Unit 17: Effective Reporting and Record-keeping in Healthcare
VerifiedAdded on 2022/07/26
|13
|3870
|39
Report
AI Summary
This report delves into the critical aspects of effective reporting and record-keeping within health and social care services. It begins with an introduction that outlines the report's objectives, including an examination of technology's role in recording and reporting, the benefits of service user involvement, and the application of digital technology in medical management procedures and care plans. The report then provides an audit report that details the usage of technology in the reporting and recording of service user care. It explores how technology is utilized in various care settings, emphasizing the shift towards digitized patient records and the advantages of electronic patient records (EPRs). The report highlights the benefits of involving service users in record-keeping processes, emphasizing increased accountability, transparency, and improved quality of care. It also reviews the use of digital technology in medical management procedures and care plans, discussing the implementation of communications and information technology for disease prevention and improving the quality of life. The report evaluates the effectiveness of technology in meeting service user needs, ensuring appropriate care, and maintaining confidentiality. The report also includes a care plan for a 60-year-old patient named Mr. P, who is admitted to the emergency room with a severe headache. The care plan outlines desired outcomes and interventions to manage the patient's symptoms and improve his condition. The report concludes by emphasizing the importance of producing accurate, legible, concise, and coherent records regarding service user care.

Unit17: Effective Reporting and Record- keeping in Health and Social Care Services
Final
Final
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Table of Contents
Introduction......................................................................................................................................2
P6 Describe how technology is used in recording and reporting in own care setting.....................2
P7 Explain the benefits of involving service users in record keeping processes.............................4
M3 Review the use of digital technology in relation to own medical management procedures or
care plan...........................................................................................................................................5
D3 Evaluate the effectiveness of the use of technology in terms of meeting service user needs,
ensuring appropriate care is given and maintaining confidentiality................................................6
P8 Produce accurate, legible, concise and coherent records regarding service user care for
different service users following their own setting’s guidelines.....................................................6
P9 Explain different aspects of own management of service user records with reference to
compliance with national and local policies and guidelines............................................................9
M4 Analyse the process of maintaining records in own setting, identifying any potential or actual
difficulties........................................................................................................................................9
D4 Evaluate the effectiveness of own completion of documentation in terms of meeting service
user needs, ensuring appropriate care is given and effective reporting is carried out...................10
References......................................................................................................................................11
1
Introduction......................................................................................................................................2
P6 Describe how technology is used in recording and reporting in own care setting.....................2
P7 Explain the benefits of involving service users in record keeping processes.............................4
M3 Review the use of digital technology in relation to own medical management procedures or
care plan...........................................................................................................................................5
D3 Evaluate the effectiveness of the use of technology in terms of meeting service user needs,
ensuring appropriate care is given and maintaining confidentiality................................................6
P8 Produce accurate, legible, concise and coherent records regarding service user care for
different service users following their own setting’s guidelines.....................................................6
P9 Explain different aspects of own management of service user records with reference to
compliance with national and local policies and guidelines............................................................9
M4 Analyse the process of maintaining records in own setting, identifying any potential or actual
difficulties........................................................................................................................................9
D4 Evaluate the effectiveness of own completion of documentation in terms of meeting service
user needs, ensuring appropriate care is given and effective reporting is carried out...................10
References......................................................................................................................................11
1
Introduction
This audit report will provide the review of the usage of technology within the reporting and
recording of the service user care along with the establishment of the ways to keep as well as
maintain the records of the service users adhering to the legal framework of health and social
care. This report will also include the benefits of the involvement of service users within the
process of record keeping. It will also include a discussion regarding the use of digital
technology within the medical management procedures or care plans along with the relevant
difficulties and benefits. This will be followed by the evaluation of the technology within
meeting the needs of the service users while ensuring that adequate care has been provided along
with the maintenance of confidentiality.
Audit Report
An audit report is referred to as the written letter from the auditor comprising of their opinion
regarding whether the financial statements of the organisation adhere to the generally accepted
accounting principles (GAAP) and are free from material misstatement.
P6 Describe how technology is used in recording and reporting in own care setting
The records of the patients have rapidly turned out to be digitized. Electronic Patient Records
(ERPs) allow real-time sharing in and throughout the boundary of care. The digital interventions
in the ERP, for instance, Computerised Physician Order Entry (CPOE) or electronic prescribing
(prescribing) can minimise the risk of error (Solomon and Rudin, 2020). The delivery of care to
the patient is reliant on efficient communication between the staff and patients and the healthcare
staff. The digital environment has now been providing new as well as exciting ways for
increasing the processes. The norm in modern healthcare is multidisciplinary working which
means that the accessibility and contribution towards the ERP are related to all of the individuals.
The increased usage of digital records means that huge volumes of digital data are being
produced which can be utilised for encouraging the improvement in quality within healthcare
(Gianfrancesco, Tamang, Yazdany and Schmajuk, 2018).
2
This audit report will provide the review of the usage of technology within the reporting and
recording of the service user care along with the establishment of the ways to keep as well as
maintain the records of the service users adhering to the legal framework of health and social
care. This report will also include the benefits of the involvement of service users within the
process of record keeping. It will also include a discussion regarding the use of digital
technology within the medical management procedures or care plans along with the relevant
difficulties and benefits. This will be followed by the evaluation of the technology within
meeting the needs of the service users while ensuring that adequate care has been provided along
with the maintenance of confidentiality.
Audit Report
An audit report is referred to as the written letter from the auditor comprising of their opinion
regarding whether the financial statements of the organisation adhere to the generally accepted
accounting principles (GAAP) and are free from material misstatement.
P6 Describe how technology is used in recording and reporting in own care setting
The records of the patients have rapidly turned out to be digitized. Electronic Patient Records
(ERPs) allow real-time sharing in and throughout the boundary of care. The digital interventions
in the ERP, for instance, Computerised Physician Order Entry (CPOE) or electronic prescribing
(prescribing) can minimise the risk of error (Solomon and Rudin, 2020). The delivery of care to
the patient is reliant on efficient communication between the staff and patients and the healthcare
staff. The digital environment has now been providing new as well as exciting ways for
increasing the processes. The norm in modern healthcare is multidisciplinary working which
means that the accessibility and contribution towards the ERP are related to all of the individuals.
The increased usage of digital records means that huge volumes of digital data are being
produced which can be utilised for encouraging the improvement in quality within healthcare
(Gianfrancesco, Tamang, Yazdany and Schmajuk, 2018).
2
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
Smartphones can be used to communicate medication adherence education; information related
to behaviour change and follow up treatment protocol to the providers and members through
managed care plans. Making records at the point of care with the tablets decreases the time
which is spent on documentation. Along with this, the usage of tablets assists in the avoidance of
burdensome and error-prone entry of human data. They provide assistance with the elimination
of human-introduced errors for instance within the data entry through the input in the data from
patient care systems (Gianfrancesco, Tamang, Yazdany and Schmajuk, 2018). By eliminating the
requirement of recording information on paper, tablets have saved money, energy, time along
with making improvements within the efficiency.
The use of tablets has also allowed quick access to information whenever it is required by
healthcare professionals. Tablets have also assisted in the reduction of messy paperwork as well
as the manual workflow processes in turn leading to increased efficiencies. The multimedia,
visual and graphics abilities can be leveraged for recording as well as providing on-demand
information, for instance, the progression of the disease, visual images of the patients as well as
sounds, for example, irregular heartbeat (Solomon and Rudin, 2020).
Technology supported consulting is considered by various individuals as the partial solution
towards the complex challenges of delivering healthcare to eth increasingly diverse and ageing
population. Remote consultations provide prospective advantages to the patients and healthcare
system. Virtual clinics through Skype have been utilised for counselling and mental health
consultations. Skype has proved to be an efficient medium for providing support to the
independence and self-confidence of young individuals. Virtual clinics are responsible for
bringing specialist care to patients’ homes (Greenhalgh et al., 2016).
It is an ideal solution for allowing the patients to have access to specialist care; however, without
unreasonably exposing themselves to the high-risk environment. These clinics also minimise the
need for travelling to or from the hospitals which is also a considerable benefit as about 20 per
cent of the traffic within the UK is attributed to travel related to healthcare. Furthermore, virtual
clinics mean that less time is missed from the work which can be a recurrent challenge for the
individuals; hence, this minimisation within treatment burden is highly advantageous (Quinn,
Davies and Hadjiconstantinou, 2020).
3
to behaviour change and follow up treatment protocol to the providers and members through
managed care plans. Making records at the point of care with the tablets decreases the time
which is spent on documentation. Along with this, the usage of tablets assists in the avoidance of
burdensome and error-prone entry of human data. They provide assistance with the elimination
of human-introduced errors for instance within the data entry through the input in the data from
patient care systems (Gianfrancesco, Tamang, Yazdany and Schmajuk, 2018). By eliminating the
requirement of recording information on paper, tablets have saved money, energy, time along
with making improvements within the efficiency.
The use of tablets has also allowed quick access to information whenever it is required by
healthcare professionals. Tablets have also assisted in the reduction of messy paperwork as well
as the manual workflow processes in turn leading to increased efficiencies. The multimedia,
visual and graphics abilities can be leveraged for recording as well as providing on-demand
information, for instance, the progression of the disease, visual images of the patients as well as
sounds, for example, irregular heartbeat (Solomon and Rudin, 2020).
Technology supported consulting is considered by various individuals as the partial solution
towards the complex challenges of delivering healthcare to eth increasingly diverse and ageing
population. Remote consultations provide prospective advantages to the patients and healthcare
system. Virtual clinics through Skype have been utilised for counselling and mental health
consultations. Skype has proved to be an efficient medium for providing support to the
independence and self-confidence of young individuals. Virtual clinics are responsible for
bringing specialist care to patients’ homes (Greenhalgh et al., 2016).
It is an ideal solution for allowing the patients to have access to specialist care; however, without
unreasonably exposing themselves to the high-risk environment. These clinics also minimise the
need for travelling to or from the hospitals which is also a considerable benefit as about 20 per
cent of the traffic within the UK is attributed to travel related to healthcare. Furthermore, virtual
clinics mean that less time is missed from the work which can be a recurrent challenge for the
individuals; hence, this minimisation within treatment burden is highly advantageous (Quinn,
Davies and Hadjiconstantinou, 2020).
3
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
P7 Explain the benefits of involving service users in record keeping processes
The involvement of the service users within the processes of record-keeping transfers the power
from the policymakers and healthcare professionals to the public. The involvement of the service
users allows public accountability, participatory democracy as well as transparency. Servicer
users’ involvement recognises the capacity of the individuals with regards to self-determination,
offering them a voice within the process of keeping their records. The individuals have been
provided with the duty and right for participating collectively and individually within the
planning as well as the implementation of the healthcare. The involvement of the users within the
record-keeping processes enhances their commitment to having an understanding and looking for
the impactful issues affecting them (Letellier and Eppich, 2015).
The involvement of the service users can make improvements within the quality of record-
keeping activities. For instance, the patients having long term illnesses frequently have
perceptions regarding their care which might be lacked by the policymakers and the healthcare
providers. The carers and users might not have similar conflicts of interest as the policymakers
and medical professionals. It also provides assistance in the development of partnerships
between technical experts and the public. The involvement of the service users possibly results in
more acceptable and accessible health services, health research of clinical relevance and greater
research as well as increased acceptance of findings (Lacity and Willcocks, 2016).
The care service is lawfully needed to maintain the needs assessment, care plans, case reviews
and incident records, risk assessment and for keeping some confidential notes as well as records
regarding the individual service users as the significant component of daily functioning. The
complaints and tensions regarding the accessibility to the records and information can be
minimised in case the healthcare service has facilitated the atmosphere of respect and openness
within which the service users, staff, family and friends, all get a sense of being valued and that
their rights and perspectives are significant (Letellier and Eppich, 2015). This can also be carried
out with regards to record-keeping through encouraging the healthcare staff for involving the
service users while writing the records. This provides assistance within involving the individuals
more completely within their own care and the aim of the record can be understood and
explained (Lacity and Willcocks, 2016).
4
The involvement of the service users within the processes of record-keeping transfers the power
from the policymakers and healthcare professionals to the public. The involvement of the service
users allows public accountability, participatory democracy as well as transparency. Servicer
users’ involvement recognises the capacity of the individuals with regards to self-determination,
offering them a voice within the process of keeping their records. The individuals have been
provided with the duty and right for participating collectively and individually within the
planning as well as the implementation of the healthcare. The involvement of the users within the
record-keeping processes enhances their commitment to having an understanding and looking for
the impactful issues affecting them (Letellier and Eppich, 2015).
The involvement of the service users can make improvements within the quality of record-
keeping activities. For instance, the patients having long term illnesses frequently have
perceptions regarding their care which might be lacked by the policymakers and the healthcare
providers. The carers and users might not have similar conflicts of interest as the policymakers
and medical professionals. It also provides assistance in the development of partnerships
between technical experts and the public. The involvement of the service users possibly results in
more acceptable and accessible health services, health research of clinical relevance and greater
research as well as increased acceptance of findings (Lacity and Willcocks, 2016).
The care service is lawfully needed to maintain the needs assessment, care plans, case reviews
and incident records, risk assessment and for keeping some confidential notes as well as records
regarding the individual service users as the significant component of daily functioning. The
complaints and tensions regarding the accessibility to the records and information can be
minimised in case the healthcare service has facilitated the atmosphere of respect and openness
within which the service users, staff, family and friends, all get a sense of being valued and that
their rights and perspectives are significant (Letellier and Eppich, 2015). This can also be carried
out with regards to record-keeping through encouraging the healthcare staff for involving the
service users while writing the records. This provides assistance within involving the individuals
more completely within their own care and the aim of the record can be understood and
explained (Lacity and Willcocks, 2016).
4
At present, the minority of the service users have been involved within the process of risk
assessment in an active manner. The approaches related to recovery focus that the management
of risk must be developed on the identification of the strengths of the service users and must
focus recovery and there is an increased probability that it will be attained by making use of the
collaborative approach (Luchenski et al., 2018).
The involvement within the risk assessment is more probable to develop the conditions where the
service users can build the trusting therapeutic rapports with their treating teams and hold change
for lowering their risk. Thus, it is significantly important with regards to the forensic mental
health service, the level of risks of service users and the overall recovery of the service users for
learning the ways for enhancing the involvement of the service users within the process of risk
assessment (Bombard et al., 2018).
M3 Review the use of digital technology in relation to own medical management
procedures or care plan
The implementation of communications and information technology for the provision of digital
health interventions for the prevention of disease as well as improving the quality of life is not a
new idea. The internet of medical things (IoMT) is the combination of medical devices and
applications linking to the health IT systems which make use of networking technologies. IoT
makes use of cases ranging from telemedicine technology for improving the communication
between the doctors and patients, for minimising the potential for exposure to contagious
diseases and to numerous smart sensor technologies which can collect the data at the level of
users (Ting, Carin, Dzau and Wong, 2020).
Blockchain-based EMRs are intended towards the minimisation of time required for accessing
the information of the patients while making improvements within the quality of the data and
interoperability. The benefits of the blockchain include data scalability, privacy and accessibility
to security (Daraghmi, Daraghmi and Yuan, 2019). Virtual care provides various benefits
extending to all of the members involving the patients enjoying increased access, convenience as
well as lower cost; caregivers, doctors and nurses experiencing improved access and more
flexible schedules to the patients and information and healthcare administrators and leaders
5
assessment in an active manner. The approaches related to recovery focus that the management
of risk must be developed on the identification of the strengths of the service users and must
focus recovery and there is an increased probability that it will be attained by making use of the
collaborative approach (Luchenski et al., 2018).
The involvement within the risk assessment is more probable to develop the conditions where the
service users can build the trusting therapeutic rapports with their treating teams and hold change
for lowering their risk. Thus, it is significantly important with regards to the forensic mental
health service, the level of risks of service users and the overall recovery of the service users for
learning the ways for enhancing the involvement of the service users within the process of risk
assessment (Bombard et al., 2018).
M3 Review the use of digital technology in relation to own medical management
procedures or care plan
The implementation of communications and information technology for the provision of digital
health interventions for the prevention of disease as well as improving the quality of life is not a
new idea. The internet of medical things (IoMT) is the combination of medical devices and
applications linking to the health IT systems which make use of networking technologies. IoT
makes use of cases ranging from telemedicine technology for improving the communication
between the doctors and patients, for minimising the potential for exposure to contagious
diseases and to numerous smart sensor technologies which can collect the data at the level of
users (Ting, Carin, Dzau and Wong, 2020).
Blockchain-based EMRs are intended towards the minimisation of time required for accessing
the information of the patients while making improvements within the quality of the data and
interoperability. The benefits of the blockchain include data scalability, privacy and accessibility
to security (Daraghmi, Daraghmi and Yuan, 2019). Virtual care provides various benefits
extending to all of the members involving the patients enjoying increased access, convenience as
well as lower cost; caregivers, doctors and nurses experiencing improved access and more
flexible schedules to the patients and information and healthcare administrators and leaders
5
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
reducing medical expenses and increasing operational efficiency. Virtual care offers a brief and
effective way to address the questions of the individuals and deliver the care. This efficiency can
make a contribution towards easing the workloads as well as minimising the stress. The doctors
can also consult one another more readily making use of the virtual care technology. Along with
the provision of assistance in lowering the costs, the minimisation of unnecessary referrals can
give the healthcare organisation the increased capacity for the provision of appropriate and
complex speciality care (Heyworth et al., 2020).
D3 Evaluate the effectiveness of the use of technology in terms of meeting service user
needs, ensuring appropriate care is given and maintaining confidentiality
Digital health tools have been empowering the patients for taking a more active role in
monitoring their own health. However, the huge challenges for these tools are the attainment of
validation for making sure that the anticipated usage of the device and safe management of the
data. Moreover, the manufacturers are required to prioritise the safety of the patients. The data is
required to be integrated with the medical history of the patient in an adequate manner for the
prevention of the misinterpretation of the information. The privacy of the data is also the area of
emphasis where the manufacturers are required to develop confidence among the users related to
the safety of the data of the patients (Solomon and Rudin, 2020).
P8 Produce accurate, legible, concise and coherent records regarding service user care for
different service users following their own setting’s guidelines
Care Plan
Mr P is 60 years old and has come to emergency with the complaint of severe headache mainly
upon awakening. He has also reported changes in appetite along with dizziness, vomiting and
nausea. The following is the care plan developed for him:
Desired Outcome
Mr P states that he is not suffering from headaches and looks pain-free and comfortable.
Interventions
Identifying particulars of pain, for instance, the intensity, location of pain and how long it has
been going.
Noting the attitude of the patient towards pain along with any history of substance abuse
6
effective way to address the questions of the individuals and deliver the care. This efficiency can
make a contribution towards easing the workloads as well as minimising the stress. The doctors
can also consult one another more readily making use of the virtual care technology. Along with
the provision of assistance in lowering the costs, the minimisation of unnecessary referrals can
give the healthcare organisation the increased capacity for the provision of appropriate and
complex speciality care (Heyworth et al., 2020).
D3 Evaluate the effectiveness of the use of technology in terms of meeting service user
needs, ensuring appropriate care is given and maintaining confidentiality
Digital health tools have been empowering the patients for taking a more active role in
monitoring their own health. However, the huge challenges for these tools are the attainment of
validation for making sure that the anticipated usage of the device and safe management of the
data. Moreover, the manufacturers are required to prioritise the safety of the patients. The data is
required to be integrated with the medical history of the patient in an adequate manner for the
prevention of the misinterpretation of the information. The privacy of the data is also the area of
emphasis where the manufacturers are required to develop confidence among the users related to
the safety of the data of the patients (Solomon and Rudin, 2020).
P8 Produce accurate, legible, concise and coherent records regarding service user care for
different service users following their own setting’s guidelines
Care Plan
Mr P is 60 years old and has come to emergency with the complaint of severe headache mainly
upon awakening. He has also reported changes in appetite along with dizziness, vomiting and
nausea. The following is the care plan developed for him:
Desired Outcome
Mr P states that he is not suffering from headaches and looks pain-free and comfortable.
Interventions
Identifying particulars of pain, for instance, the intensity, location of pain and how long it has
been going.
Noting the attitude of the patient towards pain along with any history of substance abuse
6
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
Limiting the movement of the patient
Encouraging rest during severe episodes of pain
Recommending method of relief, for instance, back and neck rub application of cool cloths to the
forehead and avoiding the bright lights.
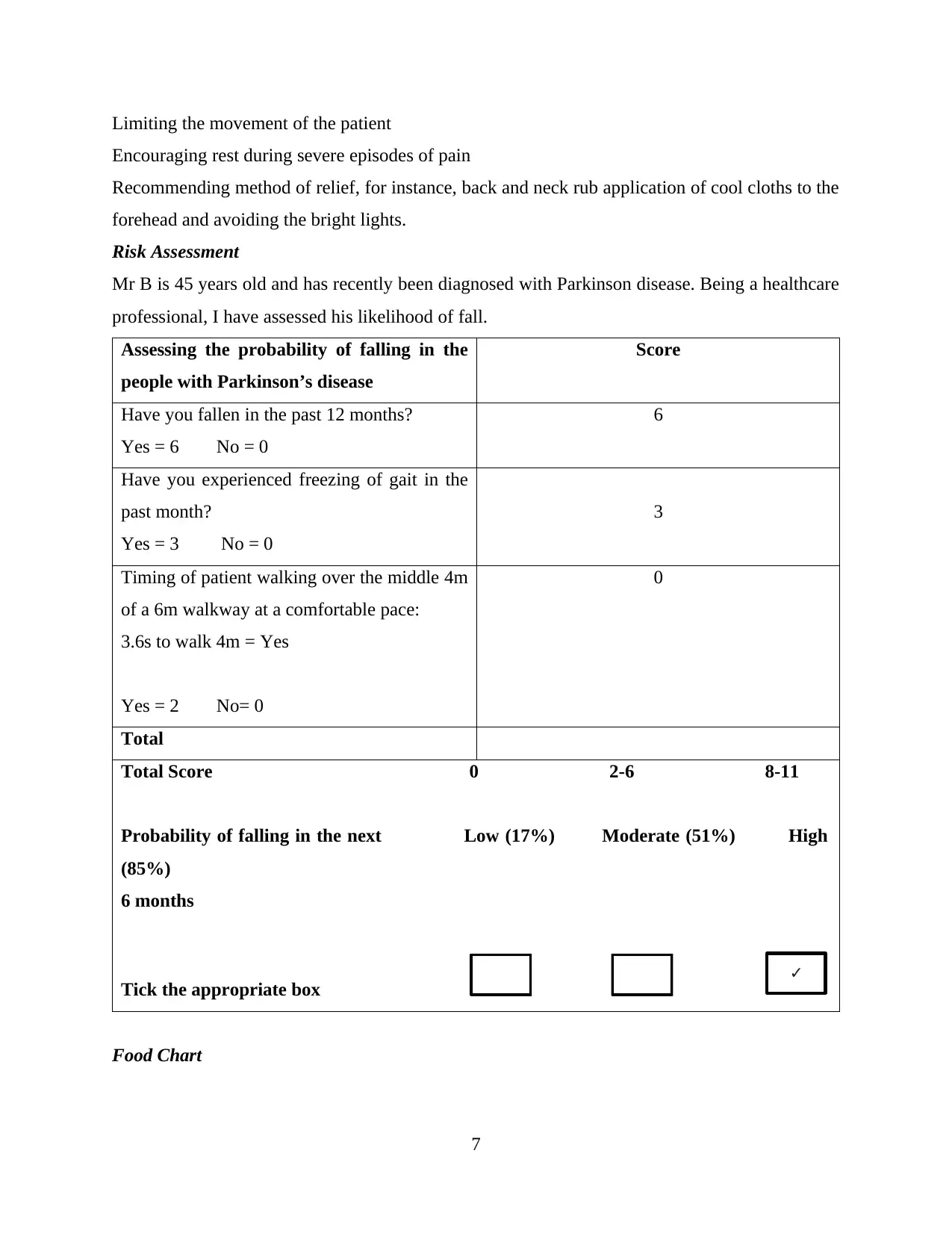
Risk Assessment
Mr B is 45 years old and has recently been diagnosed with Parkinson disease. Being a healthcare
professional, I have assessed his likelihood of fall.
Assessing the probability of falling in the
people with Parkinson’s disease
Score
Have you fallen in the past 12 months?
Yes = 6 No = 0
6
Have you experienced freezing of gait in the
past month?
Yes = 3 No = 0
3
Timing of patient walking over the middle 4m
of a 6m walkway at a comfortable pace:
3.6s to walk 4m = Yes
Yes = 2 No= 0
0
Total
Total Score 0 2-6 8-11
Probability of falling in the next Low (17%) Moderate (51%) High
(85%)
6 months
Tick the appropriate box
Food Chart
7
✓
Encouraging rest during severe episodes of pain
Recommending method of relief, for instance, back and neck rub application of cool cloths to the
forehead and avoiding the bright lights.
Risk Assessment
Mr B is 45 years old and has recently been diagnosed with Parkinson disease. Being a healthcare
professional, I have assessed his likelihood of fall.
Assessing the probability of falling in the
people with Parkinson’s disease
Score
Have you fallen in the past 12 months?
Yes = 6 No = 0
6
Have you experienced freezing of gait in the
past month?
Yes = 3 No = 0
3
Timing of patient walking over the middle 4m
of a 6m walkway at a comfortable pace:
3.6s to walk 4m = Yes
Yes = 2 No= 0
0
Total
Total Score 0 2-6 8-11
Probability of falling in the next Low (17%) Moderate (51%) High
(85%)
6 months
Tick the appropriate box
Food Chart
7
✓
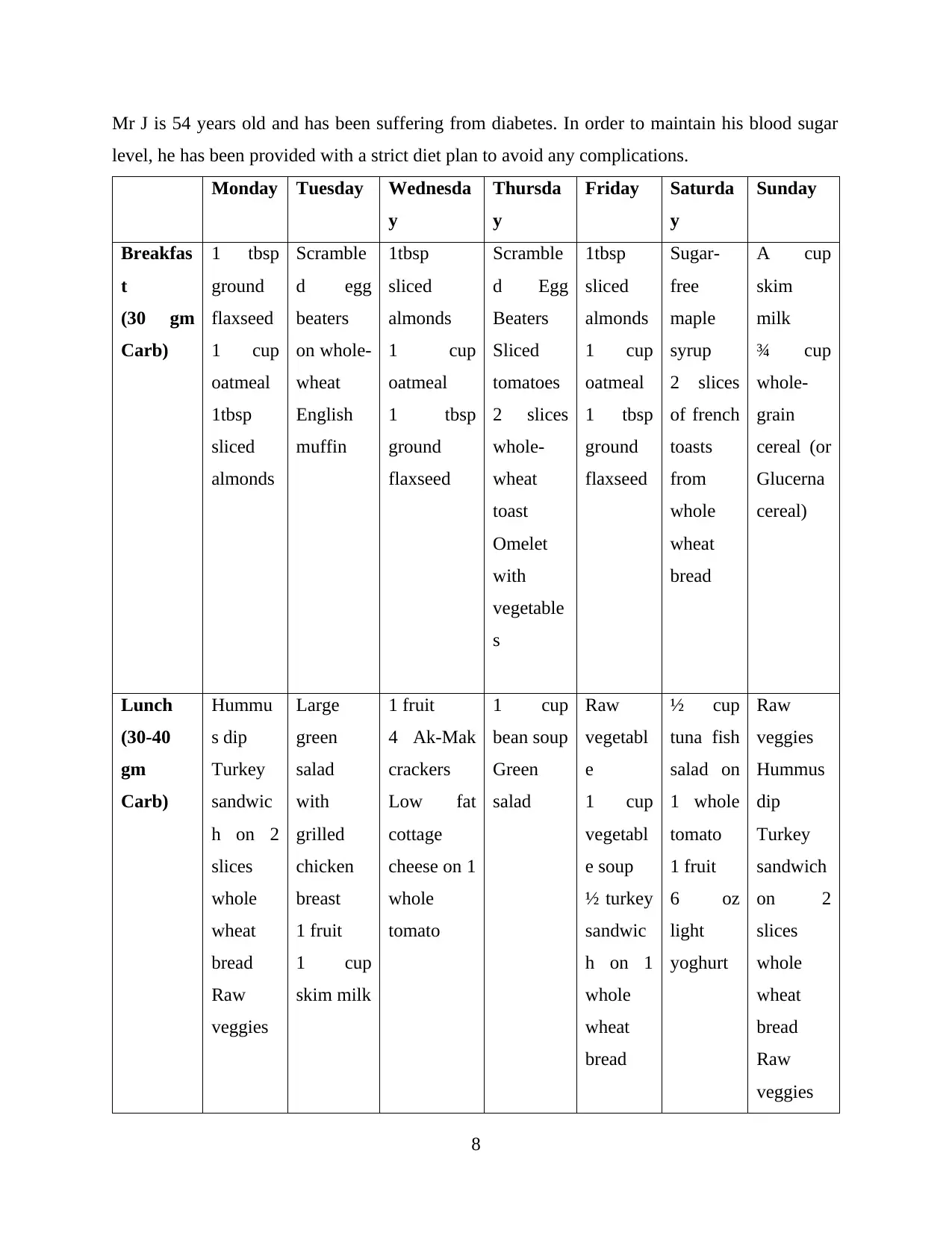
Mr J is 54 years old and has been suffering from diabetes. In order to maintain his blood sugar
level, he has been provided with a strict diet plan to avoid any complications.
Monday Tuesday Wednesda
y
Thursda
y
Friday Saturda
y
Sunday
Breakfas
t
(30 gm
Carb)
1 tbsp
ground
flaxseed
1 cup
oatmeal
1tbsp
sliced
almonds
Scramble
d egg
beaters
on whole-
wheat
English
muffin
1tbsp
sliced
almonds
1 cup
oatmeal
1 tbsp
ground
flaxseed
Scramble
d Egg
Beaters
Sliced
tomatoes
2 slices
whole-
wheat
toast
Omelet
with
vegetable
s
1tbsp
sliced
almonds
1 cup
oatmeal
1 tbsp
ground
flaxseed
Sugar-
free
maple
syrup
2 slices
of french
toasts
from
whole
wheat
bread
A cup
skim
milk
¾ cup
whole-
grain
cereal (or
Glucerna
cereal)
Lunch
(30-40
gm
Carb)
Hummu
s dip
Turkey
sandwic
h on 2
slices
whole
wheat
bread
Raw
veggies
Large
green
salad
with
grilled
chicken
breast
1 fruit
1 cup
skim milk
1 fruit
4 Ak-Mak
crackers
Low fat
cottage
cheese on 1
whole
tomato
1 cup
bean soup
Green
salad
Raw
vegetabl
e
1 cup
vegetabl
e soup
½ turkey
sandwic
h on 1
whole
wheat
bread
½ cup
tuna fish
salad on
1 whole
tomato
1 fruit
6 oz
light
yoghurt
Raw
veggies
Hummus
dip
Turkey
sandwich
on 2
slices
whole
wheat
bread
Raw
veggies
8
level, he has been provided with a strict diet plan to avoid any complications.
Monday Tuesday Wednesda
y
Thursda
y
Friday Saturda
y
Sunday
Breakfas
t
(30 gm
Carb)
1 tbsp
ground
flaxseed
1 cup
oatmeal
1tbsp
sliced
almonds
Scramble
d egg
beaters
on whole-
wheat
English
muffin
1tbsp
sliced
almonds
1 cup
oatmeal
1 tbsp
ground
flaxseed
Scramble
d Egg
Beaters
Sliced
tomatoes
2 slices
whole-
wheat
toast
Omelet
with
vegetable
s
1tbsp
sliced
almonds
1 cup
oatmeal
1 tbsp
ground
flaxseed
Sugar-
free
maple
syrup
2 slices
of french
toasts
from
whole
wheat
bread
A cup
skim
milk
¾ cup
whole-
grain
cereal (or
Glucerna
cereal)
Lunch
(30-40
gm
Carb)
Hummu
s dip
Turkey
sandwic
h on 2
slices
whole
wheat
bread
Raw
veggies
Large
green
salad
with
grilled
chicken
breast
1 fruit
1 cup
skim milk
1 fruit
4 Ak-Mak
crackers
Low fat
cottage
cheese on 1
whole
tomato
1 cup
bean soup
Green
salad
Raw
vegetabl
e
1 cup
vegetabl
e soup
½ turkey
sandwic
h on 1
whole
wheat
bread
½ cup
tuna fish
salad on
1 whole
tomato
1 fruit
6 oz
light
yoghurt
Raw
veggies
Hummus
dip
Turkey
sandwich
on 2
slices
whole
wheat
bread
Raw
veggies
8
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
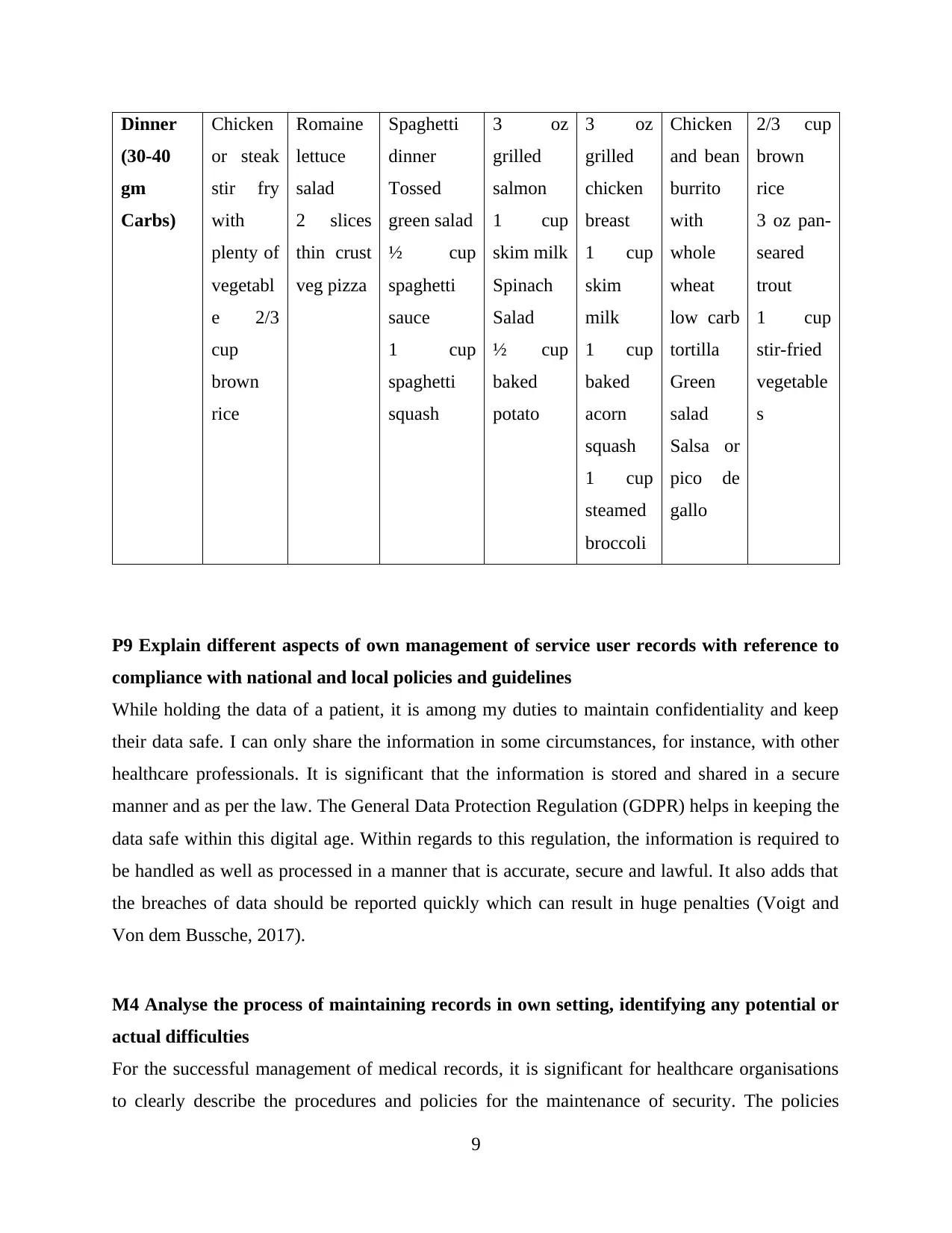
Dinner
(30-40
gm
Carbs)
Chicken
or steak
stir fry
with
plenty of
vegetabl
e 2/3
cup
brown
rice
Romaine
lettuce
salad
2 slices
thin crust
veg pizza
Spaghetti
dinner
Tossed
green salad
½ cup
spaghetti
sauce
1 cup
spaghetti
squash
3 oz
grilled
salmon
1 cup
skim milk
Spinach
Salad
½ cup
baked
potato
3 oz
grilled
chicken
breast
1 cup
skim
milk
1 cup
baked
acorn
squash
1 cup
steamed
broccoli
Chicken
and bean
burrito
with
whole
wheat
low carb
tortilla
Green
salad
Salsa or
pico de
gallo
2/3 cup
brown
rice
3 oz pan-
seared
trout
1 cup
stir-fried
vegetable
s
P9 Explain different aspects of own management of service user records with reference to
compliance with national and local policies and guidelines
While holding the data of a patient, it is among my duties to maintain confidentiality and keep
their data safe. I can only share the information in some circumstances, for instance, with other
healthcare professionals. It is significant that the information is stored and shared in a secure
manner and as per the law. The General Data Protection Regulation (GDPR) helps in keeping the
data safe within this digital age. Within regards to this regulation, the information is required to
be handled as well as processed in a manner that is accurate, secure and lawful. It also adds that
the breaches of data should be reported quickly which can result in huge penalties (Voigt and
Von dem Bussche, 2017).
M4 Analyse the process of maintaining records in own setting, identifying any potential or
actual difficulties
For the successful management of medical records, it is significant for healthcare organisations
to clearly describe the procedures and policies for the maintenance of security. The policies
9
(30-40
gm
Carbs)
Chicken
or steak
stir fry
with
plenty of
vegetabl
e 2/3
cup
brown
rice
Romaine
lettuce
salad
2 slices
thin crust
veg pizza
Spaghetti
dinner
Tossed
green salad
½ cup
spaghetti
sauce
1 cup
spaghetti
squash
3 oz
grilled
salmon
1 cup
skim milk
Spinach
Salad
½ cup
baked
potato
3 oz
grilled
chicken
breast
1 cup
skim
milk
1 cup
baked
acorn
squash
1 cup
steamed
broccoli
Chicken
and bean
burrito
with
whole
wheat
low carb
tortilla
Green
salad
Salsa or
pico de
gallo
2/3 cup
brown
rice
3 oz pan-
seared
trout
1 cup
stir-fried
vegetable
s
P9 Explain different aspects of own management of service user records with reference to
compliance with national and local policies and guidelines
While holding the data of a patient, it is among my duties to maintain confidentiality and keep
their data safe. I can only share the information in some circumstances, for instance, with other
healthcare professionals. It is significant that the information is stored and shared in a secure
manner and as per the law. The General Data Protection Regulation (GDPR) helps in keeping the
data safe within this digital age. Within regards to this regulation, the information is required to
be handled as well as processed in a manner that is accurate, secure and lawful. It also adds that
the breaches of data should be reported quickly which can result in huge penalties (Voigt and
Von dem Bussche, 2017).
M4 Analyse the process of maintaining records in own setting, identifying any potential or
actual difficulties
For the successful management of medical records, it is significant for healthcare organisations
to clearly describe the procedures and policies for the maintenance of security. The policies
9
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
should be written and must be retained for a period of about six years. The mismanagement of
health records put the patients at risk as it can result in a missed diagnosis, medication errors,
lapses in treatment and other prospective life-threatening events. The privacy of the patient is
also at risk as the medical records encompass highly sensitive personal information and when the
oversight happens, the privacy is compromised. The poor management of records can also leave
the medical practitioners, providers and hospitals vulnerable to lawsuits, costly fines and
criminal charges (Marutha, 2019).
D4 Evaluate the effectiveness of own completion of documentation in terms of meeting
service user needs, ensuring appropriate care is given and effective reporting is carried out
Each of the entries within the medical record is required to be timed, dates and legible. Every
entry must be signed by the individual who is making the entry and is required to be made
possible after the event to be documented and before the related staff member goes off duty. In
case there is a delay, the time of the event and the delay must be recorded along with the reasons
for the delay. Abbreviations must also be avoided as they can be ambiguous. Furthermore, the
entries of the medical record must be objective. The non-compliance must also be documented
within the progress record (Mathioudakis et al., 2016).
Conclusion
Digital health tools have been empowering the patients for taking a more active role in
monitoring their own health. While keeping the data of a patient, it is important to maintain
confidentiality and keep their data safe. The information is required to be handled as well as
processed in a manner that is accurate, secure and lawful. The poor management of records can
also leave the medical practitioners, providers and hospitals vulnerable to lawsuits, costly fines
and criminal charges.
10
health records put the patients at risk as it can result in a missed diagnosis, medication errors,
lapses in treatment and other prospective life-threatening events. The privacy of the patient is
also at risk as the medical records encompass highly sensitive personal information and when the
oversight happens, the privacy is compromised. The poor management of records can also leave
the medical practitioners, providers and hospitals vulnerable to lawsuits, costly fines and
criminal charges (Marutha, 2019).
D4 Evaluate the effectiveness of own completion of documentation in terms of meeting
service user needs, ensuring appropriate care is given and effective reporting is carried out
Each of the entries within the medical record is required to be timed, dates and legible. Every
entry must be signed by the individual who is making the entry and is required to be made
possible after the event to be documented and before the related staff member goes off duty. In
case there is a delay, the time of the event and the delay must be recorded along with the reasons
for the delay. Abbreviations must also be avoided as they can be ambiguous. Furthermore, the
entries of the medical record must be objective. The non-compliance must also be documented
within the progress record (Mathioudakis et al., 2016).
Conclusion
Digital health tools have been empowering the patients for taking a more active role in
monitoring their own health. While keeping the data of a patient, it is important to maintain
confidentiality and keep their data safe. The information is required to be handled as well as
processed in a manner that is accurate, secure and lawful. The poor management of records can
also leave the medical practitioners, providers and hospitals vulnerable to lawsuits, costly fines
and criminal charges.
10
References
Bombard, Y., Baker, G., Orlando, E., Fancott, C., Bhatia, P., Casalino, S., Onate, K., Denis, J.
and Pomey, M., 2018. Engaging patients to improve quality of care: a systematic review.
Implementation Science, 13(1), pp.1-22.
Daraghmi, E., Daraghmi, Y. and Yuan, S., 2019. MedChain: A design of blockchain-based
system for medical records access and permissions management. IEEE Access, pp.164595-
164613.
Gianfrancesco, M., Tamang, S., Yazdany, J. and Schmajuk, G., 2018. Potential biases in
machine learning algorithms using electronic health record data. JAMA internal medicine,
178(11), pp.1544-1547.
Greenhalgh, T., Vijayaraghavan, S., Wherton, J., Shaw, S., Byrne, E., Campbell-Richards, D.,
Bhattacharya, S., Hanson, P., Ramoutar, S., Gutteridge, C. and Hodkinson, I., 2016. Virtual
online consultations: advantages and limitations (VOCAL) study. BMJ open, 6(1), p.009388.
Heyworth, L., Kirsh, S., Zulman, D., Ferguson, J. and Kizer, K., 2020. Expanding access through
virtual care: The VA’s early experience with Covid-19. NEJM Catalyst Innovations in Care
Delivery, 1(4).
Lacity, M. and Willcocks, L., 2016. A new approach to automating services. MIT Sloan
Management Review, 58(1), pp.41-49.
Letellier, R. and Eppich, R., 2015. Recording, documentation and information management for
the conservation of heritage places.. Routledge.
Luchenski, S., Maguire, N., Aldridge, R., Hayward, A., Story, A., Perri, P., Withers, J., Clint, S.,
Fitzpatrick, S. and Hewett, N., 2018. What works in inclusion health: overview of effective
interventions for marginalised and excluded populations. The Lancet, 391(10117), pp.266-280.
Marutha, N., 2019. The application of legislative frameworks for the management of medical
records in Limpopo Province, South Africa. Information Development, 35(4), pp.551-563.
11
Bombard, Y., Baker, G., Orlando, E., Fancott, C., Bhatia, P., Casalino, S., Onate, K., Denis, J.
and Pomey, M., 2018. Engaging patients to improve quality of care: a systematic review.
Implementation Science, 13(1), pp.1-22.
Daraghmi, E., Daraghmi, Y. and Yuan, S., 2019. MedChain: A design of blockchain-based
system for medical records access and permissions management. IEEE Access, pp.164595-
164613.
Gianfrancesco, M., Tamang, S., Yazdany, J. and Schmajuk, G., 2018. Potential biases in
machine learning algorithms using electronic health record data. JAMA internal medicine,
178(11), pp.1544-1547.
Greenhalgh, T., Vijayaraghavan, S., Wherton, J., Shaw, S., Byrne, E., Campbell-Richards, D.,
Bhattacharya, S., Hanson, P., Ramoutar, S., Gutteridge, C. and Hodkinson, I., 2016. Virtual
online consultations: advantages and limitations (VOCAL) study. BMJ open, 6(1), p.009388.
Heyworth, L., Kirsh, S., Zulman, D., Ferguson, J. and Kizer, K., 2020. Expanding access through
virtual care: The VA’s early experience with Covid-19. NEJM Catalyst Innovations in Care
Delivery, 1(4).
Lacity, M. and Willcocks, L., 2016. A new approach to automating services. MIT Sloan
Management Review, 58(1), pp.41-49.
Letellier, R. and Eppich, R., 2015. Recording, documentation and information management for
the conservation of heritage places.. Routledge.
Luchenski, S., Maguire, N., Aldridge, R., Hayward, A., Story, A., Perri, P., Withers, J., Clint, S.,
Fitzpatrick, S. and Hewett, N., 2018. What works in inclusion health: overview of effective
interventions for marginalised and excluded populations. The Lancet, 391(10117), pp.266-280.
Marutha, N., 2019. The application of legislative frameworks for the management of medical
records in Limpopo Province, South Africa. Information Development, 35(4), pp.551-563.
11
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 13
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.