Psychological Assessment: DASS-21 Validation in North Queensland
VerifiedAdded on 2023/01/17
|19
|4894
|57
Report
AI Summary
This report presents a psychometric validation study of the DASS-21 questionnaire, a self-report measure of depression, anxiety, and stress, within the North Queensland population. The study aimed to assess the reliability, convergent and discriminant validity, and factor structure of the DASS-21. Participants (n=170) completed the DASS-21, the MHC-SF (a measure of well-being), and the BASIS-24 (a measure of mental illness). The results indicated high internal consistency for the DASS-21 subscales and overall scale. Convergent validity was established through positive correlations with the BASIS-24, while discriminant validity was demonstrated through negative correlations with the MHC-SF. Factor analysis confirmed the expected three-factor structure of the DASS-21. These findings support the use of the DASS-21 as a reliable and valid tool for assessing psychological distress in the North Queensland region. The study contributes to the understanding of mental health assessment in the region and provides a basis for future research and clinical applications.

Psychological Assessment – A North Queensland Case Study
By (Name of Student)
(Institutional Affiliation)
(Date of Submission)
By (Name of Student)
(Institutional Affiliation)
(Date of Submission)
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Psychometric Validation of DASS21 in North-Queensland
Introduction
DASS-21 is a 21-item self-report questionnaire that contains a three Seven -item scale that
measures depression, stress and the anxiety (Henry & Crawford, 2005). This scale has not yet
been validated for North Queensland population despite the fact that DASS-21 was found to
have sufficient psychometric features (Antony, Bieling, Cox, Enns & Swinson, 1998). This
work thus aims to validate DASS, its internal consistency, convergent and discriminant
validity and factor structure for North Queensland population. This study established a strong
positive correlation and convergent validity with BASIS-24, a mental illness measure. Also,
DASS-21 established discriminant validity with MHC-SF, a measure of positive well-being.
Introduction
DASS-21 is a 21-item self-report questionnaire that contains a three Seven -item scale that
measures depression, stress and the anxiety (Henry & Crawford, 2005). This scale has not yet
been validated for North Queensland population despite the fact that DASS-21 was found to
have sufficient psychometric features (Antony, Bieling, Cox, Enns & Swinson, 1998). This
work thus aims to validate DASS, its internal consistency, convergent and discriminant
validity and factor structure for North Queensland population. This study established a strong
positive correlation and convergent validity with BASIS-24, a mental illness measure. Also,
DASS-21 established discriminant validity with MHC-SF, a measure of positive well-being.
Depression can be defined as a mood disorder bounded as a determined state of low
mood and anhedonia (Tully, 2009). According to Clark & Watson (1991), a positive effect is
either low or absent when experiencing depression and thus those people experience loss of
self-esteem, a sense of hopelessness and dysphonia.
Anxiety on the other hand is defined as a state of autonomic arousal and fearfulness
that is out of bound and proportion. Stress is well-defined by persistent muscle tension,
irritability, and a low threshold for becoming upset or frustrated (5th ed.; DSM–5; APA,
2013). It is associated to the negative effects as observed in generalized anxiety disorders
(Clark & Watson, 1991).
According to Kaspe (2005), anxiety and depression are believed to be the two primary
roots of mental illness disorders, and often co-occur, which led to explain the common
features of anxiety and depression. Many developed nations such United States and Australia,
face the problem of increasing mental illnesses such as depression and anxiety (Edmunds,
2018). Accordingly, the Australia’s estimated annual expenditure on curing mental illness has
now risen to a whopping twenty billion (National Mental Health report, 2013). Clark and
Watson (1991) thus asserted that anxiety and depression can be notable by unique
characteristics and proposed a tripartite framework of anxiety and depression that consist of
positive affect, physiological hyper arousal, and general distress. This is in conformity with
three psychometrically distinct factors namely depression, anxiety and stress which are also
primary constructs of the Depression Anxiety Stress Scale (DASS) (Brown, Chorpita,
Korotitsch & Barlow, 1997).
DASS-42 was developed as a screening tool for depression and anxiety disorders.
Psychometric validation has provided strong support for the scale’s internal consistency and
its convergent and discriminant validity with other existing measures like Beck Depression
and Anxiety Inventories in clinical and non-clinical samples (Lovibond & Lovibond, 1995).
mood and anhedonia (Tully, 2009). According to Clark & Watson (1991), a positive effect is
either low or absent when experiencing depression and thus those people experience loss of
self-esteem, a sense of hopelessness and dysphonia.
Anxiety on the other hand is defined as a state of autonomic arousal and fearfulness
that is out of bound and proportion. Stress is well-defined by persistent muscle tension,
irritability, and a low threshold for becoming upset or frustrated (5th ed.; DSM–5; APA,
2013). It is associated to the negative effects as observed in generalized anxiety disorders
(Clark & Watson, 1991).
According to Kaspe (2005), anxiety and depression are believed to be the two primary
roots of mental illness disorders, and often co-occur, which led to explain the common
features of anxiety and depression. Many developed nations such United States and Australia,
face the problem of increasing mental illnesses such as depression and anxiety (Edmunds,
2018). Accordingly, the Australia’s estimated annual expenditure on curing mental illness has
now risen to a whopping twenty billion (National Mental Health report, 2013). Clark and
Watson (1991) thus asserted that anxiety and depression can be notable by unique
characteristics and proposed a tripartite framework of anxiety and depression that consist of
positive affect, physiological hyper arousal, and general distress. This is in conformity with
three psychometrically distinct factors namely depression, anxiety and stress which are also
primary constructs of the Depression Anxiety Stress Scale (DASS) (Brown, Chorpita,
Korotitsch & Barlow, 1997).
DASS-42 was developed as a screening tool for depression and anxiety disorders.
Psychometric validation has provided strong support for the scale’s internal consistency and
its convergent and discriminant validity with other existing measures like Beck Depression
and Anxiety Inventories in clinical and non-clinical samples (Lovibond & Lovibond, 1995).
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Exploratory and confirmatory factor analyses of DASS-42 items have consistently
reproduced the three-factor structure in large nonclinical samples (Antony, Bieling, Cox,
Enns & Swinson, 1998). DASS-21, a shortened version of DASS-42, has fewer items, which
revealed cleaner factor structure and produced smaller inter-factor correlations, and was
subsequently adopted by numerous studies. DASS-21 has also been found to have strong
internal consistency (Henry & Crawford, 2005), convergent validity (Le et al., 2017) and
discriminant validity (Osman et al., 2012). Conducted factor analysis investigation revealed
that DASS-21 components were explicitly clustered into three sub-scales which measure
depression, anxiety and stress. The Depression scale measures symptoms associated with
worthlessness or sadness. The Anxiety scale included symptoms of fear, panic attacks, and
physical arousal. The Stress scales included symptoms such as irritability, overreaction, and
tension (Henry, & Crawford, 2005). DASS-21 has been verified across a multitude of
populations and proven useful (Azma,
Rusli, Quek, & Noah, 2014; Tran, Tran & Fisher, 2013; Teo et al., 2018).
Demographically, DASS-21 has also proven its validity through several Australian studies on
various groups to analyze the severity of depression, anxiety and stress. More recent
Australian studies include outpatient chemotherapy patients from Western Australia hospitals
(McMullen et al., 2017), patients undergoing traumatic brain injury rehabilitation from New
South Wales hospitals (Randall, Thomas, Whiting & McGrath, 2017), registered nurses
(Hegney et al., 2014), Australian mothers (Lovell, Huntsman & Hedley-Ward, 2015) as well
as younger and older adolescents (Tully, Zajac & Venning, 2009; Shaw, Campbell, Runions
& Zubrick, 2017).
Currently it is deemed that there is lack of validation in the North Queensland
population. Given the potential usefulness for research and clinical screening in North
Queensland, it is important to further examine the psychometric properties of the DASS-21
reproduced the three-factor structure in large nonclinical samples (Antony, Bieling, Cox,
Enns & Swinson, 1998). DASS-21, a shortened version of DASS-42, has fewer items, which
revealed cleaner factor structure and produced smaller inter-factor correlations, and was
subsequently adopted by numerous studies. DASS-21 has also been found to have strong
internal consistency (Henry & Crawford, 2005), convergent validity (Le et al., 2017) and
discriminant validity (Osman et al., 2012). Conducted factor analysis investigation revealed
that DASS-21 components were explicitly clustered into three sub-scales which measure
depression, anxiety and stress. The Depression scale measures symptoms associated with
worthlessness or sadness. The Anxiety scale included symptoms of fear, panic attacks, and
physical arousal. The Stress scales included symptoms such as irritability, overreaction, and
tension (Henry, & Crawford, 2005). DASS-21 has been verified across a multitude of
populations and proven useful (Azma,
Rusli, Quek, & Noah, 2014; Tran, Tran & Fisher, 2013; Teo et al., 2018).
Demographically, DASS-21 has also proven its validity through several Australian studies on
various groups to analyze the severity of depression, anxiety and stress. More recent
Australian studies include outpatient chemotherapy patients from Western Australia hospitals
(McMullen et al., 2017), patients undergoing traumatic brain injury rehabilitation from New
South Wales hospitals (Randall, Thomas, Whiting & McGrath, 2017), registered nurses
(Hegney et al., 2014), Australian mothers (Lovell, Huntsman & Hedley-Ward, 2015) as well
as younger and older adolescents (Tully, Zajac & Venning, 2009; Shaw, Campbell, Runions
& Zubrick, 2017).
Currently it is deemed that there is lack of validation in the North Queensland
population. Given the potential usefulness for research and clinical screening in North
Queensland, it is important to further examine the psychometric properties of the DASS-21
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

and its applicability in that context. To that end, DASS-21 was equated with other scales
namely MHC-SF and BASIS-24.
The four hypotheses in this study were;
H1: DASS-21 exhibits reliability
H2: There exists convergent validity with BASIS-24
H3: There exist divergent validity with MHC-SF
H4: There exist a three pure factor structure of DASS-21.
Methods
Participants
Participants (n= 171) aged 18–62 (M= 31.09, SD= 11.27), having 75.4% of female
(n= 129) respondents took part in the questionnaire. Participants were mostly native to
Australia (n=149) and mostly employed (n=110). Their education level varies in nature.
Table 1 indicates participants’ ethnicities.
Table 1: Ethnicity of Participants
Australian Aboriginal or
Torres Strait
Islander
Another
cultural group
Total
Number 149 3 19 171
Percentage 87.1 1.8 11.1 100
Table 2 indicates participants’ current employment status. One of the participant’s data was
missing.
Table 2 Current employments Status of Participants
namely MHC-SF and BASIS-24.
The four hypotheses in this study were;
H1: DASS-21 exhibits reliability
H2: There exists convergent validity with BASIS-24
H3: There exist divergent validity with MHC-SF
H4: There exist a three pure factor structure of DASS-21.
Methods
Participants
Participants (n= 171) aged 18–62 (M= 31.09, SD= 11.27), having 75.4% of female
(n= 129) respondents took part in the questionnaire. Participants were mostly native to
Australia (n=149) and mostly employed (n=110). Their education level varies in nature.
Table 1 indicates participants’ ethnicities.
Table 1: Ethnicity of Participants
Australian Aboriginal or
Torres Strait
Islander
Another
cultural group
Total
Number 149 3 19 171
Percentage 87.1 1.8 11.1 100
Table 2 indicates participants’ current employment status. One of the participant’s data was
missing.
Table 2 Current employments Status of Participants
Employed
Unemployed
Student Pensioner Retired
None of the Above
Number 110
14
39 5 1 1
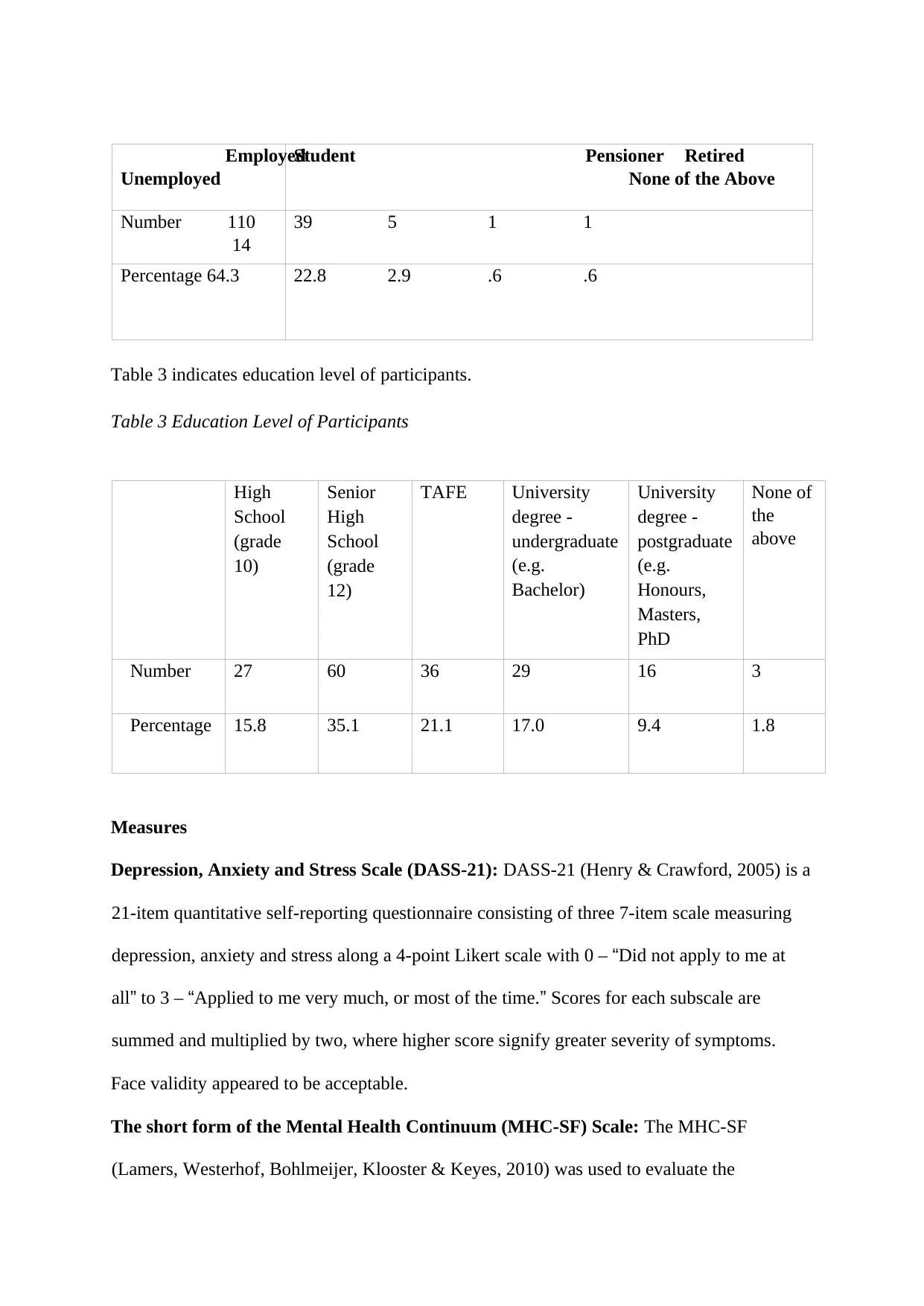
Percentage 64.3 22.8 2.9 .6 .6
Table 3 indicates education level of participants.
Table 3 Education Level of Participants
High
School
(grade
10)
Senior
High
School
(grade
12)
TAFE University
degree -
undergraduate
(e.g.
Bachelor)
University
degree -
postgraduate
(e.g.
Honours,
Masters,
PhD
None of
the
above
Number 27 60 36 29 16 3
Percentage 15.8 35.1 21.1 17.0 9.4 1.8
Measures
Depression, Anxiety and Stress Scale (DASS-21): DASS-21 (Henry & Crawford, 2005) is a
21-item quantitative self-reporting questionnaire consisting of three 7-item scale measuring
depression, anxiety and stress along a 4-point Likert scale with 0 – “Did not apply to me at
all” to 3 – “Applied to me very much, or most of the time.” Scores for each subscale are
summed and multiplied by two, where higher score signify greater severity of symptoms.
Face validity appeared to be acceptable.
The short form of the Mental Health Continuum (MHC-SF) Scale: The MHC-SF
(Lamers, Westerhof, Bohlmeijer, Klooster & Keyes, 2010) was used to evaluate the
Unemployed
Student Pensioner Retired
None of the Above
Number 110
14
39 5 1 1
Percentage 64.3 22.8 2.9 .6 .6
Table 3 indicates education level of participants.
Table 3 Education Level of Participants
High
School
(grade
10)
Senior
High
School
(grade
12)
TAFE University
degree -
undergraduate
(e.g.
Bachelor)
University
degree -
postgraduate
(e.g.
Honours,
Masters,
PhD
None of
the
above
Number 27 60 36 29 16 3
Percentage 15.8 35.1 21.1 17.0 9.4 1.8
Measures
Depression, Anxiety and Stress Scale (DASS-21): DASS-21 (Henry & Crawford, 2005) is a
21-item quantitative self-reporting questionnaire consisting of three 7-item scale measuring
depression, anxiety and stress along a 4-point Likert scale with 0 – “Did not apply to me at
all” to 3 – “Applied to me very much, or most of the time.” Scores for each subscale are
summed and multiplied by two, where higher score signify greater severity of symptoms.
Face validity appeared to be acceptable.
The short form of the Mental Health Continuum (MHC-SF) Scale: The MHC-SF
(Lamers, Westerhof, Bohlmeijer, Klooster & Keyes, 2010) was used to evaluate the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
discriminant validity of the DASS-21. It is a 14-item quantitative self-report questionnaire
measuring mental health and well-being comprising of three measures on emotional
wellbeing (EWB), six on psychological well-being (PWB), and five on social well-being
(SWB), rating the frequency in the past month along a 6-point Likert scale ranging from 0 –
‘‘never’’ to 5 – ‘‘every-day.’’ Items in each dimension were summed. Higher ratings indicated
higher levels of well-being. MHC-SF exhibited high internal consistency with an overall
Cronbach’s alpha of above .74 for both the subscale and total scale of well-being, therefore
the scale is reliable.
Further, moderate test-retest reliability suggests that the MHC-SF is both sensitive and
stable to changes over time. Convergent validity was established with respect to wellbeing
and functioning. Discriminant validity was reported whereby mental illness was negatively
and moderately correlated to positive mental health in the MHC-SF.
The Behaviour and Symptom Identification Scale (BASIS-24): BASIS-24 was used to
evaluate the convergent validity of the DASS-21 (Cameron et al, 2007). It is a 24-item self-
reporting questionnaire measuring six subscales namely psychiatric, substance abuse and
functioning such as depression, relationships, self-harm, emotional ability, psychosis, and
substance abuse, rated along a 5-point Likert scale with scores ranging from 0 – “no
difficulty/symptoms never present” to 4 –“extreme difficulty/symptoms always present”. Six
items require reverse scoring and a mean score is calculated for each subscale and also for the
total scale. Higher scores represent greater severity of the symptoms and problems.
Psychometric properties of BASIS-24 suggest high internal consistency with a Cronbach’s
Alpha of .75 to .91.
A change of .56 had also been reported suggesting the scale being responsive to
change indicating an effect size. Therefore, concurrent criterion validity was established.
measuring mental health and well-being comprising of three measures on emotional
wellbeing (EWB), six on psychological well-being (PWB), and five on social well-being
(SWB), rating the frequency in the past month along a 6-point Likert scale ranging from 0 –
‘‘never’’ to 5 – ‘‘every-day.’’ Items in each dimension were summed. Higher ratings indicated
higher levels of well-being. MHC-SF exhibited high internal consistency with an overall
Cronbach’s alpha of above .74 for both the subscale and total scale of well-being, therefore
the scale is reliable.
Further, moderate test-retest reliability suggests that the MHC-SF is both sensitive and
stable to changes over time. Convergent validity was established with respect to wellbeing
and functioning. Discriminant validity was reported whereby mental illness was negatively
and moderately correlated to positive mental health in the MHC-SF.
The Behaviour and Symptom Identification Scale (BASIS-24): BASIS-24 was used to
evaluate the convergent validity of the DASS-21 (Cameron et al, 2007). It is a 24-item self-
reporting questionnaire measuring six subscales namely psychiatric, substance abuse and
functioning such as depression, relationships, self-harm, emotional ability, psychosis, and
substance abuse, rated along a 5-point Likert scale with scores ranging from 0 – “no
difficulty/symptoms never present” to 4 –“extreme difficulty/symptoms always present”. Six
items require reverse scoring and a mean score is calculated for each subscale and also for the
total scale. Higher scores represent greater severity of the symptoms and problems.
Psychometric properties of BASIS-24 suggest high internal consistency with a Cronbach’s
Alpha of .75 to .91.
A change of .56 had also been reported suggesting the scale being responsive to
change indicating an effect size. Therefore, concurrent criterion validity was established.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
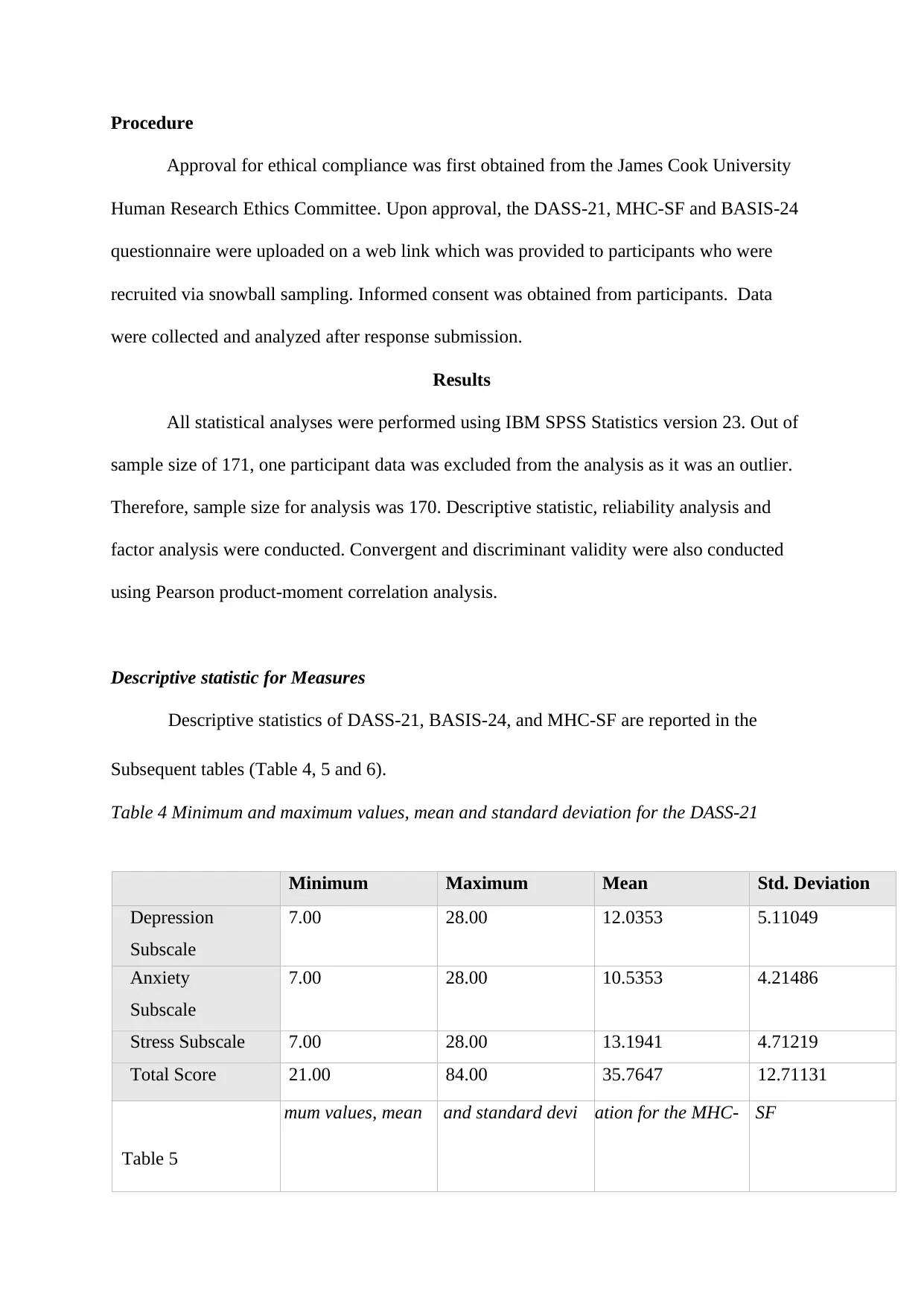
Procedure
Approval for ethical compliance was first obtained from the James Cook University
Human Research Ethics Committee. Upon approval, the DASS-21, MHC-SF and BASIS-24
questionnaire were uploaded on a web link which was provided to participants who were
recruited via snowball sampling. Informed consent was obtained from participants. Data
were collected and analyzed after response submission.
Results
All statistical analyses were performed using IBM SPSS Statistics version 23. Out of
sample size of 171, one participant data was excluded from the analysis as it was an outlier.
Therefore, sample size for analysis was 170. Descriptive statistic, reliability analysis and
factor analysis were conducted. Convergent and discriminant validity were also conducted
using Pearson product-moment correlation analysis.
Descriptive statistic for Measures
Descriptive statistics of DASS-21, BASIS-24, and MHC-SF are reported in the
Subsequent tables (Table 4, 5 and 6).
Table 4 Minimum and maximum values, mean and standard deviation for the DASS-21
Minimum Maximum Mean Std. Deviation
Depression
Subscale
7.00 28.00 12.0353 5.11049
Anxiety
Subscale
7.00 28.00 10.5353 4.21486
Stress Subscale 7.00 28.00 13.1941 4.71219
Total Score 21.00 84.00 35.7647 12.71131
Table 5
mum values, mean and standard devi ation for the MHC- SF
Approval for ethical compliance was first obtained from the James Cook University
Human Research Ethics Committee. Upon approval, the DASS-21, MHC-SF and BASIS-24
questionnaire were uploaded on a web link which was provided to participants who were
recruited via snowball sampling. Informed consent was obtained from participants. Data
were collected and analyzed after response submission.
Results
All statistical analyses were performed using IBM SPSS Statistics version 23. Out of
sample size of 171, one participant data was excluded from the analysis as it was an outlier.
Therefore, sample size for analysis was 170. Descriptive statistic, reliability analysis and
factor analysis were conducted. Convergent and discriminant validity were also conducted
using Pearson product-moment correlation analysis.
Descriptive statistic for Measures
Descriptive statistics of DASS-21, BASIS-24, and MHC-SF are reported in the
Subsequent tables (Table 4, 5 and 6).
Table 4 Minimum and maximum values, mean and standard deviation for the DASS-21
Minimum Maximum Mean Std. Deviation
Depression
Subscale
7.00 28.00 12.0353 5.11049
Anxiety
Subscale
7.00 28.00 10.5353 4.21486
Stress Subscale 7.00 28.00 13.1941 4.71219
Total Score 21.00 84.00 35.7647 12.71131
Table 5
mum values, mean and standard devi ation for the MHC- SF
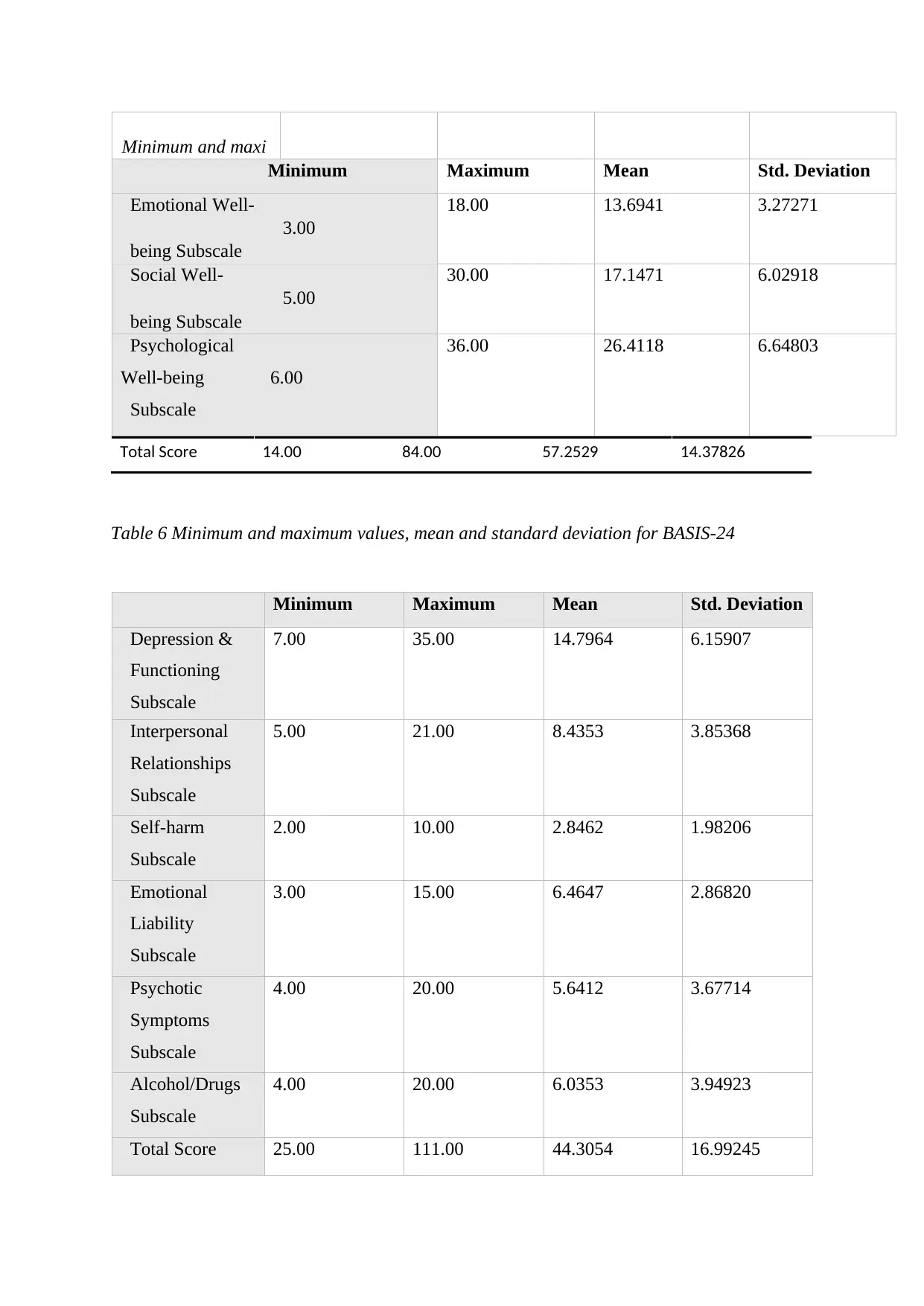
Minimum and maxi
Minimum Maximum Mean Std. Deviation
Emotional Well-
3.00
being Subscale
18.00 13.6941 3.27271
Social Well-
5.00
being Subscale
30.00 17.1471 6.02918
Psychological
Well-being 6.00
Subscale
36.00 26.4118 6.64803
Table 6 Minimum and maximum values, mean and standard deviation for BASIS-24
Minimum Maximum Mean Std. Deviation
Depression &
Functioning
Subscale
7.00 35.00 14.7964 6.15907
Interpersonal
Relationships
Subscale
5.00 21.00 8.4353 3.85368
Self-harm
Subscale
2.00 10.00 2.8462 1.98206
Emotional
Liability
Subscale
3.00 15.00 6.4647 2.86820
Psychotic
Symptoms
Subscale
4.00 20.00 5.6412 3.67714
Alcohol/Drugs
Subscale
4.00 20.00 6.0353 3.94923
Total Score 25.00 111.00 44.3054 16.99245
Total Score 14.00 84.00 57.2529 14.37826
Minimum Maximum Mean Std. Deviation
Emotional Well-
3.00
being Subscale
18.00 13.6941 3.27271
Social Well-
5.00
being Subscale
30.00 17.1471 6.02918
Psychological
Well-being 6.00
Subscale
36.00 26.4118 6.64803
Table 6 Minimum and maximum values, mean and standard deviation for BASIS-24
Minimum Maximum Mean Std. Deviation
Depression &
Functioning
Subscale
7.00 35.00 14.7964 6.15907
Interpersonal
Relationships
Subscale
5.00 21.00 8.4353 3.85368
Self-harm
Subscale
2.00 10.00 2.8462 1.98206
Emotional
Liability
Subscale
3.00 15.00 6.4647 2.86820
Psychotic
Symptoms
Subscale
4.00 20.00 5.6412 3.67714
Alcohol/Drugs
Subscale
4.00 20.00 6.0353 3.94923
Total Score 25.00 111.00 44.3054 16.99245
Total Score 14.00 84.00 57.2529 14.37826
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
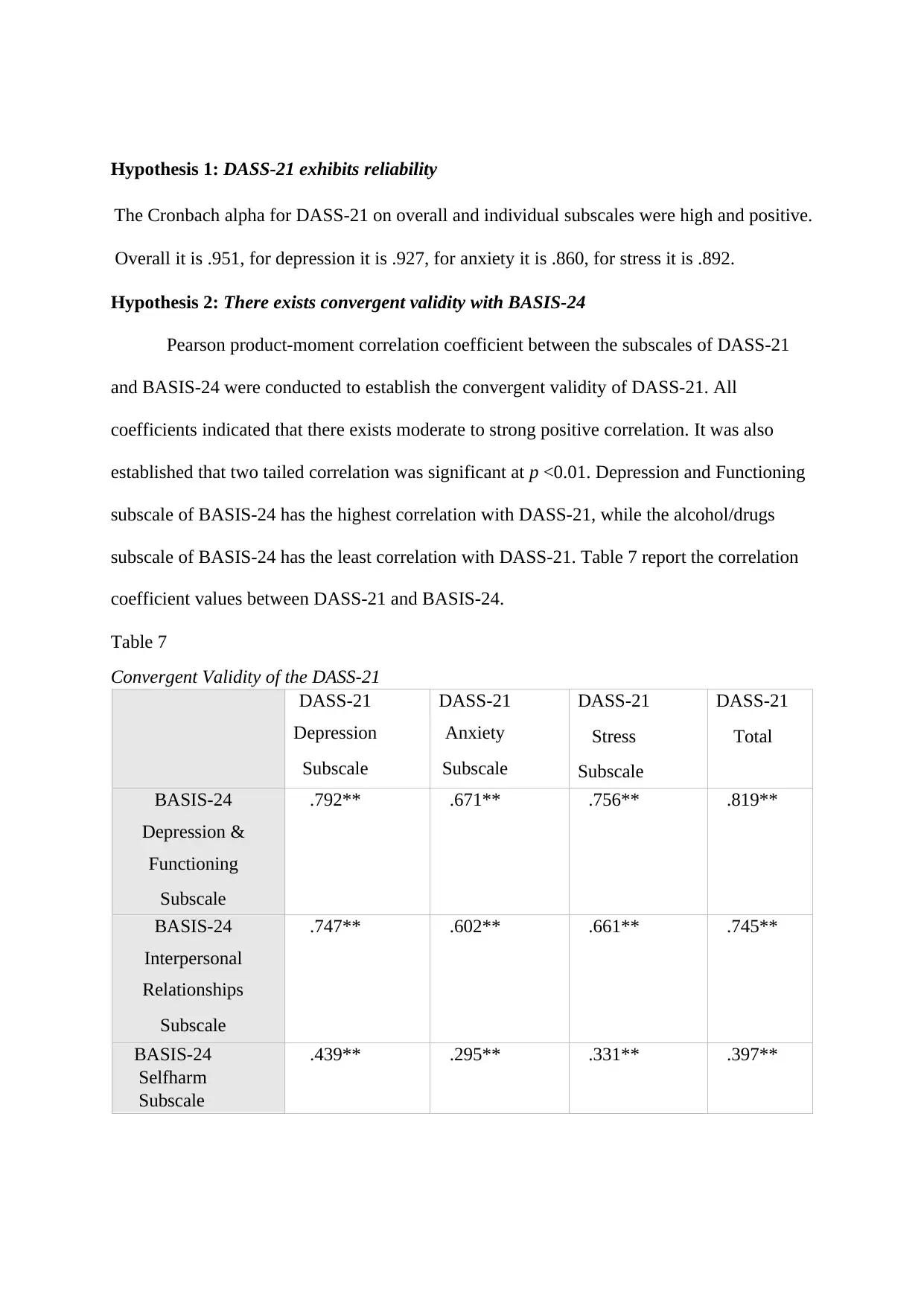
Hypothesis 1: DASS-21 exhibits reliability
The Cronbach alpha for DASS-21 on overall and individual subscales were high and positive.
Overall it is .951, for depression it is .927, for anxiety it is .860, for stress it is .892.
Hypothesis 2: There exists convergent validity with BASIS-24
Pearson product-moment correlation coefficient between the subscales of DASS-21
and BASIS-24 were conducted to establish the convergent validity of DASS-21. All
coefficients indicated that there exists moderate to strong positive correlation. It was also
established that two tailed correlation was significant at p <0.01. Depression and Functioning
subscale of BASIS-24 has the highest correlation with DASS-21, while the alcohol/drugs
subscale of BASIS-24 has the least correlation with DASS-21. Table 7 report the correlation
coefficient values between DASS-21 and BASIS-24.
Table 7
Convergent Validity of the DASS-21
DASS-21
Depression
Subscale
DASS-21
Anxiety
Subscale
DASS-21
Stress
Subscale
DASS-21
Total
BASIS-24
Depression &
Functioning
Subscale
.792** .671** .756** .819**
BASIS-24
Interpersonal
Relationships
Subscale
.747** .602** .661** .745**
BASIS-24
Selfharm
Subscale
.439** .295** .331** .397**
The Cronbach alpha for DASS-21 on overall and individual subscales were high and positive.
Overall it is .951, for depression it is .927, for anxiety it is .860, for stress it is .892.
Hypothesis 2: There exists convergent validity with BASIS-24
Pearson product-moment correlation coefficient between the subscales of DASS-21
and BASIS-24 were conducted to establish the convergent validity of DASS-21. All
coefficients indicated that there exists moderate to strong positive correlation. It was also
established that two tailed correlation was significant at p <0.01. Depression and Functioning
subscale of BASIS-24 has the highest correlation with DASS-21, while the alcohol/drugs
subscale of BASIS-24 has the least correlation with DASS-21. Table 7 report the correlation
coefficient values between DASS-21 and BASIS-24.
Table 7
Convergent Validity of the DASS-21
DASS-21
Depression
Subscale
DASS-21
Anxiety
Subscale
DASS-21
Stress
Subscale
DASS-21
Total
BASIS-24
Depression &
Functioning
Subscale
.792** .671** .756** .819**
BASIS-24
Interpersonal
Relationships
Subscale
.747** .602** .661** .745**
BASIS-24
Selfharm
Subscale
.439** .295** .331** .397**
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
BASIS-24
Emotional
Liability
Subscale
.579** .537** .665** .657**
BASIS-24
Psychotic
Symptoms
Subscale
.299** .251** .296** .313**
BASIS-24
Alcohol/Drugs
Subscale
.236** .246** .282** .281**
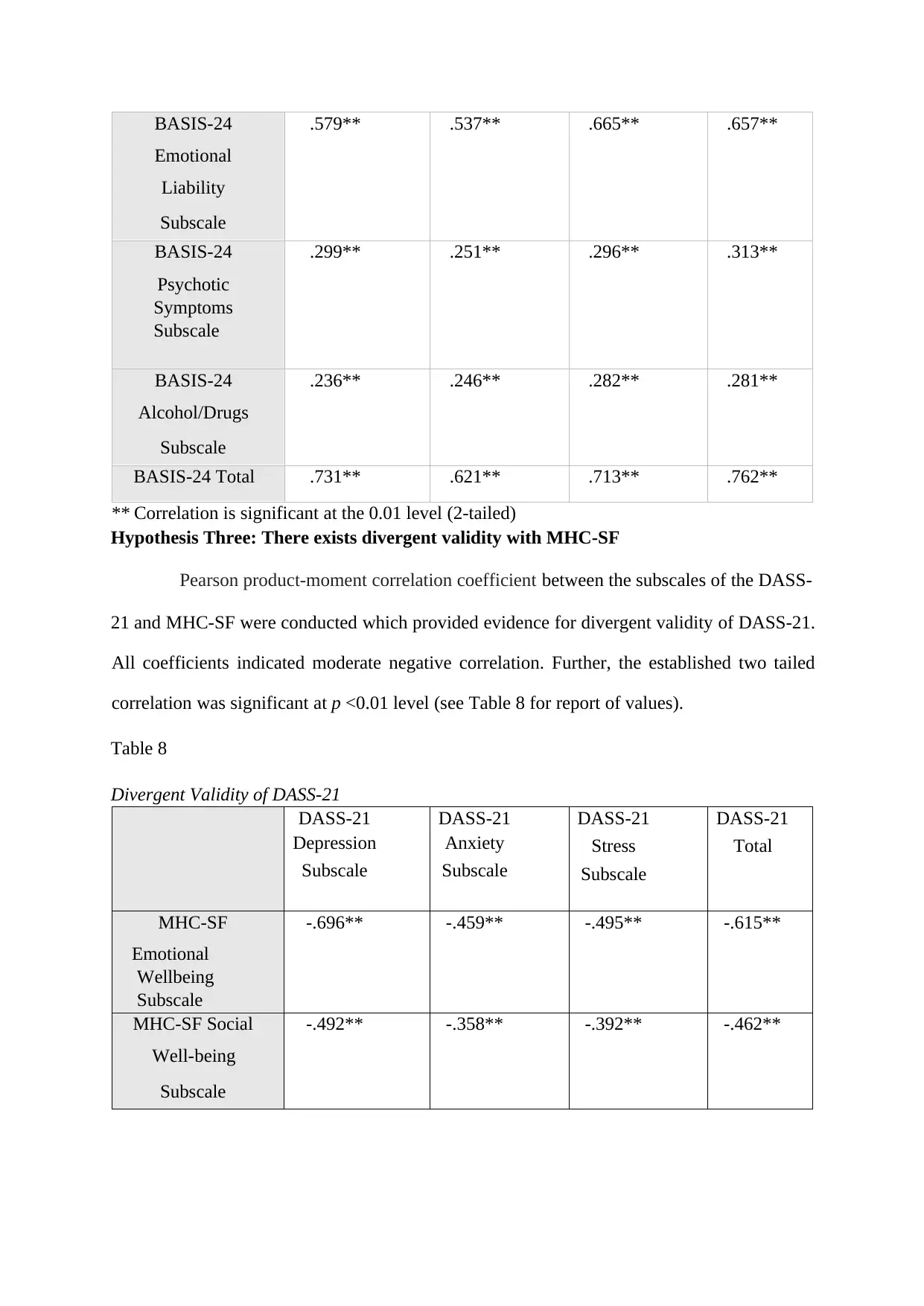
BASIS-24 Total .731** .621** .713** .762**
** Correlation is significant at the 0.01 level (2-tailed)
Hypothesis Three: There exists divergent validity with MHC-SF
Pearson product-moment correlation coefficient between the subscales of the DASS-
21 and MHC-SF were conducted which provided evidence for divergent validity of DASS-21.
All coefficients indicated moderate negative correlation. Further, the established two tailed
correlation was significant at p <0.01 level (see Table 8 for report of values).
Table 8
Divergent Validity of DASS-21
DASS-21
Depression
Subscale
DASS-21
Anxiety
Subscale
DASS-21
Stress
Subscale
DASS-21
Total
MHC-SF
Emotional
Wellbeing
Subscale
-.696** -.459** -.495** -.615**
MHC-SF Social
Well-being
Subscale
-.492** -.358** -.392** -.462**
Emotional
Liability
Subscale
.579** .537** .665** .657**
BASIS-24
Psychotic
Symptoms
Subscale
.299** .251** .296** .313**
BASIS-24
Alcohol/Drugs
Subscale
.236** .246** .282** .281**
BASIS-24 Total .731** .621** .713** .762**
** Correlation is significant at the 0.01 level (2-tailed)
Hypothesis Three: There exists divergent validity with MHC-SF
Pearson product-moment correlation coefficient between the subscales of the DASS-
21 and MHC-SF were conducted which provided evidence for divergent validity of DASS-21.
All coefficients indicated moderate negative correlation. Further, the established two tailed
correlation was significant at p <0.01 level (see Table 8 for report of values).
Table 8
Divergent Validity of DASS-21
DASS-21
Depression
Subscale
DASS-21
Anxiety
Subscale
DASS-21
Stress
Subscale
DASS-21
Total
MHC-SF
Emotional
Wellbeing
Subscale
-.696** -.459** -.495** -.615**
MHC-SF Social
Well-being
Subscale
-.492** -.358** -.392** -.462**
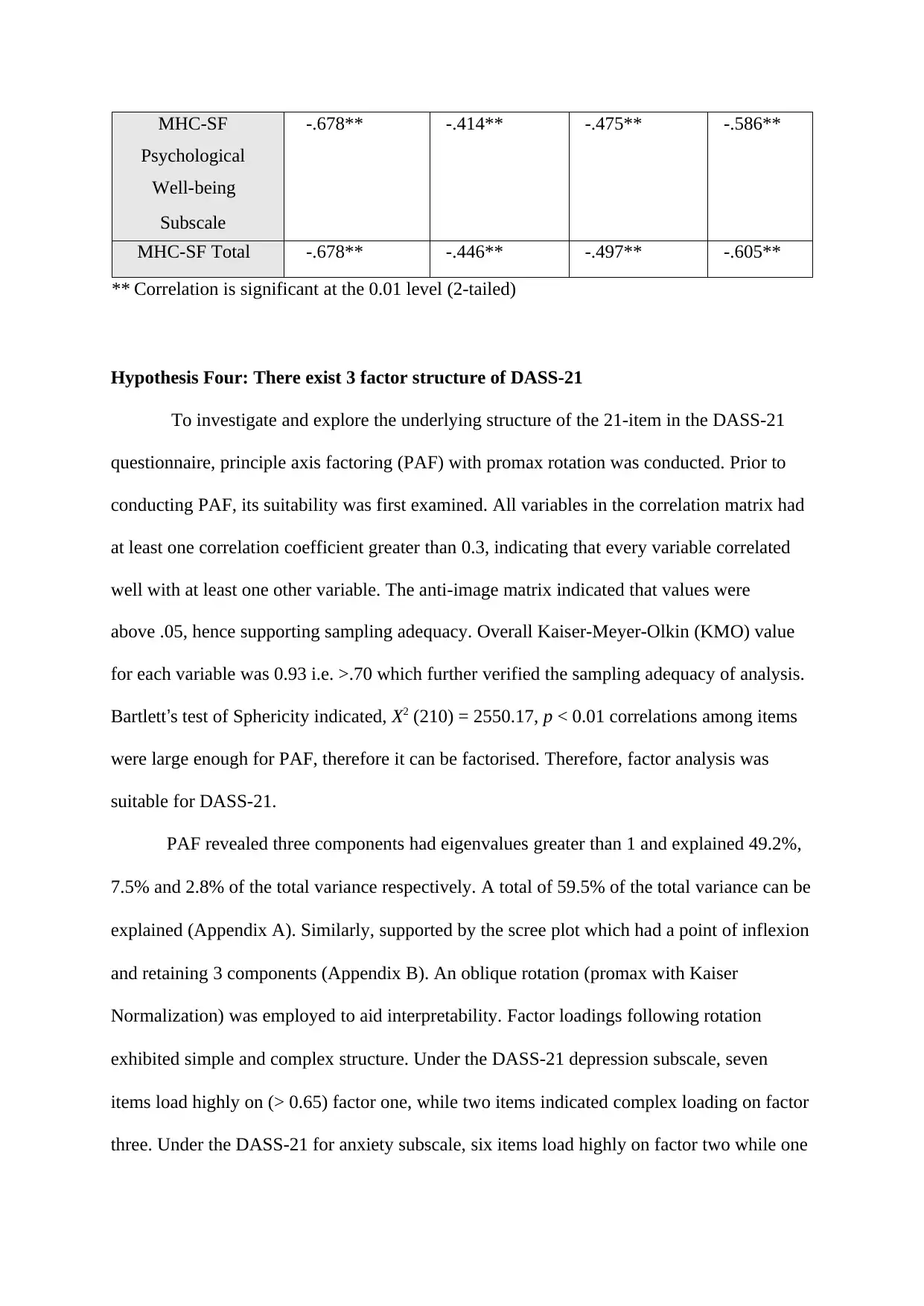
MHC-SF
Psychological
Well-being
Subscale
-.678** -.414** -.475** -.586**
MHC-SF Total -.678** -.446** -.497** -.605**
** Correlation is significant at the 0.01 level (2-tailed)
Hypothesis Four: There exist 3 factor structure of DASS-21
To investigate and explore the underlying structure of the 21-item in the DASS-21
questionnaire, principle axis factoring (PAF) with promax rotation was conducted. Prior to
conducting PAF, its suitability was first examined. All variables in the correlation matrix had
at least one correlation coefficient greater than 0.3, indicating that every variable correlated
well with at least one other variable. The anti-image matrix indicated that values were
above .05, hence supporting sampling adequacy. Overall Kaiser-Meyer-Olkin (KMO) value
for each variable was 0.93 i.e. >.70 which further verified the sampling adequacy of analysis.
Bartlett’s test of Sphericity indicated, X2 (210) = 2550.17, p < 0.01 correlations among items
were large enough for PAF, therefore it can be factorised. Therefore, factor analysis was
suitable for DASS-21.
PAF revealed three components had eigenvalues greater than 1 and explained 49.2%,
7.5% and 2.8% of the total variance respectively. A total of 59.5% of the total variance can be
explained (Appendix A). Similarly, supported by the scree plot which had a point of inflexion
and retaining 3 components (Appendix B). An oblique rotation (promax with Kaiser
Normalization) was employed to aid interpretability. Factor loadings following rotation
exhibited simple and complex structure. Under the DASS-21 depression subscale, seven
items load highly on (> 0.65) factor one, while two items indicated complex loading on factor
three. Under the DASS-21 for anxiety subscale, six items load highly on factor two while one
Psychological
Well-being
Subscale
-.678** -.414** -.475** -.586**
MHC-SF Total -.678** -.446** -.497** -.605**
** Correlation is significant at the 0.01 level (2-tailed)
Hypothesis Four: There exist 3 factor structure of DASS-21
To investigate and explore the underlying structure of the 21-item in the DASS-21
questionnaire, principle axis factoring (PAF) with promax rotation was conducted. Prior to
conducting PAF, its suitability was first examined. All variables in the correlation matrix had
at least one correlation coefficient greater than 0.3, indicating that every variable correlated
well with at least one other variable. The anti-image matrix indicated that values were
above .05, hence supporting sampling adequacy. Overall Kaiser-Meyer-Olkin (KMO) value
for each variable was 0.93 i.e. >.70 which further verified the sampling adequacy of analysis.
Bartlett’s test of Sphericity indicated, X2 (210) = 2550.17, p < 0.01 correlations among items
were large enough for PAF, therefore it can be factorised. Therefore, factor analysis was
suitable for DASS-21.
PAF revealed three components had eigenvalues greater than 1 and explained 49.2%,
7.5% and 2.8% of the total variance respectively. A total of 59.5% of the total variance can be
explained (Appendix A). Similarly, supported by the scree plot which had a point of inflexion
and retaining 3 components (Appendix B). An oblique rotation (promax with Kaiser
Normalization) was employed to aid interpretability. Factor loadings following rotation
exhibited simple and complex structure. Under the DASS-21 depression subscale, seven
items load highly on (> 0.65) factor one, while two items indicated complex loading on factor
three. Under the DASS-21 for anxiety subscale, six items load highly on factor two while one
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 19
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.