Healthcare Change Project: Patient Waiting Times (Part C)
VerifiedAdded on 2023/04/23
|12
|2432
|107
Report
AI Summary
This report presents an analysis of patient waiting times at Mediclinic Parkview Hospital in Dubai, focusing on outpatient and inpatient data for children. The study examines waiting times across various age groups (0-15 and 16-64 months) and time bands, revealing that the majority of children with prolonged waiting times belong to the 0-15 months age group and the 0-3 months time band. The report includes tables, graphs, and pie charts to illustrate the data, along with a data summary highlighting key findings. It also discusses data limitations, ethical concerns, and recommendations for improved data collection, clustering, and patient feedback. The analysis underscores the need for organizational change to reduce waiting times and enhance patient satisfaction, including suggestions for data filtering, customer surveys, and maintaining data security and patient privacy.

Running head: HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
HEALTHCARE ORGANIZATIONAL CHANGE PROJECT: Reduction of
Patient Waiting Times and Improvement of Patient Satisfaction (Part C)
Name of the Student:
Name of the University:
Author note
HEALTHCARE ORGANIZATIONAL CHANGE PROJECT: Reduction of
Patient Waiting Times and Improvement of Patient Satisfaction (Part C)
Name of the Student:
Name of the University:
Author note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser

1HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
Executive Summary
Long duration waiting times have been a major shortcoming associated with
healthcare organizations resulting in numerous patients being deprived of quality
treatment and associated negative customer feedback. The followed report assesses
the number of children in queue for a healthcare organization in the United Arab
Emirates, distributed across age groups pf 0-15 and 16-64 months and time bands of
0-3, 3-6, 6-9, 9-12, 12-15, 15-18 and 18+ months. From the represented data, it can
be observed that the largest number of children in waiting lists belong to the age
group of 0-15 months and time band of 0-3 months. However, data filtering and
clustering are recommended since analysis of day-wise data of 4,599 entries was
cumbersome due to which the first 100 entries were considered as a starting point.
Maintenance of data security, patient privacy and consent are key ethical issues to
be taken into consideration while managing large healthcare data.
Executive Summary
Long duration waiting times have been a major shortcoming associated with
healthcare organizations resulting in numerous patients being deprived of quality
treatment and associated negative customer feedback. The followed report assesses
the number of children in queue for a healthcare organization in the United Arab
Emirates, distributed across age groups pf 0-15 and 16-64 months and time bands of
0-3, 3-6, 6-9, 9-12, 12-15, 15-18 and 18+ months. From the represented data, it can
be observed that the largest number of children in waiting lists belong to the age
group of 0-15 months and time band of 0-3 months. However, data filtering and
clustering are recommended since analysis of day-wise data of 4,599 entries was
cumbersome due to which the first 100 entries were considered as a starting point.
Maintenance of data security, patient privacy and consent are key ethical issues to
be taken into consideration while managing large healthcare data.
2HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
Table of Contents
Data Presentation of Waiting Times..................................................................3
Table 1: Waiting Patients: Number of Children (As designed by the Author)3
Graph 1: Number of Children in Waiting Time Bands (As designed by the
Author).......................................................................................................................3
Pie Chart: Waiting Time Bands (As designed by the Author)........................4
Table 2: Total Waiting Times (As designed by the Author)...........................5
Data Summary...................................................................................................9
Additional Data Limitations and Recommendations..........................................9
Ethical Concerns..............................................................................................10
References.......................................................................................................11
Table of Contents
Data Presentation of Waiting Times..................................................................3
Table 1: Waiting Patients: Number of Children (As designed by the Author)3
Graph 1: Number of Children in Waiting Time Bands (As designed by the
Author).......................................................................................................................3
Pie Chart: Waiting Time Bands (As designed by the Author)........................4
Table 2: Total Waiting Times (As designed by the Author)...........................5
Data Summary...................................................................................................9
Additional Data Limitations and Recommendations..........................................9
Ethical Concerns..............................................................................................10
References.......................................................................................................11
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
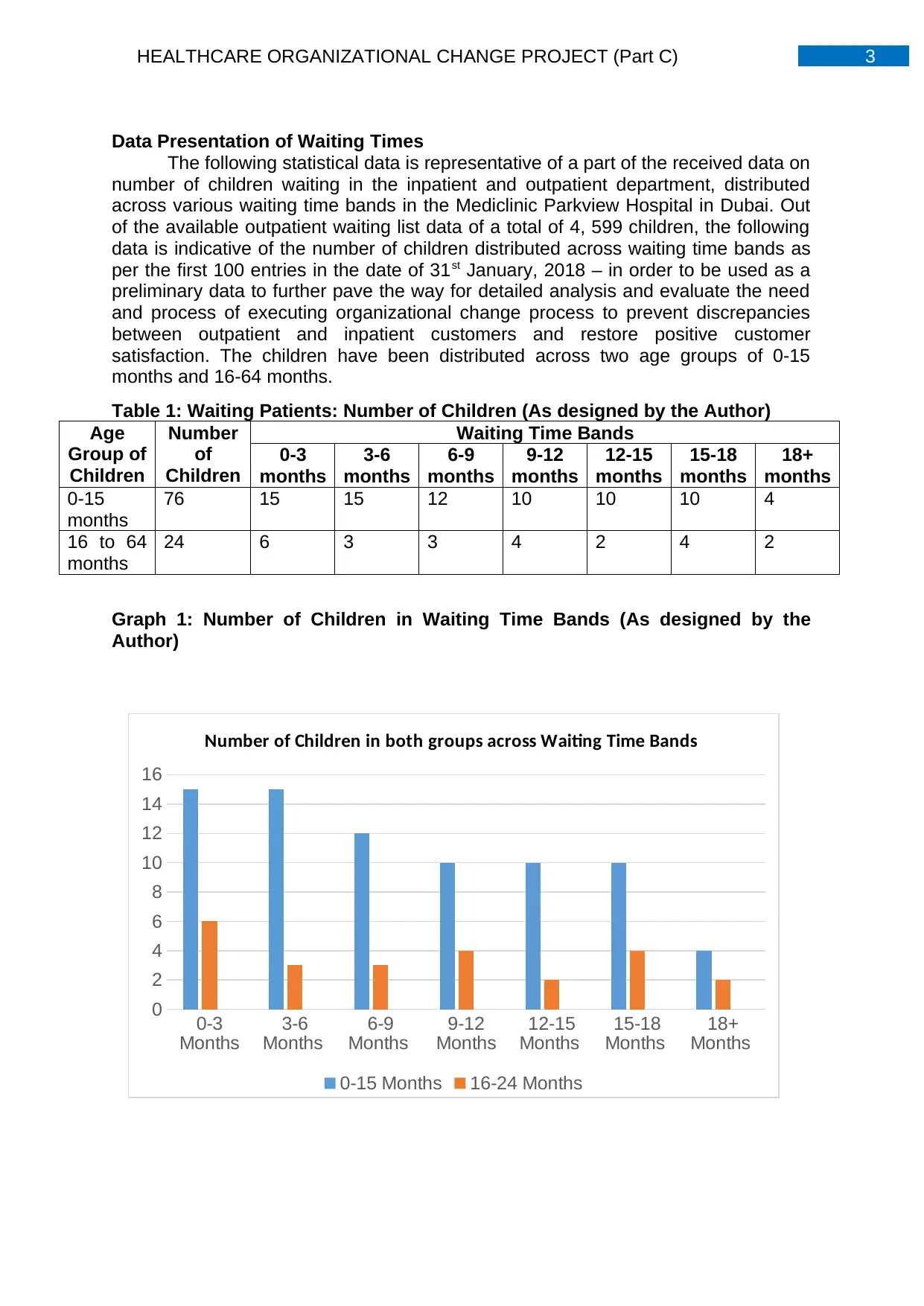
Data Presentation of Waiting Times
The following statistical data is representative of a part of the received data on
number of children waiting in the inpatient and outpatient department, distributed
across various waiting time bands in the Mediclinic Parkview Hospital in Dubai. Out
of the available outpatient waiting list data of a total of 4, 599 children, the following
data is indicative of the number of children distributed across waiting time bands as
per the first 100 entries in the date of 31st January, 2018 – in order to be used as a
preliminary data to further pave the way for detailed analysis and evaluate the need
and process of executing organizational change process to prevent discrepancies
between outpatient and inpatient customers and restore positive customer
satisfaction. The children have been distributed across two age groups of 0-15
months and 16-64 months.
Table 1: Waiting Patients: Number of Children (As designed by the Author)
Age
Group of
Children
Number
of
Children
Waiting Time Bands
0-3
months
3-6
months
6-9
months
9-12
months
12-15
months
15-18
months
18+
months
0-15
months
76 15 15 12 10 10 10 4
16 to 64
months
24 6 3 3 4 2 4 2
Graph 1: Number of Children in Waiting Time Bands (As designed by the
Author)
0-3
Months
3-6
Months
6-9
Months
9-12
Months
12-15
Months
15-18
Months
18+
Months
0
2
4
6
8
10
12
14
16
Number of Children in both groups across Waiting Time Bands
0-15 Months 16-24 Months
Data Presentation of Waiting Times
The following statistical data is representative of a part of the received data on
number of children waiting in the inpatient and outpatient department, distributed
across various waiting time bands in the Mediclinic Parkview Hospital in Dubai. Out
of the available outpatient waiting list data of a total of 4, 599 children, the following
data is indicative of the number of children distributed across waiting time bands as
per the first 100 entries in the date of 31st January, 2018 – in order to be used as a
preliminary data to further pave the way for detailed analysis and evaluate the need
and process of executing organizational change process to prevent discrepancies
between outpatient and inpatient customers and restore positive customer
satisfaction. The children have been distributed across two age groups of 0-15
months and 16-64 months.
Table 1: Waiting Patients: Number of Children (As designed by the Author)
Age
Group of
Children
Number
of
Children
Waiting Time Bands
0-3
months
3-6
months
6-9
months
9-12
months
12-15
months
15-18
months
18+
months
0-15
months
76 15 15 12 10 10 10 4
16 to 64
months
24 6 3 3 4 2 4 2
Graph 1: Number of Children in Waiting Time Bands (As designed by the
Author)
0-3
Months
3-6
Months
6-9
Months
9-12
Months
12-15
Months
15-18
Months
18+
Months
0
2
4
6
8
10
12
14
16
Number of Children in both groups across Waiting Time Bands
0-15 Months 16-24 Months
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
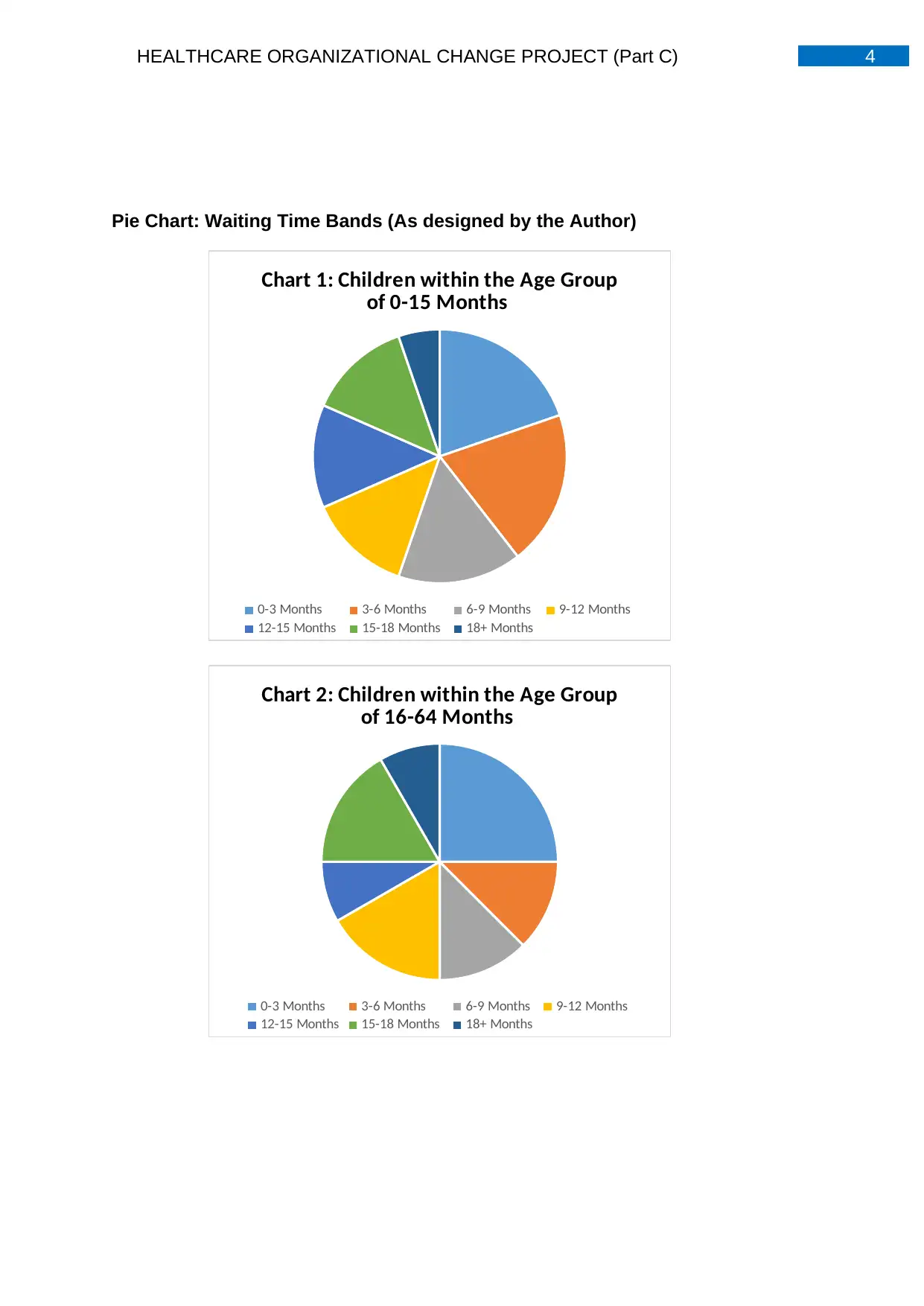
Pie Chart: Waiting Time Bands (As designed by the Author)
Chart 1: Children within the Age Group
of 0-15 Months
0-3 Months 3-6 Months 6-9 Months 9-12 Months
12-15 Months 15-18 Months 18+ Months
Chart 2: Children within the Age Group
of 16-64 Months
0-3 Months 3-6 Months 6-9 Months 9-12 Months
12-15 Months 15-18 Months 18+ Months
Pie Chart: Waiting Time Bands (As designed by the Author)
Chart 1: Children within the Age Group
of 0-15 Months
0-3 Months 3-6 Months 6-9 Months 9-12 Months
12-15 Months 15-18 Months 18+ Months
Chart 2: Children within the Age Group
of 16-64 Months
0-3 Months 3-6 Months 6-9 Months 9-12 Months
12-15 Months 15-18 Months 18+ Months
5HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
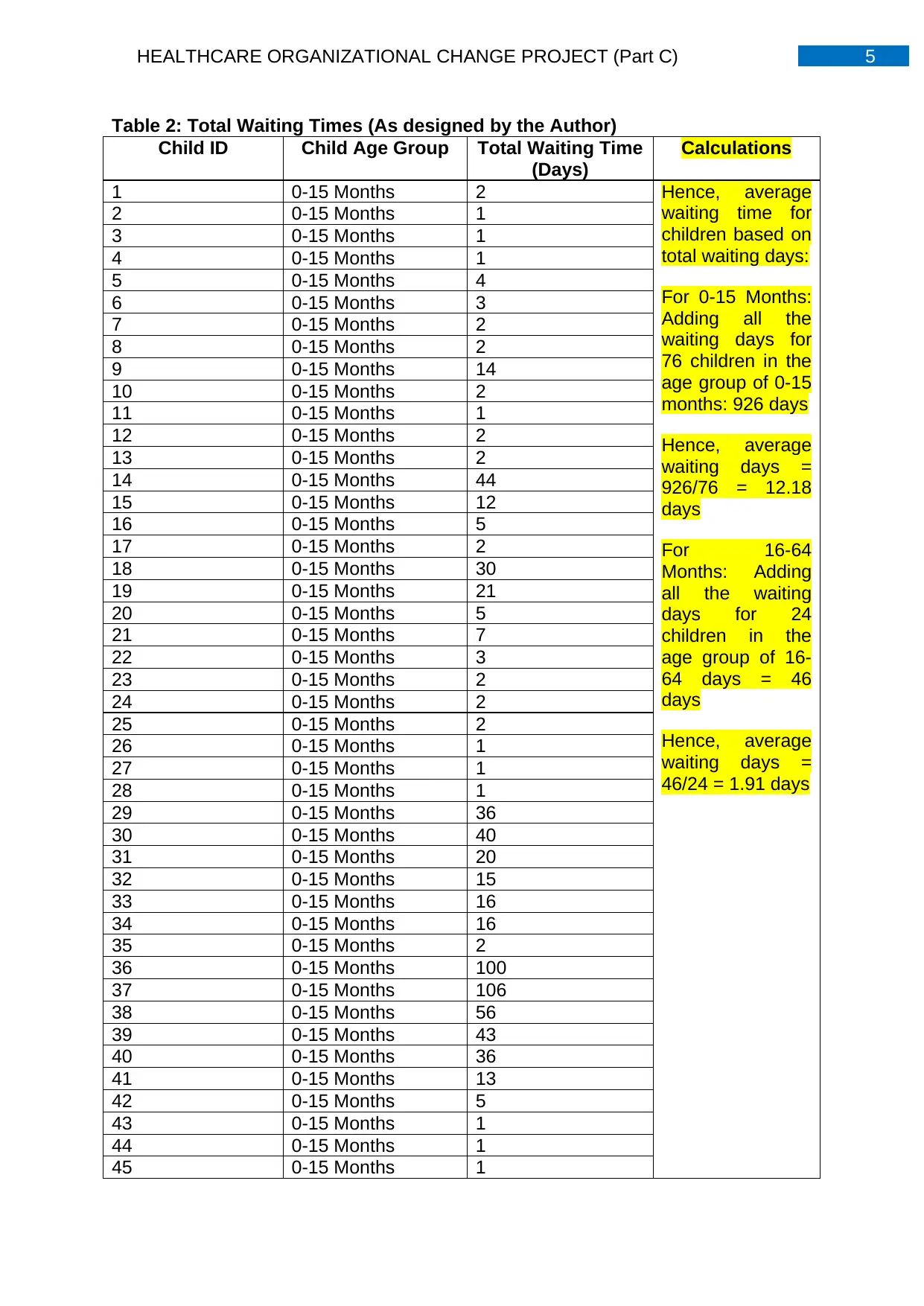
Table 2: Total Waiting Times (As designed by the Author)
Child ID Child Age Group Total Waiting Time
(Days)
Calculations
1 0-15 Months 2 Hence, average
waiting time for
children based on
total waiting days:
For 0-15 Months:
Adding all the
waiting days for
76 children in the
age group of 0-15
months: 926 days
Hence, average
waiting days =
926/76 = 12.18
days
For 16-64
Months: Adding
all the waiting
days for 24
children in the
age group of 16-
64 days = 46
days
Hence, average
waiting days =
46/24 = 1.91 days
2 0-15 Months 1
3 0-15 Months 1
4 0-15 Months 1
5 0-15 Months 4
6 0-15 Months 3
7 0-15 Months 2
8 0-15 Months 2
9 0-15 Months 14
10 0-15 Months 2
11 0-15 Months 1
12 0-15 Months 2
13 0-15 Months 2
14 0-15 Months 44
15 0-15 Months 12
16 0-15 Months 5
17 0-15 Months 2
18 0-15 Months 30
19 0-15 Months 21
20 0-15 Months 5
21 0-15 Months 7
22 0-15 Months 3
23 0-15 Months 2
24 0-15 Months 2
25 0-15 Months 2
26 0-15 Months 1
27 0-15 Months 1
28 0-15 Months 1
29 0-15 Months 36
30 0-15 Months 40
31 0-15 Months 20
32 0-15 Months 15
33 0-15 Months 16
34 0-15 Months 16
35 0-15 Months 2
36 0-15 Months 100
37 0-15 Months 106
38 0-15 Months 56
39 0-15 Months 43
40 0-15 Months 36
41 0-15 Months 13
42 0-15 Months 5
43 0-15 Months 1
44 0-15 Months 1
45 0-15 Months 1
Table 2: Total Waiting Times (As designed by the Author)
Child ID Child Age Group Total Waiting Time
(Days)
Calculations
1 0-15 Months 2 Hence, average
waiting time for
children based on
total waiting days:
For 0-15 Months:
Adding all the
waiting days for
76 children in the
age group of 0-15
months: 926 days
Hence, average
waiting days =
926/76 = 12.18
days
For 16-64
Months: Adding
all the waiting
days for 24
children in the
age group of 16-
64 days = 46
days
Hence, average
waiting days =
46/24 = 1.91 days
2 0-15 Months 1
3 0-15 Months 1
4 0-15 Months 1
5 0-15 Months 4
6 0-15 Months 3
7 0-15 Months 2
8 0-15 Months 2
9 0-15 Months 14
10 0-15 Months 2
11 0-15 Months 1
12 0-15 Months 2
13 0-15 Months 2
14 0-15 Months 44
15 0-15 Months 12
16 0-15 Months 5
17 0-15 Months 2
18 0-15 Months 30
19 0-15 Months 21
20 0-15 Months 5
21 0-15 Months 7
22 0-15 Months 3
23 0-15 Months 2
24 0-15 Months 2
25 0-15 Months 2
26 0-15 Months 1
27 0-15 Months 1
28 0-15 Months 1
29 0-15 Months 36
30 0-15 Months 40
31 0-15 Months 20
32 0-15 Months 15
33 0-15 Months 16
34 0-15 Months 16
35 0-15 Months 2
36 0-15 Months 100
37 0-15 Months 106
38 0-15 Months 56
39 0-15 Months 43
40 0-15 Months 36
41 0-15 Months 13
42 0-15 Months 5
43 0-15 Months 1
44 0-15 Months 1
45 0-15 Months 1
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
46 0-15 Months 38
47 0-15 Months 25
48 0-15 Months 13
49 0-15 Months 2
50 0-15 Months 1
51 0-15 Months 3
52 0-15 Months 10
53 0-15 Months 3
54 0-15 Months 1
55 0-15 Months 1
56 0-15 Months 3
57 0-15 Months 1
58 0-15 Months 1
59 0-15 Months 1
60 0-15 Months 1
61 0-15 Months 2
62 0-15 Months 20
63 0-15 Months 13
64 0-15 Months 10
65 0-15 Months 10
67 0-15 Months 14
68 0-15 Months 5
69 0-15 Months 25
70 0-15 Months 11
71 0-15 Months 13
72 0-15 Months 6
73 0-15 Months 3
74 0-15 Months 2
75 0-15 Months 2
76 0-15 Months 1
77 16-64 Months 1
78 16-64 Months 1
79 16-64 Months 1
80 16-64 Months 4
81 16-64 Months 4
82 16-64 Months 4
83 16-64 Months 3
84 16-64 Months 3
85 16-64 Months 2
86 16-64 Months 2
87 16-64 Months 2
88 16-64 Months 3
89 16-64 Months 1
90 16-64 Months 2
91 16-64 Months 1
92 16-64 Months 3
93 16-64 Months 1
94 16-64 Months 1
46 0-15 Months 38
47 0-15 Months 25
48 0-15 Months 13
49 0-15 Months 2
50 0-15 Months 1
51 0-15 Months 3
52 0-15 Months 10
53 0-15 Months 3
54 0-15 Months 1
55 0-15 Months 1
56 0-15 Months 3
57 0-15 Months 1
58 0-15 Months 1
59 0-15 Months 1
60 0-15 Months 1
61 0-15 Months 2
62 0-15 Months 20
63 0-15 Months 13
64 0-15 Months 10
65 0-15 Months 10
67 0-15 Months 14
68 0-15 Months 5
69 0-15 Months 25
70 0-15 Months 11
71 0-15 Months 13
72 0-15 Months 6
73 0-15 Months 3
74 0-15 Months 2
75 0-15 Months 2
76 0-15 Months 1
77 16-64 Months 1
78 16-64 Months 1
79 16-64 Months 1
80 16-64 Months 4
81 16-64 Months 4
82 16-64 Months 4
83 16-64 Months 3
84 16-64 Months 3
85 16-64 Months 2
86 16-64 Months 2
87 16-64 Months 2
88 16-64 Months 3
89 16-64 Months 1
90 16-64 Months 2
91 16-64 Months 1
92 16-64 Months 3
93 16-64 Months 1
94 16-64 Months 1
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
95 16-64 Months 1
96 16-64 Months 1
97 16-64 Months 1
98 16-64 Months 1
99 16-64 Months 1
100 16-64 Months 2
95 16-64 Months 1
96 16-64 Months 1
97 16-64 Months 1
98 16-64 Months 1
99 16-64 Months 1
100 16-64 Months 2
8HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
0-15
Months
16-64
Months
0
2
4
6
8
10
12
14
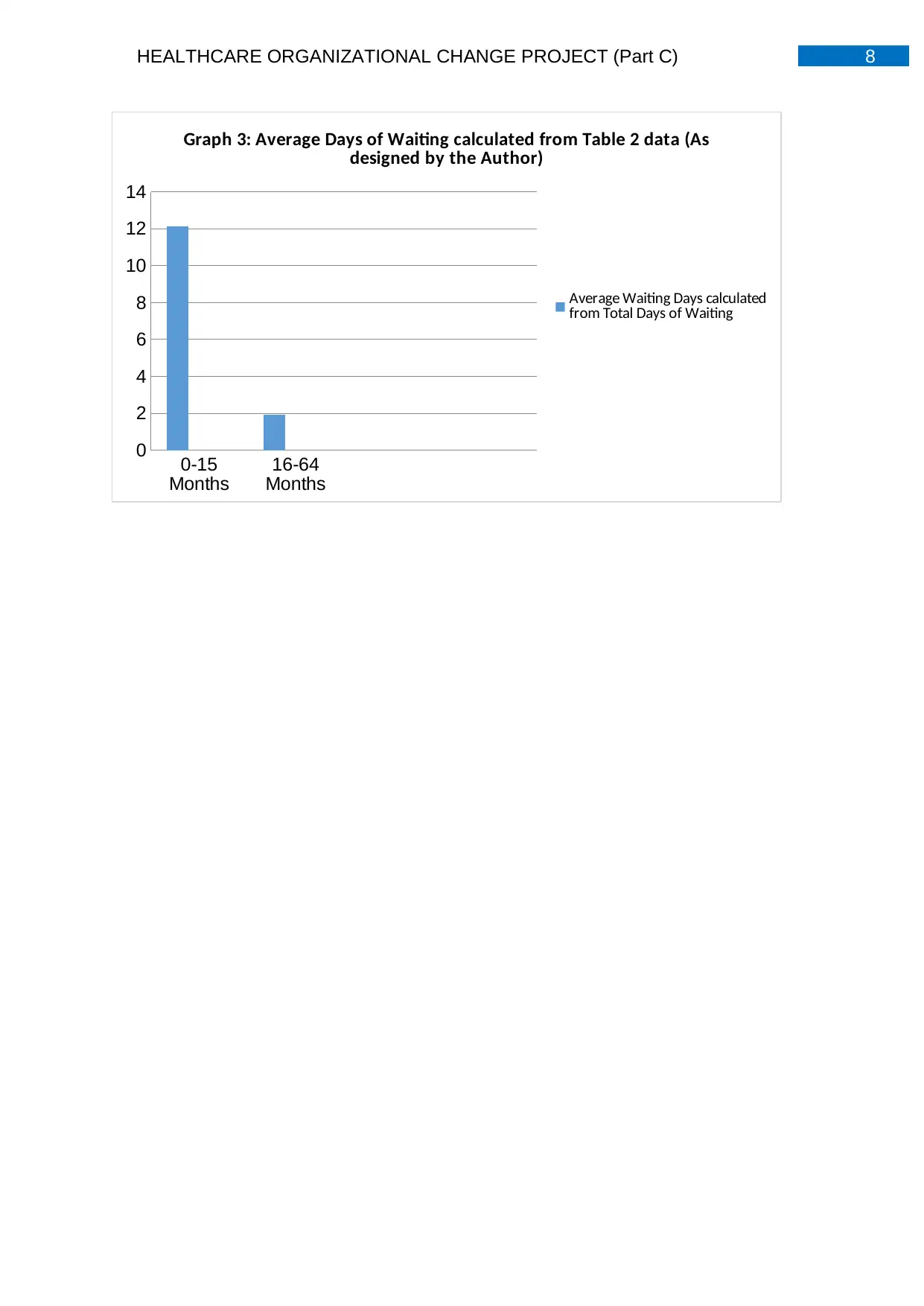
Graph 3: Average Days of Waiting calculated from Table 2 data (As
designed by the Author)
Average Waiting Days calculated
from Total Days of Waiting
0-15
Months
16-64
Months
0
2
4
6
8
10
12
14
Graph 3: Average Days of Waiting calculated from Table 2 data (As
designed by the Author)
Average Waiting Days calculated
from Total Days of Waiting
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
Data Summary
The above data represents the first 100 entries of the children belonging to a
prolonged waiting list in the inpatient and outpatient department of the Mediclinic
Parkview Hospital, Dubai, United Arab Emirates. From Table 1 it can be observed
that an increased number of younger children within the age group of 0-15 months
have been in the inpatient and outpatient waiting list for a long time, as compared to
the children in the age group 16-64 monthsFrom the graphs it can be observed that
the time band containing the largest number of waiting children across both age
groups, is that of 0-3 months followed by 9-12 months and 15-18 months, with the
least number of children belonging to the time band of 18+ months. Pie Chart 1
indicates that the largest number of waiting list inpatient and inpatient and outpatient
children in the age group of 0-15 months belong to the time band of 0-3 months,
followed by time bands of 3-6, 6-9, 9-12, 12-15, 15-18 and 18+ months. Pie Chart 2
indicates that the largest number of waiting list inpatient and outpatient children in
the age group of 16-64 months belong to the time band of 0-3 months, followed by 9-
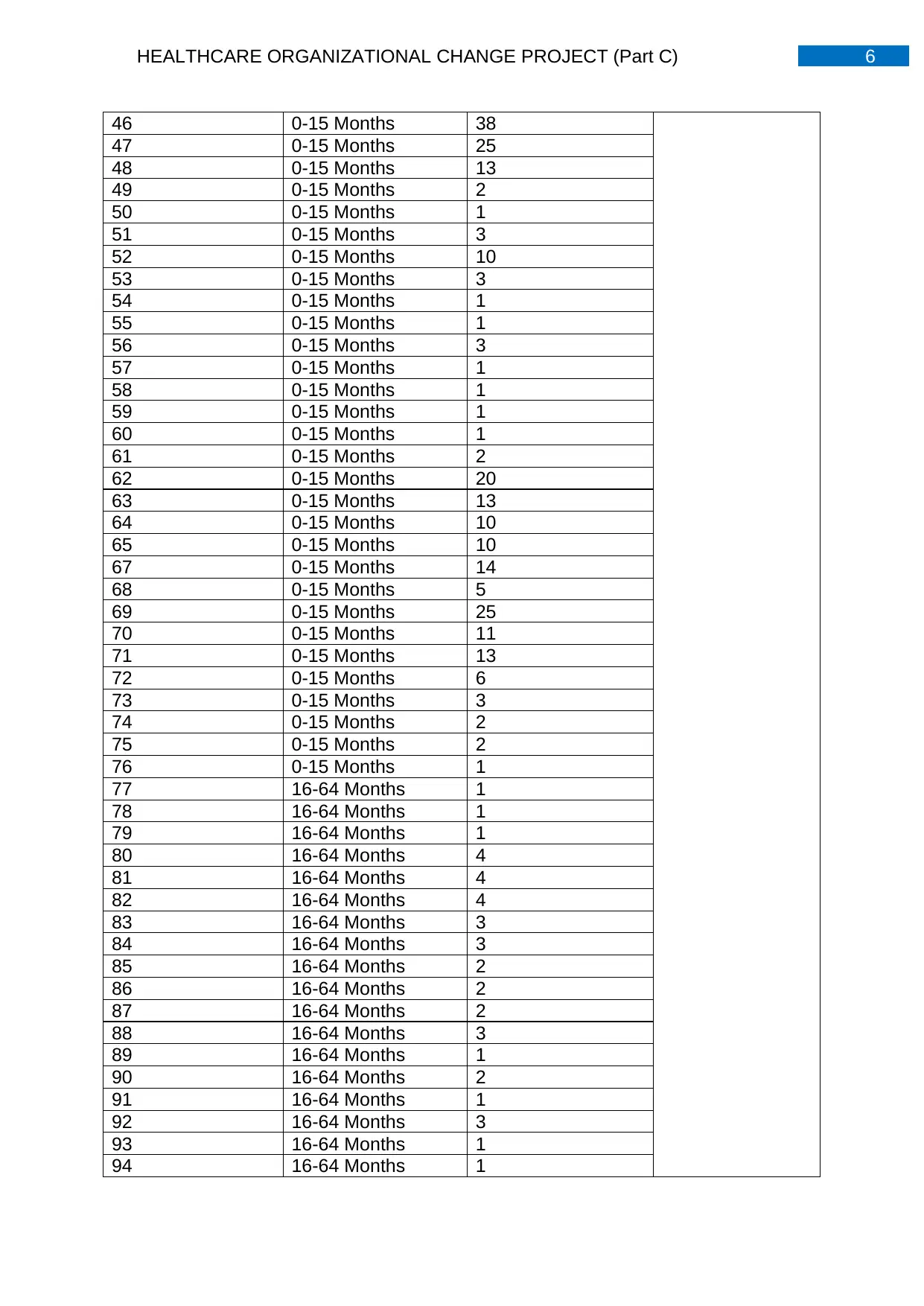
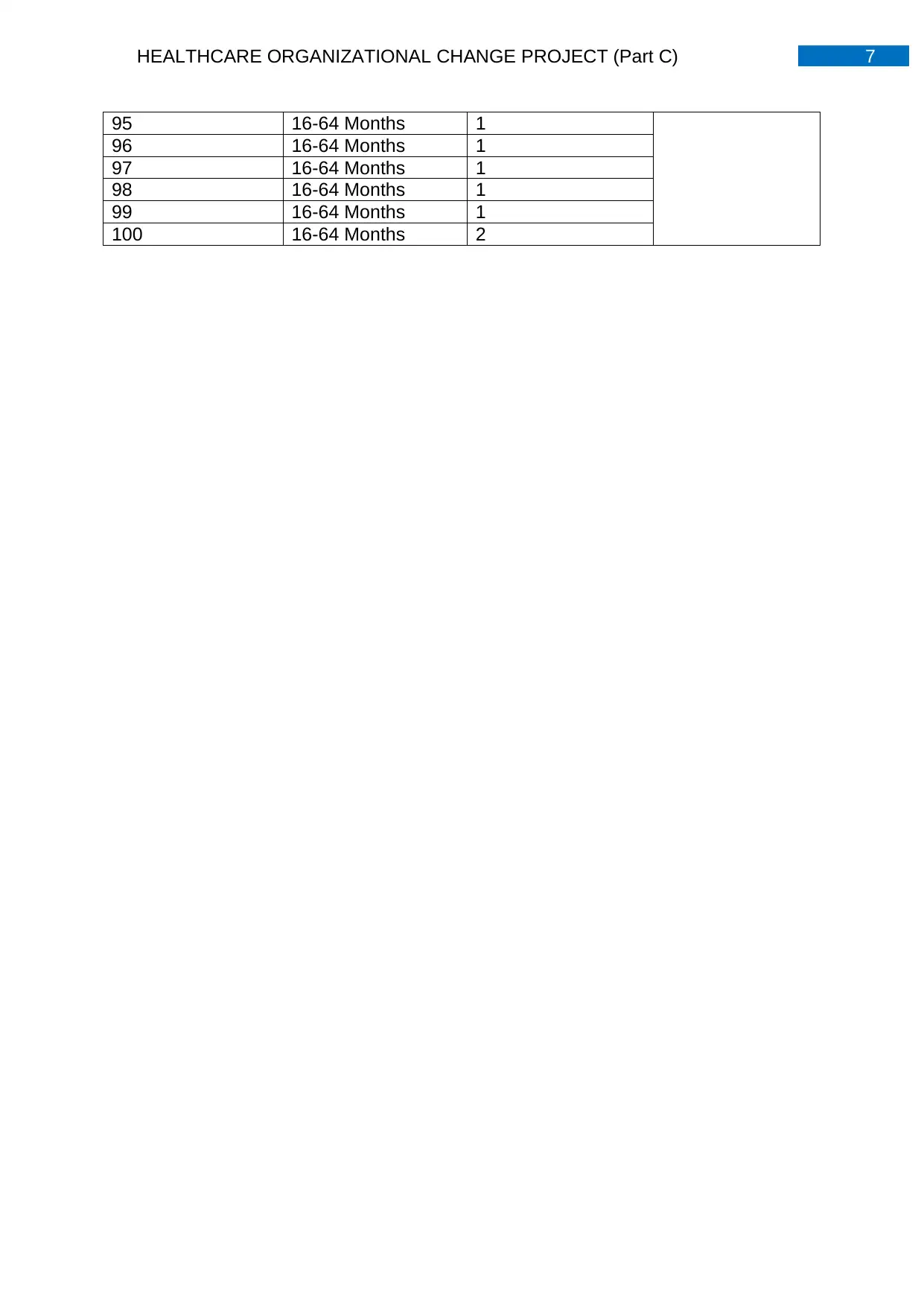
12, 15-18, 3-6, 6-9, 12-15 and 18+ months. From Table 2 it can be observed that the
inpatient and outpatient children are unequally distributed in terms of number of days
in waiting, which further indicates a discrepancy in data represented by waiting time
band distributions. While a large number of children seem to be in line for treatment
for less than 5 days, a number of children have been in the waiting list for almost
more than 20 days and often extending alarmingly to more than 100 days, indicating
data extremities which have been masked by the data represented by time bands.
Additional Data Limitations and Recommendations
The following limitations can be observed: it can be observed that Medical
services such as psychology, X-rays, speech and language therapy, diagnostic
services and dietetics have been excluded from the data collection. Hence, it is
recommended that a more comprehensive data collection be performed involving all
medical departments which indicate comparative analysis across various
departments of the hospital resulting in avoidance of discrimination (Mutondo,
Farolfi& Dinar, 2016). Further, it was observed that the data represents waiting list
details for every day across seven months of the year 2018, which made it very
difficult and time consuming to analyse the vast data resulting in consideration of the
first 100 entries for want of time. Hence, it is recommended that the data be
clustered and segregated further resulting in filtering to inpatient and outpatient data
for every month. Such forms of data filtering and classification will enhance the ease
with which data can be analysed since the number of inpatient and outpatient
children can be compared across various months and the data can be viewed for
every month leading to less confusion and time constraints associated with a
analysing a large chunk of data for each data across seven months (Miller, Nagy
&Schlueter, 2015).For improved health organization change process and enhanced
customer satisfaction, obtaining information on the customer’s needs is also
necessary. Hence, in addition to the available data, conducting feedback surveys
among the parents of the inpatient and outpatient children is recommended since it
will provide key insights of the client’s expectations and hospital services which are
attracting negative customer feedback (Guetterman, Fetters & Creswell, 2015).
Hence, it is recommended that provision of complete interdepartmental information,
data clustering and filtering and obtaining customer feedback be additionally
Data Summary
The above data represents the first 100 entries of the children belonging to a
prolonged waiting list in the inpatient and outpatient department of the Mediclinic
Parkview Hospital, Dubai, United Arab Emirates. From Table 1 it can be observed
that an increased number of younger children within the age group of 0-15 months
have been in the inpatient and outpatient waiting list for a long time, as compared to
the children in the age group 16-64 monthsFrom the graphs it can be observed that
the time band containing the largest number of waiting children across both age
groups, is that of 0-3 months followed by 9-12 months and 15-18 months, with the
least number of children belonging to the time band of 18+ months. Pie Chart 1
indicates that the largest number of waiting list inpatient and inpatient and outpatient
children in the age group of 0-15 months belong to the time band of 0-3 months,
followed by time bands of 3-6, 6-9, 9-12, 12-15, 15-18 and 18+ months. Pie Chart 2
indicates that the largest number of waiting list inpatient and outpatient children in
the age group of 16-64 months belong to the time band of 0-3 months, followed by 9-
12, 15-18, 3-6, 6-9, 12-15 and 18+ months. From Table 2 it can be observed that the
inpatient and outpatient children are unequally distributed in terms of number of days
in waiting, which further indicates a discrepancy in data represented by waiting time
band distributions. While a large number of children seem to be in line for treatment
for less than 5 days, a number of children have been in the waiting list for almost
more than 20 days and often extending alarmingly to more than 100 days, indicating
data extremities which have been masked by the data represented by time bands.
Additional Data Limitations and Recommendations
The following limitations can be observed: it can be observed that Medical
services such as psychology, X-rays, speech and language therapy, diagnostic
services and dietetics have been excluded from the data collection. Hence, it is
recommended that a more comprehensive data collection be performed involving all
medical departments which indicate comparative analysis across various
departments of the hospital resulting in avoidance of discrimination (Mutondo,
Farolfi& Dinar, 2016). Further, it was observed that the data represents waiting list
details for every day across seven months of the year 2018, which made it very
difficult and time consuming to analyse the vast data resulting in consideration of the
first 100 entries for want of time. Hence, it is recommended that the data be
clustered and segregated further resulting in filtering to inpatient and outpatient data
for every month. Such forms of data filtering and classification will enhance the ease
with which data can be analysed since the number of inpatient and outpatient
children can be compared across various months and the data can be viewed for
every month leading to less confusion and time constraints associated with a
analysing a large chunk of data for each data across seven months (Miller, Nagy
&Schlueter, 2015).For improved health organization change process and enhanced
customer satisfaction, obtaining information on the customer’s needs is also
necessary. Hence, in addition to the available data, conducting feedback surveys
among the parents of the inpatient and outpatient children is recommended since it
will provide key insights of the client’s expectations and hospital services which are
attracting negative customer feedback (Guetterman, Fetters & Creswell, 2015).
Hence, it is recommended that provision of complete interdepartmental information,
data clustering and filtering and obtaining customer feedback be additionally
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
performed for procuring clarified data on key areas of change resulting in enhanced
execution of change process (Semrau et al., 2017).
Ethical Concerns
The personal information of every children must be kept confidential and
anonymous to protect patient privacy, and if revealed, a letter of ‘no disclosure’ must
be attached prior to handing over the essential information. Informed consent must
be obtained from all the parents of the children belonging to the waiting list of the
inpatient and outpatient department, in case of any requirement of assessing the
personal profiles of their concerned children (Vayena et al., 2015).Further the
Information Technology department must ensure that the high levels of security are
maintained and the data is accessible to only authorised professionals in order to
avoid any breach of security, leaking or misuse of the concerned data by unwanted
or unauthorised parties (Docherty & Lone, 2015).In order to further maintain the
ethical concern of patient safety, privacy and confidentiality, appropriate software
and well-functioning computers or databases must be used which will be less likely
to incur technical glitches or security breaches by hackers or unwanted parties
(Phillips, 2015).
performed for procuring clarified data on key areas of change resulting in enhanced
execution of change process (Semrau et al., 2017).
Ethical Concerns
The personal information of every children must be kept confidential and
anonymous to protect patient privacy, and if revealed, a letter of ‘no disclosure’ must
be attached prior to handing over the essential information. Informed consent must
be obtained from all the parents of the children belonging to the waiting list of the
inpatient and outpatient department, in case of any requirement of assessing the
personal profiles of their concerned children (Vayena et al., 2015).Further the
Information Technology department must ensure that the high levels of security are
maintained and the data is accessible to only authorised professionals in order to
avoid any breach of security, leaking or misuse of the concerned data by unwanted
or unauthorised parties (Docherty & Lone, 2015).In order to further maintain the
ethical concern of patient safety, privacy and confidentiality, appropriate software
and well-functioning computers or databases must be used which will be less likely
to incur technical glitches or security breaches by hackers or unwanted parties
(Phillips, 2015).
11HEALTHCARE ORGANIZATIONAL CHANGE PROJECT (Part C)
References
Docherty, A. B., & Lone, N. I. (2015). Exploiting big data for critical care research.
Current opinion in critical care, 21(5), 467-472.
Guetterman, T. C., Fetters, M. D., & Creswell, J. W. (2015). Integrating quantitative
and qualitative results in health science mixed methods research through joint
displays. The Annals of Family Medicine, 13(6), 554-561.
Miller, C., Nagy, Z., &Schlueter, A. (2015). Automated daily pattern filtering of
measured building performance data. Automation in Construction, 49, 1-17.
Mutondo, J., Farolfi, S., & Dinar, A. (2016). Quantitative Analysis: Empirical Models
and Data Collection Process. In Water Governance Decentralization in Sub-
Saharan Africa (pp. 35-41). Springer, Cham.
Phillips, W. (2015). Ethical controversies about proper health informatics practices.
Missouri Medicine, 112(1), 53.
Semrau, M., Lempp, H., Keynejad, R., Evans-Lacko, S., Mugisha, J., Raja, S., ...&
Hanlon, C. (2016). Service user and caregiver involvement in mental health
system strengthening in low-and middle-income countries: systematic review.
BMC health services research, 16(1), 79.
Vayena, E., Salathé, M., Madoff, L. C., & Brownstein, J. S. (2015). Ethical challenges
of big data in public health. PLoS computational biology, 11(2), e1003904.
References
Docherty, A. B., & Lone, N. I. (2015). Exploiting big data for critical care research.
Current opinion in critical care, 21(5), 467-472.
Guetterman, T. C., Fetters, M. D., & Creswell, J. W. (2015). Integrating quantitative
and qualitative results in health science mixed methods research through joint
displays. The Annals of Family Medicine, 13(6), 554-561.
Miller, C., Nagy, Z., &Schlueter, A. (2015). Automated daily pattern filtering of
measured building performance data. Automation in Construction, 49, 1-17.
Mutondo, J., Farolfi, S., & Dinar, A. (2016). Quantitative Analysis: Empirical Models
and Data Collection Process. In Water Governance Decentralization in Sub-
Saharan Africa (pp. 35-41). Springer, Cham.
Phillips, W. (2015). Ethical controversies about proper health informatics practices.
Missouri Medicine, 112(1), 53.
Semrau, M., Lempp, H., Keynejad, R., Evans-Lacko, S., Mugisha, J., Raja, S., ...&
Hanlon, C. (2016). Service user and caregiver involvement in mental health
system strengthening in low-and middle-income countries: systematic review.
BMC health services research, 16(1), 79.
Vayena, E., Salathé, M., Madoff, L. C., & Brownstein, J. S. (2015). Ethical challenges
of big data in public health. PLoS computational biology, 11(2), e1003904.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.