PUBH6007: Evaluating and Improving Diabetes Policies in Australia
VerifiedAdded on 2023/06/10
|9
|2095
|204
Report
AI Summary
This report provides a comprehensive needs assessment of diabetes management in Australia, addressing the prevalence of diabetes mellitus and its subtypes, particularly among the indigenous community. It evaluates existing policies, identifies challenges such as reduced awareness, access to treatment, and early diagnosis barriers, and proposes improvements using the NEEDS assessment tool. The analysis considers biomedical, behavioral, and structural interventions, emphasizing prevention, integration of strategies, and healthcare reformation. The report concludes by highlighting the importance of effective needs assessment in policy reframing and identifying potential issues for improved diabetes management.

Running head: PROGRAM DESIGN
PROGRAM DESIGN
Name of the Student:
Name of the University:
Author Note:
PROGRAM DESIGN
Name of the Student:
Name of the University:
Author Note:
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1PROGRAM DESIGN
Introduction:
Diabetes mellitus has emerged out to be the most common chronic illness issue in
Australia. Diabetes can be defined as a physiological disorder that is characterized by the
abnormal blood-glucose regulation in the body (Lee et al., 2013). Diabetes has been broadly
characterized under subtypes such as Type II Diabetes, Type I Diabetes, Prediabetes and
Gestational Diabetes (Kibbey et al., 2013). In accordance with the statistical data generated in
the year 2017, it had been revealed that approximately 1.2 million people of the entire population
were diagnosed with Diabetes. It should also be mentioned in this context that, by the end of the
year 2015, it was estimated that 1,002,000 people were already surviving with reported Diabetes
type II (Australian Institute of Health and Welfare, 2018). 13.5% of the people from the total
population were affected with Diabetes Type I (Australian Institute of Health and Welfare,
2018). The primary cause of the wide spread prevalence was identified as the sedentary lifestyle,
poor fibre intake, obesity, excessive body weight, smoking and alcohol consumption and reduced
physical fitness. The hike in the number of diagnosed individuals significantly points out the
seriousness of the prevalence rate of the disorder. At the end of every year, a notable 16.8% of
new diagnosed cases are coming up that is making the disease scenario even more critical
(Australian Institute of Health and Welfare, 2018). It should further be noted that according to
the statistical data collected the disease prevalence rate has increased considerably over the years
with an increase of 7% cases in men in the year 2015, 5% in women, 17% in old-age patients and
5% in middle aged individuals in comparison to previous years. A significant 29% of newly
diagnosed cases had been recorded in the second half of the year 2015 (Australian Institute of
Health and Welfare, 2018). This report intends to evaluate the existing policies with respect to
Diabetes management in Australia and critically analyze the scenario with the help of needs
Introduction:
Diabetes mellitus has emerged out to be the most common chronic illness issue in
Australia. Diabetes can be defined as a physiological disorder that is characterized by the
abnormal blood-glucose regulation in the body (Lee et al., 2013). Diabetes has been broadly
characterized under subtypes such as Type II Diabetes, Type I Diabetes, Prediabetes and
Gestational Diabetes (Kibbey et al., 2013). In accordance with the statistical data generated in
the year 2017, it had been revealed that approximately 1.2 million people of the entire population
were diagnosed with Diabetes. It should also be mentioned in this context that, by the end of the
year 2015, it was estimated that 1,002,000 people were already surviving with reported Diabetes
type II (Australian Institute of Health and Welfare, 2018). 13.5% of the people from the total
population were affected with Diabetes Type I (Australian Institute of Health and Welfare,
2018). The primary cause of the wide spread prevalence was identified as the sedentary lifestyle,
poor fibre intake, obesity, excessive body weight, smoking and alcohol consumption and reduced
physical fitness. The hike in the number of diagnosed individuals significantly points out the
seriousness of the prevalence rate of the disorder. At the end of every year, a notable 16.8% of
new diagnosed cases are coming up that is making the disease scenario even more critical
(Australian Institute of Health and Welfare, 2018). It should further be noted that according to
the statistical data collected the disease prevalence rate has increased considerably over the years
with an increase of 7% cases in men in the year 2015, 5% in women, 17% in old-age patients and
5% in middle aged individuals in comparison to previous years. A significant 29% of newly
diagnosed cases had been recorded in the second half of the year 2015 (Australian Institute of
Health and Welfare, 2018). This report intends to evaluate the existing policies with respect to
Diabetes management in Australia and critically analyze the scenario with the help of needs
2PROGRAM DESIGN
assessment. Further, the paper aims to cover the evaluation outcome on the basis of strong
recommendations.
Literature Review:
Australia follows a comprehensive strategy to analyze the Diabetes prevalence data. It
should be noted here that the disease prevalence data is collected at the stage of diagnosis across
all health care organization operating at the territory and state level. The collected data is
analyzed by the Australian Institute of Health and Welfare. In close association with the
evidence furnished by the statistical figures, it can be mentioned that the prevalence rate of
Diabetes has been considerably high in the members of the indigenous community (Zimmet et
al., 2016). The prevalence rate has been recorded to be higher among aboriginal community
member particularly because of reduced access to health care facilities. Particularly, studies
suggest that from the time frame of 2013-2017 a stark increase of 13% of increase in the rate of
prevalence was observed aboriginal men and women who had lack of access to education and
awareness about the disease condition (Stoneman et al., 2014). The reports revealed that 46,200
aboriginal adults had diabetes. On the contrary, it should be noted that the prevalence of TIIDM
was considerably higher among the female aboriginal members compared to men (Australian
Institute of Health and Welfare, 2018). The recorded prevalence rate has been retrieved to be
approximately 1 individual out of every 8 individuals (Australian Institute of Health and
Welfare, 2018). A total of 56% of the female aboriginals were recorded to be affected with
TIIDM compared to 44% men by the end of the year 2013 (Lee et al.,2013). The results stated
that Diabetes was more prevalent in aboriginal women compared to men (Kibbey et al., 2013).
Also, 6091 of the Type-I Diabetes cases were reported in children by the end of the year 2013
(Hollis et al., 2014). In addition to this 12.8% of individuals aged 15 years and above showed
assessment. Further, the paper aims to cover the evaluation outcome on the basis of strong
recommendations.
Literature Review:
Australia follows a comprehensive strategy to analyze the Diabetes prevalence data. It
should be noted here that the disease prevalence data is collected at the stage of diagnosis across
all health care organization operating at the territory and state level. The collected data is
analyzed by the Australian Institute of Health and Welfare. In close association with the
evidence furnished by the statistical figures, it can be mentioned that the prevalence rate of
Diabetes has been considerably high in the members of the indigenous community (Zimmet et
al., 2016). The prevalence rate has been recorded to be higher among aboriginal community
member particularly because of reduced access to health care facilities. Particularly, studies
suggest that from the time frame of 2013-2017 a stark increase of 13% of increase in the rate of
prevalence was observed aboriginal men and women who had lack of access to education and
awareness about the disease condition (Stoneman et al., 2014). The reports revealed that 46,200
aboriginal adults had diabetes. On the contrary, it should be noted that the prevalence of TIIDM
was considerably higher among the female aboriginal members compared to men (Australian
Institute of Health and Welfare, 2018). The recorded prevalence rate has been retrieved to be
approximately 1 individual out of every 8 individuals (Australian Institute of Health and
Welfare, 2018). A total of 56% of the female aboriginals were recorded to be affected with
TIIDM compared to 44% men by the end of the year 2013 (Lee et al.,2013). The results stated
that Diabetes was more prevalent in aboriginal women compared to men (Kibbey et al., 2013).
Also, 6091 of the Type-I Diabetes cases were reported in children by the end of the year 2013
(Hollis et al., 2014). In addition to this 12.8% of individuals aged 15 years and above showed
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide

3PROGRAM DESIGN
positive screening for Type II diabetes (Harris et al., 2013). The seriousness of the situation
alarmed the Australian government that led to the launch of a multitude of disease management
and prevention programs (Harding et al.,2014). Some of the successful disease prevention
programs constitute of initiatives such as public health programs, community engagement
programs and Diabetes management programs (Grantham et al., 2013).
Fig: NEEDS Assessment Tool
The Needs Assessment tool serves as an efficient tool that helps in analyzing the existing
situation and accordingly devises a solution on the basis of the consistency and feasibility of
implementing a reform. In order to effectively devise an effective reformed policy, the NEEDS
assessment would be used to evaluate the existing scenario (Adegbija et al., 2015). It should be
noted that despite the incorporation of health campaign programs on a massive scale, the
prevalence rate of the disease has still not gone down. The primary reasons that can be enlisted
for the same would incorporate the following reasons.
positive screening for Type II diabetes (Harris et al., 2013). The seriousness of the situation
alarmed the Australian government that led to the launch of a multitude of disease management
and prevention programs (Harding et al.,2014). Some of the successful disease prevention
programs constitute of initiatives such as public health programs, community engagement
programs and Diabetes management programs (Grantham et al., 2013).
Fig: NEEDS Assessment Tool
The Needs Assessment tool serves as an efficient tool that helps in analyzing the existing
situation and accordingly devises a solution on the basis of the consistency and feasibility of
implementing a reform. In order to effectively devise an effective reformed policy, the NEEDS
assessment would be used to evaluate the existing scenario (Adegbija et al., 2015). It should be
noted that despite the incorporation of health campaign programs on a massive scale, the
prevalence rate of the disease has still not gone down. The primary reasons that can be enlisted
for the same would incorporate the following reasons.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4PROGRAM DESIGN
The status of disease treatment has changed: Innovation in treatment facilities and
efficacy of insulin therapy has made it easier for the people to deal with the disease
condition and enhance the quality of life
Reduced awareness regarding the efficacy of available treatment facilities to manage the
illness condition
Reduced access to illness management programs so as to lead an enhanced quality of life
Barriers to early diagnosis and screening of Diabetes in the indigenous population base
Failure of detection at the initial stage
Failure in identification in high-risk population
Best Analysis Approach:
The best analysis approach that can be implied to combat the seriousness of the program
would comprise of reviewing the existing national level policies and incorporate amendment for
the benefit of the target population. The rationale for the chosen analysis has been considered at
the national level so as to critically consider the statistical data collected across each state and
accordingly implement effective reforms for the benefit of the identified target population in
each state.
Challenges:
The challenges that could be encountered while framing and implementation of the
revised policies would comprise of consideration of the social health determinants of the target
population and the existing socio-political scenario. In addition to the same, the effective
implementation of the proposed program design in compliance with the involved stakeholders
and the infrastructural status to assimilate the proposed reform strategy (Abouzeid et al., 2013).
The status of disease treatment has changed: Innovation in treatment facilities and
efficacy of insulin therapy has made it easier for the people to deal with the disease
condition and enhance the quality of life
Reduced awareness regarding the efficacy of available treatment facilities to manage the
illness condition
Reduced access to illness management programs so as to lead an enhanced quality of life
Barriers to early diagnosis and screening of Diabetes in the indigenous population base
Failure of detection at the initial stage
Failure in identification in high-risk population
Best Analysis Approach:
The best analysis approach that can be implied to combat the seriousness of the program
would comprise of reviewing the existing national level policies and incorporate amendment for
the benefit of the target population. The rationale for the chosen analysis has been considered at
the national level so as to critically consider the statistical data collected across each state and
accordingly implement effective reforms for the benefit of the identified target population in
each state.
Challenges:
The challenges that could be encountered while framing and implementation of the
revised policies would comprise of consideration of the social health determinants of the target
population and the existing socio-political scenario. In addition to the same, the effective
implementation of the proposed program design in compliance with the involved stakeholders
and the infrastructural status to assimilate the proposed reform strategy (Abouzeid et al., 2013).
5PROGRAM DESIGN
In addition to this, the minimal skill of the workforce to feasibly incorporate the proposed reform
strategy and uphold the vision of health and wellness for entire community.
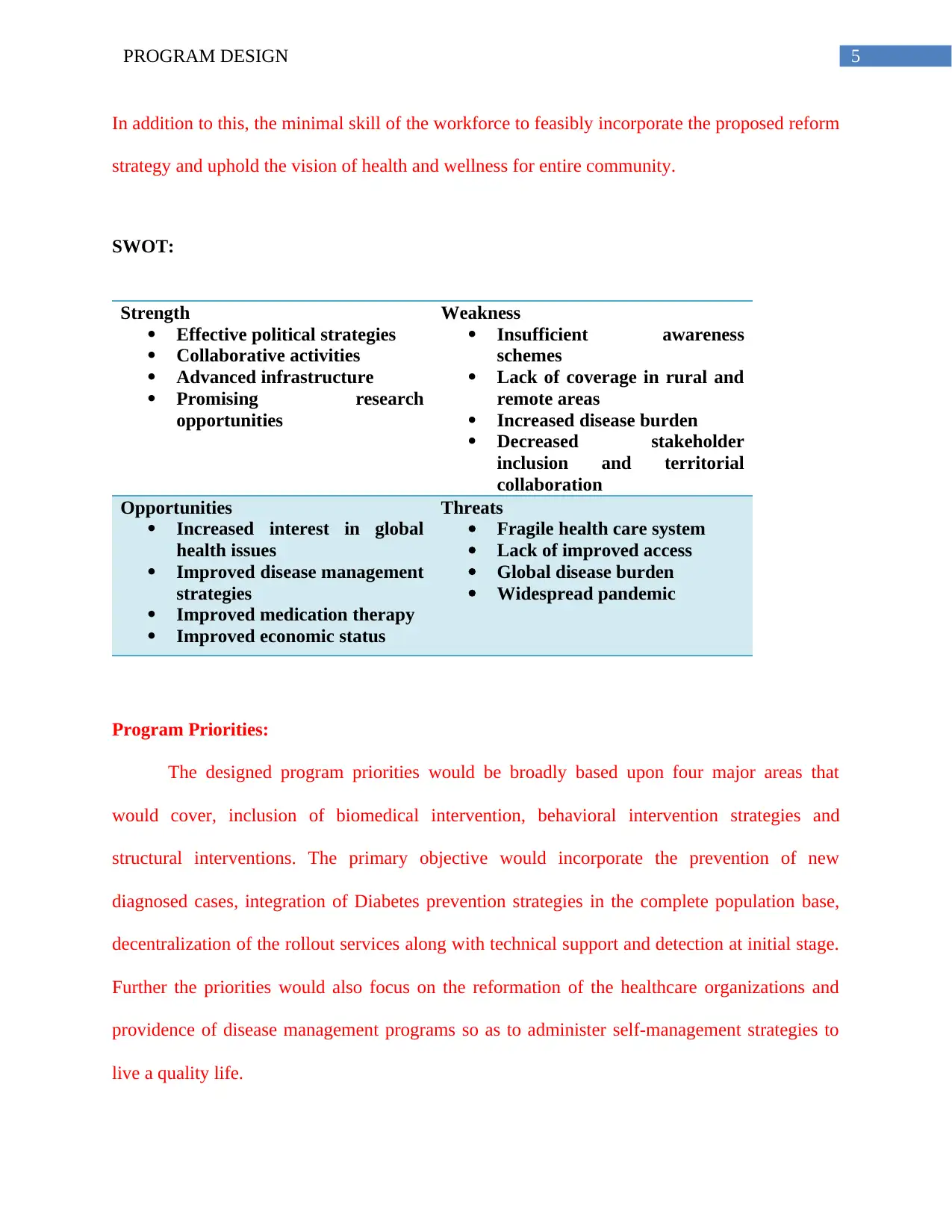
SWOT:
Strength
Effective political strategies
Collaborative activities
Advanced infrastructure
Promising research
opportunities
Weakness
Insufficient awareness
schemes
Lack of coverage in rural and
remote areas
Increased disease burden
Decreased stakeholder
inclusion and territorial
collaboration
Opportunities
Increased interest in global
health issues
Improved disease management
strategies
Improved medication therapy
Improved economic status
Threats
Fragile health care system
Lack of improved access
Global disease burden
Widespread pandemic
Program Priorities:
The designed program priorities would be broadly based upon four major areas that
would cover, inclusion of biomedical intervention, behavioral intervention strategies and
structural interventions. The primary objective would incorporate the prevention of new
diagnosed cases, integration of Diabetes prevention strategies in the complete population base,
decentralization of the rollout services along with technical support and detection at initial stage.
Further the priorities would also focus on the reformation of the healthcare organizations and
providence of disease management programs so as to administer self-management strategies to
live a quality life.
In addition to this, the minimal skill of the workforce to feasibly incorporate the proposed reform
strategy and uphold the vision of health and wellness for entire community.
SWOT:
Strength
Effective political strategies
Collaborative activities
Advanced infrastructure
Promising research
opportunities
Weakness
Insufficient awareness
schemes
Lack of coverage in rural and
remote areas
Increased disease burden
Decreased stakeholder
inclusion and territorial
collaboration
Opportunities
Increased interest in global
health issues
Improved disease management
strategies
Improved medication therapy
Improved economic status
Threats
Fragile health care system
Lack of improved access
Global disease burden
Widespread pandemic
Program Priorities:
The designed program priorities would be broadly based upon four major areas that
would cover, inclusion of biomedical intervention, behavioral intervention strategies and
structural interventions. The primary objective would incorporate the prevention of new
diagnosed cases, integration of Diabetes prevention strategies in the complete population base,
decentralization of the rollout services along with technical support and detection at initial stage.
Further the priorities would also focus on the reformation of the healthcare organizations and
providence of disease management programs so as to administer self-management strategies to
live a quality life.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6PROGRAM DESIGN
Conclusion:
Hence, to conclude it can be said that effective needs assessment has helped in the
generation of relevant data so as to identify the key priorities of the health issue. Further, it has
also helped in the reframing process of the existing policy with minimal hindrance and has
helped in the collection and interpretation of the invasive data findings collected from the
research study. It has also helped in identifying unanticipated issues that might come up while
designing policies and has substantially helped in finding effective solutions.
Conclusion:
Hence, to conclude it can be said that effective needs assessment has helped in the
generation of relevant data so as to identify the key priorities of the health issue. Further, it has
also helped in the reframing process of the existing policy with minimal hindrance and has
helped in the collection and interpretation of the invasive data findings collected from the
research study. It has also helped in identifying unanticipated issues that might come up while
designing policies and has substantially helped in finding effective solutions.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7PROGRAM DESIGN
References:
Abouzeid, M., Philpot, B., Janus, E. D., Coates, M. J., & Dunbar, J. A. (2013). Type 2 diabetes
prevalence varies by socio-economic status within and between migrant groups: analysis
and implications for Australia. BMC public health, 13(1), 252.
Adegbija, O., Hoy, W., & Wang, Z. (2015). Predicting absolute risk of type 2 diabetes using age
and waist circumference values in an aboriginal Australian community. PloS one, 10(4),
e0123788.
Australian Institute of Health and Welfare. (2018). Diabetes snapshot, How many Australians
have diabetes? - Australian Institute of Health and Welfare. Retrieved from
https://www.aihw.gov.au/reports/diabetes/diabetes-snapshot/contents/how-many-
australians-have-diabetes
Grantham, N. M., Magliano, D. J., Hodge, A., Jowett, J., Meikle, P., & Shaw, J. E. (2013). The
association between dairy food intake and the incidence of diabetes in Australia: the
Australian Diabetes Obesity and Lifestyle Study (AusDiab). Public health
nutrition, 16(2), 339-345.
Harding, J. L., Shaw, J. E., Peeters, A., Guiver, T., Davidson, S., & Magliano, D. J. (2014).
Mortality trends among people with type 1 and type 2 diabetes in Australia: 1997–
2010. Diabetes Care, DC_140096.
Harris, S. B., Bhattacharyya, O., Dyck, R., Hayward, M. N., & Toth, E. L. (2013). Type 2
diabetes in Aboriginal peoples. Canadian journal of diabetes, 37, S191-S196.
References:
Abouzeid, M., Philpot, B., Janus, E. D., Coates, M. J., & Dunbar, J. A. (2013). Type 2 diabetes
prevalence varies by socio-economic status within and between migrant groups: analysis
and implications for Australia. BMC public health, 13(1), 252.
Adegbija, O., Hoy, W., & Wang, Z. (2015). Predicting absolute risk of type 2 diabetes using age
and waist circumference values in an aboriginal Australian community. PloS one, 10(4),
e0123788.
Australian Institute of Health and Welfare. (2018). Diabetes snapshot, How many Australians
have diabetes? - Australian Institute of Health and Welfare. Retrieved from
https://www.aihw.gov.au/reports/diabetes/diabetes-snapshot/contents/how-many-
australians-have-diabetes
Grantham, N. M., Magliano, D. J., Hodge, A., Jowett, J., Meikle, P., & Shaw, J. E. (2013). The
association between dairy food intake and the incidence of diabetes in Australia: the
Australian Diabetes Obesity and Lifestyle Study (AusDiab). Public health
nutrition, 16(2), 339-345.
Harding, J. L., Shaw, J. E., Peeters, A., Guiver, T., Davidson, S., & Magliano, D. J. (2014).
Mortality trends among people with type 1 and type 2 diabetes in Australia: 1997–
2010. Diabetes Care, DC_140096.
Harris, S. B., Bhattacharyya, O., Dyck, R., Hayward, M. N., & Toth, E. L. (2013). Type 2
diabetes in Aboriginal peoples. Canadian journal of diabetes, 37, S191-S196.
8PROGRAM DESIGN
Hollis, M., Glaister, K., & Anne Lapsley, J. (2014). Do practice nurses have the knowledge to
provide diabetes self-management education?. Contemporary nurse, 46(2), 234-241.
Kibbey, K. J., Speight, J., Wong, J. L. A., Smith, L. A., & Teede, H. J. (2013). Diabetes care
provision: barriers, enablers and service needs of young adults with type 1 diabetes from
a region of social disadvantage. Diabetic medicine, 30(7), 878-884.
Lee, C. M. Y., Colagiuri, R., Magliano, D. J., Cameron, A. J., Shaw, J., Zimmet, P., & Colagiuri,
S. (2013). The cost of diabetes in adults in Australia. Diabetes research and clinical
practice, 99(3), 385-390.
Stoneman, A., Atkinson, D., Davey, M., & Marley, J. V. (2014). Quality improvement in
practice: improving diabetes care and patient outcomes in Aboriginal Community
Controlled Health Services. BMC health services research, 14(1), 481.
Zimmet, P., Alberti, K. G., Magliano, D. J., & Bennett, P. H. (2016). Diabetes mellitus statistics
on prevalence and mortality: facts and fallacies. Nature Reviews Endocrinology, 12(10),
616.
Hollis, M., Glaister, K., & Anne Lapsley, J. (2014). Do practice nurses have the knowledge to
provide diabetes self-management education?. Contemporary nurse, 46(2), 234-241.
Kibbey, K. J., Speight, J., Wong, J. L. A., Smith, L. A., & Teede, H. J. (2013). Diabetes care
provision: barriers, enablers and service needs of young adults with type 1 diabetes from
a region of social disadvantage. Diabetic medicine, 30(7), 878-884.
Lee, C. M. Y., Colagiuri, R., Magliano, D. J., Cameron, A. J., Shaw, J., Zimmet, P., & Colagiuri,
S. (2013). The cost of diabetes in adults in Australia. Diabetes research and clinical
practice, 99(3), 385-390.
Stoneman, A., Atkinson, D., Davey, M., & Marley, J. V. (2014). Quality improvement in
practice: improving diabetes care and patient outcomes in Aboriginal Community
Controlled Health Services. BMC health services research, 14(1), 481.
Zimmet, P., Alberti, K. G., Magliano, D. J., & Bennett, P. H. (2016). Diabetes mellitus statistics
on prevalence and mortality: facts and fallacies. Nature Reviews Endocrinology, 12(10),
616.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 9
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.