NSB203 Report: Strategies for Preventing Medication Errors
VerifiedAdded on 2022/11/02
|2
|1761
|284
Report
AI Summary
This report addresses the critical issue of medication errors in healthcare, examining their causes, consequences, and potential solutions. It begins by highlighting the significant ramifications of medication errors, including increased hospital stays and patient harm. The report then explores two approaches to addressing these errors: identifying individual issues and evaluating flawed system designs. It emphasizes that both individual and systemic factors contribute to errors, with systemic issues often influencing individual mistakes. The report summarizes the evidence, noting that chart reviews are a widely used monitoring intervention, though they are better at detecting adverse events than medication errors. It discusses the PICO framework for structuring clinical questions and the importance of a strong culture of safety. The report also provides recommendations for improving patient safety, including electronic health records, standardized units of measure, and pharmacist involvement. The report concludes by emphasizing the need for collaborative efforts to reduce medication errors and improve patient care outcomes, recommending strategies such as improved error reporting and system enhancements.
Background
Medication errors and medication related antagonistic occasions have
significant ramifications – from expanded length of hospitalization and
expenses to undue inconvenience and inability or expanded mortality. Reason
has proposed two ways to deal with considering mistakes and mishaps. To start
with, distinguish singular issues and insufficiencies that can prompt mistake;
second, investigate defective frameworks plan. Issues with the two people and
frameworks are in charge of generally mishaps. Nonetheless, singular issues can
likewise result from damaged frameworks. The recurrence and seriousness of
medication blunders are not uniformly conveyed in the populace, and there are
groups of patients, medications, and settings that are related with higher
dangers; nonetheless, these can by and large be ascribed to regular fundamental
contributory/idle variables
Summary of evidence
It was found that chart reviews were the most widely used monitoring and error detecting
intervention. It was also suitable to most care settings which was a reason behind its
popularity. Chart review is the most exact methodology for identifying unfriendly occasions,
yet is less great at distinguishing medication mistakes. Cases are assessed freely by at least
two specialists. Great arranging is required for definitions, incorporation criteria, and
triggers. The drawbacks of this technique are the trouble in preparing analysts and the assets
required, both financial and human. Moreover, the outcomes rely upon the nature of
documentation and commentators' capacities to catch triggers. A comprehension of the
blunders in a framework is the establishment for structure a solid culture of security. Data
from blunder announcing and underlying driver examinations of basic cases could likewise
contribute altogether to inhabitants' training. Since the focal point of most medical clinic
mistake detailing projects has been on framework wide issues as opposed to on the
individual, and they much of the time ensure secrecy, they regularly don’t note attributes of
the person who was associated with the occasion, for example, calling, control, and
preparing status.
Search strategies and critical appraisal
The point of the pursuit procedure was to discover proper and proof-based
practice systems that can be applied to general settings. Likewise, the source
should be upheld by obvious and inclination less research methods. The PICO
addresses help to build up four primary concerns including the focus on crowd,
the picked intercession for the issue, correlation of another mediation and the
result noted when the picked mediation is tried. The PICO questions
additionally help to restrict the pursuits as it sets the intended interest group
which limits the hunt. The odds of medication blunder can likewise be available
in close to home consideration settings and when unpaid consideration suppliers
are working. Nonetheless, the examination articles utilized concentrated
uniquely towards the recognition and counteractive action of mistake
medication in expert settings. Boolean administrator like "and" was additionally
used to limit the inquiry. Other than the distribution year and substance of the
articles were found were surveyed to picked five articles among the numerous
accessible.
Limitations
The greatest limitation in choosing an intervention for decreasing the
chances of medication errors depends on the nature and care settings.
Implement into practice. However, the most common limitation in the
approaches is that they are time consuming, difficult, often require
intense labour, understanding and identification skills, a lot of planning
goes on in managing the nursing professionals and dividing the duties
amidst them. and yet, only some severe elements of wrong medication
can be judged this way. This is because it cannot be ensured that the
professional in charge of reviewing the charts has all the knowledge
about the all the health cases of the patients and full information about
their diagnosis.
Preventing medication errors and improving patient safety
What is the impact of detection and
monitoring intervention for
medication errors when compared
to the direct observational
techniques among the in-house
patients of a hospital or other
healthcare organisation?
Details of critical appraisal tool
The CASP appraisal tool was used which consists of a series of questions that
determine the validity of the research. One has to answer the questions after
going through the article and fill the checklist. A detailed explanation needs to
be provided when a question has a negative answer. This ensures the validity of
the research findings present in the article. The tool aims to allow the user to
take informed decision based on the findings and information presented in the
research.
Strategies
The evidence suggests that the chances of errors can be minimised by
stabling professional leadership and cooperation among the healthcare
professionals. Most cases of medication errors occur due to the lack of
information shared among the professionals. Also, by improving their
handovers or transition of patient in different departments, the transfer
of information can also be improved. This way more professionals will
be able to access the information and be accountable for the health
decisions of the patient. The continuity of information needs to be
maintained at all times along with the quality of information that is
shared. It may not be conceivable to end the discontinuity inside and
out in healthcare settings, yet the preparation framework can
endeavour to limit its belongings by upgrading the nature of handovers
and mistake detailing, advancing patient-focused methodologies, and
improving doctor connections by encouraging correspondence through
group structures. Recommendations for these regions of the framework
are ones that the advisory group accepts merit prompt consideration
and can manage positive outcomes if successfully applied.
Recommendations
Frameworks can help decline clinic medication mistakes. A few models incorporate
electronic restorative records, institutionalized units of measure, abstaining from
confounding units of measure, weight-based dosing, and having a drug specialist accessible
to help with computing the right portion. To maintain a strategic distance from preventable
medication mistakes, audit medication and dosing before organization. Standardized tag
organization and handheld individual computerized aides increment medication organization
wellbeing . Giving constant patient data, medication profiles, lab esteems, sedate data, and
documentation decreases blunders. Electronic medication organization distinguishes off base
and precluded medications and dropped or changed medication orders. Dodging
standardized tag methods diminishes security at the purpose of consideration. Programmed
administering frameworks that make drugs accessible to patients rapidly at the purpose of
cheerful up drug specialists and attendants time to participate in other security exercises, for
example, medication compromise.
Evidence bottom line statement
Supported and cooperative endeavours to
lessen the event and seriousness of
medicinal services blunders are required
with the goal that more secure, more
excellent consideration results. To improve
security, blunder detailing methodologies
ought to incorporate recognizing mistakes,
conceding botches, revising hazardous
conditions, and revealing frameworks
upgrades to partners. The more prominent
the quantity of real blunders and close to
misses announced, the more dependable a
social insurance association or framework
could be, from a security perspective, when
frameworks enhancements are reliable with
mistake designs .
References
1. NCBI, (2009), Prevention of medication errors: detection and audit , Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2723204/
2. NCBI, (2009), System Strategies to Improve Patient Safety and Error Prevention, Retrieved from
https://www.ncbi.nlm.nih.gov/books/NBK214937/
3. Johnson A, Guirguis E, Grace Y. Preventing medication errors in transitions of care: a patient case approach. Journal of the
American Pharmacists Association. 2015 Mar 1;55(2):e264-76. Retrieved from Johnson A, Guirguis E, Grace Y. Preventing
medication errors in transitions of care: a patient case approach. Journal of the American Pharmacists Association. 2015
Mar 1;55(2):e264-76.
4. Stefanacci R, Riddle A. Preventing medication errors. Geriatric Nursing. 2016 Jul 1;37(4):307-10. Retrieved from
https://insights.ovid.com/gern/201607000/00003971-201607000-00011
5. Miladinia M, Zarea K, Baraz S, Mousavi Nouri E, Pishgooie AH, Gholamzadeh Baeis M. Pediatric nurses’ medication
error: the self-reporting of frequency, types and causes. International Journal of Pediatrics. 2016 Mar 1;4(3):1439-44.
Retrieved from http://ijp.mums.ac.ir/article_6593_c530ee6f801bcc3906cdf086ff44c9e8.pdf
6. NCBI, (2016)The Importance of Medication Errors Reporting in Improving the Quality of Clinical Care Services,
Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5016354/
7. Härkänen M, Saano S, Vehviläinen‐Julkunen K. Using incident reports to inform the prevention of medication
administration errors. Journal of clinical nursing. 2017 Nov;26(21-22):3486-99.
8. NCBI, (2017), Causes of Medication Errors in Intensive Care Units from the Perspective of Healthcare Professionals, Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632936/
9. Durham B. The nurse's role in medication safety. Nursing2019. 2015 Apr 1;45(4):1-4. Retrieved from
https://journals.lww.com/nursing/fulltext/2015/04000/The_nurse_s_role_in_medication_safety.20.aspx
10. Latimer S, Hewitt J, Stanbrough R, McAndrew R. Reducing medication errors: Teaching strategies that increase nursing students' awareness of
medication errors and their prevention. Retrieved from
https://www.researchgate.net/profile/Sharon_Latimer/publication/313740760_Reducing_medication_errors_Teaching_strategies_that_increase_nu
rsing_students%27_awareness_of_medication_errors_and_their_prevention/links/5baacb2792851ca9ed25de05/Reducing-medication-errors-
Teaching-strategies-that-increase-nursing-students-awareness-of-medication-errors-and-their-prevention.pdf
11. Kavanagh C. Medication governance: preventing errors and promoting patient safety. British Journal of Nursing. 2017 Feb 9;26(3):159-65.
Retrieved from https://www.magonlinelibrary.com/doi/abs/10.12968/bjon.2017.26.3.159
Implementation
The implementation of the above-mentioned strategies will be able to
limit the effect of the barriers and decrease the chance of medication
errors. Further steps can be taken by holding regular staff and nursing
professional meetings where they discuss the issues that prevent
smooth functioning. It is recommended to pay heed to their opinions as
they have to work in the practical setting and as a result have greater
insight into the problem. Also, the patients or care seekers can be
identified or distinguished from others who are more vulnerable and
critical. So that the chances of harm to them from wrong medication is
reduced to none. Also, by conducting periodic training for implementing
safe medication strategies and running period tests to ensure that the
strategies or interventions are used properly.
Medication errors and medication related antagonistic occasions have
significant ramifications – from expanded length of hospitalization and
expenses to undue inconvenience and inability or expanded mortality. Reason
has proposed two ways to deal with considering mistakes and mishaps. To start
with, distinguish singular issues and insufficiencies that can prompt mistake;
second, investigate defective frameworks plan. Issues with the two people and
frameworks are in charge of generally mishaps. Nonetheless, singular issues can
likewise result from damaged frameworks. The recurrence and seriousness of
medication blunders are not uniformly conveyed in the populace, and there are
groups of patients, medications, and settings that are related with higher
dangers; nonetheless, these can by and large be ascribed to regular fundamental
contributory/idle variables
Summary of evidence
It was found that chart reviews were the most widely used monitoring and error detecting
intervention. It was also suitable to most care settings which was a reason behind its
popularity. Chart review is the most exact methodology for identifying unfriendly occasions,
yet is less great at distinguishing medication mistakes. Cases are assessed freely by at least
two specialists. Great arranging is required for definitions, incorporation criteria, and
triggers. The drawbacks of this technique are the trouble in preparing analysts and the assets
required, both financial and human. Moreover, the outcomes rely upon the nature of
documentation and commentators' capacities to catch triggers. A comprehension of the
blunders in a framework is the establishment for structure a solid culture of security. Data
from blunder announcing and underlying driver examinations of basic cases could likewise
contribute altogether to inhabitants' training. Since the focal point of most medical clinic
mistake detailing projects has been on framework wide issues as opposed to on the
individual, and they much of the time ensure secrecy, they regularly don’t note attributes of
the person who was associated with the occasion, for example, calling, control, and
preparing status.
Search strategies and critical appraisal
The point of the pursuit procedure was to discover proper and proof-based
practice systems that can be applied to general settings. Likewise, the source
should be upheld by obvious and inclination less research methods. The PICO
addresses help to build up four primary concerns including the focus on crowd,
the picked intercession for the issue, correlation of another mediation and the
result noted when the picked mediation is tried. The PICO questions
additionally help to restrict the pursuits as it sets the intended interest group
which limits the hunt. The odds of medication blunder can likewise be available
in close to home consideration settings and when unpaid consideration suppliers
are working. Nonetheless, the examination articles utilized concentrated
uniquely towards the recognition and counteractive action of mistake
medication in expert settings. Boolean administrator like "and" was additionally
used to limit the inquiry. Other than the distribution year and substance of the
articles were found were surveyed to picked five articles among the numerous
accessible.
Limitations
The greatest limitation in choosing an intervention for decreasing the
chances of medication errors depends on the nature and care settings.
Implement into practice. However, the most common limitation in the
approaches is that they are time consuming, difficult, often require
intense labour, understanding and identification skills, a lot of planning
goes on in managing the nursing professionals and dividing the duties
amidst them. and yet, only some severe elements of wrong medication
can be judged this way. This is because it cannot be ensured that the
professional in charge of reviewing the charts has all the knowledge
about the all the health cases of the patients and full information about
their diagnosis.
Preventing medication errors and improving patient safety
What is the impact of detection and
monitoring intervention for
medication errors when compared
to the direct observational
techniques among the in-house
patients of a hospital or other
healthcare organisation?
Details of critical appraisal tool
The CASP appraisal tool was used which consists of a series of questions that
determine the validity of the research. One has to answer the questions after
going through the article and fill the checklist. A detailed explanation needs to
be provided when a question has a negative answer. This ensures the validity of
the research findings present in the article. The tool aims to allow the user to
take informed decision based on the findings and information presented in the
research.
Strategies
The evidence suggests that the chances of errors can be minimised by
stabling professional leadership and cooperation among the healthcare
professionals. Most cases of medication errors occur due to the lack of
information shared among the professionals. Also, by improving their
handovers or transition of patient in different departments, the transfer
of information can also be improved. This way more professionals will
be able to access the information and be accountable for the health
decisions of the patient. The continuity of information needs to be
maintained at all times along with the quality of information that is
shared. It may not be conceivable to end the discontinuity inside and
out in healthcare settings, yet the preparation framework can
endeavour to limit its belongings by upgrading the nature of handovers
and mistake detailing, advancing patient-focused methodologies, and
improving doctor connections by encouraging correspondence through
group structures. Recommendations for these regions of the framework
are ones that the advisory group accepts merit prompt consideration
and can manage positive outcomes if successfully applied.
Recommendations
Frameworks can help decline clinic medication mistakes. A few models incorporate
electronic restorative records, institutionalized units of measure, abstaining from
confounding units of measure, weight-based dosing, and having a drug specialist accessible
to help with computing the right portion. To maintain a strategic distance from preventable
medication mistakes, audit medication and dosing before organization. Standardized tag
organization and handheld individual computerized aides increment medication organization
wellbeing . Giving constant patient data, medication profiles, lab esteems, sedate data, and
documentation decreases blunders. Electronic medication organization distinguishes off base
and precluded medications and dropped or changed medication orders. Dodging
standardized tag methods diminishes security at the purpose of consideration. Programmed
administering frameworks that make drugs accessible to patients rapidly at the purpose of
cheerful up drug specialists and attendants time to participate in other security exercises, for
example, medication compromise.
Evidence bottom line statement
Supported and cooperative endeavours to
lessen the event and seriousness of
medicinal services blunders are required
with the goal that more secure, more
excellent consideration results. To improve
security, blunder detailing methodologies
ought to incorporate recognizing mistakes,
conceding botches, revising hazardous
conditions, and revealing frameworks
upgrades to partners. The more prominent
the quantity of real blunders and close to
misses announced, the more dependable a
social insurance association or framework
could be, from a security perspective, when
frameworks enhancements are reliable with
mistake designs .
References
1. NCBI, (2009), Prevention of medication errors: detection and audit , Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2723204/
2. NCBI, (2009), System Strategies to Improve Patient Safety and Error Prevention, Retrieved from
https://www.ncbi.nlm.nih.gov/books/NBK214937/
3. Johnson A, Guirguis E, Grace Y. Preventing medication errors in transitions of care: a patient case approach. Journal of the
American Pharmacists Association. 2015 Mar 1;55(2):e264-76. Retrieved from Johnson A, Guirguis E, Grace Y. Preventing
medication errors in transitions of care: a patient case approach. Journal of the American Pharmacists Association. 2015
Mar 1;55(2):e264-76.
4. Stefanacci R, Riddle A. Preventing medication errors. Geriatric Nursing. 2016 Jul 1;37(4):307-10. Retrieved from
https://insights.ovid.com/gern/201607000/00003971-201607000-00011
5. Miladinia M, Zarea K, Baraz S, Mousavi Nouri E, Pishgooie AH, Gholamzadeh Baeis M. Pediatric nurses’ medication
error: the self-reporting of frequency, types and causes. International Journal of Pediatrics. 2016 Mar 1;4(3):1439-44.
Retrieved from http://ijp.mums.ac.ir/article_6593_c530ee6f801bcc3906cdf086ff44c9e8.pdf
6. NCBI, (2016)The Importance of Medication Errors Reporting in Improving the Quality of Clinical Care Services,
Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5016354/
7. Härkänen M, Saano S, Vehviläinen‐Julkunen K. Using incident reports to inform the prevention of medication
administration errors. Journal of clinical nursing. 2017 Nov;26(21-22):3486-99.
8. NCBI, (2017), Causes of Medication Errors in Intensive Care Units from the Perspective of Healthcare Professionals, Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632936/
9. Durham B. The nurse's role in medication safety. Nursing2019. 2015 Apr 1;45(4):1-4. Retrieved from
https://journals.lww.com/nursing/fulltext/2015/04000/The_nurse_s_role_in_medication_safety.20.aspx
10. Latimer S, Hewitt J, Stanbrough R, McAndrew R. Reducing medication errors: Teaching strategies that increase nursing students' awareness of
medication errors and their prevention. Retrieved from
https://www.researchgate.net/profile/Sharon_Latimer/publication/313740760_Reducing_medication_errors_Teaching_strategies_that_increase_nu
rsing_students%27_awareness_of_medication_errors_and_their_prevention/links/5baacb2792851ca9ed25de05/Reducing-medication-errors-
Teaching-strategies-that-increase-nursing-students-awareness-of-medication-errors-and-their-prevention.pdf
11. Kavanagh C. Medication governance: preventing errors and promoting patient safety. British Journal of Nursing. 2017 Feb 9;26(3):159-65.
Retrieved from https://www.magonlinelibrary.com/doi/abs/10.12968/bjon.2017.26.3.159
Implementation
The implementation of the above-mentioned strategies will be able to
limit the effect of the barriers and decrease the chance of medication
errors. Further steps can be taken by holding regular staff and nursing
professional meetings where they discuss the issues that prevent
smooth functioning. It is recommended to pay heed to their opinions as
they have to work in the practical setting and as a result have greater
insight into the problem. Also, the patients or care seekers can be
identified or distinguished from others who are more vulnerable and
critical. So that the chances of harm to them from wrong medication is
reduced to none. Also, by conducting periodic training for implementing
safe medication strategies and running period tests to ensure that the
strategies or interventions are used properly.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
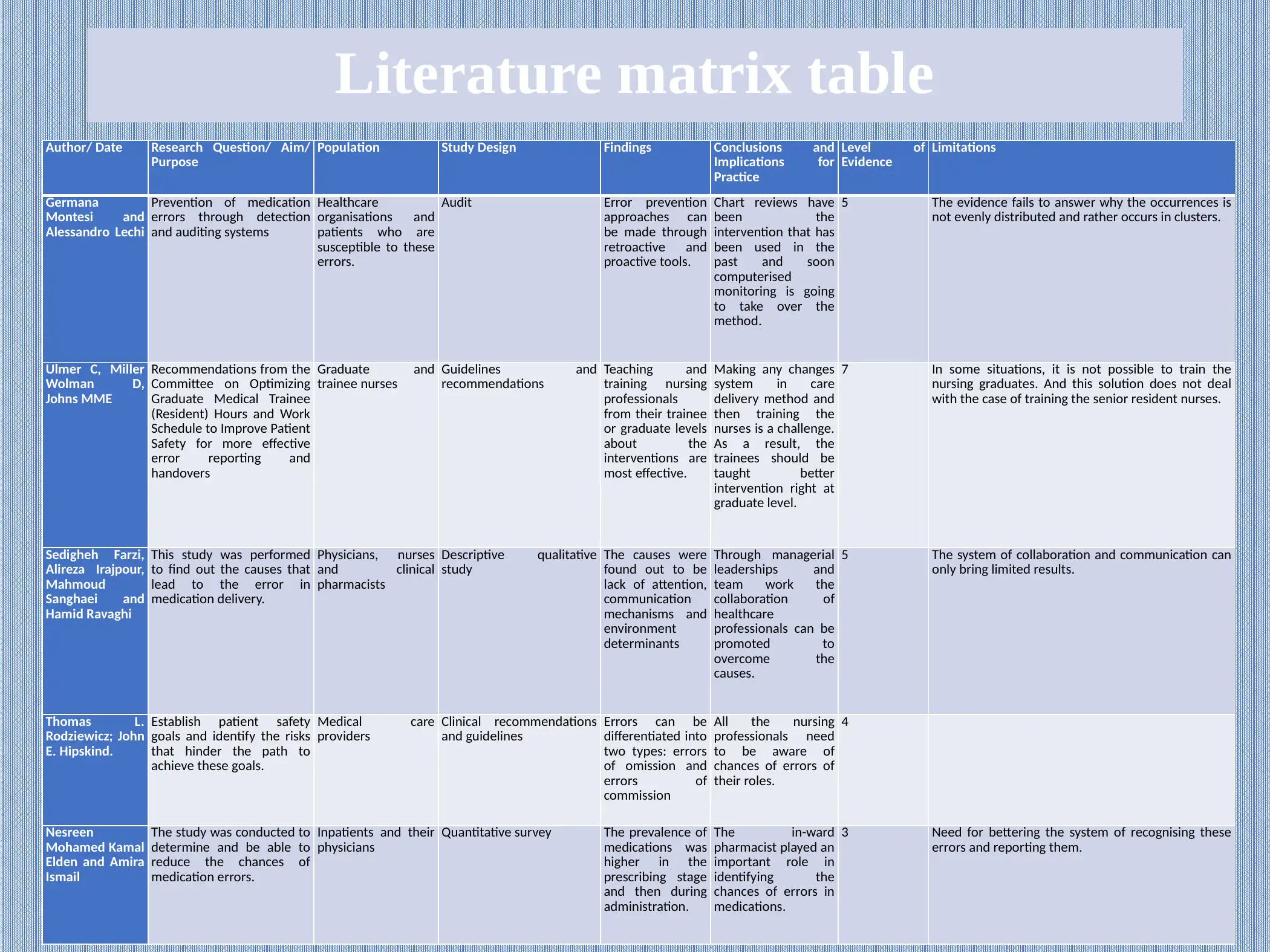
Literature matrix table
Author/ Date Research Question/ Aim/
Purpose
Population Study Design Findings Conclusions and
Implications for
Practice
Level of
Evidence
Limitations
Germana
Montesi and
Alessandro Lechi
Prevention of medication
errors through detection
and auditing systems
Healthcare
organisations and
patients who are
susceptible to these
errors.
Audit Error prevention
approaches can
be made through
retroactive and
proactive tools.
Chart reviews have
been the
intervention that has
been used in the
past and soon
computerised
monitoring is going
to take over the
method.
5 The evidence fails to answer why the occurrences is
not evenly distributed and rather occurs in clusters.
Ulmer C, Miller
Wolman D,
Johns MME
Recommendations from the
Committee on Optimizing
Graduate Medical Trainee
(Resident) Hours and Work
Schedule to Improve Patient
Safety for more effective
error reporting and
handovers
Graduate and
trainee nurses
Guidelines and
recommendations
Teaching and
training nursing
professionals
from their trainee
or graduate levels
about the
interventions are
most effective.
Making any changes
system in care
delivery method and
then training the
nurses is a challenge.
As a result, the
trainees should be
taught better
intervention right at
graduate level.
7 In some situations, it is not possible to train the
nursing graduates. And this solution does not deal
with the case of training the senior resident nurses.
Sedigheh Farzi,
Alireza Irajpour,
Mahmoud
Sanghaei and
Hamid Ravaghi
This study was performed
to find out the causes that
lead to the error in
medication delivery.
Physicians, nurses
and clinical
pharmacists
Descriptive qualitative
study
The causes were
found out to be
lack of attention,
communication
mechanisms and
environment
determinants
Through managerial
leaderships and
team work the
collaboration of
healthcare
professionals can be
promoted to
overcome the
causes.
5 The system of collaboration and communication can
only bring limited results.
Thomas L.
Rodziewicz; John
E. Hipskind.
Establish patient safety
goals and identify the risks
that hinder the path to
achieve these goals.
Medical care
providers
Clinical recommendations
and guidelines
Errors can be
differentiated into
two types: errors
of omission and
errors of
commission
All the nursing
professionals need
to be aware of
chances of errors of
their roles.
4
Nesreen
Mohamed Kamal
Elden and Amira
Ismail
The study was conducted to
determine and be able to
reduce the chances of
medication errors.
Inpatients and their
physicians
Quantitative survey The prevalence of
medications was
higher in the
prescribing stage
and then during
administration.
The in-ward
pharmacist played an
important role in
identifying the
chances of errors in
medications.
3 Need for bettering the system of recognising these
errors and reporting them.
Author/ Date Research Question/ Aim/
Purpose
Population Study Design Findings Conclusions and
Implications for
Practice
Level of
Evidence
Limitations
Germana
Montesi and
Alessandro Lechi
Prevention of medication
errors through detection
and auditing systems
Healthcare
organisations and
patients who are
susceptible to these
errors.
Audit Error prevention
approaches can
be made through
retroactive and
proactive tools.
Chart reviews have
been the
intervention that has
been used in the
past and soon
computerised
monitoring is going
to take over the
method.
5 The evidence fails to answer why the occurrences is
not evenly distributed and rather occurs in clusters.
Ulmer C, Miller
Wolman D,
Johns MME
Recommendations from the
Committee on Optimizing
Graduate Medical Trainee
(Resident) Hours and Work
Schedule to Improve Patient
Safety for more effective
error reporting and
handovers
Graduate and
trainee nurses
Guidelines and
recommendations
Teaching and
training nursing
professionals
from their trainee
or graduate levels
about the
interventions are
most effective.
Making any changes
system in care
delivery method and
then training the
nurses is a challenge.
As a result, the
trainees should be
taught better
intervention right at
graduate level.
7 In some situations, it is not possible to train the
nursing graduates. And this solution does not deal
with the case of training the senior resident nurses.
Sedigheh Farzi,
Alireza Irajpour,
Mahmoud
Sanghaei and
Hamid Ravaghi
This study was performed
to find out the causes that
lead to the error in
medication delivery.
Physicians, nurses
and clinical
pharmacists
Descriptive qualitative
study
The causes were
found out to be
lack of attention,
communication
mechanisms and
environment
determinants
Through managerial
leaderships and
team work the
collaboration of
healthcare
professionals can be
promoted to
overcome the
causes.
5 The system of collaboration and communication can
only bring limited results.
Thomas L.
Rodziewicz; John
E. Hipskind.
Establish patient safety
goals and identify the risks
that hinder the path to
achieve these goals.
Medical care
providers
Clinical recommendations
and guidelines
Errors can be
differentiated into
two types: errors
of omission and
errors of
commission
All the nursing
professionals need
to be aware of
chances of errors of
their roles.
4
Nesreen
Mohamed Kamal
Elden and Amira
Ismail
The study was conducted to
determine and be able to
reduce the chances of
medication errors.
Inpatients and their
physicians
Quantitative survey The prevalence of
medications was
higher in the
prescribing stage
and then during
administration.
The in-ward
pharmacist played an
important role in
identifying the
chances of errors in
medications.
3 Need for bettering the system of recognising these
errors and reporting them.
1 out of 2
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.