Reflective Analysis: Patient Complaint and Holistic Surgical Care
VerifiedAdded on 2022/11/23
|12
|3730
|413
Report
AI Summary
This report presents a reflective analysis of a surgical patient's complaint within an operating department setting, utilizing the Gibbs reflective cycle to examine the incident. The report begins with an introduction to reflective practice, emphasizing its importance in healthcare and the use of the Gibbs model for structuring the reflection. The core of the report involves a detailed description of the patient's complaint, focusing on issues of communication, infection control, and overall patient care. The student reflects on their feelings, evaluates the positives and negatives of the situation, and analyzes the root causes of the problems, including poor communication, infection control breaches, and safety concerns. The analysis highlights the importance of adhering to professional guidelines from HCPC and NICE. The report concludes with a summary of lessons learned and proposes an action plan for future practice, emphasizing the need for improved communication, adherence to infection control protocols, and a commitment to patient safety and dignity. The report underscores the need for assertive patient advocacy and a commitment to providing holistic care.
Holistic Care of the Surgical Patient
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of contents
INTRODUCTION...........................................................................................................................3
Reflective cycle...........................................................................................................................4
Description...................................................................................................................................4
Feelings........................................................................................................................................4
Analysis.......................................................................................................................................6
Conclusion to the cycle................................................................................................................8
Overall summary.........................................................................................................................9
REFRENCES.................................................................................................................................10
INTRODUCTION...........................................................................................................................3
Reflective cycle...........................................................................................................................4
Description...................................................................................................................................4
Feelings........................................................................................................................................4
Analysis.......................................................................................................................................6
Conclusion to the cycle................................................................................................................8
Overall summary.........................................................................................................................9
REFRENCES.................................................................................................................................10
INTRODUCTION
The assignment is about the student in the operating department practitioner will be reflecting on
the patients complaint on the pay. The confidentiality of the patient is maintained by the
guidance from the General Data Protection and Health (GDPR, 2018) and Care Professionals
Council (HCPC, 2016), this is done by referring the people by their roles.
The different industries such as the education, healthcare and therapy use reflective practice as
the key aspect, the reflective practitioner is able to learn from their mistakes as well as help in
improving the practise. MacCallum and Casey (2017) said that the reflective practise for the
naïve practitioner can be difficult process that can lead to the under-confidence or self-criticism
and this is very problematic. Thus, the experienced practitioner should be helping and supporting
the naïve practitioner in the reflection. The reflection for a practitioner can be negative, positive,
small and large but for more of the time it is found to be negative. According to Jarvis and
Baloyi (2020), the reflection is either in or on action. The in action means active reflection while
on action means after the event the retrospective reflection. The naïve practitioner finds it much
more difficult to achieve the reflection-in-action and the practitioner finds it easier to achieve the
reflection-on-action. The practitioner becomes more fluent with the reflection-on-action as
compared to the reflection-in-action. This will be appropriate as the author of the naïve
practitioner will be reflecting the occurred incident.
The reflection in the health care is very important as it help in bridging the theory-practise gap
for the practitioner though making them learn the new theories and applying in to the practise.
This help in improving the practice of the practitioner by the evidence based measures (Wu and
et.al, 2018). The HDPC ensures that the registrants are capable of reflecting and improving their
practice, the key part of being a worker as a registered healthcare professional is continuously
involving in the actions that are improving the practise as well as quality of care along with the
safety of the patient and learning from the mistakes.
The reflective models are suggested to the practitioners as the framework of the reflective model
is will guide them in the reflection that is difficult or complex in the starting. WIDIASTUTI and
BUDIYANTO (2018) suggest that using Kolb’s Experimental Learning Cycle for the reflection
by the naïve practitioner. The Kolb’s Experimental Learning Cycle ha four phases that are
concrete experience, abstract conceptualisation, active experimentation and reflective
observation. The author also suggests that the practitioner might find it difficult as the Kolb’s
The assignment is about the student in the operating department practitioner will be reflecting on
the patients complaint on the pay. The confidentiality of the patient is maintained by the
guidance from the General Data Protection and Health (GDPR, 2018) and Care Professionals
Council (HCPC, 2016), this is done by referring the people by their roles.
The different industries such as the education, healthcare and therapy use reflective practice as
the key aspect, the reflective practitioner is able to learn from their mistakes as well as help in
improving the practise. MacCallum and Casey (2017) said that the reflective practise for the
naïve practitioner can be difficult process that can lead to the under-confidence or self-criticism
and this is very problematic. Thus, the experienced practitioner should be helping and supporting
the naïve practitioner in the reflection. The reflection for a practitioner can be negative, positive,
small and large but for more of the time it is found to be negative. According to Jarvis and
Baloyi (2020), the reflection is either in or on action. The in action means active reflection while
on action means after the event the retrospective reflection. The naïve practitioner finds it much
more difficult to achieve the reflection-in-action and the practitioner finds it easier to achieve the
reflection-on-action. The practitioner becomes more fluent with the reflection-on-action as
compared to the reflection-in-action. This will be appropriate as the author of the naïve
practitioner will be reflecting the occurred incident.
The reflection in the health care is very important as it help in bridging the theory-practise gap
for the practitioner though making them learn the new theories and applying in to the practise.
This help in improving the practice of the practitioner by the evidence based measures (Wu and
et.al, 2018). The HDPC ensures that the registrants are capable of reflecting and improving their
practice, the key part of being a worker as a registered healthcare professional is continuously
involving in the actions that are improving the practise as well as quality of care along with the
safety of the patient and learning from the mistakes.
The reflective models are suggested to the practitioners as the framework of the reflective model
is will guide them in the reflection that is difficult or complex in the starting. WIDIASTUTI and
BUDIYANTO (2018) suggest that using Kolb’s Experimental Learning Cycle for the reflection
by the naïve practitioner. The Kolb’s Experimental Learning Cycle ha four phases that are
concrete experience, abstract conceptualisation, active experimentation and reflective
observation. The author also suggests that the practitioner might find it difficult as the Kolb’s
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Experimental Learning Cycle lack of the structural guidance. On the other hand Adeani, Febriani
and Syafryadin (2020) suggest that Gibb’s reflective cycle is the easy to use by the naïve
practitioner. The Gibb’s reflective cycle includes six stages that are descriptions of the event,
feelings of the practitioner, evaluation for the identification of the positives as well as negatives,
analysis of the event and conclusion of the cycle of the event along with the action plan where
the actions that can be done different the next time. The assignment will be using the Gibb’s
reflective cycle as it is more appropriate for the naïve practitioner along with this it suits the
learning cycle of the students. The Gibb’s reflective cycle is used for the structuring of the
assignment. This will be focusing on the surrounding issues that are maintaining a safe
environment, communication and infection control.
Reflective cycle
The Gibb’s model is the famous cyclic model of the reflection that helps lead to the six stages for
the exploration of an experience by the practitioner. It gives the learning from the experience. It
also provides with the framework for examining the experience and the cyclic nature repeat the
experiences that help in learning through the things that went well and that does not (Markkanen
and et.al, 2020). The six stages are:
Description of the event.
Feelings about the experience.
Evaluation of the event for the good and the bad.
Analysis for making sense out of the event.
Conclusion of what has been learned.
Action plan for the things that can be done differently the next time.
Description
The student of ODP is given the complaint of the patient from the theatres and is asked to reflect
using the Gibbs reflective cycle that need to be focused upon the aspects of holistic care,
infection control, communication and maintenance (Fergusson, van der Laan and Baker, 2019).
Feelings
The student after reading the complaint of the patient felt very ashamed and distressed the way
the patient is been treated. The student felt really bad for the patient as they had to go through
such traumatic phase and was angry as nobody helped the patient. The student as angry as many
and Syafryadin (2020) suggest that Gibb’s reflective cycle is the easy to use by the naïve
practitioner. The Gibb’s reflective cycle includes six stages that are descriptions of the event,
feelings of the practitioner, evaluation for the identification of the positives as well as negatives,
analysis of the event and conclusion of the cycle of the event along with the action plan where
the actions that can be done different the next time. The assignment will be using the Gibb’s
reflective cycle as it is more appropriate for the naïve practitioner along with this it suits the
learning cycle of the students. The Gibb’s reflective cycle is used for the structuring of the
assignment. This will be focusing on the surrounding issues that are maintaining a safe
environment, communication and infection control.
Reflective cycle
The Gibb’s model is the famous cyclic model of the reflection that helps lead to the six stages for
the exploration of an experience by the practitioner. It gives the learning from the experience. It
also provides with the framework for examining the experience and the cyclic nature repeat the
experiences that help in learning through the things that went well and that does not (Markkanen
and et.al, 2020). The six stages are:
Description of the event.
Feelings about the experience.
Evaluation of the event for the good and the bad.
Analysis for making sense out of the event.
Conclusion of what has been learned.
Action plan for the things that can be done differently the next time.
Description
The student of ODP is given the complaint of the patient from the theatres and is asked to reflect
using the Gibbs reflective cycle that need to be focused upon the aspects of holistic care,
infection control, communication and maintenance (Fergusson, van der Laan and Baker, 2019).
Feelings
The student after reading the complaint of the patient felt very ashamed and distressed the way
the patient is been treated. The student felt really bad for the patient as they had to go through
such traumatic phase and was angry as nobody helped the patient. The student as angry as many
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
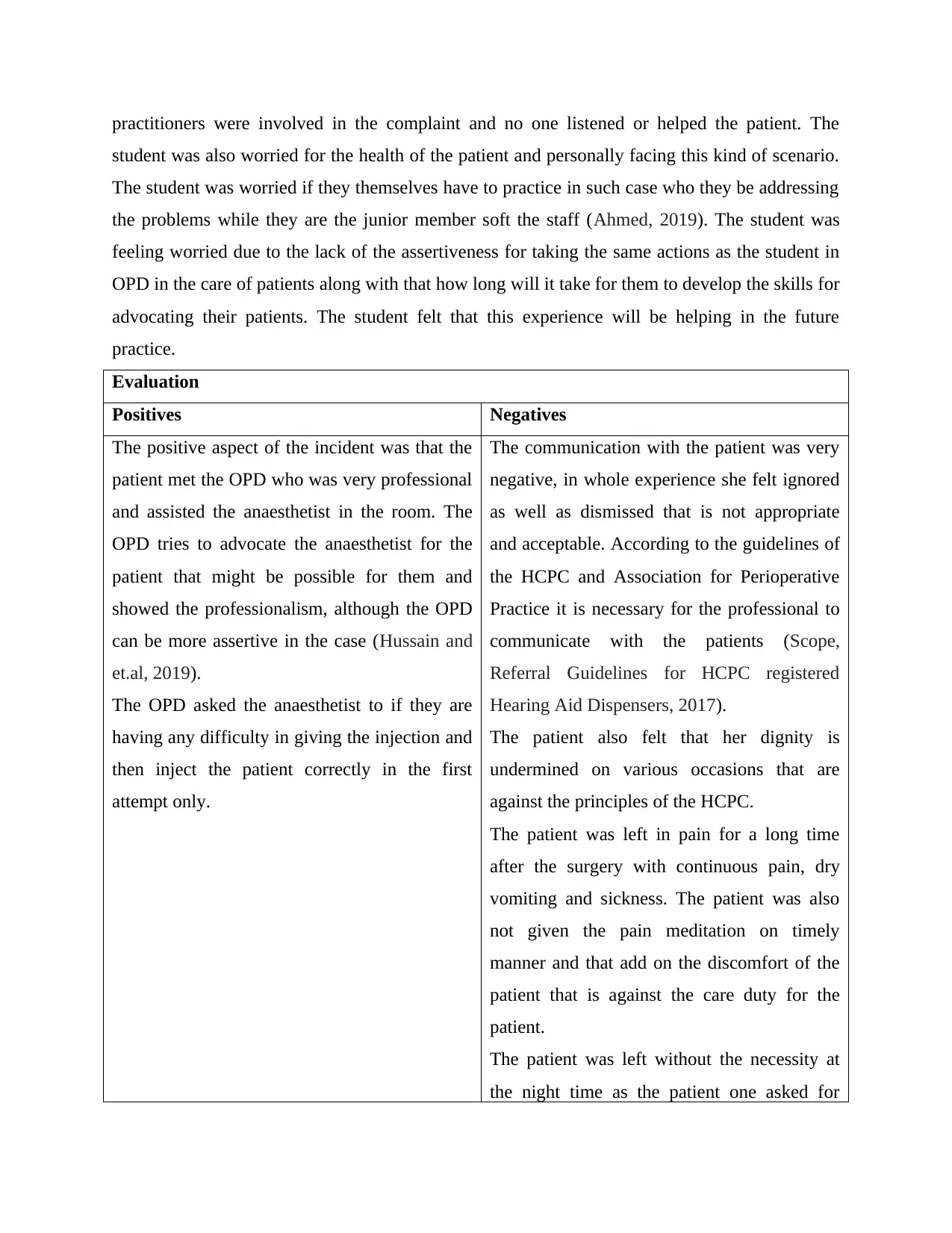
practitioners were involved in the complaint and no one listened or helped the patient. The
student was also worried for the health of the patient and personally facing this kind of scenario.
The student was worried if they themselves have to practice in such case who they be addressing
the problems while they are the junior member soft the staff (Ahmed, 2019). The student was
feeling worried due to the lack of the assertiveness for taking the same actions as the student in
OPD in the care of patients along with that how long will it take for them to develop the skills for
advocating their patients. The student felt that this experience will be helping in the future
practice.
Evaluation
Positives Negatives
The positive aspect of the incident was that the
patient met the OPD who was very professional
and assisted the anaesthetist in the room. The
OPD tries to advocate the anaesthetist for the
patient that might be possible for them and
showed the professionalism, although the OPD
can be more assertive in the case (Hussain and
et.al, 2019).
The OPD asked the anaesthetist to if they are
having any difficulty in giving the injection and
then inject the patient correctly in the first
attempt only.
The communication with the patient was very
negative, in whole experience she felt ignored
as well as dismissed that is not appropriate
and acceptable. According to the guidelines of
the HCPC and Association for Perioperative
Practice it is necessary for the professional to
communicate with the patients (Scope,
Referral Guidelines for HCPC registered
Hearing Aid Dispensers, 2017).
The patient also felt that her dignity is
undermined on various occasions that are
against the principles of the HCPC.
The patient was left in pain for a long time
after the surgery with continuous pain, dry
vomiting and sickness. The patient was also
not given the pain meditation on timely
manner and that add on the discomfort of the
patient that is against the care duty for the
patient.
The patient was left without the necessity at
the night time as the patient one asked for
student was also worried for the health of the patient and personally facing this kind of scenario.
The student was worried if they themselves have to practice in such case who they be addressing
the problems while they are the junior member soft the staff (Ahmed, 2019). The student was
feeling worried due to the lack of the assertiveness for taking the same actions as the student in
OPD in the care of patients along with that how long will it take for them to develop the skills for
advocating their patients. The student felt that this experience will be helping in the future
practice.
Evaluation
Positives Negatives
The positive aspect of the incident was that the
patient met the OPD who was very professional
and assisted the anaesthetist in the room. The
OPD tries to advocate the anaesthetist for the
patient that might be possible for them and
showed the professionalism, although the OPD
can be more assertive in the case (Hussain and
et.al, 2019).
The OPD asked the anaesthetist to if they are
having any difficulty in giving the injection and
then inject the patient correctly in the first
attempt only.
The communication with the patient was very
negative, in whole experience she felt ignored
as well as dismissed that is not appropriate
and acceptable. According to the guidelines of
the HCPC and Association for Perioperative
Practice it is necessary for the professional to
communicate with the patients (Scope,
Referral Guidelines for HCPC registered
Hearing Aid Dispensers, 2017).
The patient also felt that her dignity is
undermined on various occasions that are
against the principles of the HCPC.
The patient was left in pain for a long time
after the surgery with continuous pain, dry
vomiting and sickness. The patient was also
not given the pain meditation on timely
manner and that add on the discomfort of the
patient that is against the care duty for the
patient.
The patient was left without the necessity at
the night time as the patient one asked for
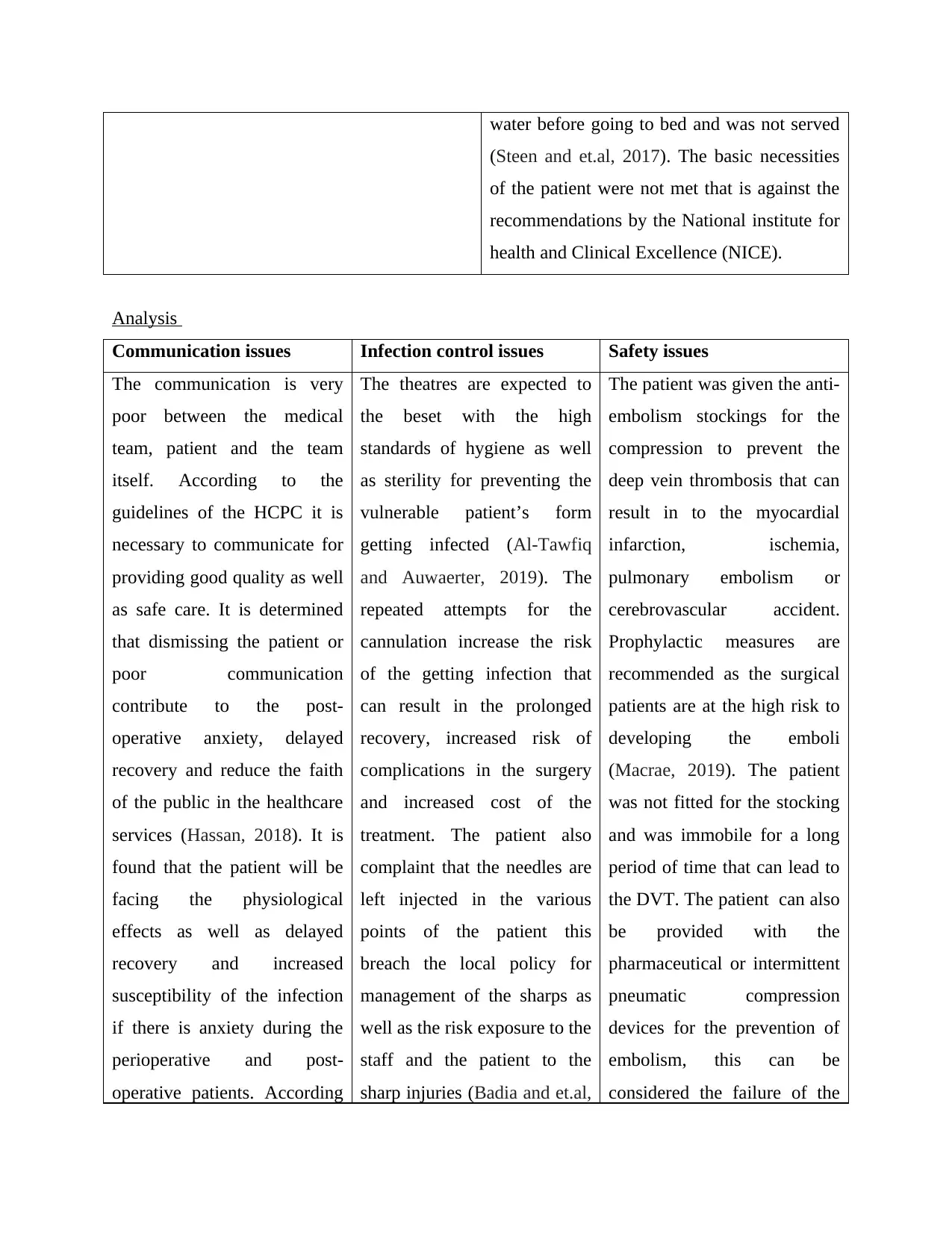
water before going to bed and was not served
(Steen and et.al, 2017). The basic necessities
of the patient were not met that is against the
recommendations by the National institute for
health and Clinical Excellence (NICE).
Analysis
Communication issues Infection control issues Safety issues
The communication is very
poor between the medical
team, patient and the team
itself. According to the
guidelines of the HCPC it is
necessary to communicate for
providing good quality as well
as safe care. It is determined
that dismissing the patient or
poor communication
contribute to the post-
operative anxiety, delayed
recovery and reduce the faith
of the public in the healthcare
services (Hassan, 2018). It is
found that the patient will be
facing the physiological
effects as well as delayed
recovery and increased
susceptibility of the infection
if there is anxiety during the
perioperative and post-
operative patients. According
The theatres are expected to
the beset with the high
standards of hygiene as well
as sterility for preventing the
vulnerable patient’s form
getting infected (Al-Tawfiq
and Auwaerter, 2019). The
repeated attempts for the
cannulation increase the risk
of the getting infection that
can result in the prolonged
recovery, increased risk of
complications in the surgery
and increased cost of the
treatment. The patient also
complaint that the needles are
left injected in the various
points of the patient this
breach the local policy for
management of the sharps as
well as the risk exposure to the
staff and the patient to the
sharp injuries (Badia and et.al,
The patient was given the anti-
embolism stockings for the
compression to prevent the
deep vein thrombosis that can
result in to the myocardial
infarction, ischemia,
pulmonary embolism or
cerebrovascular accident.
Prophylactic measures are
recommended as the surgical
patients are at the high risk to
developing the emboli
(Macrae, 2019). The patient
was not fitted for the stocking
and was immobile for a long
period of time that can lead to
the DVT. The patient can also
be provided with the
pharmaceutical or intermittent
pneumatic compression
devices for the prevention of
embolism, this can be
considered the failure of the
(Steen and et.al, 2017). The basic necessities
of the patient were not met that is against the
recommendations by the National institute for
health and Clinical Excellence (NICE).
Analysis
Communication issues Infection control issues Safety issues
The communication is very
poor between the medical
team, patient and the team
itself. According to the
guidelines of the HCPC it is
necessary to communicate for
providing good quality as well
as safe care. It is determined
that dismissing the patient or
poor communication
contribute to the post-
operative anxiety, delayed
recovery and reduce the faith
of the public in the healthcare
services (Hassan, 2018). It is
found that the patient will be
facing the physiological
effects as well as delayed
recovery and increased
susceptibility of the infection
if there is anxiety during the
perioperative and post-
operative patients. According
The theatres are expected to
the beset with the high
standards of hygiene as well
as sterility for preventing the
vulnerable patient’s form
getting infected (Al-Tawfiq
and Auwaerter, 2019). The
repeated attempts for the
cannulation increase the risk
of the getting infection that
can result in the prolonged
recovery, increased risk of
complications in the surgery
and increased cost of the
treatment. The patient also
complaint that the needles are
left injected in the various
points of the patient this
breach the local policy for
management of the sharps as
well as the risk exposure to the
staff and the patient to the
sharp injuries (Badia and et.al,
The patient was given the anti-
embolism stockings for the
compression to prevent the
deep vein thrombosis that can
result in to the myocardial
infarction, ischemia,
pulmonary embolism or
cerebrovascular accident.
Prophylactic measures are
recommended as the surgical
patients are at the high risk to
developing the emboli
(Macrae, 2019). The patient
was not fitted for the stocking
and was immobile for a long
period of time that can lead to
the DVT. The patient can also
be provided with the
pharmaceutical or intermittent
pneumatic compression
devices for the prevention of
embolism, this can be
considered the failure of the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
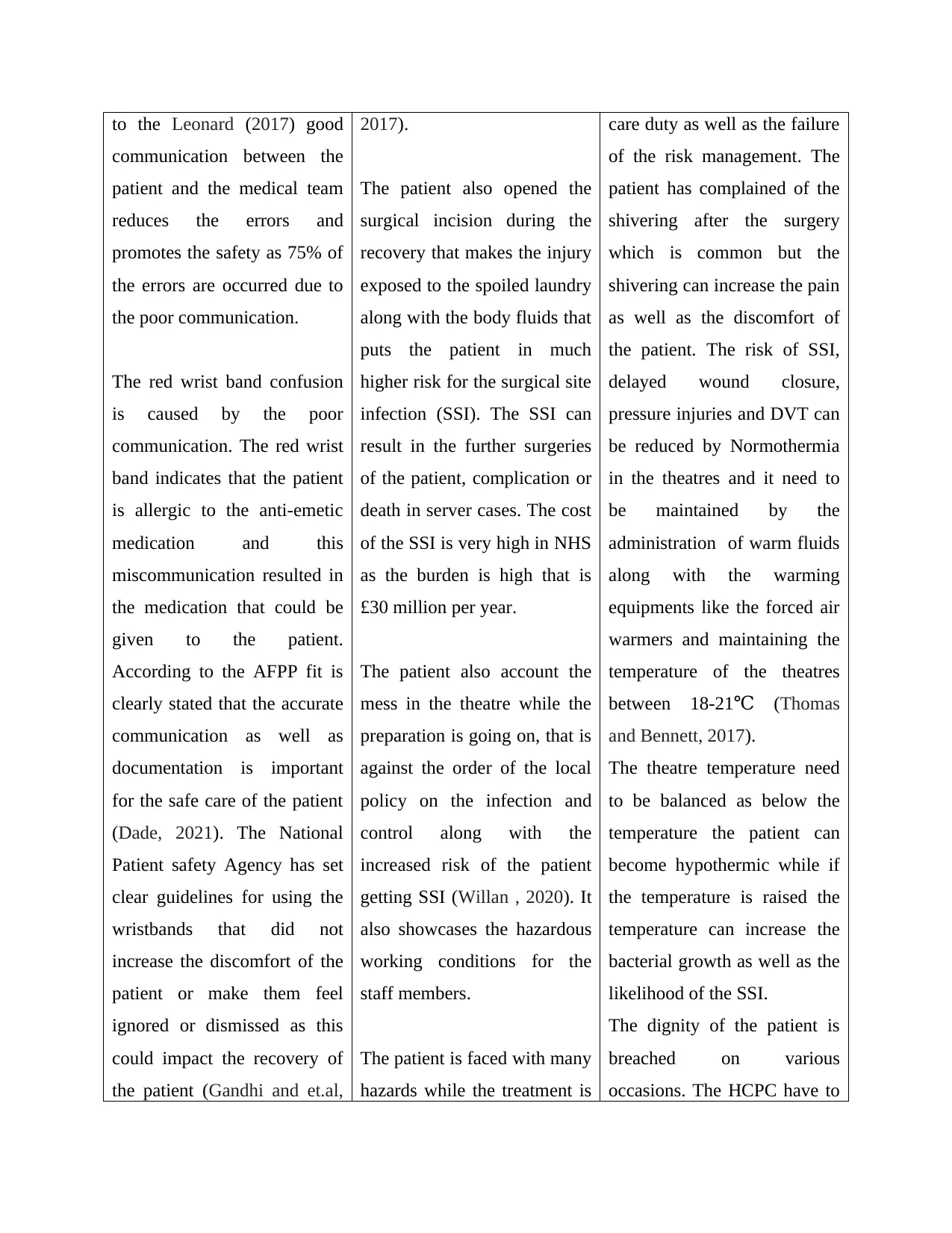
to the Leonard (2017) good
communication between the
patient and the medical team
reduces the errors and
promotes the safety as 75% of
the errors are occurred due to
the poor communication.
The red wrist band confusion
is caused by the poor
communication. The red wrist
band indicates that the patient
is allergic to the anti-emetic
medication and this
miscommunication resulted in
the medication that could be
given to the patient.
According to the AFPP fit is
clearly stated that the accurate
communication as well as
documentation is important
for the safe care of the patient
(Dade, 2021). The National
Patient safety Agency has set
clear guidelines for using the
wristbands that did not
increase the discomfort of the
patient or make them feel
ignored or dismissed as this
could impact the recovery of
the patient (Gandhi and et.al,
2017).
The patient also opened the
surgical incision during the
recovery that makes the injury
exposed to the spoiled laundry
along with the body fluids that
puts the patient in much
higher risk for the surgical site
infection (SSI). The SSI can
result in the further surgeries
of the patient, complication or
death in server cases. The cost
of the SSI is very high in NHS
as the burden is high that is
£30 million per year.
The patient also account the
mess in the theatre while the
preparation is going on, that is
against the order of the local
policy on the infection and
control along with the
increased risk of the patient
getting SSI (Willan , 2020). It
also showcases the hazardous
working conditions for the
staff members.
The patient is faced with many
hazards while the treatment is
care duty as well as the failure
of the risk management. The
patient has complained of the
shivering after the surgery
which is common but the
shivering can increase the pain
as well as the discomfort of
the patient. The risk of SSI,
delayed wound closure,
pressure injuries and DVT can
be reduced by Normothermia
in the theatres and it need to
be maintained by the
administration of warm fluids
along with the warming
equipments like the forced air
warmers and maintaining the
temperature of the theatres
between 18-21 (℃ Thomas
and Bennett, 2017).
The theatre temperature need
to be balanced as below the
temperature the patient can
become hypothermic while if
the temperature is raised the
temperature can increase the
bacterial growth as well as the
likelihood of the SSI.
The dignity of the patient is
breached on various
occasions. The HCPC have to
communication between the
patient and the medical team
reduces the errors and
promotes the safety as 75% of
the errors are occurred due to
the poor communication.
The red wrist band confusion
is caused by the poor
communication. The red wrist
band indicates that the patient
is allergic to the anti-emetic
medication and this
miscommunication resulted in
the medication that could be
given to the patient.
According to the AFPP fit is
clearly stated that the accurate
communication as well as
documentation is important
for the safe care of the patient
(Dade, 2021). The National
Patient safety Agency has set
clear guidelines for using the
wristbands that did not
increase the discomfort of the
patient or make them feel
ignored or dismissed as this
could impact the recovery of
the patient (Gandhi and et.al,
2017).
The patient also opened the
surgical incision during the
recovery that makes the injury
exposed to the spoiled laundry
along with the body fluids that
puts the patient in much
higher risk for the surgical site
infection (SSI). The SSI can
result in the further surgeries
of the patient, complication or
death in server cases. The cost
of the SSI is very high in NHS
as the burden is high that is
£30 million per year.
The patient also account the
mess in the theatre while the
preparation is going on, that is
against the order of the local
policy on the infection and
control along with the
increased risk of the patient
getting SSI (Willan , 2020). It
also showcases the hazardous
working conditions for the
staff members.
The patient is faced with many
hazards while the treatment is
care duty as well as the failure
of the risk management. The
patient has complained of the
shivering after the surgery
which is common but the
shivering can increase the pain
as well as the discomfort of
the patient. The risk of SSI,
delayed wound closure,
pressure injuries and DVT can
be reduced by Normothermia
in the theatres and it need to
be maintained by the
administration of warm fluids
along with the warming
equipments like the forced air
warmers and maintaining the
temperature of the theatres
between 18-21 (℃ Thomas
and Bennett, 2017).
The theatre temperature need
to be balanced as below the
temperature the patient can
become hypothermic while if
the temperature is raised the
temperature can increase the
bacterial growth as well as the
likelihood of the SSI.
The dignity of the patient is
breached on various
occasions. The HCPC have to
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
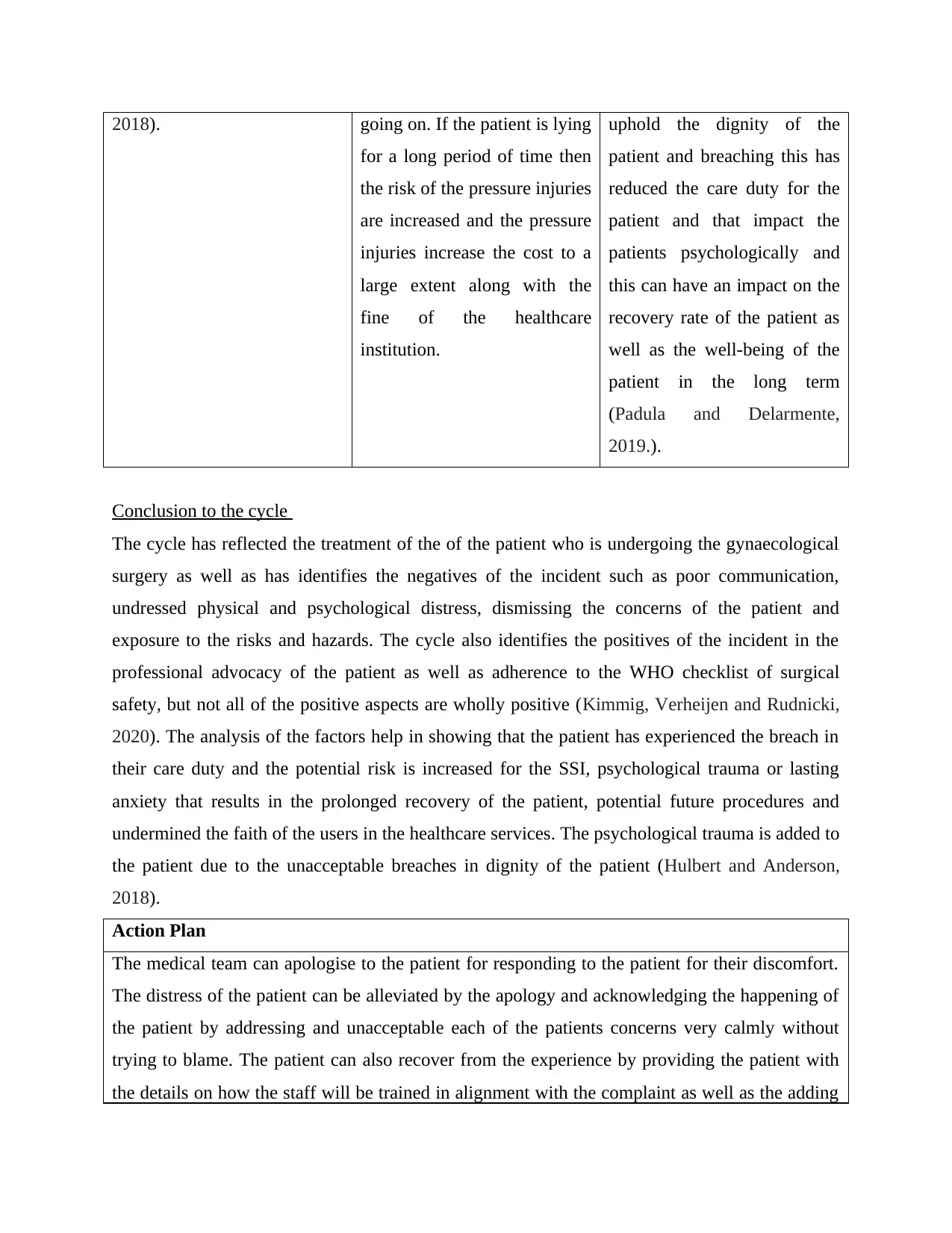
2018). going on. If the patient is lying
for a long period of time then
the risk of the pressure injuries
are increased and the pressure
injuries increase the cost to a
large extent along with the
fine of the healthcare
institution.
uphold the dignity of the
patient and breaching this has
reduced the care duty for the
patient and that impact the
patients psychologically and
this can have an impact on the
recovery rate of the patient as
well as the well-being of the
patient in the long term
(Padula and Delarmente,
2019.).
Conclusion to the cycle
The cycle has reflected the treatment of the of the patient who is undergoing the gynaecological
surgery as well as has identifies the negatives of the incident such as poor communication,
undressed physical and psychological distress, dismissing the concerns of the patient and
exposure to the risks and hazards. The cycle also identifies the positives of the incident in the
professional advocacy of the patient as well as adherence to the WHO checklist of surgical
safety, but not all of the positive aspects are wholly positive (Kimmig, Verheijen and Rudnicki,
2020). The analysis of the factors help in showing that the patient has experienced the breach in
their care duty and the potential risk is increased for the SSI, psychological trauma or lasting
anxiety that results in the prolonged recovery of the patient, potential future procedures and
undermined the faith of the users in the healthcare services. The psychological trauma is added to
the patient due to the unacceptable breaches in dignity of the patient (Hulbert and Anderson,
2018).
Action Plan
The medical team can apologise to the patient for responding to the patient for their discomfort.
The distress of the patient can be alleviated by the apology and acknowledging the happening of
the patient by addressing and unacceptable each of the patients concerns very calmly without
trying to blame. The patient can also recover from the experience by providing the patient with
the details on how the staff will be trained in alignment with the complaint as well as the adding
for a long period of time then
the risk of the pressure injuries
are increased and the pressure
injuries increase the cost to a
large extent along with the
fine of the healthcare
institution.
uphold the dignity of the
patient and breaching this has
reduced the care duty for the
patient and that impact the
patients psychologically and
this can have an impact on the
recovery rate of the patient as
well as the well-being of the
patient in the long term
(Padula and Delarmente,
2019.).
Conclusion to the cycle
The cycle has reflected the treatment of the of the patient who is undergoing the gynaecological
surgery as well as has identifies the negatives of the incident such as poor communication,
undressed physical and psychological distress, dismissing the concerns of the patient and
exposure to the risks and hazards. The cycle also identifies the positives of the incident in the
professional advocacy of the patient as well as adherence to the WHO checklist of surgical
safety, but not all of the positive aspects are wholly positive (Kimmig, Verheijen and Rudnicki,
2020). The analysis of the factors help in showing that the patient has experienced the breach in
their care duty and the potential risk is increased for the SSI, psychological trauma or lasting
anxiety that results in the prolonged recovery of the patient, potential future procedures and
undermined the faith of the users in the healthcare services. The psychological trauma is added to
the patient due to the unacceptable breaches in dignity of the patient (Hulbert and Anderson,
2018).
Action Plan
The medical team can apologise to the patient for responding to the patient for their discomfort.
The distress of the patient can be alleviated by the apology and acknowledging the happening of
the patient by addressing and unacceptable each of the patients concerns very calmly without
trying to blame. The patient can also recover from the experience by providing the patient with
the details on how the staff will be trained in alignment with the complaint as well as the adding

of the new procedures that needs to be put in place for the prevention of the incidents happening
again.
The students that are experience the care pathway that are similar to this incident can advocate
and assertive for the patient throughout and will be making efforts for the communicating with
the patient in the theatre environment as well as provide reassurance for the patient (Norrving
and et.al, 2018). The student will also ensure that the explain the patient that sometime due to
certain conditions the patient will feel the like vomiting, nausea and shivering , that is very
difficult to control. The student can also find a more experienced practitioner for explaining the
patient and reassuring. The patients can be provided with the warm blankets or changing the
soiled sheets for more comfort. The student can be anxious as being a naïve practitioner this can
be challenging for the assertiveness level but the student knows that it is important for the
professional acknowledgement and development and the native practitioner can also be more
conscientious as well as less complacent than the experienced practitioner.
Overall summary
The reflection has shown to the students that looking back to the negatives of the incident can
help the student in learning from the mistakes that are previously made and find ways for
improving the practices that are in accordance with the HCPC (Courtier and et.al, 2021). The
student is able to learn new theory for applying it into the future practice along with that the
information is gained that the 75% of the incident are caused by the error in the communication
or poor communication. The student gets to know that the patient has suffered from distress due
to the breaches in the duty of the care of the patients by the medical team and this help the
student in being more aware about the need to advocate, uphold the professional standards and
assertive in the future for preventing such incidents from happening.
again.
The students that are experience the care pathway that are similar to this incident can advocate
and assertive for the patient throughout and will be making efforts for the communicating with
the patient in the theatre environment as well as provide reassurance for the patient (Norrving
and et.al, 2018). The student will also ensure that the explain the patient that sometime due to
certain conditions the patient will feel the like vomiting, nausea and shivering , that is very
difficult to control. The student can also find a more experienced practitioner for explaining the
patient and reassuring. The patients can be provided with the warm blankets or changing the
soiled sheets for more comfort. The student can be anxious as being a naïve practitioner this can
be challenging for the assertiveness level but the student knows that it is important for the
professional acknowledgement and development and the native practitioner can also be more
conscientious as well as less complacent than the experienced practitioner.
Overall summary
The reflection has shown to the students that looking back to the negatives of the incident can
help the student in learning from the mistakes that are previously made and find ways for
improving the practices that are in accordance with the HCPC (Courtier and et.al, 2021). The
student is able to learn new theory for applying it into the future practice along with that the
information is gained that the 75% of the incident are caused by the error in the communication
or poor communication. The student gets to know that the patient has suffered from distress due
to the breaches in the duty of the care of the patients by the medical team and this help the
student in being more aware about the need to advocate, uphold the professional standards and
assertive in the future for preventing such incidents from happening.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
REFRENCES
Books and Journals
Adeani, Febriani and Syafryadin, 2020. USING GIBBS’REFLECTIVE CYCLE IN MAKING
REFLECTIONS OF LITERARY ANALYSIS. Indonesian EFL Journal. 6(2). pp.139-
148.
Ahmed, 2019. Students’ reflective journaling: an impactful strategy that informs instructional
practices in an EFL writing university context in Qatar. Reflective Practice. 20(4).
pp.483-500.
Al-Tawfiq and Auwaerter, 2019. Healthcare-associated infections: the hallmark of Middle East
respiratory syndrome coronavirus with review of the literature. Journal of Hospital
Infection. 101(1). pp.20-29.
Badia and et.al, 2017. Impact of surgical site infection on healthcare costs and patient outcomes:
a systematic review in six European countries. Journal of Hospital Infection. 96(1). pp.1-
15.
Courtier and et.al, 2021. Expectations of therapeutic radiography students in Wales about
transitioning to practice during the Covid-19 pandemic as registrants on the HCPC temporary
register. Radiography. 27(2). pp.316-321.
Dade, 2021. Can you name one person who was responsible for your introduction to healthcare
as a career?.
Fergusson, van der Laan and Baker, 2019. Reflective practice and work-based research: a
description of micro-and macro-reflective cycles. Reflective Practice. 20(2). pp.289-303.
Gandhi and et.al, 2018. Transforming concepts in patient safety: a progress report. BMJ Quality
& Safety. 27(12). pp.1019-1026.
good communication
guidelines of the HCPC
Hassan, 2018. Avoiding medication errors through effective communication in healthcare
environment. Movement, Health & Exercise. 7(1). pp.113-126.
Hulbert and Anderson, 2018. What doesn’t kill you makes you stronger: Psychological trauma
and its relationship to enhanced memory control. Journal of Experimental Psychology:
General. 147(12). p.1931.
Books and Journals
Adeani, Febriani and Syafryadin, 2020. USING GIBBS’REFLECTIVE CYCLE IN MAKING
REFLECTIONS OF LITERARY ANALYSIS. Indonesian EFL Journal. 6(2). pp.139-
148.
Ahmed, 2019. Students’ reflective journaling: an impactful strategy that informs instructional
practices in an EFL writing university context in Qatar. Reflective Practice. 20(4).
pp.483-500.
Al-Tawfiq and Auwaerter, 2019. Healthcare-associated infections: the hallmark of Middle East
respiratory syndrome coronavirus with review of the literature. Journal of Hospital
Infection. 101(1). pp.20-29.
Badia and et.al, 2017. Impact of surgical site infection on healthcare costs and patient outcomes:
a systematic review in six European countries. Journal of Hospital Infection. 96(1). pp.1-
15.
Courtier and et.al, 2021. Expectations of therapeutic radiography students in Wales about
transitioning to practice during the Covid-19 pandemic as registrants on the HCPC temporary
register. Radiography. 27(2). pp.316-321.
Dade, 2021. Can you name one person who was responsible for your introduction to healthcare
as a career?.
Fergusson, van der Laan and Baker, 2019. Reflective practice and work-based research: a
description of micro-and macro-reflective cycles. Reflective Practice. 20(2). pp.289-303.
Gandhi and et.al, 2018. Transforming concepts in patient safety: a progress report. BMJ Quality
& Safety. 27(12). pp.1019-1026.
good communication
guidelines of the HCPC
Hassan, 2018. Avoiding medication errors through effective communication in healthcare
environment. Movement, Health & Exercise. 7(1). pp.113-126.
Hulbert and Anderson, 2018. What doesn’t kill you makes you stronger: Psychological trauma
and its relationship to enhanced memory control. Journal of Experimental Psychology:
General. 147(12). p.1931.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Hussain and et.al, 2019. Promoting OPD patient satisfaction through different healthcare
determinants: a study of public sector hospitals. International journal of environmental
research and public health. 16(19). p.3719.
Jarvis and Baloyi, 2020. Scaffolding in reflective journaling: A means to develop higher order
thinking skills in undergraduate learners. International Journal of Africa Nursing
Sciences. 12. p.100195.
Kimmig, Verheijen and Rudnicki, 2020. Robot assisted surgery during the COVID-19 pandemic,
especially for gynecological cancer: a statement of the Society of European Robotic
Gynaecological Surgery (SERGS). Journal of gynecologic oncology. 31(3).
Leonard, 2017. Exploring ways to manage healthcare professional—patient communication
issues. Supportive Care in Cancer. 25(1). pp.7-9.
MacCallum and Casey, 2017. Enhancing skills development and reflective practise in students
during their programme of study. New Directions in the Teaching of Physical Sciences,
(12).
Macrae, 2019. Governing the safety of artificial intelligence in healthcare. BMJ quality &
safety. 28(6). pp.495-498.
Markkanen and et.al, 2020. A reflective cycle: Understanding challenging situations in a school
setting. Educational Research. 62(1). pp.46-62.
Norrving and et.al, 2018. Action plan for stroke in Europe 2018–2030. European Stroke
Journal. 3(4). pp.309-336.
Padula and Delarmente, 2019. The national cost of hospital‐acquired pressure injuries in the
United States. International wound journal. 16(3). pp.634-640.
Rivera and et.al, 2020. Development and Utility of the Observational Research in Oncology
Toolbox: Cancer Medications Enquiry Database-Healthcare Common Procedure Coding
System (HCPCS). JNCI Monographs. 2020(55). pp.39-45.
Scope, Referral Guidelines for HCPC registered Hearing Aid Dispensers (Updated September
2017).
Snodgrass and Bush, 2017. Re-operative urethroplasty after failed hypospadias repair: how prior
surgery impacts risk for additional complications. Journal of pediatric urology. 13(3). pp.289-e1.
Steen and et.al, 2017. Retrospective examination of lipid-lowering treatment patterns in a real-
world high-risk cohort in the UK in 2014: comparison with the National Institute for
determinants: a study of public sector hospitals. International journal of environmental
research and public health. 16(19). p.3719.
Jarvis and Baloyi, 2020. Scaffolding in reflective journaling: A means to develop higher order
thinking skills in undergraduate learners. International Journal of Africa Nursing
Sciences. 12. p.100195.
Kimmig, Verheijen and Rudnicki, 2020. Robot assisted surgery during the COVID-19 pandemic,
especially for gynecological cancer: a statement of the Society of European Robotic
Gynaecological Surgery (SERGS). Journal of gynecologic oncology. 31(3).
Leonard, 2017. Exploring ways to manage healthcare professional—patient communication
issues. Supportive Care in Cancer. 25(1). pp.7-9.
MacCallum and Casey, 2017. Enhancing skills development and reflective practise in students
during their programme of study. New Directions in the Teaching of Physical Sciences,
(12).
Macrae, 2019. Governing the safety of artificial intelligence in healthcare. BMJ quality &
safety. 28(6). pp.495-498.
Markkanen and et.al, 2020. A reflective cycle: Understanding challenging situations in a school
setting. Educational Research. 62(1). pp.46-62.
Norrving and et.al, 2018. Action plan for stroke in Europe 2018–2030. European Stroke
Journal. 3(4). pp.309-336.
Padula and Delarmente, 2019. The national cost of hospital‐acquired pressure injuries in the
United States. International wound journal. 16(3). pp.634-640.
Rivera and et.al, 2020. Development and Utility of the Observational Research in Oncology
Toolbox: Cancer Medications Enquiry Database-Healthcare Common Procedure Coding
System (HCPCS). JNCI Monographs. 2020(55). pp.39-45.
Scope, Referral Guidelines for HCPC registered Hearing Aid Dispensers (Updated September
2017).
Snodgrass and Bush, 2017. Re-operative urethroplasty after failed hypospadias repair: how prior
surgery impacts risk for additional complications. Journal of pediatric urology. 13(3). pp.289-e1.
Steen and et.al, 2017. Retrospective examination of lipid-lowering treatment patterns in a real-
world high-risk cohort in the UK in 2014: comparison with the National Institute for
Health and Care Excellence (NICE) 2014 lipid modification guidelines. BMJ open. 7(2).
p.e013255.
Thomas and Bennett, 2017. Introducing a device to assist in the application of anti-embolism
stockings. British Journal of Nursing. 26(9). pp.510-513.
WIDIASTUTI and BUDIYANTO, 2018. Applying an experiential learning cycle with the aid of
finite element analysis in engineering education. Journal of Turkish science
education. 15(Special). pp.97-103.
Willan , 2020. Challenges for NHS hospitals during covid-19 epidemic.
Wu and et.al, 2018. Parameter extraction of photovoltaic models from measured IV
characteristics curves using a hybrid trust-region reflective algorithm. Applied
Energy. 232. pp.36-53.
p.e013255.
Thomas and Bennett, 2017. Introducing a device to assist in the application of anti-embolism
stockings. British Journal of Nursing. 26(9). pp.510-513.
WIDIASTUTI and BUDIYANTO, 2018. Applying an experiential learning cycle with the aid of
finite element analysis in engineering education. Journal of Turkish science
education. 15(Special). pp.97-103.
Willan , 2020. Challenges for NHS hospitals during covid-19 epidemic.
Wu and et.al, 2018. Parameter extraction of photovoltaic models from measured IV
characteristics curves using a hybrid trust-region reflective algorithm. Applied
Energy. 232. pp.36-53.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.