USC Public Health Programs: Health Promotion Setting Analysis Report
VerifiedAdded on 2023/06/04
|4
|1491
|82
Report
AI Summary
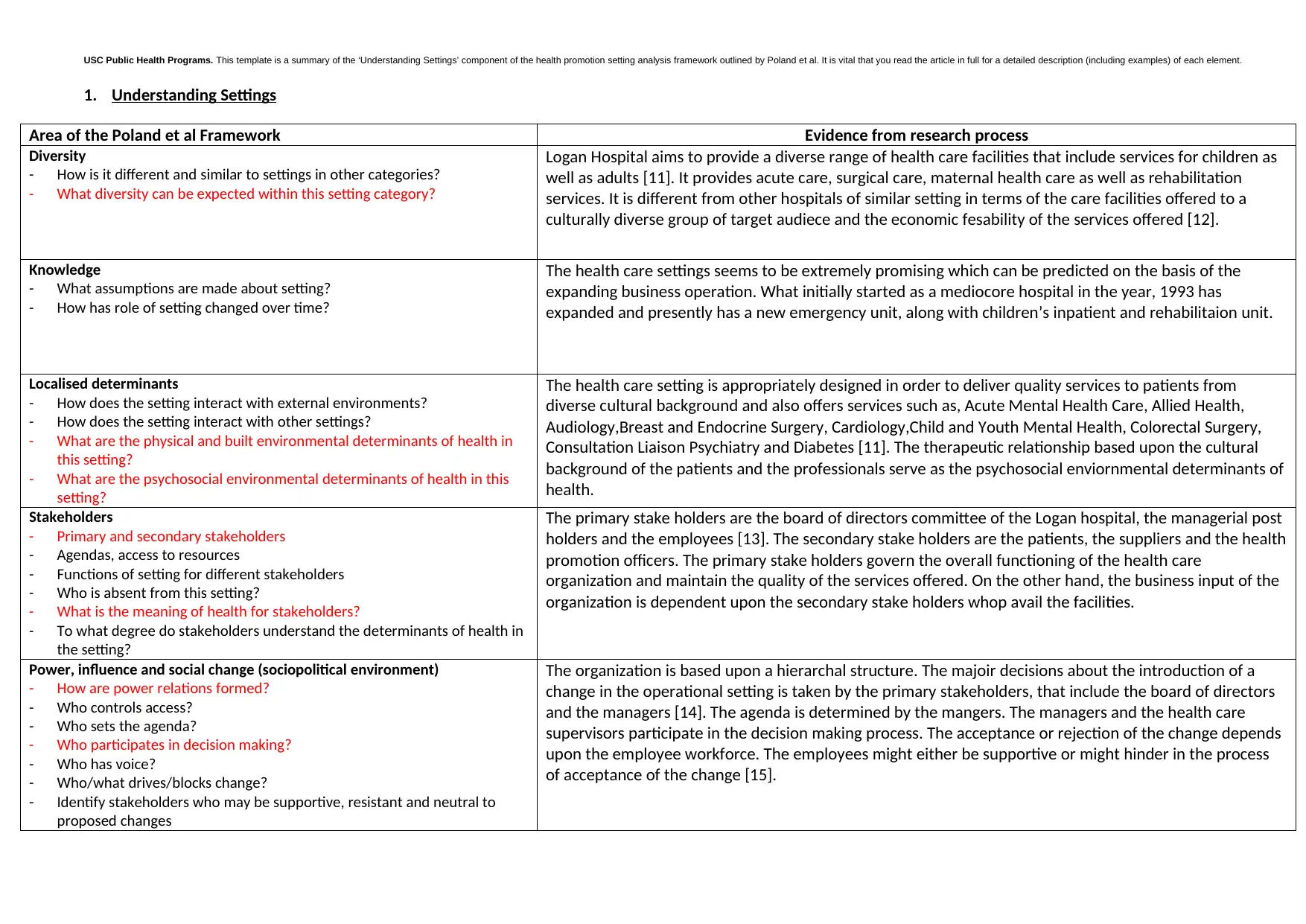
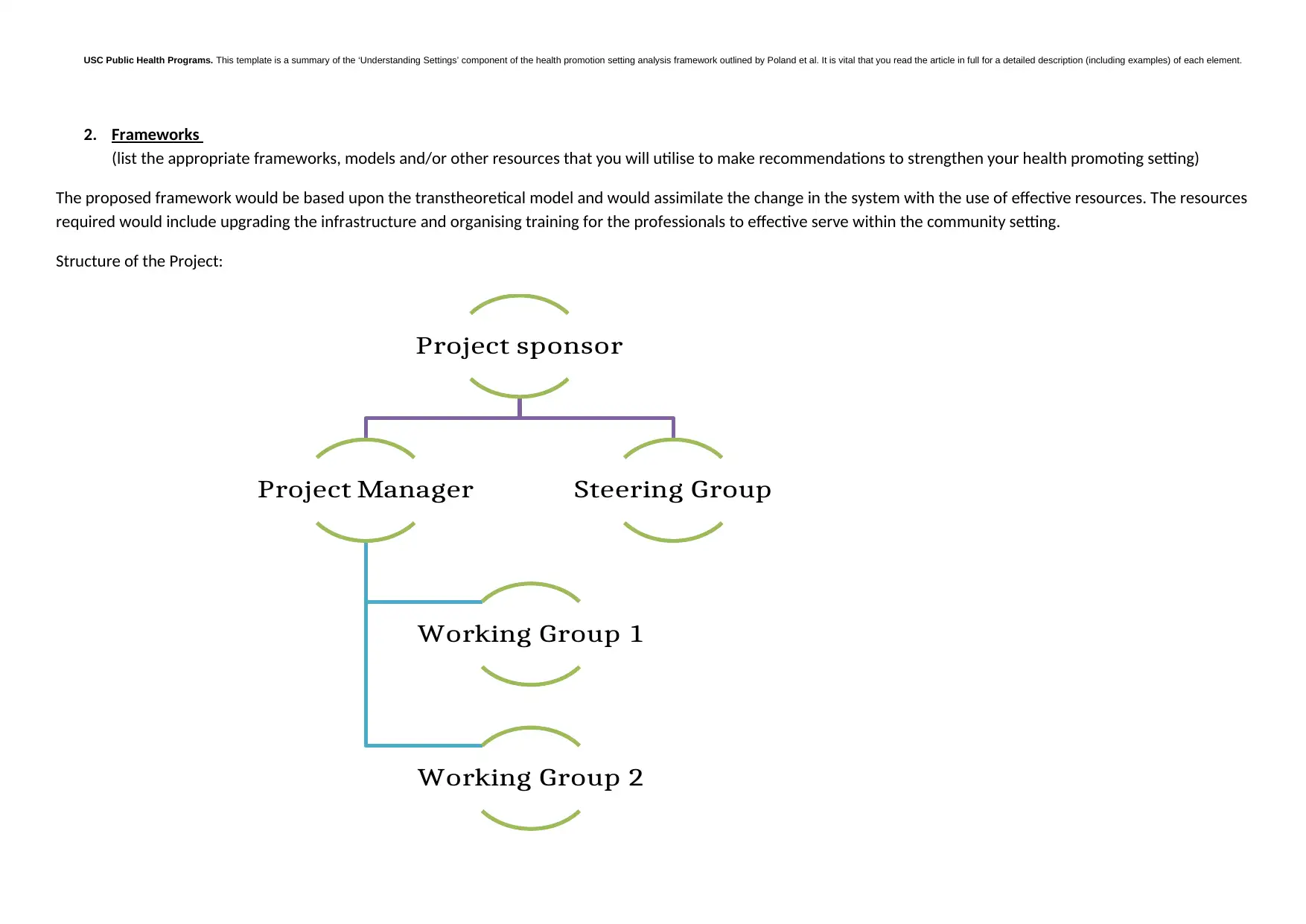
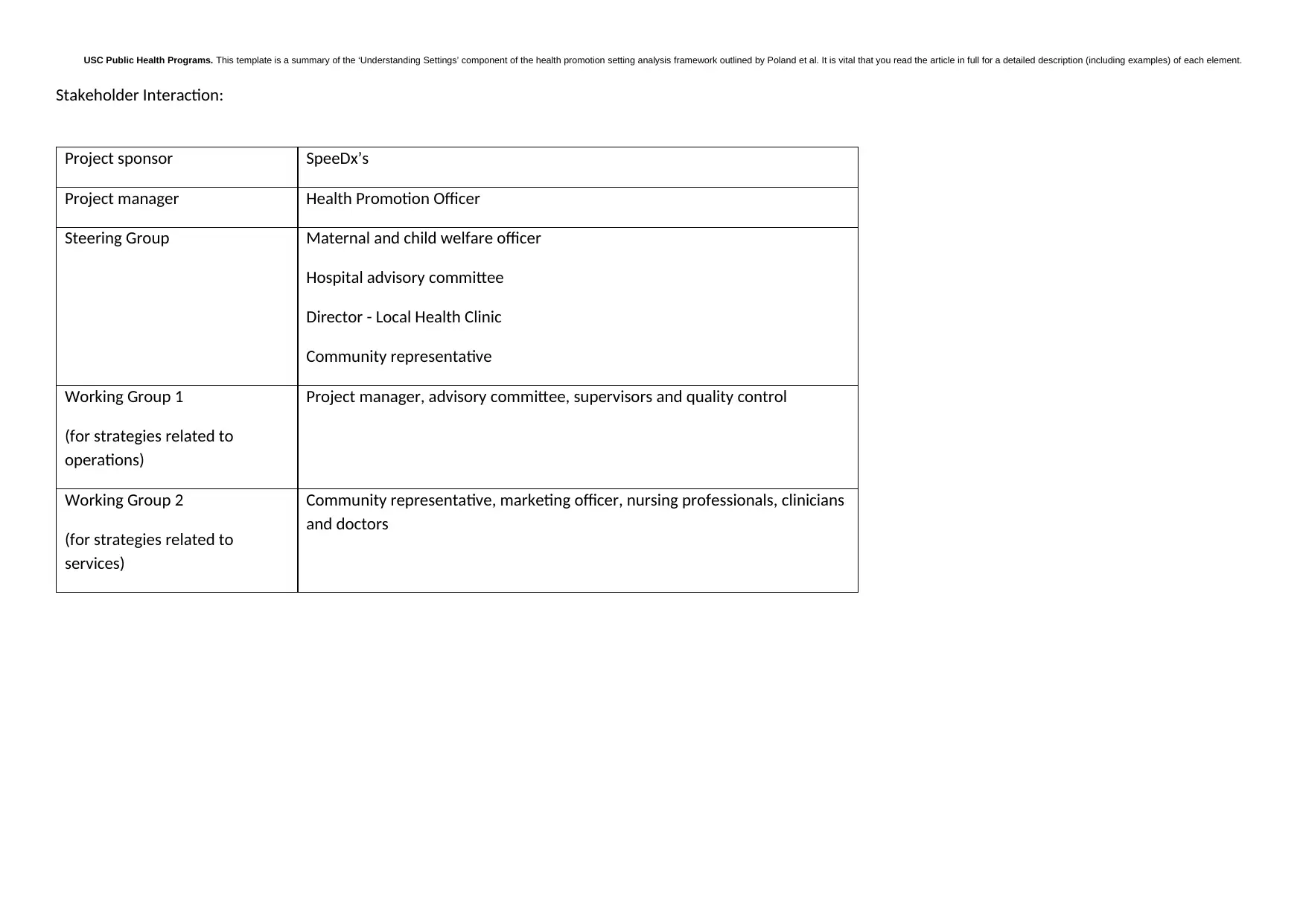
This report presents a health promotion setting analysis within the context of USC Public Health Programs, utilizing the framework outlined by Poland et al. It examines the diversity, knowledge, and localized determinants within a healthcare setting, specifically Logan Hospital, highlighting its services and cultural diversity. The analysis identifies primary stakeholders (board of directors, managers, employees) and secondary stakeholders (patients, suppliers, health promotion officers), detailing their roles and influence. Power dynamics and decision-making processes are explored, with a focus on how changes are implemented and accepted within the organization. Furthermore, the report proposes a framework based on the transtheoretical model, emphasizing resource allocation and professional training. It outlines stakeholder interactions and governance structures, including project sponsors, managers, steering groups, and working groups. The document also includes a strategy plan table, aligning strategies with relevant domains and evidence-based practices to strengthen health promotion efforts, referencing various studies and guidelines to support the analysis and proposed interventions.
1 out of 4
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.