Evaluation of a Randomized Controlled Trial using JBI Checklist
VerifiedAdded on 2022/08/11
|4
|1598
|272
Homework Assignment
AI Summary
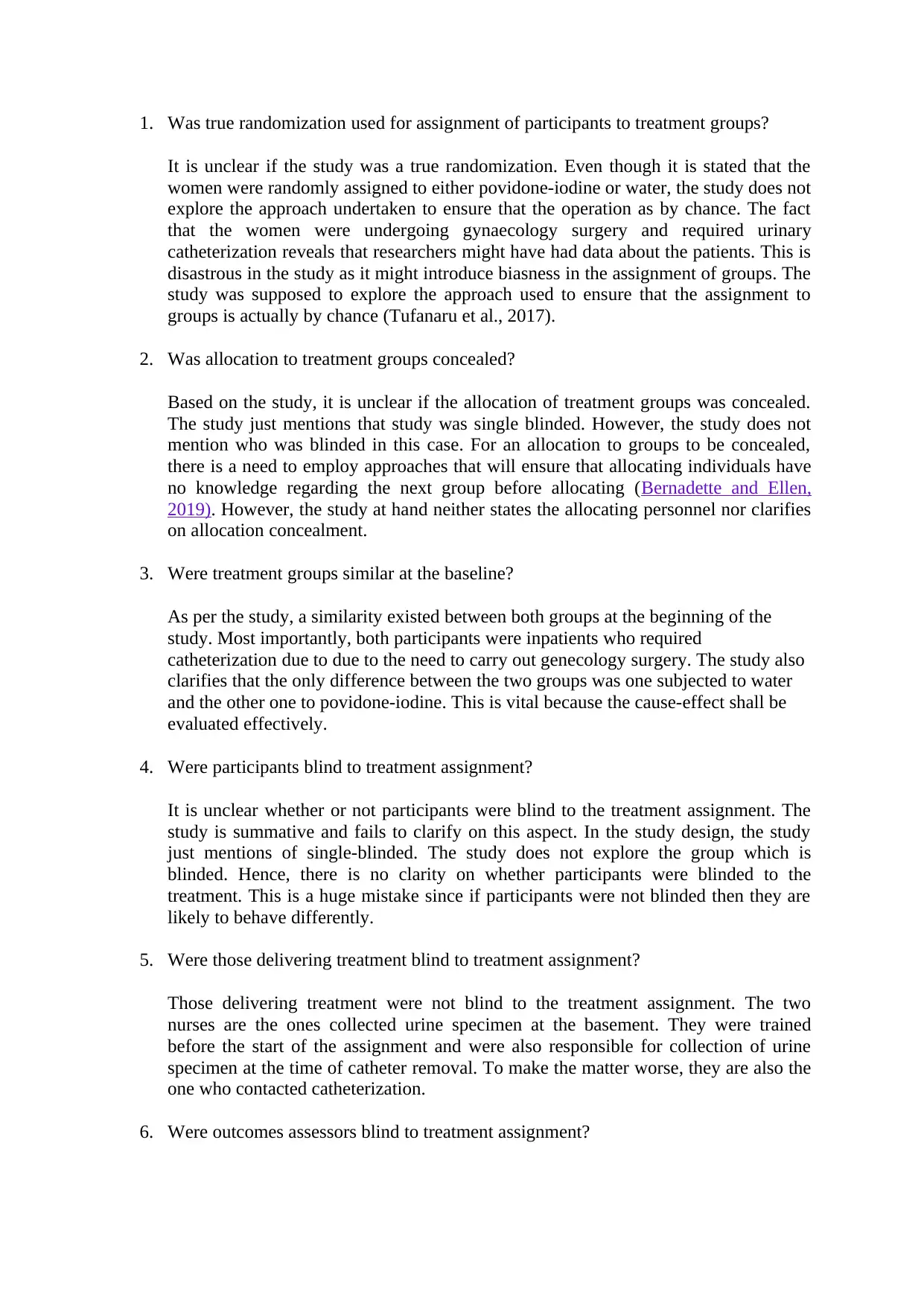
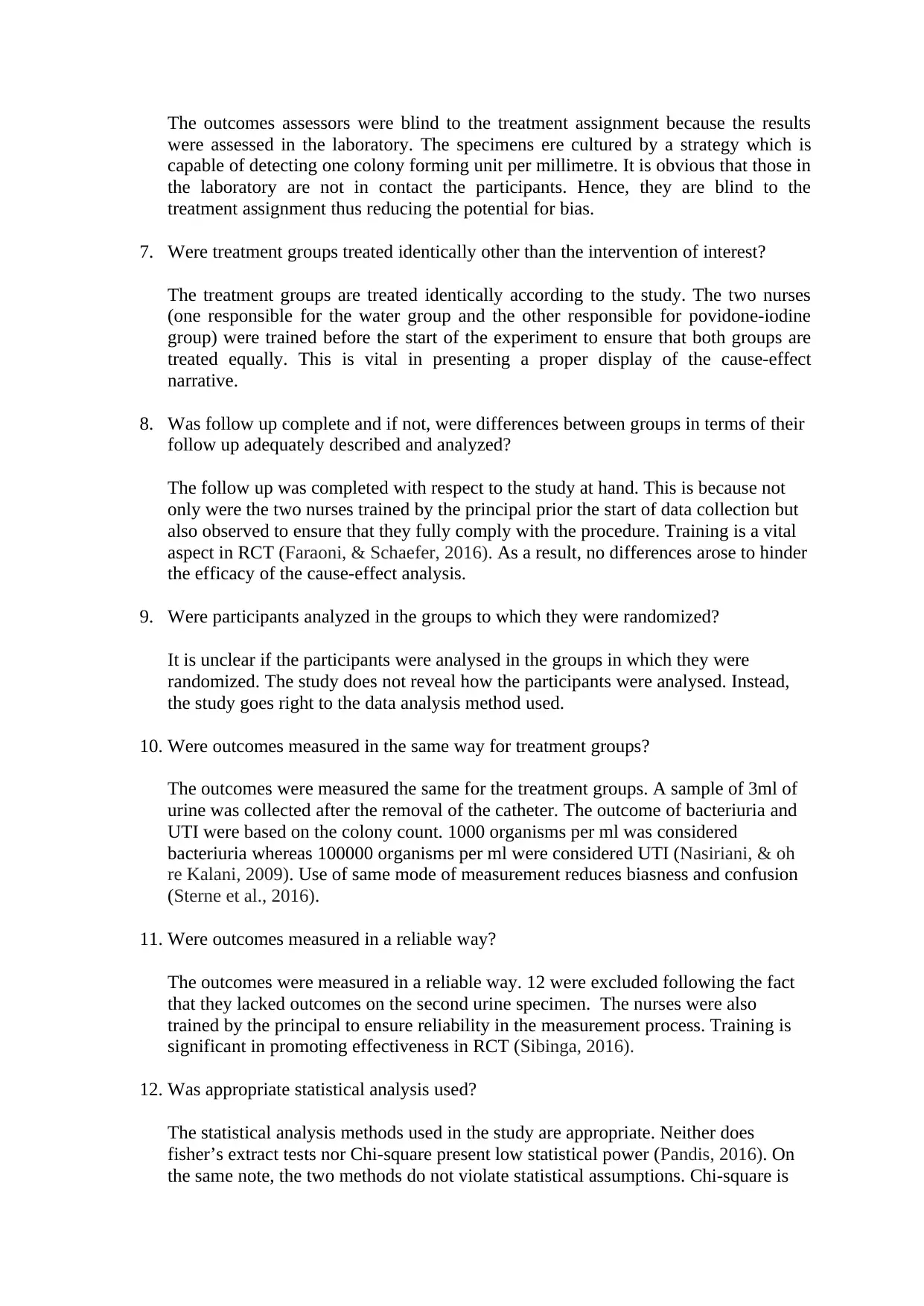
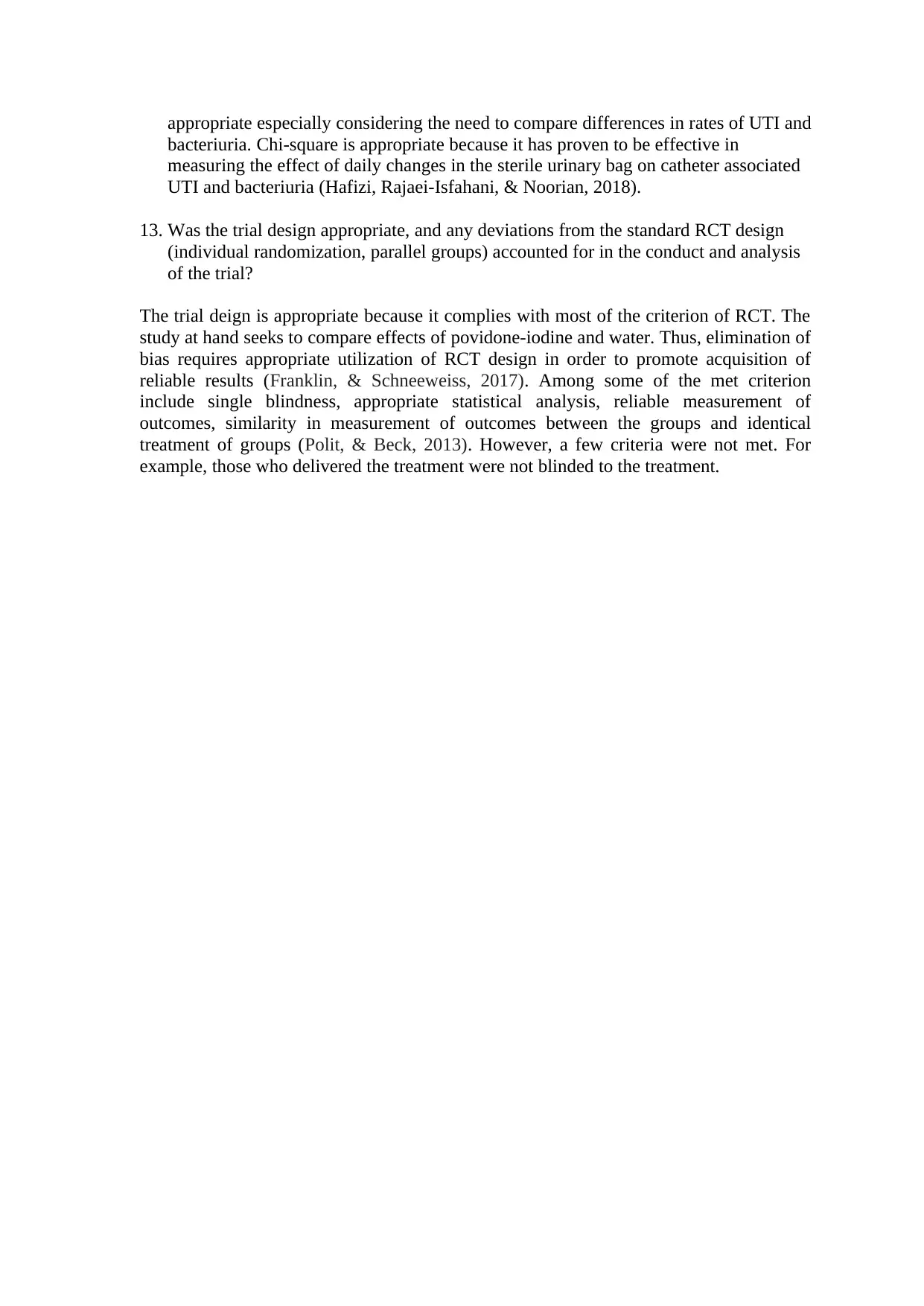
This assignment critically appraises a randomized controlled trial (RCT) investigating the effects of povidone-iodine versus water for periurethral cleaning in women undergoing gynecologic surgery and requiring urinary catheterization, using the Joanna Briggs Institute (JBI) checklist. The evaluation assesses key aspects of the RCT's design and conduct. The assessment determines whether true randomization was used, the allocation concealment, and the similarity of treatment groups at baseline. The study's blinding procedures for participants, treatment providers, and outcome assessors are examined, along with the identical treatment of groups other than the intervention of interest, and the completeness of follow-up. The assignment also analyzes whether participants were analyzed in the groups to which they were randomized, if outcomes were measured consistently, and if appropriate statistical analyses were employed. Finally, the study's overall design and adherence to RCT standards are evaluated, highlighting strengths, weaknesses, and potential biases. The study reveals that the RCT was single-blinded. The outcome assessors were blind to treatment assignment, and that follow up was completed. The treatment groups were treated identically other than the intervention of interest.
1 out of 4
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.