Comprehensive Analysis of Pulmonary Function Test Case Studies
VerifiedAdded on 2022/10/06
|13
|2957
|18
Report
AI Summary
This report provides a detailed analysis of three pulmonary function test case studies. Each case study involves the interpretation of spirometry results, including FEV1, FVC, and TLCO values, to diagnose respiratory conditions. The first case study identifies chronic obstructive pulmonary disease (COPD) through an obstructive pattern and pulmonary fibrosis, evidenced by a reduced FEV1/FVC ratio, low TLCO, and reduced alveolar volume. The second case study reveals a restrictive lung disorder, characterized by a high FEV1/FVC ratio, reduced vital capacity, and decreased total lung capacity and functional residual capacity. The third case study indicates normal spirometry results but suggests a problem with alveolar capillary membrane due to a low TLCO value and increased alveolar volume. The report explains the underlying physiological disturbances and provides clinical interpretations of the test results, integrating the results from the various tests conducted.
Running Head: LUNG FUNCTION TEST
LUNG FUNCTION TEST
Name of the Student
Name of the University
Author Note
LUNG FUNCTION TEST
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
Running Head: LUNG FUNCTION TEST
Table of Contents
Case Study 1:..............................................................................................................................2
Case Study 2:..............................................................................................................................4
Case Study 3:..............................................................................................................................6
References:.................................................................................................................................8
Running Head: LUNG FUNCTION TEST
Table of Contents
Case Study 1:..............................................................................................................................2
Case Study 2:..............................................................................................................................4
Case Study 3:..............................................................................................................................6
References:.................................................................................................................................8
2
Running Head: LUNG FUNCTION TEST
Case Study 1:
This case study is based on a lung function test. The tests provide the results as
measurements of lung volumes, co transfer factors, arterial gases present in blood and
spirometry assays. Results were obtained as stated in the laboratory report, and the diseased
condition will be interpreted from those reports. The disease can either be obstructive,
restrictive or a mixture of the two conditions. Obstructive condition is characterised by
obstruction of the airways, restrictive is characterised by prevention of lung expansion with
air and combination of the above two conditions also occur (Negewo, McDonald & Gibson,
2015). Spirometry can be used to measure the diseased condition by repeated and acceptable
states (Overstreet et al., 2017).
A brief description of the report states the TLCO (Transfer factor for carbon monoxide),
FEV1 (Forced Expiratory Volume), FRC (Functional Residual Capacity) and the pressures of
various gases in the lungs. Other measurements have also been done in order to diagnose lung
disease. FEV stands for forced respiratory rate. This factor is the total amount of air that can
be exhaled out of the lungs in one second (Vanoirbeek et al., 2016). FVC is the amount of air,
that is exhaled out during the test of FEV (Shah & Choudhury, 2015). FEV1/FVC ratio will
be used to identify the lung disease in this case. This ratio will be reduced in the case of
obstructive lung disease (DeCato et al., 2017). According to the National Institute of Cholera
for Clinical Excellence, the value of the ratio should be less than 0.7 for obstructive lung
disease (Quanjer, Steenbruggen & Berg, 2016). In other words, this value is stated to be
seventy-five per cent less than the average value.
In this case, the FEV1/FVC ratio is calculated to be ( 0.44
1.16 ), which equates to a value
of 0.3. This value is far less than 0.7 and is also 75% less than the standard value of 1.44.
Running Head: LUNG FUNCTION TEST
Case Study 1:
This case study is based on a lung function test. The tests provide the results as
measurements of lung volumes, co transfer factors, arterial gases present in blood and
spirometry assays. Results were obtained as stated in the laboratory report, and the diseased
condition will be interpreted from those reports. The disease can either be obstructive,
restrictive or a mixture of the two conditions. Obstructive condition is characterised by
obstruction of the airways, restrictive is characterised by prevention of lung expansion with
air and combination of the above two conditions also occur (Negewo, McDonald & Gibson,
2015). Spirometry can be used to measure the diseased condition by repeated and acceptable
states (Overstreet et al., 2017).
A brief description of the report states the TLCO (Transfer factor for carbon monoxide),
FEV1 (Forced Expiratory Volume), FRC (Functional Residual Capacity) and the pressures of
various gases in the lungs. Other measurements have also been done in order to diagnose lung
disease. FEV stands for forced respiratory rate. This factor is the total amount of air that can
be exhaled out of the lungs in one second (Vanoirbeek et al., 2016). FVC is the amount of air,
that is exhaled out during the test of FEV (Shah & Choudhury, 2015). FEV1/FVC ratio will
be used to identify the lung disease in this case. This ratio will be reduced in the case of
obstructive lung disease (DeCato et al., 2017). According to the National Institute of Cholera
for Clinical Excellence, the value of the ratio should be less than 0.7 for obstructive lung
disease (Quanjer, Steenbruggen & Berg, 2016). In other words, this value is stated to be
seventy-five per cent less than the average value.
In this case, the FEV1/FVC ratio is calculated to be ( 0.44
1.16 ), which equates to a value
of 0.3. This value is far less than 0.7 and is also 75% less than the standard value of 1.44.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
Running Head: LUNG FUNCTION TEST
This proves that the person is having a obstructive lung disease. However, the FVC value
was not abnormal as it had a minimal deviation from the normal value of 1.95. Here the FVC
value was 1.53. Therefore, this condition cannot be tagged under restrictive lung disorder.
TLCO measures the extent by which the oxygen gas passes from the air sacs of the
lungs into the blood (Stanojevic et al., 2016). This value will reduce if the air sacs of the
lungs are obstructed. The TLCO test resulted in a very low value in the case of this patient.
The standard value is stated to be 13.5 ml/min/mm Hg or more. However, in this case, study,
the value has been found to be 5.6 ml/min/mm Hg. This number is an abnormally low value
and can be linked to a diseased condition called chronic obstructive pulmonary disease
(COPD) (Wapeenar et al., 2019). Unusually low values of TLCO are caused by pulmonary
fibrosis in which the lung tissues get scarred (Yanagihara et al., 2019). However, the arterial
blood gas tests were found to be normal, and thus, no more complications can be derived.
Also, it can be found that the alveolar volume (VA) is very less in the case of this patient.
The normal value stated here is more significant than 3.8 L BTPS, whereas the measured
value was 2.8 L BTPS. This condition occurred due to the fact that obstructive lung disease
blocks the alveoli and thus decreases its volume (Graham et al., 2017). This disease could
have been classified as a reversible obstructive disorder. However, this was not possible
because of the absence of the interpreted table format of the graph provided. As per the graph
states, this lung disorder can be called as a reversible obstructive disorder because of the
nature of the curve (Shadduck et al., 2015). The pathophysiology of COPD states that it has
two primary conditions. These conditions are emphysema and chronic bronchitis. A mixed
condition can also be found to have been occurring. As stated before the alveolar volume in
case of this patient is far less the the normal value. This condition proves that he was affected
by the chronic bronchitis in which the airways of the bronchioles get blocked (Kim, 2017).
The airway linings gets inflamed during the chronic bronchitis condition of COPD. However,
Running Head: LUNG FUNCTION TEST
This proves that the person is having a obstructive lung disease. However, the FVC value
was not abnormal as it had a minimal deviation from the normal value of 1.95. Here the FVC
value was 1.53. Therefore, this condition cannot be tagged under restrictive lung disorder.
TLCO measures the extent by which the oxygen gas passes from the air sacs of the
lungs into the blood (Stanojevic et al., 2016). This value will reduce if the air sacs of the
lungs are obstructed. The TLCO test resulted in a very low value in the case of this patient.
The standard value is stated to be 13.5 ml/min/mm Hg or more. However, in this case, study,
the value has been found to be 5.6 ml/min/mm Hg. This number is an abnormally low value
and can be linked to a diseased condition called chronic obstructive pulmonary disease
(COPD) (Wapeenar et al., 2019). Unusually low values of TLCO are caused by pulmonary
fibrosis in which the lung tissues get scarred (Yanagihara et al., 2019). However, the arterial
blood gas tests were found to be normal, and thus, no more complications can be derived.
Also, it can be found that the alveolar volume (VA) is very less in the case of this patient.
The normal value stated here is more significant than 3.8 L BTPS, whereas the measured
value was 2.8 L BTPS. This condition occurred due to the fact that obstructive lung disease
blocks the alveoli and thus decreases its volume (Graham et al., 2017). This disease could
have been classified as a reversible obstructive disorder. However, this was not possible
because of the absence of the interpreted table format of the graph provided. As per the graph
states, this lung disorder can be called as a reversible obstructive disorder because of the
nature of the curve (Shadduck et al., 2015). The pathophysiology of COPD states that it has
two primary conditions. These conditions are emphysema and chronic bronchitis. A mixed
condition can also be found to have been occurring. As stated before the alveolar volume in
case of this patient is far less the the normal value. This condition proves that he was affected
by the chronic bronchitis in which the airways of the bronchioles get blocked (Kim, 2017).
The airway linings gets inflamed during the chronic bronchitis condition of COPD. However,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
Running Head: LUNG FUNCTION TEST
the decrease in the TLCO values as stated earlier, is also very less than the normal value
(Wapeenar et al., 2019). This condition proves that the person was having pulmonary fibrosis
in which his air sacs of the lungs gets scarred. Therefore the patient was also suffering from
emphysema. Therefore it can be concluded that the lung disorder in this case study was
COPD (chronic obstructive pulmonary disease), a combination of obstructive and
pulmonary fibrosis in lungs.
Running Head: LUNG FUNCTION TEST
the decrease in the TLCO values as stated earlier, is also very less than the normal value
(Wapeenar et al., 2019). This condition proves that the person was having pulmonary fibrosis
in which his air sacs of the lungs gets scarred. Therefore the patient was also suffering from
emphysema. Therefore it can be concluded that the lung disorder in this case study was
COPD (chronic obstructive pulmonary disease), a combination of obstructive and
pulmonary fibrosis in lungs.
5
Running Head: LUNG FUNCTION TEST
Case Study 2:
This case will also be interpreted in the same procedure as the previous case.
However, some changes have been observed here which are just the reverse of the previous
report. Absence of graphical representations of the data collected prevents the interpretation
of reversible and irreversible cases of the disorders.
First comes the FEV1/FVC ratio. This term has been defined in the previous section as a
measure of the amount of air a person can exhale in one second. Here the FEV1/FVC ratio
has been found to be high. This value has been calculated from the data provided.
Normal ratio=1.83
2.53 = 0.72
Ratio for this patient =1.77
2.07 =0.86
Therefore it can be observed that a higher value of 0.86 has been found in the case of this
study. A higher value indicates restrictive ventilatory defect associated with lung disorder
(Jones, Jones & Killian, 2016). The pathophysiology of the disease states that, restrictive lung
disorder prevents the lungs to expand at its full volume. This condition makes the patient
harder to inhale fully. The structure of parenchyma cells occurs during this disease. This
alteration in structure causes the lung volume to decrease and makes the person unable to
inhale properly. This situation is accompanied by a fast decrease in the vital capacity of the
lungs. Vital capacity also becomes smaller in this case. This is also evident from the report
where the vital capacity of the lungs is stated to be 2.10. However, the normal value is found
to be 2.53. Thus there is a reduction in the vital capacity of the lungs. This condition has
arisen due to the restrictive lung disorder in case of this case study.
Running Head: LUNG FUNCTION TEST
Case Study 2:
This case will also be interpreted in the same procedure as the previous case.
However, some changes have been observed here which are just the reverse of the previous
report. Absence of graphical representations of the data collected prevents the interpretation
of reversible and irreversible cases of the disorders.
First comes the FEV1/FVC ratio. This term has been defined in the previous section as a
measure of the amount of air a person can exhale in one second. Here the FEV1/FVC ratio
has been found to be high. This value has been calculated from the data provided.
Normal ratio=1.83
2.53 = 0.72
Ratio for this patient =1.77
2.07 =0.86
Therefore it can be observed that a higher value of 0.86 has been found in the case of this
study. A higher value indicates restrictive ventilatory defect associated with lung disorder
(Jones, Jones & Killian, 2016). The pathophysiology of the disease states that, restrictive lung
disorder prevents the lungs to expand at its full volume. This condition makes the patient
harder to inhale fully. The structure of parenchyma cells occurs during this disease. This
alteration in structure causes the lung volume to decrease and makes the person unable to
inhale properly. This situation is accompanied by a fast decrease in the vital capacity of the
lungs. Vital capacity also becomes smaller in this case. This is also evident from the report
where the vital capacity of the lungs is stated to be 2.10. However, the normal value is found
to be 2.53. Thus there is a reduction in the vital capacity of the lungs. This condition has
arisen due to the restrictive lung disorder in case of this case study.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
Running Head: LUNG FUNCTION TEST
TLCO also plays a significant role in this restrictive lung disorder. In this case study,
the TLCO value has been found to be elevated. However, it stays near the normal range in
case of this restrictive condition.
The alveolar volume has been found to be very less as compared to the normal
condition. The normal value provided here is greater than 4.9, whereas the measured value
for the patient is 3.7 L BTPS. Lower alveolar volume indicates that the lungs cannot perform
well or cannot transfer enough oxygen to the blood as it can adequately expand.
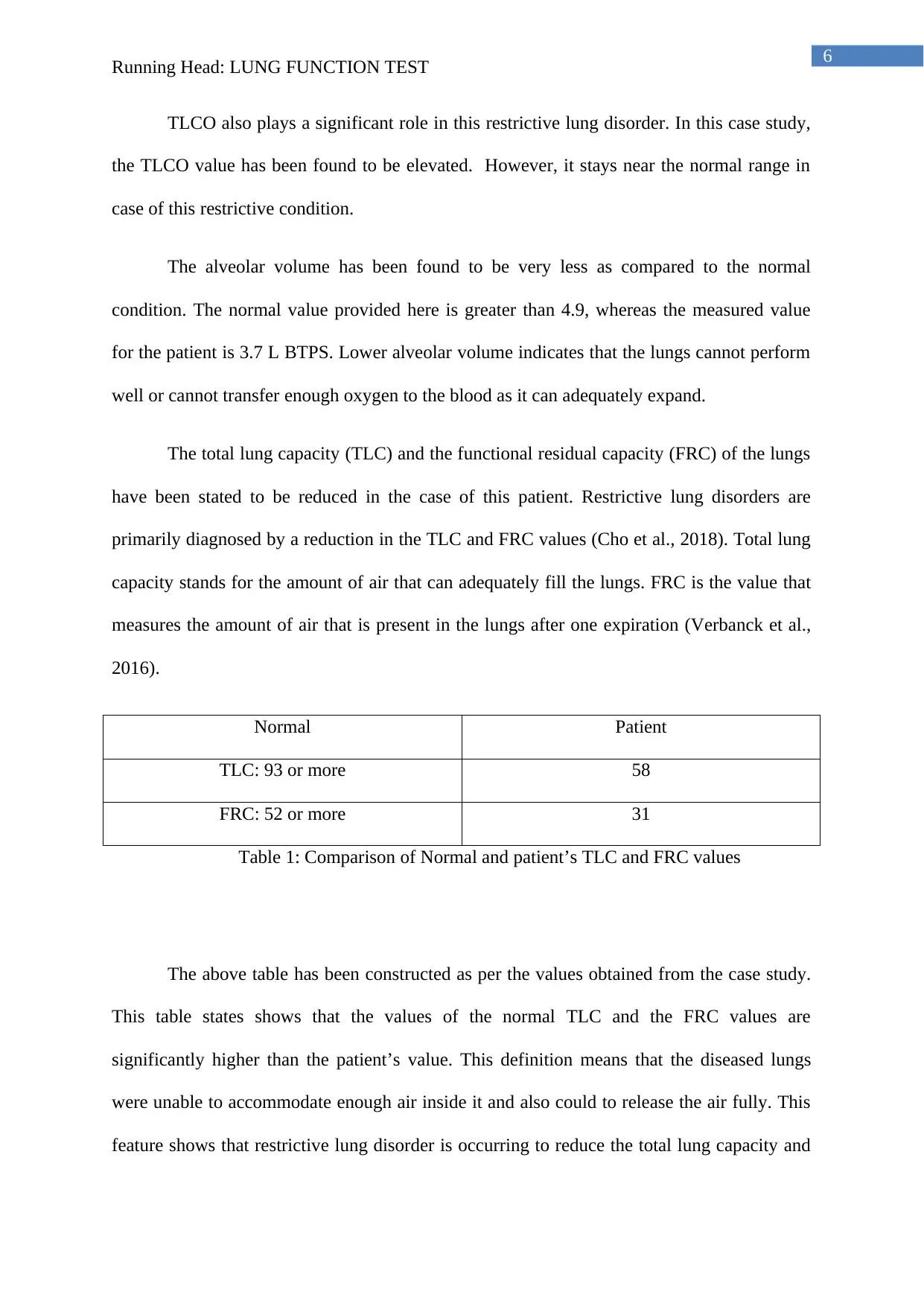
The total lung capacity (TLC) and the functional residual capacity (FRC) of the lungs
have been stated to be reduced in the case of this patient. Restrictive lung disorders are
primarily diagnosed by a reduction in the TLC and FRC values (Cho et al., 2018). Total lung
capacity stands for the amount of air that can adequately fill the lungs. FRC is the value that
measures the amount of air that is present in the lungs after one expiration (Verbanck et al.,
2016).
Normal Patient
TLC: 93 or more 58
FRC: 52 or more 31
Table 1: Comparison of Normal and patient’s TLC and FRC values
The above table has been constructed as per the values obtained from the case study.
This table states shows that the values of the normal TLC and the FRC values are
significantly higher than the patient’s value. This definition means that the diseased lungs
were unable to accommodate enough air inside it and also could to release the air fully. This
feature shows that restrictive lung disorder is occurring to reduce the total lung capacity and
Running Head: LUNG FUNCTION TEST
TLCO also plays a significant role in this restrictive lung disorder. In this case study,
the TLCO value has been found to be elevated. However, it stays near the normal range in
case of this restrictive condition.
The alveolar volume has been found to be very less as compared to the normal
condition. The normal value provided here is greater than 4.9, whereas the measured value
for the patient is 3.7 L BTPS. Lower alveolar volume indicates that the lungs cannot perform
well or cannot transfer enough oxygen to the blood as it can adequately expand.
The total lung capacity (TLC) and the functional residual capacity (FRC) of the lungs
have been stated to be reduced in the case of this patient. Restrictive lung disorders are
primarily diagnosed by a reduction in the TLC and FRC values (Cho et al., 2018). Total lung
capacity stands for the amount of air that can adequately fill the lungs. FRC is the value that
measures the amount of air that is present in the lungs after one expiration (Verbanck et al.,
2016).
Normal Patient
TLC: 93 or more 58
FRC: 52 or more 31
Table 1: Comparison of Normal and patient’s TLC and FRC values
The above table has been constructed as per the values obtained from the case study.
This table states shows that the values of the normal TLC and the FRC values are
significantly higher than the patient’s value. This definition means that the diseased lungs
were unable to accommodate enough air inside it and also could to release the air fully. This
feature shows that restrictive lung disorder is occurring to reduce the total lung capacity and
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

7
Running Head: LUNG FUNCTION TEST
the functional residual capacity. As a result, from all the above statements and data provided,
it can be concluded that the patient is suffering from restrictive lung disorder associated with
ventilator problem.
Running Head: LUNG FUNCTION TEST
the functional residual capacity. As a result, from all the above statements and data provided,
it can be concluded that the patient is suffering from restrictive lung disorder associated with
ventilator problem.
8
Running Head: LUNG FUNCTION TEST
Case Study 3:
In the above case study, the data provided seems to be normal in the spiromentry
report. Obstructive or restrictive lung disorders did not occur in case of this patient. This is
because, the spirometry results shows no obstruction or retention disorder in lungs.
The normal value for the ratio of FEV1/FVC is equal to 0.6, as found from the case study
report provided. The calculated amount is also found to be around 0.60. This value is lower
than 0.7 or seventy per cent. However, no further implications are present for the occurrence
of obstructive or restrictive lung disorder. Further interpretation will be made by using TLCO
values.
The standard TLCO value as per the case study is more than 15.1 ml/min/mm Hg. However,
the TLCO value for the patient is 11,7 ml/min/mm Hg. This proves that the TLCO value
calculated for the patient is less than the standard value. This low TLCO value proves that the
patient has an problem in the alveolar capillary membrane. Carbon monoxide used for this
test could not be transferred by the patient’s blood. The above statement is well justified by
the patients TLCO values. The alveolar volume (VA) was found to be higher than the normal
value in this case study. Therefore it can be stated that, the capillary membranes of the
alveolar ducts have expanded than their normal configuration.
The graphical representations of the paper state that after the volume time curve
before the tests states a curve with abrupt slopes. This slope was found to be normal in the
second curve after the tests were performed. In this curve, no part of the curve was found to
be in the negative coordinate (-,-) of the graph. The graph for the third trial given in the case
study shows that the slope for the flow-volume curve was attaining a normal nature from the
abrupt one found previously. A reversible nature of the disorder is proved when the curve has
Running Head: LUNG FUNCTION TEST
Case Study 3:
In the above case study, the data provided seems to be normal in the spiromentry
report. Obstructive or restrictive lung disorders did not occur in case of this patient. This is
because, the spirometry results shows no obstruction or retention disorder in lungs.
The normal value for the ratio of FEV1/FVC is equal to 0.6, as found from the case study
report provided. The calculated amount is also found to be around 0.60. This value is lower
than 0.7 or seventy per cent. However, no further implications are present for the occurrence
of obstructive or restrictive lung disorder. Further interpretation will be made by using TLCO
values.
The standard TLCO value as per the case study is more than 15.1 ml/min/mm Hg. However,
the TLCO value for the patient is 11,7 ml/min/mm Hg. This proves that the TLCO value
calculated for the patient is less than the standard value. This low TLCO value proves that the
patient has an problem in the alveolar capillary membrane. Carbon monoxide used for this
test could not be transferred by the patient’s blood. The above statement is well justified by
the patients TLCO values. The alveolar volume (VA) was found to be higher than the normal
value in this case study. Therefore it can be stated that, the capillary membranes of the
alveolar ducts have expanded than their normal configuration.
The graphical representations of the paper state that after the volume time curve
before the tests states a curve with abrupt slopes. This slope was found to be normal in the
second curve after the tests were performed. In this curve, no part of the curve was found to
be in the negative coordinate (-,-) of the graph. The graph for the third trial given in the case
study shows that the slope for the flow-volume curve was attaining a normal nature from the
abrupt one found previously. A reversible nature of the disorder is proved when the curve has
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
Running Head: LUNG FUNCTION TEST
a position in the (-,-) coordinate of a graph. However, the nature of the curves did not provide
any instances of a reversible condition of the disease. The pathophysiology of this disorder
related to alveolar disorder is associated with the increase in the permeability of the alveolar
membranes. This causes increase in gas exchange rates higher than the normal value.
Therefore a respiratory imbalance occurs and the ratio of oxygen to carbon dioxide amounts
are disturbed (Stromberg et al., 2015). This condition is evident in the case of this case study
in which the graphs show a rise in the peak suddenly.
Running Head: LUNG FUNCTION TEST
a position in the (-,-) coordinate of a graph. However, the nature of the curves did not provide
any instances of a reversible condition of the disease. The pathophysiology of this disorder
related to alveolar disorder is associated with the increase in the permeability of the alveolar
membranes. This causes increase in gas exchange rates higher than the normal value.
Therefore a respiratory imbalance occurs and the ratio of oxygen to carbon dioxide amounts
are disturbed (Stromberg et al., 2015). This condition is evident in the case of this case study
in which the graphs show a rise in the peak suddenly.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
Running Head: LUNG FUNCTION TEST
References:
Cho, R. J., Wyrzos, K., Corazalla, E. O., & Kim, H. (2018). To Determine Which Pulmonary
Function Parameters Should Be Considered for Grading Severity of Restrictive Lung
Disease. In A43. ILD SCIENTIFIC ABSTRACTS: GENERAL (pp. A1701-A1701).
American Thoracic Society.
DeCato, T. W., Hegewald, M. J., Linares, O., Collingridge, D. S., & Morris, A. H. (2017).
Correlation Between Fev1/FVC Ratio, Total Lung Capacity, And Single-Breath
Diffusing Capacity. In A76. WHAT'S IN THE TOOL BOX TO ASSESS LUNG
FUNCTION (pp. A2516-A2516). American Thoracic Society.
Graham, B. L., Brusasco, V., Burgos, F., Cooper, B. G., Jensen, R., Kendrick, A., ... &
Wanger, J. (2017). DLCO: adjust for lung volume, standardised reporting and
interpretation. European Respiratory Journal, 50(2), 1701144.
Jones, G. L., Jones, N. L., & Killian, K. J. (2016). The Contribution Of Ventilatory Capacity,
Gas Transfer Capacity And The Presence Of Airflow Obstruction To Limitations In
Maximum Power Output. In B56. THE ART AND SCIENCE OF REHABILITATION:
NOVEL TREATMENTS AND OUTCOMES IN PULMONARY
REHABILITATION (pp. A4001-A4001). American Thoracic Society.
Karimi-Shah, B. A., & Chowdhury, B. A. (2015). Forced vital capacity in idiopathic
pulmonary fibrosis—FDA review of pirfenidone and nintedanib. New England
Journal of Medicine, 372(13), 1189-1191.
Kim, E. K. (2017). Pathophysiology of COPD. In COPD (pp. 57-63). Springer, Berlin,
Heidelberg.
Running Head: LUNG FUNCTION TEST
References:
Cho, R. J., Wyrzos, K., Corazalla, E. O., & Kim, H. (2018). To Determine Which Pulmonary
Function Parameters Should Be Considered for Grading Severity of Restrictive Lung
Disease. In A43. ILD SCIENTIFIC ABSTRACTS: GENERAL (pp. A1701-A1701).
American Thoracic Society.
DeCato, T. W., Hegewald, M. J., Linares, O., Collingridge, D. S., & Morris, A. H. (2017).
Correlation Between Fev1/FVC Ratio, Total Lung Capacity, And Single-Breath
Diffusing Capacity. In A76. WHAT'S IN THE TOOL BOX TO ASSESS LUNG
FUNCTION (pp. A2516-A2516). American Thoracic Society.
Graham, B. L., Brusasco, V., Burgos, F., Cooper, B. G., Jensen, R., Kendrick, A., ... &
Wanger, J. (2017). DLCO: adjust for lung volume, standardised reporting and
interpretation. European Respiratory Journal, 50(2), 1701144.
Jones, G. L., Jones, N. L., & Killian, K. J. (2016). The Contribution Of Ventilatory Capacity,
Gas Transfer Capacity And The Presence Of Airflow Obstruction To Limitations In
Maximum Power Output. In B56. THE ART AND SCIENCE OF REHABILITATION:
NOVEL TREATMENTS AND OUTCOMES IN PULMONARY
REHABILITATION (pp. A4001-A4001). American Thoracic Society.
Karimi-Shah, B. A., & Chowdhury, B. A. (2015). Forced vital capacity in idiopathic
pulmonary fibrosis—FDA review of pirfenidone and nintedanib. New England
Journal of Medicine, 372(13), 1189-1191.
Kim, E. K. (2017). Pathophysiology of COPD. In COPD (pp. 57-63). Springer, Berlin,
Heidelberg.
11
Running Head: LUNG FUNCTION TEST
Negewo, N. A., McDonald, V. M., & Gibson, P. G. (2015). Comorbidity in chronic
obstructive pulmonary disease. Respiratory investigation, 53(6), 249-258.
Overstreet, B. S., Bassett, J. D., Crouter, S. E., Rider, B. C., & Parr, B. B. (2017). Portable
open-circuit spirometry systems. The Journal of sports medicine and physical
fitness, 57(3), 227-237.
Quanjer, P. H., Steenbruggen, I., & van den Berg, J. W. (2016). Diagnosis of airways
obstruction should be based on symptoms and an FEV1/FVC ratio below the lower
limit of normal. Bmj, 352, i397.
Shadduck, J. H. (2015). U.S. Patent No. 9,113,944. Washington, DC: U.S. Patent and
Trademark Office.
Stanojevic, S., Grham, B., Cooper, B., Thompson, B., Carter, K., & Hall, G. (2016). Global
lung function initiative: Reference equations for the transfer factor for carbon
monoxide (TLCO).
Stromberg, S. E., Russell, M. E., & Carlson, C. R. (2015). Diaphragmatic breathing and its
effectiveness for the management of motion sickness. Aerospace medicine and human
performance, 86(5), 452-457.
van Dijk, W., Tan, W., Li, P., Guo, B., Li, S., Benedetti, A., ... & CanCOLD Study Group.
(2015). Clinical relevance of fixed ratio vs lower limit of normal of FEV1/FVC in
COPD: patient-reported outcomes from the CanCOLD cohort. The Annals of Family
Medicine, 13(1), 41-48.
Vanoirbeek, J., Maaske, A., Aznar Lopez, C., Pollaris, L., Nemery, B., Hoet, P. H., ... &
Devos, F. (2016). Forced Expiratory Volume (fev) Measurements In Mouse Models
Running Head: LUNG FUNCTION TEST
Negewo, N. A., McDonald, V. M., & Gibson, P. G. (2015). Comorbidity in chronic
obstructive pulmonary disease. Respiratory investigation, 53(6), 249-258.
Overstreet, B. S., Bassett, J. D., Crouter, S. E., Rider, B. C., & Parr, B. B. (2017). Portable
open-circuit spirometry systems. The Journal of sports medicine and physical
fitness, 57(3), 227-237.
Quanjer, P. H., Steenbruggen, I., & van den Berg, J. W. (2016). Diagnosis of airways
obstruction should be based on symptoms and an FEV1/FVC ratio below the lower
limit of normal. Bmj, 352, i397.
Shadduck, J. H. (2015). U.S. Patent No. 9,113,944. Washington, DC: U.S. Patent and
Trademark Office.
Stanojevic, S., Grham, B., Cooper, B., Thompson, B., Carter, K., & Hall, G. (2016). Global
lung function initiative: Reference equations for the transfer factor for carbon
monoxide (TLCO).
Stromberg, S. E., Russell, M. E., & Carlson, C. R. (2015). Diaphragmatic breathing and its
effectiveness for the management of motion sickness. Aerospace medicine and human
performance, 86(5), 452-457.
van Dijk, W., Tan, W., Li, P., Guo, B., Li, S., Benedetti, A., ... & CanCOLD Study Group.
(2015). Clinical relevance of fixed ratio vs lower limit of normal of FEV1/FVC in
COPD: patient-reported outcomes from the CanCOLD cohort. The Annals of Family
Medicine, 13(1), 41-48.
Vanoirbeek, J., Maaske, A., Aznar Lopez, C., Pollaris, L., Nemery, B., Hoet, P. H., ... &
Devos, F. (2016). Forced Expiratory Volume (fev) Measurements In Mouse Models
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.