Public Health Workforce Plan: Addressing Shortages in Indonesia
VerifiedAdded on 2023/06/10
|21
|4763
|440
Report
AI Summary
This report presents a comprehensive health workforce plan specifically tailored for Indonesia, addressing the critical shortages in healthcare professionals and the challenges in HRH management. The report begins with an executive summary outlining the importance of a skilled health workforce for effective healthcare delivery and human development. It highlights the issues faced by Indonesia, a middle-income country, including shortages of doctors, nurses, and other healthcare providers, as well as uneven distribution of personnel. The report then delves into the nature and extent of the issue, providing an environmental scan and a health workforce data profile to analyze the challenges faced by Indonesia. It examines the impact of decentralization on the healthcare system and the implications of these shortages. The core of the report is the health workforce plan, which covers education, skills, job creation, technology, service delivery, HRH utilization, financial aspects, partnerships, information, and humanitarian settings. A strategic plan is also developed, outlining a five-year roadmap (2019-2023) for improving the health workforce, including specific actions and targets for each year to enhance quality of care and meet the needs of the population. The report concludes with a strategic plan to mitigate the healthcare challenges in Indonesia.

Running head: PUBLIC HEALTH
Public health
Name of the Student
Name of the University
Author note
Public health
Name of the Student
Name of the University
Author note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
PUBLIC HEALTH
Executive summary
The following report focuses on the importance of a health workforce essential for health
services and human development in a country. Population health is of paramount importance that
requires careful planning in recruiting a skilled health workforce. For an efficient healthcare
delivery, HRH need to plan, recruit and select health personnel who are able to meet the health
needs of the population. However, in low and middle-income countries, the scenario is different
as they face critical shortage in healthcare providers. According to WHO, “World Health
Statistics Report, 2015” Indonesia falls under middle-income country category facing inadequate
human resource and health workers due to international migration and imbalances in demand and
supply. There are shortages of staffs ranging from doctors, nurses, midwives, clinicians and
pharmacists. The data profile showed that there is unequal distribution of health personnel, lack
of retention strategies and motivation among the health personnel. This shortage has significant
impact on the population contributing to low quality of services to the population. Therefore, this
report provides a health workforce plan that is aimed to mitigate the critical shortages witnessed
by Indonesia through HRH management and improvement of infrastructural processes.
Furthermore, this report will also provide a strategic plan on improving the health workforce in
Indonesia and enhance quality of care in meeting the needs of the population.
PUBLIC HEALTH
Executive summary
The following report focuses on the importance of a health workforce essential for health
services and human development in a country. Population health is of paramount importance that
requires careful planning in recruiting a skilled health workforce. For an efficient healthcare
delivery, HRH need to plan, recruit and select health personnel who are able to meet the health
needs of the population. However, in low and middle-income countries, the scenario is different
as they face critical shortage in healthcare providers. According to WHO, “World Health
Statistics Report, 2015” Indonesia falls under middle-income country category facing inadequate
human resource and health workers due to international migration and imbalances in demand and
supply. There are shortages of staffs ranging from doctors, nurses, midwives, clinicians and
pharmacists. The data profile showed that there is unequal distribution of health personnel, lack
of retention strategies and motivation among the health personnel. This shortage has significant
impact on the population contributing to low quality of services to the population. Therefore, this
report provides a health workforce plan that is aimed to mitigate the critical shortages witnessed
by Indonesia through HRH management and improvement of infrastructural processes.
Furthermore, this report will also provide a strategic plan on improving the health workforce in
Indonesia and enhance quality of care in meeting the needs of the population.
2
PUBLIC HEALTH
Table of Contents
1. Introduction..............................................................................................................................4
2. Nature and Extent of Issue.......................................................................................................4
2.1 Environmental scan...........................................................................................................4
2.2 Health workforce data profile................................................................................................7
3. Health workforce plan............................................................................................................10
3.1 Education, Skills and training..............................................................................................10
3.2 Job creation..........................................................................................................................11
3.3 Women and gender rights....................................................................................................11
3.4 Technology..........................................................................................................................11
3.5 Healthcare service delivery..................................................................................................12
3.6 HRH utilization....................................................................................................................12
3.7 Financial space.....................................................................................................................13
3.8 Partnership and coordination...............................................................................................13
3.9 Information, data and accountability...................................................................................14
3.10 Humanitarian and crisis settings........................................................................................14
4. Conclusion..............................................................................................................................14
5. Strategic plan..........................................................................................................................15
5.1 Health and HR plan in Indonesia:........................................................................................15
5.1.1 Year 1- 2019................................................................................................................16
PUBLIC HEALTH
Table of Contents
1. Introduction..............................................................................................................................4
2. Nature and Extent of Issue.......................................................................................................4
2.1 Environmental scan...........................................................................................................4
2.2 Health workforce data profile................................................................................................7
3. Health workforce plan............................................................................................................10
3.1 Education, Skills and training..............................................................................................10
3.2 Job creation..........................................................................................................................11
3.3 Women and gender rights....................................................................................................11
3.4 Technology..........................................................................................................................11
3.5 Healthcare service delivery..................................................................................................12
3.6 HRH utilization....................................................................................................................12
3.7 Financial space.....................................................................................................................13
3.8 Partnership and coordination...............................................................................................13
3.9 Information, data and accountability...................................................................................14
3.10 Humanitarian and crisis settings........................................................................................14
4. Conclusion..............................................................................................................................14
5. Strategic plan..........................................................................................................................15
5.1 Health and HR plan in Indonesia:........................................................................................15
5.1.1 Year 1- 2019................................................................................................................16
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
PUBLIC HEALTH
5.1.2 Year 2- 2020..................................................................................................................16
5.1.3 Year 3- 2021................................................................................................................16
5.1.4 Year 4- 2022................................................................................................................16
5.1.5 Year 5- 2023................................................................................................................16
References......................................................................................................................................18
PUBLIC HEALTH
5.1.2 Year 2- 2020..................................................................................................................16
5.1.3 Year 3- 2021................................................................................................................16
5.1.4 Year 4- 2022................................................................................................................16
5.1.5 Year 5- 2023................................................................................................................16
References......................................................................................................................................18
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
PUBLIC HEALTH
1. Introduction
The skills, motivation, knowledge and deployment are the factors that define the ability
of a country in meeting their health goals. The number of health workers is directly linked to the
population health outcomes as outlined in literature. There is also need for formulation of
healthcare workforce plans and formulations for meeting the objectives of health development
with sound evidence and information. “World Health Statistics Report, 2015” by WHO has
segmented the low and lower middle income countries and while analyzing the report, Indonesia
face major concerns in terms of shortage of healthcare professionals with uneven distribution in
various healthcare settings and management of health workforce in a decentralized healthcare
system (Fulton et al., 2011). The rationale for choosing this country is that Indonesia is lacking
these building blocks especially in terms of good health facing a critical shortage of healthcare
professionals. Indonesia is facing challenges related to human health resources like inequitable
health workers distribution, shortage of skilled staffs, absenteeism and lack of motivation. There
is also poor supervision lack of support and unsatisfactory working environments in Indonesia.
There is need for advocating the human resource issues and situational analysis on the national
agenda. Therefore, the following report analyzes the health workforce profile and critical issues
witnessed in Indonesia along with recommendations on the shortage and migration of healthcare
professionals using WHO framework.
2. Nature and Extent of Issue
2.1 Environmental scan
Indonesia faces critical challenges in terms of human resources for health (HRH)
that is related to planning and development of HRH (Human Resource for Health) policy
PUBLIC HEALTH
1. Introduction
The skills, motivation, knowledge and deployment are the factors that define the ability
of a country in meeting their health goals. The number of health workers is directly linked to the
population health outcomes as outlined in literature. There is also need for formulation of
healthcare workforce plans and formulations for meeting the objectives of health development
with sound evidence and information. “World Health Statistics Report, 2015” by WHO has
segmented the low and lower middle income countries and while analyzing the report, Indonesia
face major concerns in terms of shortage of healthcare professionals with uneven distribution in
various healthcare settings and management of health workforce in a decentralized healthcare
system (Fulton et al., 2011). The rationale for choosing this country is that Indonesia is lacking
these building blocks especially in terms of good health facing a critical shortage of healthcare
professionals. Indonesia is facing challenges related to human health resources like inequitable
health workers distribution, shortage of skilled staffs, absenteeism and lack of motivation. There
is also poor supervision lack of support and unsatisfactory working environments in Indonesia.
There is need for advocating the human resource issues and situational analysis on the national
agenda. Therefore, the following report analyzes the health workforce profile and critical issues
witnessed in Indonesia along with recommendations on the shortage and migration of healthcare
professionals using WHO framework.
2. Nature and Extent of Issue
2.1 Environmental scan
Indonesia faces critical challenges in terms of human resources for health (HRH)
that is related to planning and development of HRH (Human Resource for Health) policy
5
PUBLIC HEALTH
with mismatches between production, demand and supply, mal-distribution and
remuneration in rural, urban and remote areas. The decentralization of health system in
Indonesia is the main reason that the country is facing challenges in terms of healthcare
system. The law was enacted in 2001 on local autonomy and that marked the beginning
of decentralization, however, its implementation was different at each level of
government (Pepinsky & Wihardja, 2011). The transferring of autonomy gave districts
more independence in terms of regulation and management of affairs in the health sector.
The line of coordination was ignored at the upper level that did not function as command
line. Although, the central line wanted to control the main line, however, the HRH
situation deteriorated due to decentralization.
As per the 2010 census, Indonesia ranked last among the ten populous countries
with respect to physicians density per 1000 population compared to Russia, United States
and China ranking first, second and fourth respectively. Similarly, Indonesia ranked fifth
in nurse and midwives density (2.04/1000) with United States, Russia, Brazil and Japan
occupying the first four positions (Rokx, 2010). During the years 2000-2012, the number
of nurses, midwives and physicians increased substantially, however, it was not
significant. The increase in health workforce was not enough to meet the needs of the
population in terms of health. Moreover, hospital beds per 1000 population were quite
low as per 2010 census on the global scale (Hoyler et al., 2014).
Decentralization in Indonesia has given the local governments to take up the
direct authority of prioritizing healthcare sectors for development. HRH planning is now
in the hands of regional governments that resulted in diverse funding and no attention
was given to these challenges in the regions. Critical shortage of HRH due to inadequate
PUBLIC HEALTH
with mismatches between production, demand and supply, mal-distribution and
remuneration in rural, urban and remote areas. The decentralization of health system in
Indonesia is the main reason that the country is facing challenges in terms of healthcare
system. The law was enacted in 2001 on local autonomy and that marked the beginning
of decentralization, however, its implementation was different at each level of
government (Pepinsky & Wihardja, 2011). The transferring of autonomy gave districts
more independence in terms of regulation and management of affairs in the health sector.
The line of coordination was ignored at the upper level that did not function as command
line. Although, the central line wanted to control the main line, however, the HRH
situation deteriorated due to decentralization.
As per the 2010 census, Indonesia ranked last among the ten populous countries
with respect to physicians density per 1000 population compared to Russia, United States
and China ranking first, second and fourth respectively. Similarly, Indonesia ranked fifth
in nurse and midwives density (2.04/1000) with United States, Russia, Brazil and Japan
occupying the first four positions (Rokx, 2010). During the years 2000-2012, the number
of nurses, midwives and physicians increased substantially, however, it was not
significant. The increase in health workforce was not enough to meet the needs of the
population in terms of health. Moreover, hospital beds per 1000 population were quite
low as per 2010 census on the global scale (Hoyler et al., 2014).
Decentralization in Indonesia has given the local governments to take up the
direct authority of prioritizing healthcare sectors for development. HRH planning is now
in the hands of regional governments that resulted in diverse funding and no attention
was given to these challenges in the regions. Critical shortage of HRH due to inadequate
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
PUBLIC HEALTH
resources and understaffing is making Indonesia suffer at every level of healthcare
system (Heywood & Choi, 2010). There is acute shortage of health workers in low and
middle-income countries and this scenario is witnessed in Indonesia. There is
understaffing of healthcare professionals that has led to their inequitable distribution that
can be witnessed from the range 10.36 to 53.89 per 100,000 populations as per Indonesia
Heath profile, 2008 (Meliala, Hort & Trisnantoro, 2013). Moreover, HRH also face
challenges in terms of planning, recruitment and healthcare workers retention in the face
of challenging HRH from Indonesia’s neighbouring countries. The quality of care also
deteriorated during these years that are related to lack of effective licensing and oversight
in HRH. Majority of healthcare professionals in the public sector have opted for second
jobs due to lack of adequate wages in this sector.
There are also deficient information in HRH policy development that is
hampering planning and development efforts of policy makers. The average number of
HRH in Indonesia per 1000 population is quite below the threshold level that is important
to achieve the UHC and health-related MDGs. The Indonesian policy emphasizes on
production, recruitment and retention of human resources in various cadres. However,
there is less number of healthcare professionals with poor quality of quality services and
unequal distribution in rural and remote regions as there is lack of deployment policy in
terms of non-financial and financial incentives for the healthcare providers (Efendi,
2012).
These HRH critical shortages impede the progress of Indonesia that can envisage
for health system strengthening so that there is equitable access to lifesaving and essential
primary healthcare services. Furthermore, this shortage poses obstacles for health-related
PUBLIC HEALTH
resources and understaffing is making Indonesia suffer at every level of healthcare
system (Heywood & Choi, 2010). There is acute shortage of health workers in low and
middle-income countries and this scenario is witnessed in Indonesia. There is
understaffing of healthcare professionals that has led to their inequitable distribution that
can be witnessed from the range 10.36 to 53.89 per 100,000 populations as per Indonesia
Heath profile, 2008 (Meliala, Hort & Trisnantoro, 2013). Moreover, HRH also face
challenges in terms of planning, recruitment and healthcare workers retention in the face
of challenging HRH from Indonesia’s neighbouring countries. The quality of care also
deteriorated during these years that are related to lack of effective licensing and oversight
in HRH. Majority of healthcare professionals in the public sector have opted for second
jobs due to lack of adequate wages in this sector.
There are also deficient information in HRH policy development that is
hampering planning and development efforts of policy makers. The average number of
HRH in Indonesia per 1000 population is quite below the threshold level that is important
to achieve the UHC and health-related MDGs. The Indonesian policy emphasizes on
production, recruitment and retention of human resources in various cadres. However,
there is less number of healthcare professionals with poor quality of quality services and
unequal distribution in rural and remote regions as there is lack of deployment policy in
terms of non-financial and financial incentives for the healthcare providers (Efendi,
2012).
These HRH critical shortages impede the progress of Indonesia that can envisage
for health system strengthening so that there is equitable access to lifesaving and essential
primary healthcare services. Furthermore, this shortage poses obstacles for health-related
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
PUBLIC HEALTH
attainment of Millennium Development Goals (MDGs) and Universal Health
Coverage (UHC). Most of the health workforce in Indonesia is concentrated in Java
Island that left rural and remote areas underserved (Utomo, Sucahya & Utami, 2011).
This is the reason that there is an urgency to develop a national health workforce for
Indonesia curbing the HRH program faced by the country.
2.2 Health workforce data profile
Although, there are no appropriate norms to calculate the optimum ratio of healthcare
workers, however, WHO has identified the threshold doctors density of 2.28 per 1,000
population with nurses and midwives ranging from 2.02 to 2.54 (Short, 2016). Indonesia
falls under this threshold and there is lack of 80% coverage of skilled attendance at the
time of delivery, measles immunization and reduction of infant and maternal, mortality
rate for meeting the goals of health-related MDGs (Grewal, 2016). There is unequal
distribution of doctors in Indonesia where there is one doctor for every 3,000 people in
urban areas and one doctor for 22,000 people in rural areas as reported by World Bank
found in Java-Bali, the most populous Indonesian region (Boyle & Plummer, 2017).
According to World Bank 2009, there is only 1 doctor for every 12,000 rural people and
one doctor for every 15,000 people residing in remote areas and one doctor per 2,430
people in urban areas (Anderson et al., 2014). The situation is worse outside Bali where
nurses are less because of voluntary registration. The people in remote and rural areas
rely heavily on health services provided by nurses and were found to be critically short in
the underserved areas.
While looking into the health workforce trends in Indonesia as per 2010 data,
there is an absolute increment in the number of pharmacy practitioners, nurses, midwives,
PUBLIC HEALTH
attainment of Millennium Development Goals (MDGs) and Universal Health
Coverage (UHC). Most of the health workforce in Indonesia is concentrated in Java
Island that left rural and remote areas underserved (Utomo, Sucahya & Utami, 2011).
This is the reason that there is an urgency to develop a national health workforce for
Indonesia curbing the HRH program faced by the country.
2.2 Health workforce data profile
Although, there are no appropriate norms to calculate the optimum ratio of healthcare
workers, however, WHO has identified the threshold doctors density of 2.28 per 1,000
population with nurses and midwives ranging from 2.02 to 2.54 (Short, 2016). Indonesia
falls under this threshold and there is lack of 80% coverage of skilled attendance at the
time of delivery, measles immunization and reduction of infant and maternal, mortality
rate for meeting the goals of health-related MDGs (Grewal, 2016). There is unequal
distribution of doctors in Indonesia where there is one doctor for every 3,000 people in
urban areas and one doctor for 22,000 people in rural areas as reported by World Bank
found in Java-Bali, the most populous Indonesian region (Boyle & Plummer, 2017).
According to World Bank 2009, there is only 1 doctor for every 12,000 rural people and
one doctor for every 15,000 people residing in remote areas and one doctor per 2,430
people in urban areas (Anderson et al., 2014). The situation is worse outside Bali where
nurses are less because of voluntary registration. The people in remote and rural areas
rely heavily on health services provided by nurses and were found to be critically short in
the underserved areas.
While looking into the health workforce trends in Indonesia as per 2010 data,
there is an absolute increment in the number of pharmacy practitioners, nurses, midwives,
8
PUBLIC HEALTH
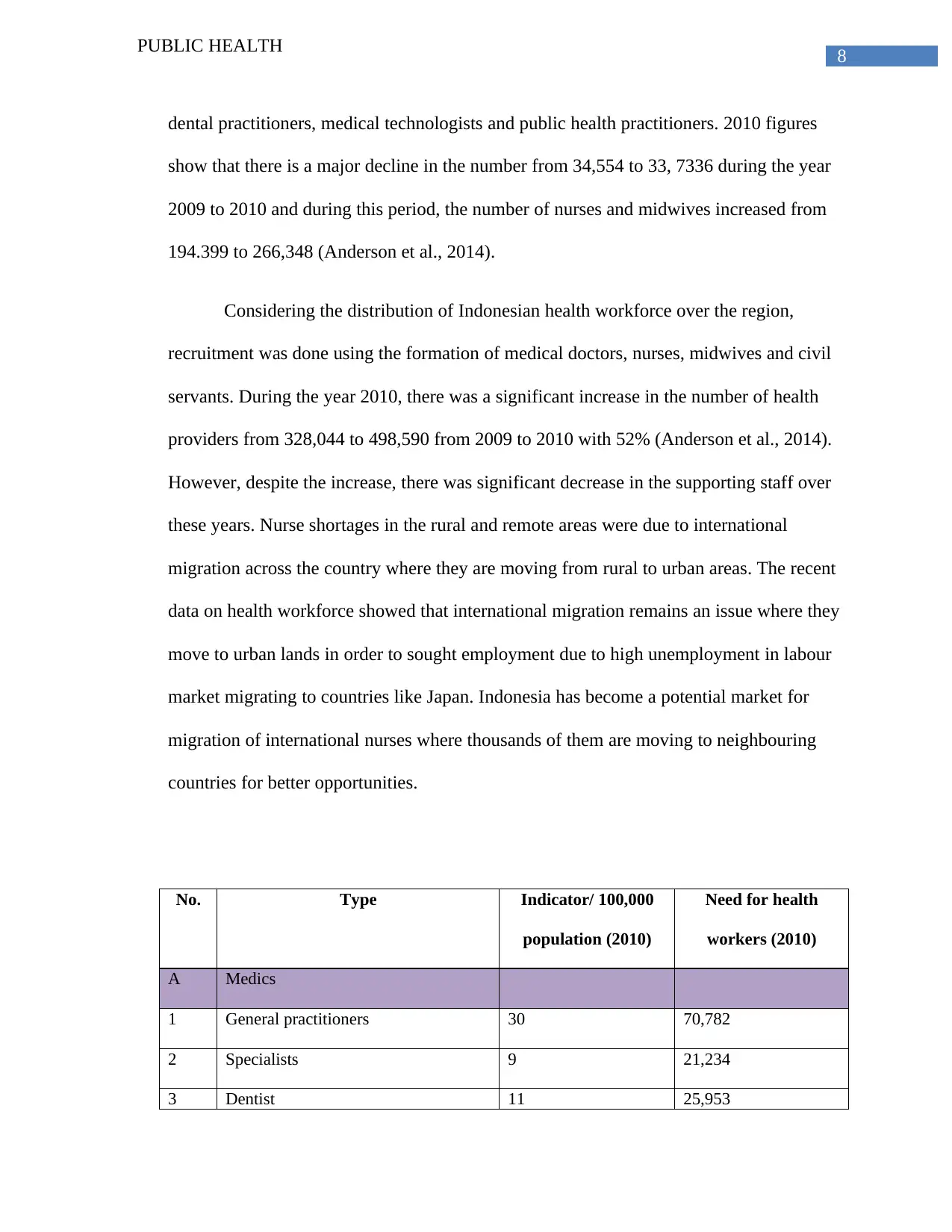
dental practitioners, medical technologists and public health practitioners. 2010 figures
show that there is a major decline in the number from 34,554 to 33, 7336 during the year
2009 to 2010 and during this period, the number of nurses and midwives increased from
194.399 to 266,348 (Anderson et al., 2014).
Considering the distribution of Indonesian health workforce over the region,
recruitment was done using the formation of medical doctors, nurses, midwives and civil
servants. During the year 2010, there was a significant increase in the number of health
providers from 328,044 to 498,590 from 2009 to 2010 with 52% (Anderson et al., 2014).
However, despite the increase, there was significant decrease in the supporting staff over
these years. Nurse shortages in the rural and remote areas were due to international
migration across the country where they are moving from rural to urban areas. The recent
data on health workforce showed that international migration remains an issue where they
move to urban lands in order to sought employment due to high unemployment in labour
market migrating to countries like Japan. Indonesia has become a potential market for
migration of international nurses where thousands of them are moving to neighbouring
countries for better opportunities.
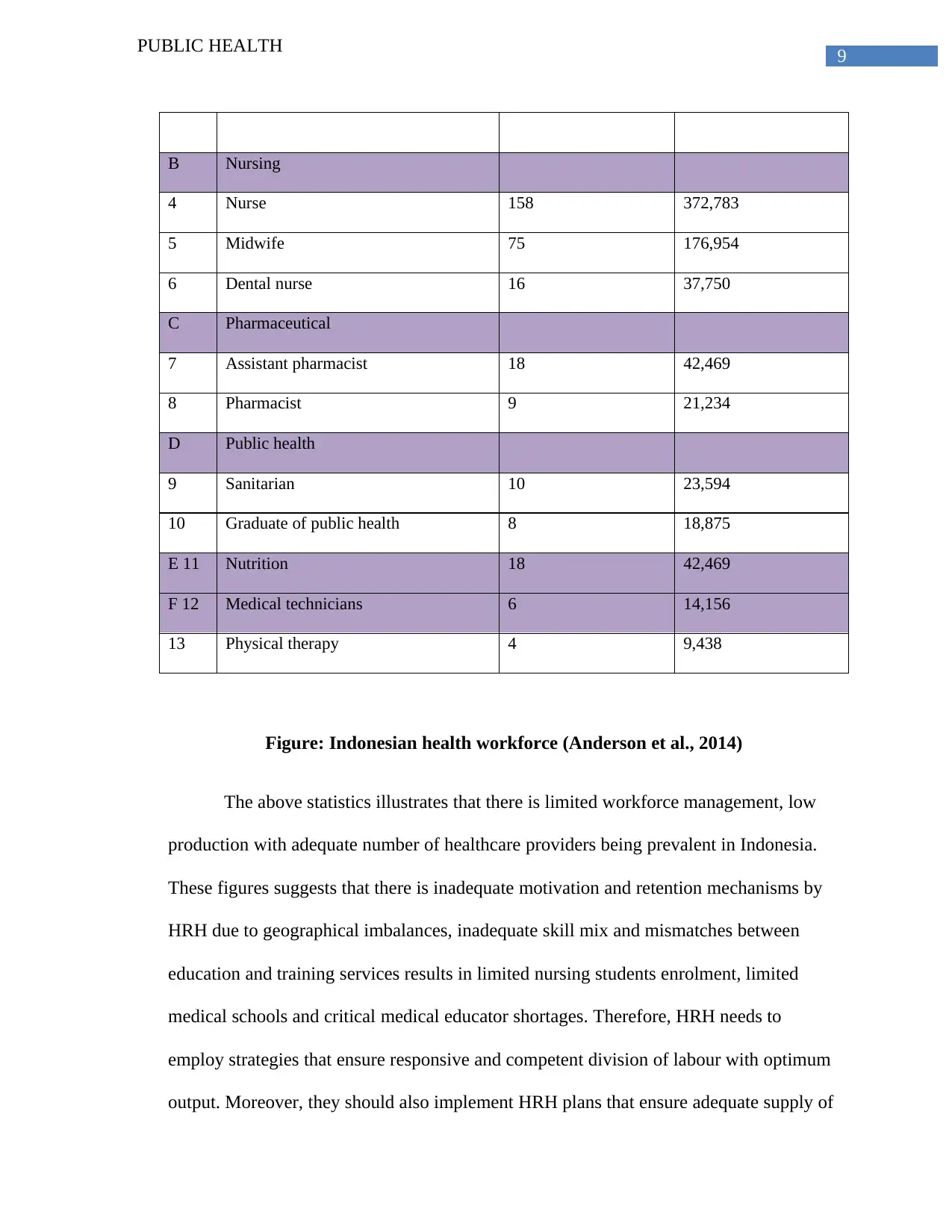
No. Type Indicator/ 100,000
population (2010)
Need for health
workers (2010)
A Medics
1 General practitioners 30 70,782
2 Specialists 9 21,234
3 Dentist 11 25,953
PUBLIC HEALTH
dental practitioners, medical technologists and public health practitioners. 2010 figures
show that there is a major decline in the number from 34,554 to 33, 7336 during the year
2009 to 2010 and during this period, the number of nurses and midwives increased from
194.399 to 266,348 (Anderson et al., 2014).
Considering the distribution of Indonesian health workforce over the region,
recruitment was done using the formation of medical doctors, nurses, midwives and civil
servants. During the year 2010, there was a significant increase in the number of health
providers from 328,044 to 498,590 from 2009 to 2010 with 52% (Anderson et al., 2014).
However, despite the increase, there was significant decrease in the supporting staff over
these years. Nurse shortages in the rural and remote areas were due to international
migration across the country where they are moving from rural to urban areas. The recent
data on health workforce showed that international migration remains an issue where they
move to urban lands in order to sought employment due to high unemployment in labour
market migrating to countries like Japan. Indonesia has become a potential market for
migration of international nurses where thousands of them are moving to neighbouring
countries for better opportunities.
No. Type Indicator/ 100,000
population (2010)
Need for health
workers (2010)
A Medics
1 General practitioners 30 70,782
2 Specialists 9 21,234
3 Dentist 11 25,953
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
PUBLIC HEALTH
B Nursing
4 Nurse 158 372,783
5 Midwife 75 176,954
6 Dental nurse 16 37,750
C Pharmaceutical
7 Assistant pharmacist 18 42,469
8 Pharmacist 9 21,234
D Public health
9 Sanitarian 10 23,594
10 Graduate of public health 8 18,875
E 11 Nutrition 18 42,469
F 12 Medical technicians 6 14,156
13 Physical therapy 4 9,438
Figure: Indonesian health workforce (Anderson et al., 2014)
The above statistics illustrates that there is limited workforce management, low
production with adequate number of healthcare providers being prevalent in Indonesia.
These figures suggests that there is inadequate motivation and retention mechanisms by
HRH due to geographical imbalances, inadequate skill mix and mismatches between
education and training services results in limited nursing students enrolment, limited
medical schools and critical medical educator shortages. Therefore, HRH needs to
employ strategies that ensure responsive and competent division of labour with optimum
output. Moreover, they should also implement HRH plans that ensure adequate supply of
PUBLIC HEALTH
B Nursing
4 Nurse 158 372,783
5 Midwife 75 176,954
6 Dental nurse 16 37,750
C Pharmaceutical
7 Assistant pharmacist 18 42,469
8 Pharmacist 9 21,234
D Public health
9 Sanitarian 10 23,594
10 Graduate of public health 8 18,875
E 11 Nutrition 18 42,469
F 12 Medical technicians 6 14,156
13 Physical therapy 4 9,438
Figure: Indonesian health workforce (Anderson et al., 2014)
The above statistics illustrates that there is limited workforce management, low
production with adequate number of healthcare providers being prevalent in Indonesia.
These figures suggests that there is inadequate motivation and retention mechanisms by
HRH due to geographical imbalances, inadequate skill mix and mismatches between
education and training services results in limited nursing students enrolment, limited
medical schools and critical medical educator shortages. Therefore, HRH needs to
employ strategies that ensure responsive and competent division of labour with optimum
output. Moreover, they should also implement HRH plans that ensure adequate supply of
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
PUBLIC HEALTH
labour with proper balance between production, demand and supply in order to improve
distribution and performance of the existing health workforce in Indonesia.
3. Health workforce plan
The health workforce plan in Indonesia is aimed challenging the decentralization as it has
hindered human resources development in the health workforce. There is improvement
needed for dividing tasks and for the sound functioning between central and local
government. This health workforce plan is aimed at improving the HRH condition, rural
services through community approach that focuses on offering quality healthcare services
and extension of healthcare workers to outreach to the rural and remote areas. This HRH
plan would be beneficial in scaling up healthcare providers in offering clinical services to
the regional and zonal levels. Most importantly, this plan is aimed at increasing the health
workforce as the current statistics shows that there is a rising demand for them in the
health services. Concisely, this plan aims to improve the healthcare staffs including,
physicians, nurses, midwives and other medical officials. Therefore, the following
recommendations would be helpful in curbing the problem of international migration
entailing a road map for the avenues in a way where the Indonesian health workforce can
address the problems.
3.1 Education, Skills and training
Indonesia is at risk for international migration especially to Japan and they need to do
more in prioritizing investments in education and training. Education models need to shift away
from specializations and move towards building of lifelong relevant competencies at the local
level. Geographical inequalities need to be addressed and provide opportunities for strengthening
PUBLIC HEALTH
labour with proper balance between production, demand and supply in order to improve
distribution and performance of the existing health workforce in Indonesia.
3. Health workforce plan
The health workforce plan in Indonesia is aimed challenging the decentralization as it has
hindered human resources development in the health workforce. There is improvement
needed for dividing tasks and for the sound functioning between central and local
government. This health workforce plan is aimed at improving the HRH condition, rural
services through community approach that focuses on offering quality healthcare services
and extension of healthcare workers to outreach to the rural and remote areas. This HRH
plan would be beneficial in scaling up healthcare providers in offering clinical services to
the regional and zonal levels. Most importantly, this plan is aimed at increasing the health
workforce as the current statistics shows that there is a rising demand for them in the
health services. Concisely, this plan aims to improve the healthcare staffs including,
physicians, nurses, midwives and other medical officials. Therefore, the following
recommendations would be helpful in curbing the problem of international migration
entailing a road map for the avenues in a way where the Indonesian health workforce can
address the problems.
3.1 Education, Skills and training
Indonesia is at risk for international migration especially to Japan and they need to do
more in prioritizing investments in education and training. Education models need to shift away
from specializations and move towards building of lifelong relevant competencies at the local
level. Geographical inequalities need to be addressed and provide opportunities for strengthening
11
PUBLIC HEALTH
youth education for successful employment in the health sector. For this, the government needs
to scale up high quality, transformative and lifelong learning for skilled workers who match the
needs of the population and work to their best potential (Kurniati et al., 2015).
3.2 Job creation
There is an urgency to develop the current Indonesian labor market for fostering the
demand for a sustainable and population-centered health workforce. There is need for
government policies that address the issues in labor market. The right mix of skills is required for
fulfilling the health needs of the population. The government should stimulate investments for
the creation of decent jobs in the health sector especially for women and youth with right skills at
right places in right numbers.
3.3 Women and gender rights
The health sector is a growing platform for women employment and gender equality. In
the healthcare sector, women are the main care providers including conflict settings and
humanitarian crises. However, there are prevailing gender biases in this sector that remains a big
challenge that need to be addressed. To curb the problem of gender inequality, there should be
maximization of women participation in the economy and fostering empowerment. This can be
achieved through leadership that addressed education inequalities, gender biases in the health
labor market, and tackle concerns regarding gender in the reform processes.
3.4 Technology
The rapidly changing phase of technology is already changing the nature of healthcare
services. Information and communication technology (ICT) is changing and there is emergence
of new cadres of healthcare providers. In such cases, digital technologies can offer opportunities
PUBLIC HEALTH
youth education for successful employment in the health sector. For this, the government needs
to scale up high quality, transformative and lifelong learning for skilled workers who match the
needs of the population and work to their best potential (Kurniati et al., 2015).
3.2 Job creation
There is an urgency to develop the current Indonesian labor market for fostering the
demand for a sustainable and population-centered health workforce. There is need for
government policies that address the issues in labor market. The right mix of skills is required for
fulfilling the health needs of the population. The government should stimulate investments for
the creation of decent jobs in the health sector especially for women and youth with right skills at
right places in right numbers.
3.3 Women and gender rights
The health sector is a growing platform for women employment and gender equality. In
the healthcare sector, women are the main care providers including conflict settings and
humanitarian crises. However, there are prevailing gender biases in this sector that remains a big
challenge that need to be addressed. To curb the problem of gender inequality, there should be
maximization of women participation in the economy and fostering empowerment. This can be
achieved through leadership that addressed education inequalities, gender biases in the health
labor market, and tackle concerns regarding gender in the reform processes.
3.4 Technology
The rapidly changing phase of technology is already changing the nature of healthcare
services. Information and communication technology (ICT) is changing and there is emergence
of new cadres of healthcare providers. In such cases, digital technologies can offer opportunities
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 21
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.