Addressing Barriers to Quality Service: A Healthcare Case Study
VerifiedAdded on 2020/03/02
|7
|1892
|127
Essay
AI Summary
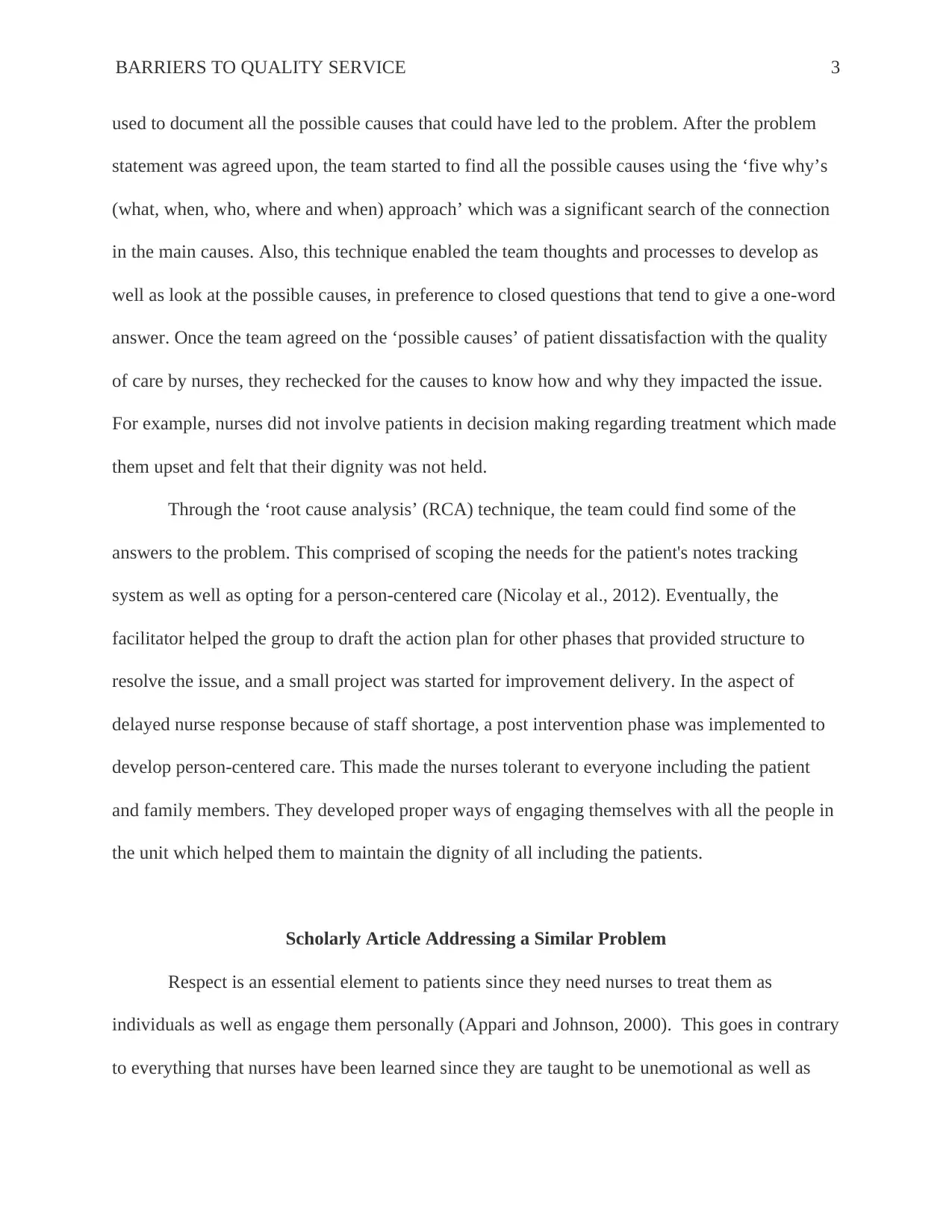
This essay examines the barriers to quality service in a healthcare setting, focusing on patient dissatisfaction with nursing care. It investigates issues such as delayed nurse response due to staff shortages and a perceived lack of respect for patient dignity. The essay details a case study where a healthcare center utilized a fishbone analysis and root cause analysis (RCA) to identify and address the underlying causes of patient concerns. The process involved gathering input from all personnel and patients, employing the 'five whys' approach to uncover connections between causes, and developing an action plan for improvement. The essay references a scholarly article that highlights the importance of patient respect and communication in healthcare, as well as the negative impact of poor communication between doctors and nurses on patient perception. The conclusion emphasizes the value of tools like fishbone diagrams and RCA in improving healthcare quality, safety, and the professional development of healthcare providers. The essay also discusses the importance of person-centered care and the role of healthcare providers in the RCA process.

1 out of 7
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.