Rheumatoid Arthritis: Pathophysiology, Aetiology and Treatment
VerifiedAdded on 2021/04/24
|6
|1178
|44
Report
AI Summary
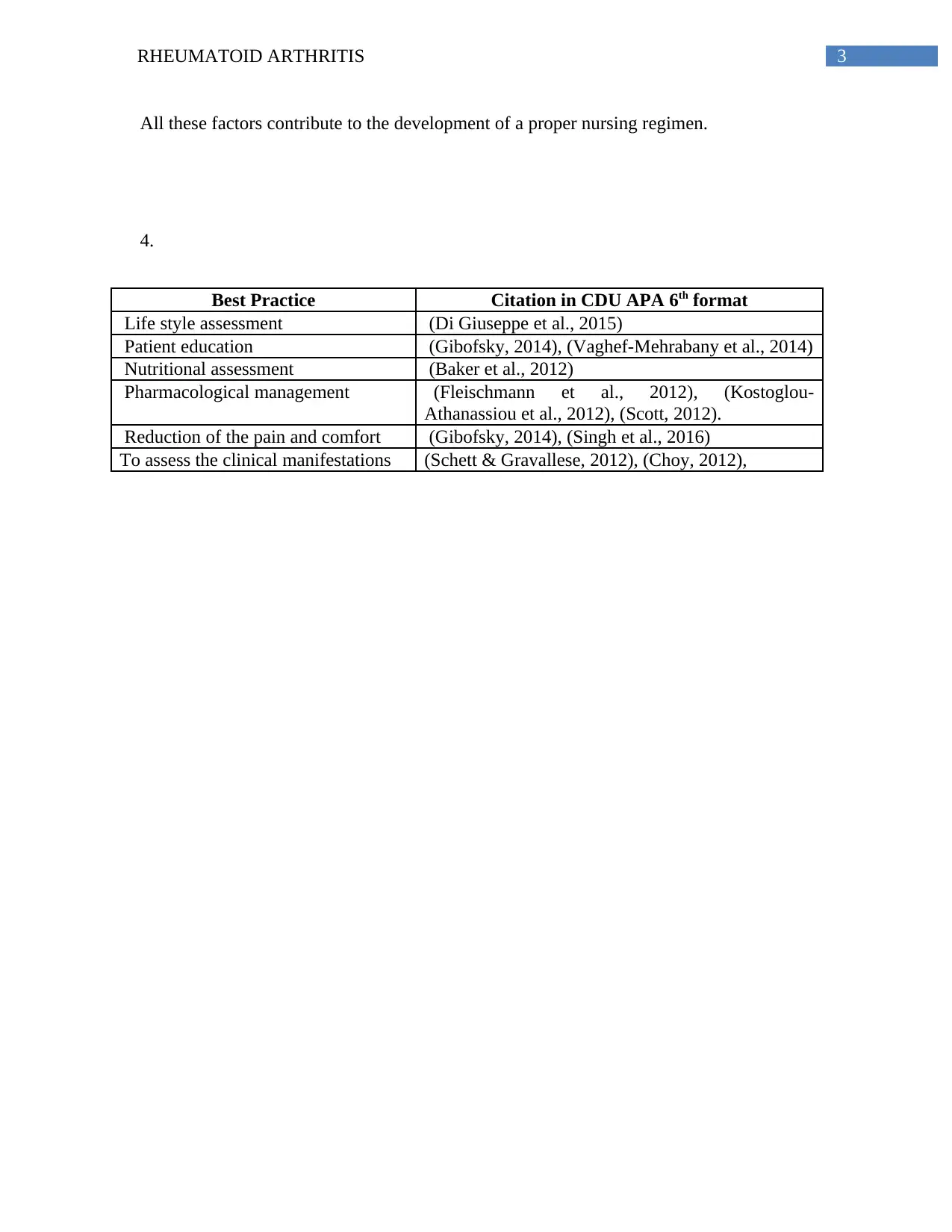
This report provides a comprehensive overview of Rheumatoid Arthritis (RA), a systemic inflammatory disease characterized by chronic joint inflammation and synovial hypertrophy. It delves into the pathophysiology, highlighting the roles of mononuclear phagocytes, fibroblasts, neutrophils, and CD4 T cells, as well as the impact of abnormal cytokine production. The report also explores the aetiology of RA, discussing genetic, environmental, immunological, hormonal, and lifestyle factors. It examines the populations most affected, including the influence of cigarette smoking, hormonal changes, and dietary factors. Furthermore, the report emphasizes the clinical problem and its relevance to nursing practice, detailing the financial costs, statistical prevalence, and workload implications of RA. It concludes with a discussion of best practices, including lifestyle assessment, patient education, nutritional assessment, pharmacological management, pain reduction, and the assessment of clinical manifestations, all supported by citations in CDU APA 6th format.

1 out of 6
Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.