South Australian Aboriginal Children: SSB Consumption Health Programme
VerifiedAdded on 2020/05/03
|28
|7044
|85
Report
AI Summary
This report outlines a 24-month health promotion program designed to reduce sugar-sweetened beverage (SSB) consumption among South Australian Aboriginal and Torres Strait Islander children. The program aims to address the rising concern of SSB consumption and its adverse health effects, including obesity and metabolic diseases. The intervention involves educational interventions for children and parents, focusing on schools and community centers, with strategies like SSB restriction and monitoring of consumption and health indicators. The report emphasizes the need for community-driven interventions due to the higher vulnerability of Aboriginal and Torres Strait Islander people to health risks. The program's objectives include increasing awareness of SSB's negative impacts and reducing SSB consumption. Strategies involve a multidisciplinary team of healthcare professionals, educators, and social workers. The program's plan includes intervention and control groups, educational sessions, and the development of school wellness committees. The goal is to reduce SSB consumption and control obesity, considering socioeconomic factors, psychological risks, and lifestyle factors. The report includes details on the target group, program goals, health problems addressed, objectives, and strategies.
Food Nutrition
1
1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Title:
Health promotion programme for the reduction of children’s consumption of sugar sweetened
beverages (SSB) among South Australian Aboriginal and Torres Strait Islander children.
Description:
In this health promotion programme, educational intervention will be provided to the children
and parents of South Australian Aboriginal and Torres Strait Islander. It is evident that health
promotion programmes through educational intervention will be useful in improving health
of the people. Health education will be provided at schools and restriction on the
consumption of SSB will be implemented among these children. Quantity and frequency of
SSB consumption will be recorded. Body weight and body mass index of children will be
measured. This programme will be implemented for 24 months. This programme will be
beneficial in reducing obesity in children.
2
Health promotion programme for the reduction of children’s consumption of sugar sweetened
beverages (SSB) among South Australian Aboriginal and Torres Strait Islander children.
Description:
In this health promotion programme, educational intervention will be provided to the children
and parents of South Australian Aboriginal and Torres Strait Islander. It is evident that health
promotion programmes through educational intervention will be useful in improving health
of the people. Health education will be provided at schools and restriction on the
consumption of SSB will be implemented among these children. Quantity and frequency of
SSB consumption will be recorded. Body weight and body mass index of children will be
measured. This programme will be implemented for 24 months. This programme will be
beneficial in reducing obesity in children.
2
Evidence of need:
Consumption of Sugar-sweetened beverages (SSB) is rising as global health concern and
multiple adverse effects are associated with its consumption. Abundant evidence is available
in the form of systemic reviews and meta analysis to establish exposure and effect
relationship between SSB and obesity. Moreover, it has been observed that SSB is the
autonomous risk factor for metabolic disease like type 2 diabetes and cardiovascular disease
and few cancers and dental caries (Te Morenga et al., 2012; Malik et al., 2013). As
consumption of SSB is associated with multiple health issues, its magnitude is high on health
and well-being of the person (Malik et al., 2010). Consumption of SSBs is more in
Aboriginal and Torres Strait Islander people as compared to the other population.
Along with obesity, there is high prevalence of metabolic disease in these people. A research
project entitled ‘Next Step’ identified association between food choices and exposure to
diseases as priority research area. This project is applicable throughout Australia and more
emphasis is given to Aboriginal and Torres Strait Islander people. This project has more
importance because it is a community driven project and importance has been given to the
needs and interests of Aboriginal and Torres Strait Islander people (King and Brown, 2015).
Comprehensive intervention for SSB consumption, need to be planned which address at
multiple levels because there is widespread availability of SSB and it is in high demand
specifically in the children. As a result, there high magnitude of negative health impact of
SSB and it is difficult to control by planning small scale or localised intervention. It is
evident that people in the lower socio-economic status are more vulnerable to adverse health
conditions as compared to the people in high-socioeconomic status (Pampel et al., 2010).
Aboriginal and Torres Strait Islander people belongs to low socio-economic class as
compared to non-indigenous people. In these people, adverse health conditions might be due
to more exposure to behavioural and environmental health risk factors, poor living conditions
and inadequate education. Cultural aspects and racism also have major impact on the health
inequalities among indigenous and non-indigenous people in Australia. Hence, for these
people community driven intervention need to be carried out (AHMAC, 2015).
As compared to the global context prevalence of obesity is more in Indigenous children. One
of the prominent reason observed for increased prevalence of obesity is consumption of
refined carbohydrates like SSB (Singh et al., 2010). There is a biological link between the
obesity and consumption of SSB. These SSBs overcome the homeostatic regulatory system
3
Consumption of Sugar-sweetened beverages (SSB) is rising as global health concern and
multiple adverse effects are associated with its consumption. Abundant evidence is available
in the form of systemic reviews and meta analysis to establish exposure and effect
relationship between SSB and obesity. Moreover, it has been observed that SSB is the
autonomous risk factor for metabolic disease like type 2 diabetes and cardiovascular disease
and few cancers and dental caries (Te Morenga et al., 2012; Malik et al., 2013). As
consumption of SSB is associated with multiple health issues, its magnitude is high on health
and well-being of the person (Malik et al., 2010). Consumption of SSBs is more in
Aboriginal and Torres Strait Islander people as compared to the other population.
Along with obesity, there is high prevalence of metabolic disease in these people. A research
project entitled ‘Next Step’ identified association between food choices and exposure to
diseases as priority research area. This project is applicable throughout Australia and more
emphasis is given to Aboriginal and Torres Strait Islander people. This project has more
importance because it is a community driven project and importance has been given to the
needs and interests of Aboriginal and Torres Strait Islander people (King and Brown, 2015).
Comprehensive intervention for SSB consumption, need to be planned which address at
multiple levels because there is widespread availability of SSB and it is in high demand
specifically in the children. As a result, there high magnitude of negative health impact of
SSB and it is difficult to control by planning small scale or localised intervention. It is
evident that people in the lower socio-economic status are more vulnerable to adverse health
conditions as compared to the people in high-socioeconomic status (Pampel et al., 2010).
Aboriginal and Torres Strait Islander people belongs to low socio-economic class as
compared to non-indigenous people. In these people, adverse health conditions might be due
to more exposure to behavioural and environmental health risk factors, poor living conditions
and inadequate education. Cultural aspects and racism also have major impact on the health
inequalities among indigenous and non-indigenous people in Australia. Hence, for these
people community driven intervention need to be carried out (AHMAC, 2015).
As compared to the global context prevalence of obesity is more in Indigenous children. One
of the prominent reason observed for increased prevalence of obesity is consumption of
refined carbohydrates like SSB (Singh et al., 2010). There is a biological link between the
obesity and consumption of SSB. These SSBs overcome the homeostatic regulatory system
3
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
and it lead to reduced satiety and consequently excessive consumption of energy (Hu, 2013).
Hence, Australian Dietary Guidelines recommend to limit consumption of SSB in the form
soft drink and cordial. Australian Medical Association and Public Health Association of
Australia also addressed importance of intervention to limit consumption of SSB.
Intervention measures include heavy taxation of soft drinks, channelling of revenue from sale
of soft drinks to preventive measures, ban on sale of soft drinks in schools, ban on promotion
and advertising of soft drinks to the children. These efforts are in line with the international
trials for reduction in SSB consumption. However, there is scarcity of literature for
description of SSB consumption based on source, demographic and other dietary habits
(NHMRC, 2013; AHMAC, 2015).
National Children's Nutrition and Physical Activity Survey (NCNPAS) conducted survey
among 4,487 children aged between 2 and 16 years. In this survey, it was concluded that SSB
intake is high in Australian children and it is the need of hour to implement public health
intervention. In this survey, it was observed that supermarkets are the primary source of SSB.
Most of these children consumed these beverages at the home. Inadequate education of
parents and children about the health consequences of SSB consumption are mainly
responsible for more consumption of SSB among Aboriginal and Torres Strait Islander
children. SSB contributed approximately 4 % energy in children of age between 2 – 3years
old and approximately 7.5 % energy in children between 14-16 years old. Independence in
the children of age 14-16 years old is mainly responsible for more consumption of SSB, even
though it is evident that approximately 75 % of the children used to consume SSB at home.
Previous interventions mainly focused on the fast food for assessing consumption of SSB.
Due to recent findings, focus of the intervention should be diverted towards SSB
consumption in supermarket and consumption at home. There is variation among children of
different age group for SSB consumption. Children in age group between 2- 3 years prefers
to drink sweetened juice and 2 - 5 years prefers to drink sweetened fruit punch and fruit
juice. Consumption of SSB at the critical phase of growth and development can have major
impact on the health of child for the rest of life (Hafekost et al., 2011; NCNPAS, 2007).
A survey was conducted among Indigenous children and in this survey, it was found that
approximately 65 % Indigenous children are consuming soft drinks containing SSB and out
of this approximately 55 % children are consuming these drinks at home. 85 % of these SSB
drinks are purchased from supermarkets. Both parents and children were incorporated in this
survey and children between age group 11 – 16 years were the target group. Data was
4
Hence, Australian Dietary Guidelines recommend to limit consumption of SSB in the form
soft drink and cordial. Australian Medical Association and Public Health Association of
Australia also addressed importance of intervention to limit consumption of SSB.
Intervention measures include heavy taxation of soft drinks, channelling of revenue from sale
of soft drinks to preventive measures, ban on sale of soft drinks in schools, ban on promotion
and advertising of soft drinks to the children. These efforts are in line with the international
trials for reduction in SSB consumption. However, there is scarcity of literature for
description of SSB consumption based on source, demographic and other dietary habits
(NHMRC, 2013; AHMAC, 2015).
National Children's Nutrition and Physical Activity Survey (NCNPAS) conducted survey
among 4,487 children aged between 2 and 16 years. In this survey, it was concluded that SSB
intake is high in Australian children and it is the need of hour to implement public health
intervention. In this survey, it was observed that supermarkets are the primary source of SSB.
Most of these children consumed these beverages at the home. Inadequate education of
parents and children about the health consequences of SSB consumption are mainly
responsible for more consumption of SSB among Aboriginal and Torres Strait Islander
children. SSB contributed approximately 4 % energy in children of age between 2 – 3years
old and approximately 7.5 % energy in children between 14-16 years old. Independence in
the children of age 14-16 years old is mainly responsible for more consumption of SSB, even
though it is evident that approximately 75 % of the children used to consume SSB at home.
Previous interventions mainly focused on the fast food for assessing consumption of SSB.
Due to recent findings, focus of the intervention should be diverted towards SSB
consumption in supermarket and consumption at home. There is variation among children of
different age group for SSB consumption. Children in age group between 2- 3 years prefers
to drink sweetened juice and 2 - 5 years prefers to drink sweetened fruit punch and fruit
juice. Consumption of SSB at the critical phase of growth and development can have major
impact on the health of child for the rest of life (Hafekost et al., 2011; NCNPAS, 2007).
A survey was conducted among Indigenous children and in this survey, it was found that
approximately 65 % Indigenous children are consuming soft drinks containing SSB and out
of this approximately 55 % children are consuming these drinks at home. 85 % of these SSB
drinks are purchased from supermarkets. Both parents and children were incorporated in this
survey and children between age group 11 – 16 years were the target group. Data was
4
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
collected by using standard questionnaires. It was hypothesized that consumption of SSB can
lead to augmentation of cases of obesity in Indigenous children. Based on this hypothesis,
protocol was developed to carry out actual health promotion programme. Our hypothesis
exhibited similar response to 2007 Australian National, Children’s Nutrition and Physical
Activity Survey.
Following are the sample of questions from the survey:
1. How much amount of SSB is present in the soft-drinks ?
2. Whether parents are accompanying children while drinking SSB containing soft-
drinks ?
3. What is frequency of purchase of soft drinks from supermarkets?
4. What is frequency of soft drink consumption at home ?
5
lead to augmentation of cases of obesity in Indigenous children. Based on this hypothesis,
protocol was developed to carry out actual health promotion programme. Our hypothesis
exhibited similar response to 2007 Australian National, Children’s Nutrition and Physical
Activity Survey.
Following are the sample of questions from the survey:
1. How much amount of SSB is present in the soft-drinks ?
2. Whether parents are accompanying children while drinking SSB containing soft-
drinks ?
3. What is frequency of purchase of soft drinks from supermarkets?
4. What is frequency of soft drink consumption at home ?
5
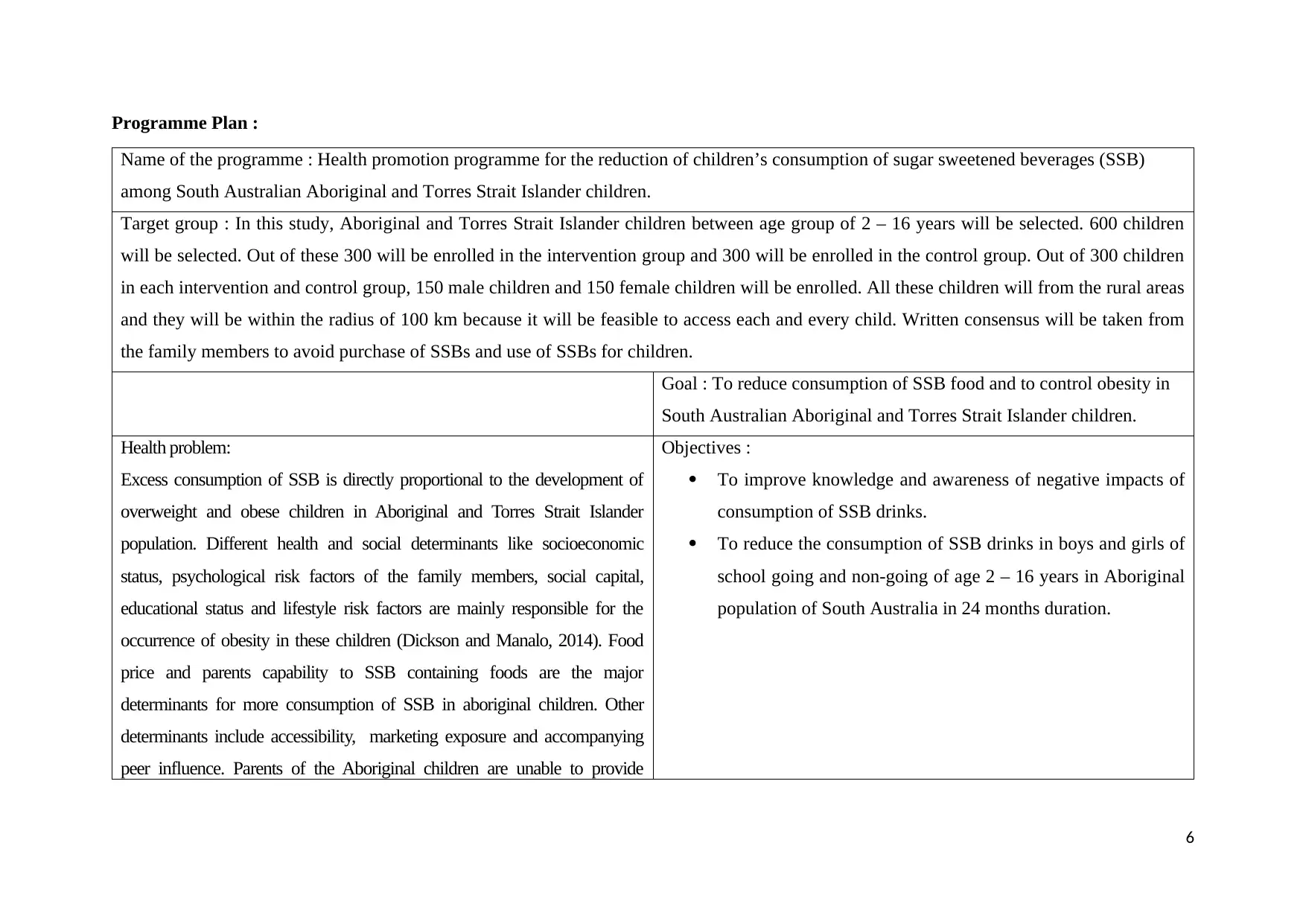
Programme Plan :
Name of the programme : Health promotion programme for the reduction of children’s consumption of sugar sweetened beverages (SSB)
among South Australian Aboriginal and Torres Strait Islander children.
Target group : In this study, Aboriginal and Torres Strait Islander children between age group of 2 – 16 years will be selected. 600 children
will be selected. Out of these 300 will be enrolled in the intervention group and 300 will be enrolled in the control group. Out of 300 children
in each intervention and control group, 150 male children and 150 female children will be enrolled. All these children will from the rural areas
and they will be within the radius of 100 km because it will be feasible to access each and every child. Written consensus will be taken from
the family members to avoid purchase of SSBs and use of SSBs for children.
Goal : To reduce consumption of SSB food and to control obesity in
South Australian Aboriginal and Torres Strait Islander children.
Health problem:
Excess consumption of SSB is directly proportional to the development of
overweight and obese children in Aboriginal and Torres Strait Islander
population. Different health and social determinants like socioeconomic
status, psychological risk factors of the family members, social capital,
educational status and lifestyle risk factors are mainly responsible for the
occurrence of obesity in these children (Dickson and Manalo, 2014). Food
price and parents capability to SSB containing foods are the major
determinants for more consumption of SSB in aboriginal children. Other
determinants include accessibility, marketing exposure and accompanying
peer influence. Parents of the Aboriginal children are unable to provide
Objectives :
To improve knowledge and awareness of negative impacts of
consumption of SSB drinks.
To reduce the consumption of SSB drinks in boys and girls of
school going and non-going of age 2 – 16 years in Aboriginal
population of South Australia in 24 months duration.
6
Name of the programme : Health promotion programme for the reduction of children’s consumption of sugar sweetened beverages (SSB)
among South Australian Aboriginal and Torres Strait Islander children.
Target group : In this study, Aboriginal and Torres Strait Islander children between age group of 2 – 16 years will be selected. 600 children
will be selected. Out of these 300 will be enrolled in the intervention group and 300 will be enrolled in the control group. Out of 300 children
in each intervention and control group, 150 male children and 150 female children will be enrolled. All these children will from the rural areas
and they will be within the radius of 100 km because it will be feasible to access each and every child. Written consensus will be taken from
the family members to avoid purchase of SSBs and use of SSBs for children.
Goal : To reduce consumption of SSB food and to control obesity in
South Australian Aboriginal and Torres Strait Islander children.
Health problem:
Excess consumption of SSB is directly proportional to the development of
overweight and obese children in Aboriginal and Torres Strait Islander
population. Different health and social determinants like socioeconomic
status, psychological risk factors of the family members, social capital,
educational status and lifestyle risk factors are mainly responsible for the
occurrence of obesity in these children (Dickson and Manalo, 2014). Food
price and parents capability to SSB containing foods are the major
determinants for more consumption of SSB in aboriginal children. Other
determinants include accessibility, marketing exposure and accompanying
peer influence. Parents of the Aboriginal children are unable to provide
Objectives :
To improve knowledge and awareness of negative impacts of
consumption of SSB drinks.
To reduce the consumption of SSB drinks in boys and girls of
school going and non-going of age 2 – 16 years in Aboriginal
population of South Australia in 24 months duration.
6
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
nutritious and healthy diet and medical treatment to their children due to
unemployment and less income. Aboriginal parents are associated with varied
psychological risk factors like psychological distress, food insecurity and
financial stress (Markwick et al., 2015). Hence, their decision-making ability
gets hampered and they can’t take timely decision to provide necessary
medical and dietary intervention to their child. There is scarcity of social
capital among all the stakeholders of Aboriginal community. Hence, they
can’t avail financial assistance and they can’t take advise for their neighbours
because most of the people in the Aboriginal community possesses similar
social status. Lack of proper education among the Aboriginal parents is
important determinant for the occurrence of obesity in children. Due to lack of
education, these parents are not aware of the adverse health effects of SSB.
Due to lack of education and psychological risk factors these parents can’t
discuss health conditions of their children with non-indigenous people.
Hence, they can’t get information about healthy lifestyle. Lifestyle risk factors
is one of the prominent reasons responsible for the prevalence of obesity in
Aboriginal children. Disproportionate and unhealthy food intake is
responsible for obesity in these children (Markwick et al., 2014; Johnston et
al., 2013).
Strategies : Reduction in the SSB consumption will comprise of
stakeholders from different fields. Nurses, physicians, retired health
7
unemployment and less income. Aboriginal parents are associated with varied
psychological risk factors like psychological distress, food insecurity and
financial stress (Markwick et al., 2015). Hence, their decision-making ability
gets hampered and they can’t take timely decision to provide necessary
medical and dietary intervention to their child. There is scarcity of social
capital among all the stakeholders of Aboriginal community. Hence, they
can’t avail financial assistance and they can’t take advise for their neighbours
because most of the people in the Aboriginal community possesses similar
social status. Lack of proper education among the Aboriginal parents is
important determinant for the occurrence of obesity in children. Due to lack of
education, these parents are not aware of the adverse health effects of SSB.
Due to lack of education and psychological risk factors these parents can’t
discuss health conditions of their children with non-indigenous people.
Hence, they can’t get information about healthy lifestyle. Lifestyle risk factors
is one of the prominent reasons responsible for the prevalence of obesity in
Aboriginal children. Disproportionate and unhealthy food intake is
responsible for obesity in these children (Markwick et al., 2014; Johnston et
al., 2013).
Strategies : Reduction in the SSB consumption will comprise of
stakeholders from different fields. Nurses, physicians, retired health
7
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
professionals, school teachers, paediatrician, research scientist,
research assistants and social workers. Overall activity of the
programme will be monitored by the principle investigator. Specific
responsibility will be handled by each stakeholder. Teachers and
retired health professionals will provide education and training to the
children and parents. Nurses, physicians and paediatrician will
perform health assessment and monitor health of the children. Data
collection will be performed by the research scientist and data
analysis will be performed by research scientist. Statistical analysis of
the collected data will be performed by statistician. Social workers
will increase awareness of the importance of reducing consumption of
SSB (Ma et al., 2016; Souza et al., 2013).
Education about the health effects of SSB will be provided to children
and family members of the intervention programme. Also, children
and family members in the intervention group will be banned from
purchasing SSB from supermarket and consumption of SSB at their
homes will also be restricted. In control group children, education
about SSB will not be provided and there will not be any ban on the
purchase and consumption of SSB. For non-school going children and
their parents education will be provided at community centres and
health centres. Education will be provided in the form of theoretical
classes and games which would be helpful for keeping abstained from
8
research assistants and social workers. Overall activity of the
programme will be monitored by the principle investigator. Specific
responsibility will be handled by each stakeholder. Teachers and
retired health professionals will provide education and training to the
children and parents. Nurses, physicians and paediatrician will
perform health assessment and monitor health of the children. Data
collection will be performed by the research scientist and data
analysis will be performed by research scientist. Statistical analysis of
the collected data will be performed by statistician. Social workers
will increase awareness of the importance of reducing consumption of
SSB (Ma et al., 2016; Souza et al., 2013).
Education about the health effects of SSB will be provided to children
and family members of the intervention programme. Also, children
and family members in the intervention group will be banned from
purchasing SSB from supermarket and consumption of SSB at their
homes will also be restricted. In control group children, education
about SSB will not be provided and there will not be any ban on the
purchase and consumption of SSB. For non-school going children and
their parents education will be provided at community centres and
health centres. Education will be provided in the form of theoretical
classes and games which would be helpful for keeping abstained from
8
the consumption of SSB (Avery et al., 2015; Zoellner et al., 2016).
Educational and health promotion programme will comprise of
(Rauba et al., 2017):
Development of school wellness committee comprising of
‘sugar free’ lesson plan.
Posters displaying ‘sugar free life’ in cafeteria of the school.
Lessons will be presented to teachers during weekly staff get-
together and in parents meeting. Suggestions from the parents
and teachers will be considered for improvement in the
programme.
Lessons will comprise of information about the adverse health
conditions related to the SSB, lifestyle measures to prevent
development of obesity, healthy diet formula for the children
and alternative drinks for SSB like real fruit juice.
Letters comprising of instructions to avoid purchase and use
of SSB will be sent to home of each student.
Special seminars will be arranged by nutritionist.
Weekly 4 X 45 min. lessons will be arranged.
Weekly 1 X 60 min. lesson will be planned of lifestyle
modifications.
Students will be advised to take part sports with more physical
9
Educational and health promotion programme will comprise of
(Rauba et al., 2017):
Development of school wellness committee comprising of
‘sugar free’ lesson plan.
Posters displaying ‘sugar free life’ in cafeteria of the school.
Lessons will be presented to teachers during weekly staff get-
together and in parents meeting. Suggestions from the parents
and teachers will be considered for improvement in the
programme.
Lessons will comprise of information about the adverse health
conditions related to the SSB, lifestyle measures to prevent
development of obesity, healthy diet formula for the children
and alternative drinks for SSB like real fruit juice.
Letters comprising of instructions to avoid purchase and use
of SSB will be sent to home of each student.
Special seminars will be arranged by nutritionist.
Weekly 4 X 45 min. lessons will be arranged.
Weekly 1 X 60 min. lesson will be planned of lifestyle
modifications.
Students will be advised to take part sports with more physical
9
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
activity.
Discounts will be provided for the bottles of real fruit juices in
the cafeteria.
Surveys will be conducted for parents and students to assess
improvement in the awareness of sugar free life. Based on the
outcome of the surveys, necessary modifications in the
programme will be implemented.
Weekly once home delivery of healthy drinks like real fruit
juice.
Children in both intervention group and control group will be
monitored for consumption of amount of SSBs and types of SSBs for
one year. All the enrolled children will also be assessed for obesity.
Body weight and body mass index will be evaluated for assessment of
obesity for 24 months.
Data collection:
Dara related to amount of SSB consumption, type of SSB, body
weight and body mass index will be collected. Semi-structured
interviews will be conducted for parents of the children for amount
and quality of SSB consumption. Semi-structured interviews have the
option of slight modification in the framework of questions.
Questionnaires will be prepared based on the validated questions
10
Discounts will be provided for the bottles of real fruit juices in
the cafeteria.
Surveys will be conducted for parents and students to assess
improvement in the awareness of sugar free life. Based on the
outcome of the surveys, necessary modifications in the
programme will be implemented.
Weekly once home delivery of healthy drinks like real fruit
juice.
Children in both intervention group and control group will be
monitored for consumption of amount of SSBs and types of SSBs for
one year. All the enrolled children will also be assessed for obesity.
Body weight and body mass index will be evaluated for assessment of
obesity for 24 months.
Data collection:
Dara related to amount of SSB consumption, type of SSB, body
weight and body mass index will be collected. Semi-structured
interviews will be conducted for parents of the children for amount
and quality of SSB consumption. Semi-structured interviews have the
option of slight modification in the framework of questions.
Questionnaires will be prepared based on the validated questions
10
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
based on the literature and these questions will be prepared by experts
in the field. Data related to food consumption will be collected over
the phone by enquiring with parents. Research assistance will collect
data for food consumption. Data related to body weight and body
mass index will be measured and recorded by nurses and other
healthcare professionals. Body weight and body mass index data will
be collected at designated healthcare centres.
Data analysis:
Collected data will be stored in Microsoft Excel and mean and
standard deviation will be calculated for this data. Compiled data will
be verified and reviewed by research assistance and research scientist
respectively. For each children data will be stored in coded form to
maintain confidentiality of the data. Data will be presented in the
form of tables and graphs and these will be prepared separately for
intervention group and control group. Power calculation will be done
for statistical significance. Mean difference between intervention
group and control will calculated. Within each group, data will be
calculated and presented for boys and girls separately. Statistical
analysis will be performed by using SPSS 18.0 software (SPSS Inc.,
Chicago, IL, USA). For comparison intervention group and control;
and boys and girls of the same group, either ‘t’ test or one-way
repeated measures ANOVA will be implemented. Post hoc
11
in the field. Data related to food consumption will be collected over
the phone by enquiring with parents. Research assistance will collect
data for food consumption. Data related to body weight and body
mass index will be measured and recorded by nurses and other
healthcare professionals. Body weight and body mass index data will
be collected at designated healthcare centres.
Data analysis:
Collected data will be stored in Microsoft Excel and mean and
standard deviation will be calculated for this data. Compiled data will
be verified and reviewed by research assistance and research scientist
respectively. For each children data will be stored in coded form to
maintain confidentiality of the data. Data will be presented in the
form of tables and graphs and these will be prepared separately for
intervention group and control group. Power calculation will be done
for statistical significance. Mean difference between intervention
group and control will calculated. Within each group, data will be
calculated and presented for boys and girls separately. Statistical
analysis will be performed by using SPSS 18.0 software (SPSS Inc.,
Chicago, IL, USA). For comparison intervention group and control;
and boys and girls of the same group, either ‘t’ test or one-way
repeated measures ANOVA will be implemented. Post hoc
11

comparisons and correlation analysis will be performed by
implementing Tukey test and Pearson’s coefficients (Petrie and Sabin,
2016).
12
implementing Tukey test and Pearson’s coefficients (Petrie and Sabin,
2016).
12
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 28
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.