Red Blood Cell Storage Lesions: Effects, Risks, and Adverse Events
VerifiedAdded on 2020/05/16
|85
|26859
|109
Report
AI Summary
This report provides a detailed overview of red blood cell storage lesions, which are alterations occurring in red blood cells during storage. It explores the morphological changes like reduced deformability and vesiculation, biochemical changes including depletion of ATP and increased potassium ion concentrations, and immunological changes such as leukocyte contaminations. The report discusses the impact of blood processing and storage temperatures on lesion development. It also addresses the short-term and long-term effects of storage lesions, adverse events like hyperkalemia and TRALI, and the efficacy of stored red blood cells in oxygen transport. The document highlights the importance of understanding storage lesions to improve transfusion safety and patient outcomes, summarizing the various risks associated with transfusion of aged red blood cells.

Running head: RED BLOOD CELL STORAGE LESION
RED BLOOD CELL STORAGE LESION
Name of the Student
Name of the University
Author Notes
RED BLOOD CELL STORAGE LESION
Name of the Student
Name of the University
Author Notes
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1RED BLOOD CELL STORAGE LESION
Abstract
Storage lesions are alterations or changes that occur in the red blood cells following storage. The
red blood cells are stored in various storage solutions and kept at low temperatures to preserve
them. However, even after the attempts made to properly store the red blood cells, these red
blood cell components undergo various changes at the morphological, biochemical and
immunological levels. The morphological changes include reduced deformability, loss of
membrane integrity, vesiculation, microparticle formation, disruption of cytoskeletons,
hemolysis, among others. The biochemical changes include depletion of 2,3, diphosphoglycerate,
adenosine triphosphate, nitric oxide, oxidative stress resulting from reactive oxygen species,
among others. Moreover, storage lesions are also associated with the increased extracellular
concentrations of potassium ions. The immunological changes associated with storage lesions
include leukocyte contaminations that can give rise to various medical conditions like TRIM,
TRALI, NHFTR, among others. Other adverse events associated with storage lesions are
hyperkalemia, hypocalcemia, nosocomial infections, post operative infections, cancer recurrence,
infections by cytomegalovirus, HIV, increased rates of morbidity and mortality, among others.
Abstract
Storage lesions are alterations or changes that occur in the red blood cells following storage. The
red blood cells are stored in various storage solutions and kept at low temperatures to preserve
them. However, even after the attempts made to properly store the red blood cells, these red
blood cell components undergo various changes at the morphological, biochemical and
immunological levels. The morphological changes include reduced deformability, loss of
membrane integrity, vesiculation, microparticle formation, disruption of cytoskeletons,
hemolysis, among others. The biochemical changes include depletion of 2,3, diphosphoglycerate,
adenosine triphosphate, nitric oxide, oxidative stress resulting from reactive oxygen species,
among others. Moreover, storage lesions are also associated with the increased extracellular
concentrations of potassium ions. The immunological changes associated with storage lesions
include leukocyte contaminations that can give rise to various medical conditions like TRIM,
TRALI, NHFTR, among others. Other adverse events associated with storage lesions are
hyperkalemia, hypocalcemia, nosocomial infections, post operative infections, cancer recurrence,
infections by cytomegalovirus, HIV, increased rates of morbidity and mortality, among others.
2RED BLOOD CELL STORAGE LESION
Table of Contents
Introduction......................................................................................................................................4
Storage lesions.................................................................................................................................7
Blood processing plays an important role in the development of storage lesions...........................8
Storage lesions and short or long term effects...............................................................................11
Short term effects.......................................................................................................................12
Long term effects.......................................................................................................................12
Morphological, structural and metabolic changes of red blood cells during storage....................12
Deformability.............................................................................................................................12
Packed cell volume and osmotic fragility..................................................................................16
Lipid peroxidation.....................................................................................................................17
Protein oxidation........................................................................................................................19
Vesiculation...............................................................................................................................21
Biochemical changes of stored red blood cells..............................................................................23
Changes in 2,3-diphosphoglycerate levels following storage of red blood cells......................24
Effect of storage on 2, 3-diphosphoglycerate concentration.....................................................26
Effect of storage on Adenosine Triphosphate (ATP) concentration.........................................27
Effect of storage on the concentration of nitric oxide in red blood cells...................................32
Increased potassium ion concentration in the stored red blood cell supernatants.....................35
Accumulation of ammonia following storage of red blood cells..............................................37
Table of Contents
Introduction......................................................................................................................................4
Storage lesions.................................................................................................................................7
Blood processing plays an important role in the development of storage lesions...........................8
Storage lesions and short or long term effects...............................................................................11
Short term effects.......................................................................................................................12
Long term effects.......................................................................................................................12
Morphological, structural and metabolic changes of red blood cells during storage....................12
Deformability.............................................................................................................................12
Packed cell volume and osmotic fragility..................................................................................16
Lipid peroxidation.....................................................................................................................17
Protein oxidation........................................................................................................................19
Vesiculation...............................................................................................................................21
Biochemical changes of stored red blood cells..............................................................................23
Changes in 2,3-diphosphoglycerate levels following storage of red blood cells......................24
Effect of storage on 2, 3-diphosphoglycerate concentration.....................................................26
Effect of storage on Adenosine Triphosphate (ATP) concentration.........................................27
Effect of storage on the concentration of nitric oxide in red blood cells...................................32
Increased potassium ion concentration in the stored red blood cell supernatants.....................35
Accumulation of ammonia following storage of red blood cells..............................................37
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3RED BLOOD CELL STORAGE LESION
Injuries resulting from oxidative stress......................................................................................37
Plasma hemolysis.......................................................................................................................38
Immunologic changes of stored red blood cells............................................................................40
Adverse events or risks associated with the transfusion of stored red blood cells........................45
Transfusion related immunomodulation or TRIM....................................................................49
Transfusion related acute lung injury or TRALI.......................................................................51
Non hemolytic febrile transfusion reaction or NHFTR.............................................................53
Hyperkalemia.............................................................................................................................54
Citrate toxicity and Hypocalcaemia...........................................................................................56
Hypomagnesemia......................................................................................................................56
Other adverse events..................................................................................................................57
Conclusion.....................................................................................................................................57
Reference List................................................................................................................................62
Injuries resulting from oxidative stress......................................................................................37
Plasma hemolysis.......................................................................................................................38
Immunologic changes of stored red blood cells............................................................................40
Adverse events or risks associated with the transfusion of stored red blood cells........................45
Transfusion related immunomodulation or TRIM....................................................................49
Transfusion related acute lung injury or TRALI.......................................................................51
Non hemolytic febrile transfusion reaction or NHFTR.............................................................53
Hyperkalemia.............................................................................................................................54
Citrate toxicity and Hypocalcaemia...........................................................................................56
Hypomagnesemia......................................................................................................................56
Other adverse events..................................................................................................................57
Conclusion.....................................................................................................................................57
Reference List................................................................................................................................62
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4RED BLOOD CELL STORAGE LESION
Introduction
Red blood cells are the commonly used blood constituents, which are used for
transfusions throughout the World (Carson et al. 2012). The use of red blood cells have long
been associated with the history of transfusion medicine (Basu and Kulkarni 2014). In the
present times, the most widely used method for storage of the red blood cells is storing them in
solutions containing anticoagulants. Red blood cells are usually stored for 42 days and the
anticoagulant solutions consists of citrate, dextrose, phosphate and adenine (Adams et al. 2015).
Red blood cells also called erythrocytes, participate in delivering oxygen to the various body
tissues and also helps in carrying the carbon dioxide from the various tissues of the body to the
lungs (Cabrales and Intaglietta 2013). Red blood cells lack a nucleus and also a number of
organelles and contains the metalloprotein tetramere called haemoglobin. The haem groups of
haemoglobin helps in the transport of the gas molecules by actively binding with them (Jang,
Jang and Park, 2012). Thus, during the storage of the red blood cells, the plasma are removed
along with leukoreduction in some cases, which in turn generates the red blood cell concentrates
(Kim et al. 2016). The red blood cell concentrates are then stored in an additive hypertonic
solution containing sodium, adenine, glucose, mannitol at 376 mOsm/L. The solution is also
called the SAGM solution (D’Amici et al. 2012). Anaemia is generally considered as the
reduction in the number of the circulating red blood cells or reductions in the complete blood
count or CBC, with regards to hematocrit vales or hemoglobin concentration. Transfusion of red
blood cells is generally considered as the treatment for anaemia (Miller 2013). The guidelines for
transfusion has evolved throughout the years and in 1980 it involved transfusion to patients who
had haemoglobin concentration levels of less than 10g/dL and hematocrit vales that are less than
30%. However, in 1999, a randomized clinical trial revealed that transfusions should be given to
Introduction
Red blood cells are the commonly used blood constituents, which are used for
transfusions throughout the World (Carson et al. 2012). The use of red blood cells have long
been associated with the history of transfusion medicine (Basu and Kulkarni 2014). In the
present times, the most widely used method for storage of the red blood cells is storing them in
solutions containing anticoagulants. Red blood cells are usually stored for 42 days and the
anticoagulant solutions consists of citrate, dextrose, phosphate and adenine (Adams et al. 2015).
Red blood cells also called erythrocytes, participate in delivering oxygen to the various body
tissues and also helps in carrying the carbon dioxide from the various tissues of the body to the
lungs (Cabrales and Intaglietta 2013). Red blood cells lack a nucleus and also a number of
organelles and contains the metalloprotein tetramere called haemoglobin. The haem groups of
haemoglobin helps in the transport of the gas molecules by actively binding with them (Jang,
Jang and Park, 2012). Thus, during the storage of the red blood cells, the plasma are removed
along with leukoreduction in some cases, which in turn generates the red blood cell concentrates
(Kim et al. 2016). The red blood cell concentrates are then stored in an additive hypertonic
solution containing sodium, adenine, glucose, mannitol at 376 mOsm/L. The solution is also
called the SAGM solution (D’Amici et al. 2012). Anaemia is generally considered as the
reduction in the number of the circulating red blood cells or reductions in the complete blood
count or CBC, with regards to hematocrit vales or hemoglobin concentration. Transfusion of red
blood cells is generally considered as the treatment for anaemia (Miller 2013). The guidelines for
transfusion has evolved throughout the years and in 1980 it involved transfusion to patients who
had haemoglobin concentration levels of less than 10g/dL and hematocrit vales that are less than
30%. However, in 1999, a randomized clinical trial revealed that transfusions should be given to
5RED BLOOD CELL STORAGE LESION
individuals with a haemoglobin concentrations ranging between 7-9g/dL (Ansari and Szallasi
2012). This was termed as restrictive transfusion and brought about reductions in the 30 day
mortality rate of critically ill patients (Holst et al. 2015).
The red blood cell storage lesion is generally referred to the changes that occur due to the
ageing of the red blood cells while in storage solutions (Sut et al. 2017). In the human body, red
blood cells are generally removed from the circulation by 2 distinct mechanisms. These are the
red blood cell ageing and senescence (Bogdanova and Lutz 2013). These mechanisms are
characterized by progressive loss of surface area also called membrane loss and reduced
metabolism. Moreover, oxidative changes to the Band 3 protein increases the binding affinity of
antibodies specific to these proteins, thereby enhancing their ability to bind to the red blood cells,
which in turn are recognized by macrophages and removed from the blood circulation (Franco et
al. 2013). Thus, while in the storage solutions the red blood cells age and undergo haemolysis,
which is associated with the increase in concentrations of extracellular free iron, haeme as well
as haemoglobin along with nitric oxide reduced bioactivity resulting from scavenging (Kanias
and Gladwin 2012). Other changes that occur as a result of ageing of the red blood cells include
morphological changes, lactic acid, potassium and calcium accumulation, decrease in the levels
of ATP and 2,3-DPG, decrease in the rate of glycolysis, decrease in pH, along with an
accumulation of shed red blood cell derived microvescicles or microparticles, lipids and
bioactive proteins (García-Roa et al. 2017). However, manufacturing procedure and storage time
can have an impact on the safety of the transfusion process due to the increase in the levels of
extracellular vesicles and mitochondrial DNA in the red blood cell units (Shih et al. 2016). These
extracellular vescicles and mitochondrial DNA represent damage associated molecular patterns
or DAMPs, which results in priming of the patient’s immune system thereby affecting the safety
individuals with a haemoglobin concentrations ranging between 7-9g/dL (Ansari and Szallasi
2012). This was termed as restrictive transfusion and brought about reductions in the 30 day
mortality rate of critically ill patients (Holst et al. 2015).
The red blood cell storage lesion is generally referred to the changes that occur due to the
ageing of the red blood cells while in storage solutions (Sut et al. 2017). In the human body, red
blood cells are generally removed from the circulation by 2 distinct mechanisms. These are the
red blood cell ageing and senescence (Bogdanova and Lutz 2013). These mechanisms are
characterized by progressive loss of surface area also called membrane loss and reduced
metabolism. Moreover, oxidative changes to the Band 3 protein increases the binding affinity of
antibodies specific to these proteins, thereby enhancing their ability to bind to the red blood cells,
which in turn are recognized by macrophages and removed from the blood circulation (Franco et
al. 2013). Thus, while in the storage solutions the red blood cells age and undergo haemolysis,
which is associated with the increase in concentrations of extracellular free iron, haeme as well
as haemoglobin along with nitric oxide reduced bioactivity resulting from scavenging (Kanias
and Gladwin 2012). Other changes that occur as a result of ageing of the red blood cells include
morphological changes, lactic acid, potassium and calcium accumulation, decrease in the levels
of ATP and 2,3-DPG, decrease in the rate of glycolysis, decrease in pH, along with an
accumulation of shed red blood cell derived microvescicles or microparticles, lipids and
bioactive proteins (García-Roa et al. 2017). However, manufacturing procedure and storage time
can have an impact on the safety of the transfusion process due to the increase in the levels of
extracellular vesicles and mitochondrial DNA in the red blood cell units (Shih et al. 2016). These
extracellular vescicles and mitochondrial DNA represent damage associated molecular patterns
or DAMPs, which results in priming of the patient’s immune system thereby affecting the safety
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6RED BLOOD CELL STORAGE LESION
of the transfusion procedures (Schaefer 2014). Moreover, formation of red blood cell lesions and
their associated changes alters the ability of the red blood cells to carry oxygen, makes them
more rigid, and prevents them to undergo microcirculation. Oxidative stress forms an important
part of red blood cell storage lesion formation. This results in protein oxidation, lipid
peroxidation and decreased integrity of the membranes of the red blood cells. These in turn
contribute to the formation of microparticles or microvescicles that results in the increased risk
of post transfusion complications (Huyut et al. 2016).
The presence of red blood cell lesions in the components of the stored blood results in
adverse events in patients receiving blood transfusions. The adverse events results from
inflammatory and immunomodulatory complications as well as changes associated with
vasoregulation (Sahu and Hemlata 2014). Studies have revealed the occurrence of adverse events
in patients receiving transfusions with older blood samples. These include postoperative
infections, multiple organ failure, prolonged mechanical ventilation, increased hospital stay of
patients and even death (Cholette et al. 2015). Various studies have indicated the link between
increased storage times of red blood cells with adverse clinical outcomes in patients receiving
transfusions. These adverse outcomes are generally observed in patients in intensive care or
those who have undergone cardiac interventions, colorectal surgery or multiple traumas. The side
effects associated with the use of old red blood cells is varied but it ranges typically between
reductions in the gastric pH to increase in mortality rates as a result of multi organ failure
(Lelubre and Vincent 2013). Other adverse events include pneumonia in patients who have
undergone an aorta coronary artery bypass, increase in susceptibility to a variety of infections as
well as life threatening complications in patients who have undergone heart surgeries (Likosky et
al. 2015). Transfusions with blood components containing red blood cell lesions can also give
of the transfusion procedures (Schaefer 2014). Moreover, formation of red blood cell lesions and
their associated changes alters the ability of the red blood cells to carry oxygen, makes them
more rigid, and prevents them to undergo microcirculation. Oxidative stress forms an important
part of red blood cell storage lesion formation. This results in protein oxidation, lipid
peroxidation and decreased integrity of the membranes of the red blood cells. These in turn
contribute to the formation of microparticles or microvescicles that results in the increased risk
of post transfusion complications (Huyut et al. 2016).
The presence of red blood cell lesions in the components of the stored blood results in
adverse events in patients receiving blood transfusions. The adverse events results from
inflammatory and immunomodulatory complications as well as changes associated with
vasoregulation (Sahu and Hemlata 2014). Studies have revealed the occurrence of adverse events
in patients receiving transfusions with older blood samples. These include postoperative
infections, multiple organ failure, prolonged mechanical ventilation, increased hospital stay of
patients and even death (Cholette et al. 2015). Various studies have indicated the link between
increased storage times of red blood cells with adverse clinical outcomes in patients receiving
transfusions. These adverse outcomes are generally observed in patients in intensive care or
those who have undergone cardiac interventions, colorectal surgery or multiple traumas. The side
effects associated with the use of old red blood cells is varied but it ranges typically between
reductions in the gastric pH to increase in mortality rates as a result of multi organ failure
(Lelubre and Vincent 2013). Other adverse events include pneumonia in patients who have
undergone an aorta coronary artery bypass, increase in susceptibility to a variety of infections as
well as life threatening complications in patients who have undergone heart surgeries (Likosky et
al. 2015). Transfusions with blood components containing red blood cell lesions can also give
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7RED BLOOD CELL STORAGE LESION
rise to complications like transfusion related acute lung injury or TRALI (Hart, Cserti‐
Gazdewich and McCluskey 2015). This report provides a brief overview of red blood cell
storage lesions, the various biochemical, morphological and immunological changes associated
with the ageing of the red blood cells in storage, short term effects of transfusion with such aged
red blood cells, adverse outcomes associated with it, presence of leukocyte contaminations, the
efficacy of the red blood cells to transport gases following ageing, among others.
Storage lesions
The ability to store blood was determined after the discovery of sodium citrate, which
acts as a blood coagulant (Zubair 2010). The discovery of blood storage techniques brought with
it the revolutionary practices of blood transfusion that can save millions of lives and also
improved the practices associated with surgery and medicine. However, along with the beneficial
effects, the blood transfusion was also associated with the storage of the red blood cell
components, which in turn gave rise to the problems associated with the formation of storage
lesions (Kor, Van Buskirk and Gajic 2009). The main objective associated with the discovery of
blood transfusion was to improve the delivery of oxygen supply to the various organs, however,
with the development of storage lesions the capacity of the red blood cells to efficiently transfer
oxygen to the various organs have been impaired (Tsai et al. 2010; Tsai et al. 2015; Chan et al.
2017).
rise to complications like transfusion related acute lung injury or TRALI (Hart, Cserti‐
Gazdewich and McCluskey 2015). This report provides a brief overview of red blood cell
storage lesions, the various biochemical, morphological and immunological changes associated
with the ageing of the red blood cells in storage, short term effects of transfusion with such aged
red blood cells, adverse outcomes associated with it, presence of leukocyte contaminations, the
efficacy of the red blood cells to transport gases following ageing, among others.
Storage lesions
The ability to store blood was determined after the discovery of sodium citrate, which
acts as a blood coagulant (Zubair 2010). The discovery of blood storage techniques brought with
it the revolutionary practices of blood transfusion that can save millions of lives and also
improved the practices associated with surgery and medicine. However, along with the beneficial
effects, the blood transfusion was also associated with the storage of the red blood cell
components, which in turn gave rise to the problems associated with the formation of storage
lesions (Kor, Van Buskirk and Gajic 2009). The main objective associated with the discovery of
blood transfusion was to improve the delivery of oxygen supply to the various organs, however,
with the development of storage lesions the capacity of the red blood cells to efficiently transfer
oxygen to the various organs have been impaired (Tsai et al. 2010; Tsai et al. 2015; Chan et al.
2017).
8RED BLOOD CELL STORAGE LESION
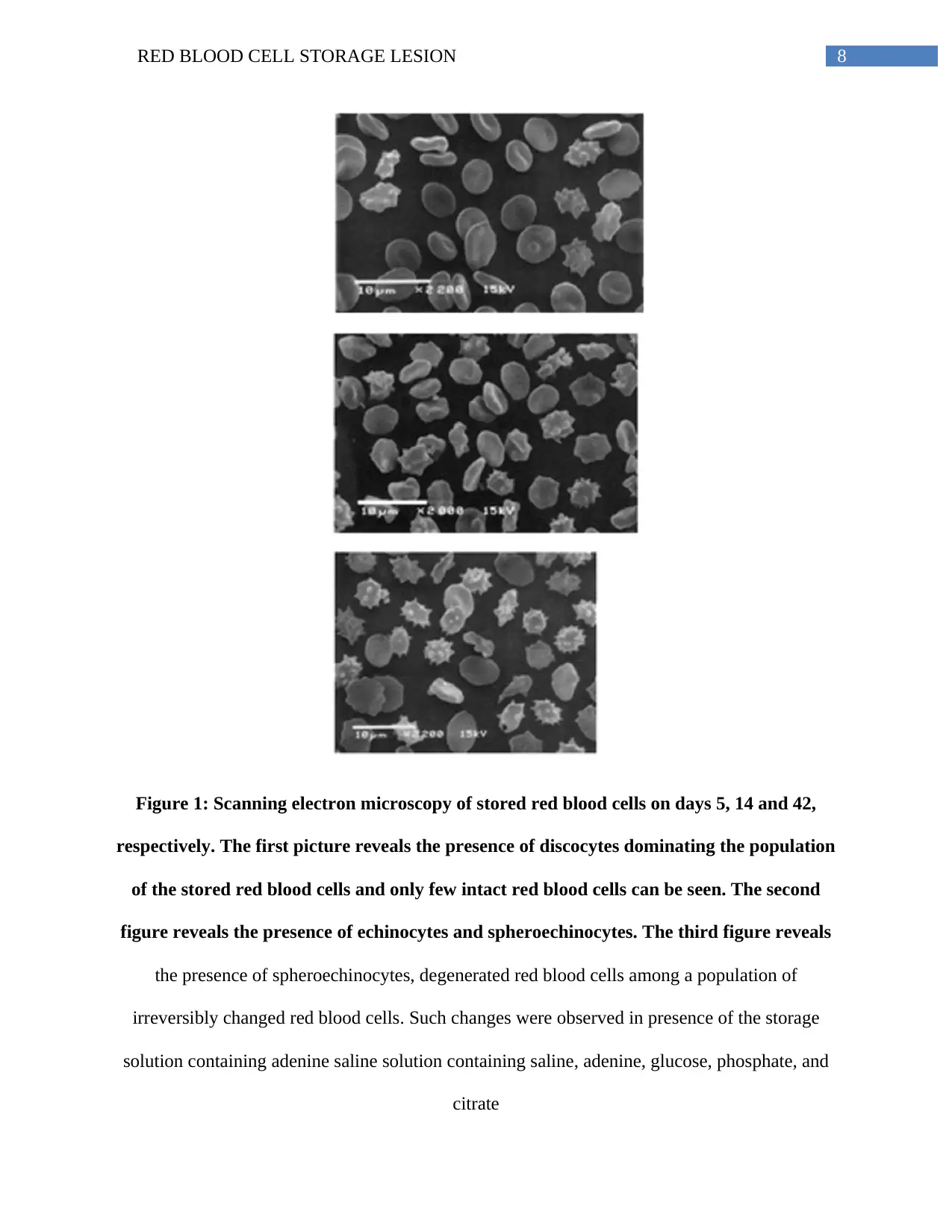
Figure 1: Scanning electron microscopy of stored red blood cells on days 5, 14 and 42,
respectively. The first picture reveals the presence of discocytes dominating the population
of the stored red blood cells and only few intact red blood cells can be seen. The second
figure reveals the presence of echinocytes and spheroechinocytes. The third figure reveals
the presence of spheroechinocytes, degenerated red blood cells among a population of
irreversibly changed red blood cells. Such changes were observed in presence of the storage
solution containing adenine saline solution containing saline, adenine, glucose, phosphate, and
citrate
Figure 1: Scanning electron microscopy of stored red blood cells on days 5, 14 and 42,
respectively. The first picture reveals the presence of discocytes dominating the population
of the stored red blood cells and only few intact red blood cells can be seen. The second
figure reveals the presence of echinocytes and spheroechinocytes. The third figure reveals
the presence of spheroechinocytes, degenerated red blood cells among a population of
irreversibly changed red blood cells. Such changes were observed in presence of the storage
solution containing adenine saline solution containing saline, adenine, glucose, phosphate, and
citrate
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9RED BLOOD CELL STORAGE LESION
(Source: Flatt, Bawazir and Bruce 2014)
Blood processing plays an important role in the development of storage lesions
The red blood cell concentrates are prepared by stripping the whole blood from the
platelet rich plasma (Basu and Kulkarni 2014; Dhurat and Sukesh 2014; Perez et al. 2014).
However, the various collection techniques and the preparation methods can have an impact on
the ageing of the stored red blood cells. One of the important factors that can have an effect on
the ageing of the stored red blood cells is the storage temperature (Zubair 2010). Packed red
blood cell concentrates are usually stored at a temperature of 1 to 6 degree Celsius. Storage at
this particular temperature results in the reduction in the metabolism of the red blood cells,
thereby reducing their demand for energy (Van de Watering and Brand 2008). As a result of
downregulation of the metabolic pathways, the shelf life of the red blood cell concentrates
increases (Sut et al. 2017; Sparrow 2012; D’Alessandro and Liumbruno 2017; Peters et al. 2017).
However, when red blood cells are stored at 4 degree Celsius or lower it results in the
impairment of the functions of the adenosine triphosphate dependent potassium ion pump and as
a result there occurs an equilibration of the potassium ion concentrations inside and outside of
the cells (Flatt, Bawazir and Bruce 2014; Yoshida and Shevkoplyas 2010). The resulting
concentration of potassium ions outside the cells increases and reaches a concentration of
90mEq/L (Kim‐Shapiro, Lee and Gladwin 2011; Zubair 2010; Adams et al. 2015; Pavenski et al.
2012). The subsequent transfusion of such packed red blood cells having high concentrations of
potassium ions results in the occurrence of hyperkalemia, renal failure and also affects the health
of the neonates (Rizos, Milionis and Elisaf 2017). Thus, it is necessary to wash the packed red
blood cell concentrates prior to transfusion. Another factor that gives rise to the development of
storage lesions are the process of leukoreduction. It is now a common practice in order to rid the
(Source: Flatt, Bawazir and Bruce 2014)
Blood processing plays an important role in the development of storage lesions
The red blood cell concentrates are prepared by stripping the whole blood from the
platelet rich plasma (Basu and Kulkarni 2014; Dhurat and Sukesh 2014; Perez et al. 2014).
However, the various collection techniques and the preparation methods can have an impact on
the ageing of the stored red blood cells. One of the important factors that can have an effect on
the ageing of the stored red blood cells is the storage temperature (Zubair 2010). Packed red
blood cell concentrates are usually stored at a temperature of 1 to 6 degree Celsius. Storage at
this particular temperature results in the reduction in the metabolism of the red blood cells,
thereby reducing their demand for energy (Van de Watering and Brand 2008). As a result of
downregulation of the metabolic pathways, the shelf life of the red blood cell concentrates
increases (Sut et al. 2017; Sparrow 2012; D’Alessandro and Liumbruno 2017; Peters et al. 2017).
However, when red blood cells are stored at 4 degree Celsius or lower it results in the
impairment of the functions of the adenosine triphosphate dependent potassium ion pump and as
a result there occurs an equilibration of the potassium ion concentrations inside and outside of
the cells (Flatt, Bawazir and Bruce 2014; Yoshida and Shevkoplyas 2010). The resulting
concentration of potassium ions outside the cells increases and reaches a concentration of
90mEq/L (Kim‐Shapiro, Lee and Gladwin 2011; Zubair 2010; Adams et al. 2015; Pavenski et al.
2012). The subsequent transfusion of such packed red blood cells having high concentrations of
potassium ions results in the occurrence of hyperkalemia, renal failure and also affects the health
of the neonates (Rizos, Milionis and Elisaf 2017). Thus, it is necessary to wash the packed red
blood cell concentrates prior to transfusion. Another factor that gives rise to the development of
storage lesions are the process of leukoreduction. It is now a common practice in order to rid the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10RED BLOOD CELL STORAGE LESION
packed red blood cells from leucocytes. Leukoreduction helps to prevent the occurrence of
alloimmunization, febrile non-hemolytic transfusion reaction, transfusion related immune
modulation (TRIM), infections that are transmitted as a result of transfusions like the infections
caused by the cytomegalovirus, the human immunodeficiency virus or HIV, among others
(Dellinger and Anaya 2004; Bassuni, Blajchman and Al-Moshary 2008; Sharma and Marwaha
2010). The presence of white blood cells affects the quality of the packed red blood cells. This in
turn affects the ability of the stored red blood cells to effectively transfer oxygen. Although some
studies suggest the role of leukoreduction in affecting the ability of stored red blood cells to
effectively transfer oxygen, however, there are no comprehensive data to validate such studies.
Another method that can impair the function of the stored red blood cells is irradiation.
Irradiation of the leukoreduced stored red blood cells are carried out in order to prevent the
occurrence of transfusion associated graft versus host disease (Acker, Marks and Sheffield
2016). The stored red blood cells are subjected to 25 Gy gamma radiations (Zubair 2010). The
principle of using irradiation on the packed red blood cells is to induce DNA damage with the
objective to prevent leukocyte proliferation in the presence of allogenic antigens. The effect of
gamma radiation on the packed red blood cells is alteration in the permeability of the membrane
(Ran et al. 2011; Adams et al. 2015; Serrano et al. 2017). This altered permeability of the red
blood cell membrane results in the leakage of various electrolytes like sodium and potassium.
Thus, following gamma irradiation, the packed red blood cells have high levels of potassium ion
concentrations. Apart from high levels of potassium ions, the stored red blood cells also have
poor viability and the shelf life of the packed red blood cells following gamma irradiation
changes from 42 days to 28 days. Thus, irradiation is also associated with the formation and
packed red blood cells from leucocytes. Leukoreduction helps to prevent the occurrence of
alloimmunization, febrile non-hemolytic transfusion reaction, transfusion related immune
modulation (TRIM), infections that are transmitted as a result of transfusions like the infections
caused by the cytomegalovirus, the human immunodeficiency virus or HIV, among others
(Dellinger and Anaya 2004; Bassuni, Blajchman and Al-Moshary 2008; Sharma and Marwaha
2010). The presence of white blood cells affects the quality of the packed red blood cells. This in
turn affects the ability of the stored red blood cells to effectively transfer oxygen. Although some
studies suggest the role of leukoreduction in affecting the ability of stored red blood cells to
effectively transfer oxygen, however, there are no comprehensive data to validate such studies.
Another method that can impair the function of the stored red blood cells is irradiation.
Irradiation of the leukoreduced stored red blood cells are carried out in order to prevent the
occurrence of transfusion associated graft versus host disease (Acker, Marks and Sheffield
2016). The stored red blood cells are subjected to 25 Gy gamma radiations (Zubair 2010). The
principle of using irradiation on the packed red blood cells is to induce DNA damage with the
objective to prevent leukocyte proliferation in the presence of allogenic antigens. The effect of
gamma radiation on the packed red blood cells is alteration in the permeability of the membrane
(Ran et al. 2011; Adams et al. 2015; Serrano et al. 2017). This altered permeability of the red
blood cell membrane results in the leakage of various electrolytes like sodium and potassium.
Thus, following gamma irradiation, the packed red blood cells have high levels of potassium ion
concentrations. Apart from high levels of potassium ions, the stored red blood cells also have
poor viability and the shelf life of the packed red blood cells following gamma irradiation
changes from 42 days to 28 days. Thus, irradiation is also associated with the formation and
11RED BLOOD CELL STORAGE LESION
acceleration of storage lesions in packed red blood cell concentrates (Zubair 2010; Agarwal et al.
2005; Yousuf et al. 2018).
Although storage of red blood cells are carried out in order to enable oxygen supply to
the various end organs but utilization of the stored red blood cell do not result in significant
availability of oxygen to the various end organs. Moreover, due to the alterations in the red blood
cell membrane permeability resulting from loss of membrane integrity and reduced
deformability, concerns are raised with respect to the potential occurrence of tissue ischemia and
microcirculatory occlusion. Resultant ischemic events have been reported in cardiac patients
receiving such transfusions of packed red blood cell concentrates (Carson, Triulzi and Ness
2017). Moreover, such transfusions also give rise to splanchnic hypoxia, which is characterized
by a reduction in the gastric mucosal pH. This medical condition is observed when transfusion is
carried out with stored red blood cells that are more than 15 days old. Moreover, such
transfusions are also associated with reduction in microcirculatory oxygenation. Other risks
involve the transmission of blood borne pathogens like the HIV virus. Moreover, increase in the
durations of storage of the red blood cells are associated with the increased risks of mortality.
The lungs are one of the targets following adverse effects of storage lesions. Transfusion related
pulmonary complications therefore arise. Other adverse events of transfusion with stored red
blood cells are multi organ failure, postoperative acute kidney injury, among others (Zubair
2010).
Storage lesions and short or long term effects
Storage lesions are the results of storage of red blood cells and the adverse events
associated with such storage. The formation of storage lesions progresses as the red blood cells
acceleration of storage lesions in packed red blood cell concentrates (Zubair 2010; Agarwal et al.
2005; Yousuf et al. 2018).
Although storage of red blood cells are carried out in order to enable oxygen supply to
the various end organs but utilization of the stored red blood cell do not result in significant
availability of oxygen to the various end organs. Moreover, due to the alterations in the red blood
cell membrane permeability resulting from loss of membrane integrity and reduced
deformability, concerns are raised with respect to the potential occurrence of tissue ischemia and
microcirculatory occlusion. Resultant ischemic events have been reported in cardiac patients
receiving such transfusions of packed red blood cell concentrates (Carson, Triulzi and Ness
2017). Moreover, such transfusions also give rise to splanchnic hypoxia, which is characterized
by a reduction in the gastric mucosal pH. This medical condition is observed when transfusion is
carried out with stored red blood cells that are more than 15 days old. Moreover, such
transfusions are also associated with reduction in microcirculatory oxygenation. Other risks
involve the transmission of blood borne pathogens like the HIV virus. Moreover, increase in the
durations of storage of the red blood cells are associated with the increased risks of mortality.
The lungs are one of the targets following adverse effects of storage lesions. Transfusion related
pulmonary complications therefore arise. Other adverse events of transfusion with stored red
blood cells are multi organ failure, postoperative acute kidney injury, among others (Zubair
2010).
Storage lesions and short or long term effects
Storage lesions are the results of storage of red blood cells and the adverse events
associated with such storage. The formation of storage lesions progresses as the red blood cells
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 85
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.