its atrocious consequences. Due to which, it is
also considered as a life threatening illness that must be detected on time for proper measures of
treatment.
It is on considering the present case of Mr Hunters who is 89 years old and is currently at
a critical state of health. Wherein, he is mostly affected by the existence of pneumonia which
was lastly diagnosed after acknowledging his current health condition that was more terrible and
impacted by some of his previous health concerns (Coulter, Parsons and Askham, 2008). At
present, the consultant has asked RN to carry a vigilant outlook towards the altering health
condition of Mr Hunters. This is basically to inform in case his heart rate start crossing 100 or
the saturations of oxygen that is being provisioned to him starts lowering below 90% and in case,
his body temperature goes beyond 38.5 degree Celsius.
It is thereby important to observe the parameters that are specifically requested by the
consultant where Mr Hunters is found to disfavour the intervention of the physicians and nurses
in his treatment. He is himself willing to take the control of his treatment that is a rightful
demand made by Mr Hunter where the RN on considering this fact is together aware of the
8
rate and altered sensorium. Further, nurses
can also monitor effectiveness of
antimicrobial therapy (Coker and et. al.,
2017).
QUESTION 5
In the context of a patient with pneumonia, explain the rationales for monitoring the specific
parameters requested by the consultant
Pneumonia being a respiratory disease is usually caused from some sort of bacteria that
leads to a state of inflammation and swelling in the lung tissues. For which, it is also known as a
form of infection in the chest that ultimately makes it hard for the sufferer to take a breath. The
adult people and the children are at a higher risk of getting contagious from it and need to take
some serious action for its treatment (Coulter and Collins, 2011). However, it is on referring to
yet another fact where this disease cannot be healed completely where it is often hard for the
patient who is too old or young to recover from its atrocious consequences. Due to which, it is
also considered as a life threatening illness that must be detected on time for proper measures of
treatment.
It is on considering the present case of Mr Hunters who is 89 years old and is currently at
a critical state of health. Wherein, he is mostly affected by the existence of pneumonia which
was lastly diagnosed after acknowledging his current health condition that was more terrible and
impacted by some of his previous health concerns (Coulter, Parsons and Askham, 2008). At
present, the consultant has asked RN to carry a vigilant outlook towards the altering health
condition of Mr Hunters. This is basically to inform in case his heart rate start crossing 100 or
the saturations of oxygen that is being provisioned to him starts lowering below 90% and in case,
his body temperature goes beyond 38.5 degree Celsius.
It is thereby important to observe the parameters that are specifically requested by the
consultant where Mr Hunters is found to disfavour the intervention of the physicians and nurses
in his treatment. He is himself willing to take the control of his treatment that is a rightful
demand made by Mr Hunter where the RN on considering this fact is together aware of the
8

negative outcomes that could atrociously impact his health (Priority Nursing Diagnosis and
Interventions for Pneumonia, 2015). However, this is together referred to be a matter of social
justice that involves such effective principles that in turn proves the rightful authority of Mr
Hunters to take the charge of his treatment on his own. These principles are self determination,
rights, equity, participation and access where all of these are apparent to reflect the universal
rights of all human beings in this world where it is hereby related to the fact of social justice.
Although, in the present case of Mr Hunters, allowing him to take the entire charge of
treatment on his own is a risky consideration for the hospital bodies where it is their
responsibility to take care of his wellbeing by ensuring the provision of proper treatments to him.
In context to which, the RN is hereby responsible to closely supervise the actions of Mr Hunters
once he is allowed to take charge of his treatment. Also, he must be given a proper medicinal
schedule with a strict instruction of following it (Helping people share decision making, 2012).
Whereas, the RN is together required to monitor whether he is considering the given directions to
accordingly take the medicines, etc., and should always stay nearby him in case he is need of any
other assistance. Above all, observing the specified parameters of the consultant is together
important to record any requisite changes in his health by together taking liable actions in case it
is not showing any favourable change.
QUESTION 6
(1) The strategies you would use to ensure Mr Hunters understands the implications of his
decisions
A foremost strategy that I am intending to apply over here in the case of Mr Hunters is to
follow the process of shared decision making. This will not only result in engaging the patient to
take his own decisions for the treatment but will together involve the other health care
professionals handling his case so as to take some liable decisions for his treatment with his due
consent. I will hereby refer to ascertain the main issue and clarify the same with Mr Hunters as a
way of distinguishing some potent solutions for it by together discoursing upon any other
alternatives and uncertainties that can arise. After which, proper treatment will be given to him
by assuring his perspective towards the intervention of his decisions.
9
Interventions for Pneumonia, 2015). However, this is together referred to be a matter of social
justice that involves such effective principles that in turn proves the rightful authority of Mr
Hunters to take the charge of his treatment on his own. These principles are self determination,
rights, equity, participation and access where all of these are apparent to reflect the universal
rights of all human beings in this world where it is hereby related to the fact of social justice.
Although, in the present case of Mr Hunters, allowing him to take the entire charge of
treatment on his own is a risky consideration for the hospital bodies where it is their
responsibility to take care of his wellbeing by ensuring the provision of proper treatments to him.
In context to which, the RN is hereby responsible to closely supervise the actions of Mr Hunters
once he is allowed to take charge of his treatment. Also, he must be given a proper medicinal
schedule with a strict instruction of following it (Helping people share decision making, 2012).
Whereas, the RN is together required to monitor whether he is considering the given directions to
accordingly take the medicines, etc., and should always stay nearby him in case he is need of any
other assistance. Above all, observing the specified parameters of the consultant is together
important to record any requisite changes in his health by together taking liable actions in case it
is not showing any favourable change.
QUESTION 6
(1) The strategies you would use to ensure Mr Hunters understands the implications of his
decisions
A foremost strategy that I am intending to apply over here in the case of Mr Hunters is to
follow the process of shared decision making. This will not only result in engaging the patient to
take his own decisions for the treatment but will together involve the other health care
professionals handling his case so as to take some liable decisions for his treatment with his due
consent. I will hereby refer to ascertain the main issue and clarify the same with Mr Hunters as a
way of distinguishing some potent solutions for it by together discoursing upon any other
alternatives and uncertainties that can arise. After which, proper treatment will be given to him
by assuring his perspective towards the intervention of his decisions.
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

(2) The actions you would take to manage the situation
This is in case the situation gets unmanageable, I will extend the implicated strategy of
shared decision to another level where I will attempt to explain the potential welfare, risks and
doubts of all possible alternatives. This will be done by together ensuring a collaborative
understanding among the practitioners and the patient, Mr Hunters. After which, I will together
refer to take feedback and perceive the responses in a generous way and implement the selected
treatment.
QUESTION 7
What are the two most important things that you have learned from this scenario and why? What
actions will you take in your future practice because of what you have learned from this
scenario?
The foremost thing that I have learned from the present scenario is the significance of
social justice where this involve some fundamental principles that are required to be followed by
each and every health care professional while handling a patient. Being an RN, I have hereby
learned the importance of these principles that included self-determination, access, rights, equity
and participation of a patient to get involved in the process of decision making so as to determine
the way in which, they will be treated for their wellbeing. Another important thing that I learned
from this scenario was in regard to undertake a strategic approach of shared decision making. It
is where such type of strategy will intend to involve the patient along with the practitioners
looking into the case. Such type of involvement where the patient is duly accessed to the human
rights will not only lead to a cooperative assistance to the care providers to treat the patient but
will also support them to provide effective treatment resulting in the wellbeing of the patient.
CONCLUSION
Summing up the entire research work, it can be said that health conditions of Mr Hunter
is changing frequently; therefore it is required for the registered nurse to look upon this situation.
Regarding this, nurses are also ought to consider specific medications so that Mr Hunter may not
come in contact with other health problems.
10
This is in case the situation gets unmanageable, I will extend the implicated strategy of
shared decision to another level where I will attempt to explain the potential welfare, risks and
doubts of all possible alternatives. This will be done by together ensuring a collaborative
understanding among the practitioners and the patient, Mr Hunters. After which, I will together
refer to take feedback and perceive the responses in a generous way and implement the selected
treatment.
QUESTION 7
What are the two most important things that you have learned from this scenario and why? What
actions will you take in your future practice because of what you have learned from this
scenario?
The foremost thing that I have learned from the present scenario is the significance of
social justice where this involve some fundamental principles that are required to be followed by
each and every health care professional while handling a patient. Being an RN, I have hereby
learned the importance of these principles that included self-determination, access, rights, equity
and participation of a patient to get involved in the process of decision making so as to determine
the way in which, they will be treated for their wellbeing. Another important thing that I learned
from this scenario was in regard to undertake a strategic approach of shared decision making. It
is where such type of strategy will intend to involve the patient along with the practitioners
looking into the case. Such type of involvement where the patient is duly accessed to the human
rights will not only lead to a cooperative assistance to the care providers to treat the patient but
will also support them to provide effective treatment resulting in the wellbeing of the patient.
CONCLUSION
Summing up the entire research work, it can be said that health conditions of Mr Hunter
is changing frequently; therefore it is required for the registered nurse to look upon this situation.
Regarding this, nurses are also ought to consider specific medications so that Mr Hunter may not
come in contact with other health problems.
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
REFERENCES
Coker, E. and et. al., 2017. Nurses' oral hygiene care practices with hospitalised older adults in
postacute settings. International journal of older people nursing. 12(1).
Faverio, P. and et. al., 2014. The management of community-acquired pneumonia in the elderly.
European journal of internal medicine. 25(4). pp.312-319.
Goljan, E. F., 2014. Rapid review pathology: with student consult online access. Elsevier Health
Sciences.
Heckman, G. A., Boscart, V. M. and McKelvie, R. S., 2014. Management considerations in the
care of elderly heart failure patients in long-term care facilities. Future cardiology. 10(4).
pp.563-577.
Luks, A. M., 2015. Physiology in Medicine: A physiologic approach to prevention and treatment
of acute high-altitude illnesses. Journal of Applied Physiology. 118(5). pp.509-519.
Lumb, A. B., 2016. Nunn's applied respiratory physiology. Elsevier Health Sciences.
Matsuda, S. and et. al., 2016. Prospective open-label randomized comparative, non-inferiority
study of two initial antibiotic strategies for patients with nursing-and healthcare-
associated pneumonia: Guideline-concordant therapy versus empiric therapy. Journal of
Infection and Chemotherapy. 22(6). pp.400-406.
Quinn, B. and et. al., 2014. Basic Nursing Care to Prevent Nonventilator Hospital‐Acquired
Pneumonia. Journal of Nursing Scholarship. 46(1). pp.11-19.
Rogus‐Pulia, N. and et. al., 2016. Effects of Device‐Facilitated Isometric Progressive Resistance
Oropharyngeal Therapy on Swallowing and Health‐Related Outcomes in Older Adults
with Dysphagia. Journal of the American Geriatrics Society. 64(2). pp.417-424.
Scannapieco, F. A. and Shay, K., 2014. Oral health disparities in older adults: oral bacteria,
inflammation, and aspiration pneumonia. Dental Clinics of North America. 58(4). pp.771-
782.
Söderström, L. and et. al., 2017. Malnutrition is associated with increased mortality in older
adults regardless of the cause of death. British Journal of Nutrition. 117(4). pp.532-540.
Online
11
Coker, E. and et. al., 2017. Nurses' oral hygiene care practices with hospitalised older adults in
postacute settings. International journal of older people nursing. 12(1).
Faverio, P. and et. al., 2014. The management of community-acquired pneumonia in the elderly.
European journal of internal medicine. 25(4). pp.312-319.
Goljan, E. F., 2014. Rapid review pathology: with student consult online access. Elsevier Health
Sciences.
Heckman, G. A., Boscart, V. M. and McKelvie, R. S., 2014. Management considerations in the
care of elderly heart failure patients in long-term care facilities. Future cardiology. 10(4).
pp.563-577.
Luks, A. M., 2015. Physiology in Medicine: A physiologic approach to prevention and treatment
of acute high-altitude illnesses. Journal of Applied Physiology. 118(5). pp.509-519.
Lumb, A. B., 2016. Nunn's applied respiratory physiology. Elsevier Health Sciences.
Matsuda, S. and et. al., 2016. Prospective open-label randomized comparative, non-inferiority
study of two initial antibiotic strategies for patients with nursing-and healthcare-
associated pneumonia: Guideline-concordant therapy versus empiric therapy. Journal of
Infection and Chemotherapy. 22(6). pp.400-406.
Quinn, B. and et. al., 2014. Basic Nursing Care to Prevent Nonventilator Hospital‐Acquired
Pneumonia. Journal of Nursing Scholarship. 46(1). pp.11-19.
Rogus‐Pulia, N. and et. al., 2016. Effects of Device‐Facilitated Isometric Progressive Resistance
Oropharyngeal Therapy on Swallowing and Health‐Related Outcomes in Older Adults
with Dysphagia. Journal of the American Geriatrics Society. 64(2). pp.417-424.
Scannapieco, F. A. and Shay, K., 2014. Oral health disparities in older adults: oral bacteria,
inflammation, and aspiration pneumonia. Dental Clinics of North America. 58(4). pp.771-
782.
Söderström, L. and et. al., 2017. Malnutrition is associated with increased mortality in older
adults regardless of the cause of death. British Journal of Nutrition. 117(4). pp.532-540.
Online
11
Coulter, A. and Collins, A., 2011. MAKING SHARED DECISION-MAKING A REALITY. [PDF].
Available through: <http://www.cnwl.nhs.uk/wp-content/uploads/2013/01/Making-
shared-decision-making-a-reality.pdf>. [Accessed on 25th May 2017].
Coulter, A., Parsons, S. and Askham, J., 2008. Where are the patients in decision-making about
their own care? [PDF]. Available through:
<http://www.wh
o.int/management/general/decisionmaking/WhereArePatientsinDecisionMaking.pdf>.
[Accessed on 25th May 2017].
Helping people share decision making. 2012. [PDF]. Available through:
<http://www.health.org.uk/sites/health/files/HelpingPeopleShareDecisionMaking.pdf>.
[Accessed on 25th May 2017].
Priority Nursing Diagnosis and Interventions for Pneumonia. 2015. [Online]. Available through:
<http://ncpnanda.com/priority-nursing-diagnosis-and-interventions-for-pneumonia/>.
[Accessed on 25th May 2017].
12
Available through: <http://www.cnwl.nhs.uk/wp-content/uploads/2013/01/Making-
shared-decision-making-a-reality.pdf>. [Accessed on 25th May 2017].
Coulter, A., Parsons, S. and Askham, J., 2008. Where are the patients in decision-making about
their own care? [PDF]. Available through:
<http://www.wh
o.int/management/general/decisionmaking/WhereArePatientsinDecisionMaking.pdf>.
[Accessed on 25th May 2017].
Helping people share decision making. 2012. [PDF]. Available through:
<http://www.health.org.uk/sites/health/files/HelpingPeopleShareDecisionMaking.pdf>.
[Accessed on 25th May 2017].
Priority Nursing Diagnosis and Interventions for Pneumonia. 2015. [Online]. Available through:
<http://ncpnanda.com/priority-nursing-diagnosis-and-interventions-for-pneumonia/>.
[Accessed on 25th May 2017].
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2025 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.