Safeguarding in Health and Social Care: Abuse Risk and Prevention
VerifiedAdded on 2023/04/20
|27
|5876
|347
Report
AI Summary
This report provides a comprehensive overview of safeguarding in health and social care, focusing on the vulnerabilities of particular individuals and groups to abuse and harm. It analyzes risk factors, the impact of social and cultural elements, and the strengths and weaknesses of current legislation and policy. The report also examines the roles of key professionals in protecting vulnerable individuals, existing working practices, and strategies designed to minimize abuse, including evaluations of their effectiveness and potential improvements. Case studies, such as Baby P and Winterbourne View Hospital, are used to illustrate the complexities and challenges in safeguarding vulnerable populations. The document emphasizes the importance of communication, collaboration, and robust policies to ensure the safety and well-being of those in health and social care settings, highlighting the need for continuous improvement in practices and strategies to minimize abuse.

Running head: SAFEGUARDING IN HEALTH AND SOCIAL CARE
Safeguarding in Health and Social Care
Student’s ID: D0917119
Group: HSS7
Lecturer: Dr. Susan Marchant-Haycox
Safeguarding in Health and Social Care
Student’s ID: D0917119
Group: HSS7
Lecturer: Dr. Susan Marchant-Haycox
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Executive Summary
Safeguarding is a difficult and delicate field in Health and Social Care society. It is about
people and organizations working together to protect people’s health and well-being and
human rights and allowing them to live safely from harm, without abuse and neglect. It is
essential for high-quality healthcare and social assistance.(Care Quality Commission, 2018)
Abuse is the harm caused to a vulnerable adult through an act, or non-fulfilment by another
adult. Abuse is a major problem all over the world and has been debated a lot in recent years
in the public domain.
After Victoria’s Climbie death in February 2000who was abused and neglected by her great-
aunt and her husband, a new guidance document was developed in same year and published
on the Government site “No secrets: It is commended to all commissioners and providers of
health and social care services including primary care groups, regulators of such care services
and appropriate criminal justice agencies. These statutory agencies should work together in
partnership (as advocated in the Health Act 1999) to ensure that appropriate policies,
procedures and practices are in place and implemented locally. They should do so in
collaboration with all agencies involved in the public, voluntary and private sectors and they
should also consult service users, their careers and representative groups”(Department of
Health (NHS), 2000)
The following report includes two severe Case Reviews: the terrible death of 17-month old
Baby P, born in London who after more than eight months suffered more than fifty injuries
while he was seen 60 times by the London Borough of Haringey Children's Services and the
National Health Service (NHS). The second case is Winterbourne View Hospital, in Bristol
concerns patients with learning disabilities and/or autism who have been subjected to
inappropriate and abusive treatments by hospital workers.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Executive Summary
Safeguarding is a difficult and delicate field in Health and Social Care society. It is about
people and organizations working together to protect people’s health and well-being and
human rights and allowing them to live safely from harm, without abuse and neglect. It is
essential for high-quality healthcare and social assistance.(Care Quality Commission, 2018)
Abuse is the harm caused to a vulnerable adult through an act, or non-fulfilment by another
adult. Abuse is a major problem all over the world and has been debated a lot in recent years
in the public domain.
After Victoria’s Climbie death in February 2000who was abused and neglected by her great-
aunt and her husband, a new guidance document was developed in same year and published
on the Government site “No secrets: It is commended to all commissioners and providers of
health and social care services including primary care groups, regulators of such care services
and appropriate criminal justice agencies. These statutory agencies should work together in
partnership (as advocated in the Health Act 1999) to ensure that appropriate policies,
procedures and practices are in place and implemented locally. They should do so in
collaboration with all agencies involved in the public, voluntary and private sectors and they
should also consult service users, their careers and representative groups”(Department of
Health (NHS), 2000)
The following report includes two severe Case Reviews: the terrible death of 17-month old
Baby P, born in London who after more than eight months suffered more than fifty injuries
while he was seen 60 times by the London Borough of Haringey Children's Services and the
National Health Service (NHS). The second case is Winterbourne View Hospital, in Bristol
concerns patients with learning disabilities and/or autism who have been subjected to
inappropriate and abusive treatments by hospital workers.
2
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Table of Contents
Task 1.1: Report: Explain why particular individuals and groups may be vulnerable to abuse
and/or harm to self and others....................................................................................................3
Task 1.2: Campaign poster: Review risk factors which may lead to incidence of abuse and/or
harm to self and others...............................................................................................................5
Task 1.3: Report: Analyse the impact of social and cultural factors on different types of abuse
and/or harm to self and others....................................................................................................7
Task 2.1: Essay: Analyse the strength and weaknesses in current legislation and policy
relating to those vulnerable to abuse..........................................................................................9
Task: 2.2: Report: Explain how key professionals are involved in the protection of
individuals and groups vulnerable to abuse.............................................................................11
Task 3.1: Presentation: Explain existing working practices and strategies designed to
minimize abuse in health and social care contexts...................................................................13
Task 3.2: Presentation: Evaluation of the effectiveness of work practices and strategies
designed to minimise abuse in health and social care contexts (3.2).......................................18
Task 3.3: Presentation: Discussion of possible improvements to working practices and
strategies to minimise abuse in health and social care contexts (3.3)......................................21
Task 3.2: Report: Evaluate the effectiveness of working practices and strategies used to
minimise abuse in health and social care contexts...................................................................24
References................................................................................................................................25
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Table of Contents
Task 1.1: Report: Explain why particular individuals and groups may be vulnerable to abuse
and/or harm to self and others....................................................................................................3
Task 1.2: Campaign poster: Review risk factors which may lead to incidence of abuse and/or
harm to self and others...............................................................................................................5
Task 1.3: Report: Analyse the impact of social and cultural factors on different types of abuse
and/or harm to self and others....................................................................................................7
Task 2.1: Essay: Analyse the strength and weaknesses in current legislation and policy
relating to those vulnerable to abuse..........................................................................................9
Task: 2.2: Report: Explain how key professionals are involved in the protection of
individuals and groups vulnerable to abuse.............................................................................11
Task 3.1: Presentation: Explain existing working practices and strategies designed to
minimize abuse in health and social care contexts...................................................................13
Task 3.2: Presentation: Evaluation of the effectiveness of work practices and strategies
designed to minimise abuse in health and social care contexts (3.2).......................................18
Task 3.3: Presentation: Discussion of possible improvements to working practices and
strategies to minimise abuse in health and social care contexts (3.3)......................................21
Task 3.2: Report: Evaluate the effectiveness of working practices and strategies used to
minimise abuse in health and social care contexts...................................................................24
References................................................................................................................................25
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 1.1: Report: Explain why particular individuals and groups may be vulnerable to
abuse and/or harm to self and others
Introduction
According to the Care Quality Commission (2018), safeguarding people is a complex
yet sensitive area in the domain of health and social care environment. It mainly deals with
protecting health and well-being of the individuals and thereby allowing them to live free,
away from harm, injury, neglect and abuse. It is the fundamental human rights as highlighted
under the high-quality health and social care. The following report deals with the case study
of 17-month-old Baby P who suffered more than fifty injuries for a tenure of 8-month leading
to tragic death while brought to London Borough of Haringey Children’s services – National
Health Services (Local Safe Guarding Children Board Haringey 2009). The report will
discuss why children are more vulnerable to physical or mental abuse in relation to the abuse
mention case report.
Discussion
As per the case study, Baby P suffered from multiple injuries which the doctors failed
to recognise. One of the reason why the doctors failed to recognise is Baby P was only 17
month old and he was unable to raise his voice in order to highlight is own shared of pain or
trauma. According to Flaherty et al. (2014), the individuals who are more vulnerable in
getting affected with the physical abuse are the children who are below 18-years of age.
Flaherty et al. (2014) further highlighted that the common form of abuse for child is physical
abuse causing bruises. As per the case study, Baby P suffered from eight fractured ribs on the
left side of the body along with fractured spine leading to death out of fracture or dislocation
of the thoraco-lumbar spine. Flaherty et al. (2014) stated that children are more vulnerable to
physical abuse and it goes detected because caregiver might have altered the history
intentionally n order to conceal the abuse. This leads to mis-diagnosis.
According to Straus, Gelles and Steinmetz (2017) adults who are found guilty in
abusing children generally have a past history of getting victimised of physical abuse during
their childhood. Ms A, mother of Baby P has a previously experience of domestic violence.
She and her brother experienced domestic violence from her father who was a sex offender.
Her mother was neglectful and one of her relative was a paedophile leading a traumatic
childhood. Mr. H, boyfriend of Ms A is fascinated by pain and is a sadist. Their (Mr. H and
Ms A) unstable psychological state increased the vulnerability of Baby P of getting
victimised by physical abuse.
Children are vulnerable for the physical or mental abuse as they are neglected by their
parents. National Society for the Prevention of Cruelty to Children (NSPCC) (2018), one out
of the 10 children experiences neglect. During the tenure of 2017, 27,000 children identified
as being neglected. Common form of neglect includes, leaving the child dirty, hungry and
depriving the child from adequate food, shelter and medical care. Under neglect, the child is
also put under the danger of physical and emotional harm. Baby P was the victim of physical
abuse and neglect in the domain of adequate medical care.
Conclusion
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 1.1: Report: Explain why particular individuals and groups may be vulnerable to
abuse and/or harm to self and others
Introduction
According to the Care Quality Commission (2018), safeguarding people is a complex
yet sensitive area in the domain of health and social care environment. It mainly deals with
protecting health and well-being of the individuals and thereby allowing them to live free,
away from harm, injury, neglect and abuse. It is the fundamental human rights as highlighted
under the high-quality health and social care. The following report deals with the case study
of 17-month-old Baby P who suffered more than fifty injuries for a tenure of 8-month leading
to tragic death while brought to London Borough of Haringey Children’s services – National
Health Services (Local Safe Guarding Children Board Haringey 2009). The report will
discuss why children are more vulnerable to physical or mental abuse in relation to the abuse
mention case report.
Discussion
As per the case study, Baby P suffered from multiple injuries which the doctors failed
to recognise. One of the reason why the doctors failed to recognise is Baby P was only 17
month old and he was unable to raise his voice in order to highlight is own shared of pain or
trauma. According to Flaherty et al. (2014), the individuals who are more vulnerable in
getting affected with the physical abuse are the children who are below 18-years of age.
Flaherty et al. (2014) further highlighted that the common form of abuse for child is physical
abuse causing bruises. As per the case study, Baby P suffered from eight fractured ribs on the
left side of the body along with fractured spine leading to death out of fracture or dislocation
of the thoraco-lumbar spine. Flaherty et al. (2014) stated that children are more vulnerable to
physical abuse and it goes detected because caregiver might have altered the history
intentionally n order to conceal the abuse. This leads to mis-diagnosis.
According to Straus, Gelles and Steinmetz (2017) adults who are found guilty in
abusing children generally have a past history of getting victimised of physical abuse during
their childhood. Ms A, mother of Baby P has a previously experience of domestic violence.
She and her brother experienced domestic violence from her father who was a sex offender.
Her mother was neglectful and one of her relative was a paedophile leading a traumatic
childhood. Mr. H, boyfriend of Ms A is fascinated by pain and is a sadist. Their (Mr. H and
Ms A) unstable psychological state increased the vulnerability of Baby P of getting
victimised by physical abuse.
Children are vulnerable for the physical or mental abuse as they are neglected by their
parents. National Society for the Prevention of Cruelty to Children (NSPCC) (2018), one out
of the 10 children experiences neglect. During the tenure of 2017, 27,000 children identified
as being neglected. Common form of neglect includes, leaving the child dirty, hungry and
depriving the child from adequate food, shelter and medical care. Under neglect, the child is
also put under the danger of physical and emotional harm. Baby P was the victim of physical
abuse and neglect in the domain of adequate medical care.
Conclusion
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Thus from the above discussion, it can be concluded that Baby P was more vulnerable
to physical abuse as his care givers were themselves victim of domestic violence during their
own childhood (Baby P’s mother) or have an unstable psychological condition (Mr. H).
Moreover, Baby P also was a victim of neglect increasing his vulnerability of abuse. If child
who are prone to physical abuse are not rescued or protected on time then it might lead to
tragic outcome like Baby P.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Thus from the above discussion, it can be concluded that Baby P was more vulnerable
to physical abuse as his care givers were themselves victim of domestic violence during their
own childhood (Baby P’s mother) or have an unstable psychological condition (Mr. H).
Moreover, Baby P also was a victim of neglect increasing his vulnerability of abuse. If child
who are prone to physical abuse are not rescued or protected on time then it might lead to
tragic outcome like Baby P.
5
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 1.2: Campaign poster: Review risk factors which may lead to incidence of abuse
and/or harm to self and others
Speaker Notes
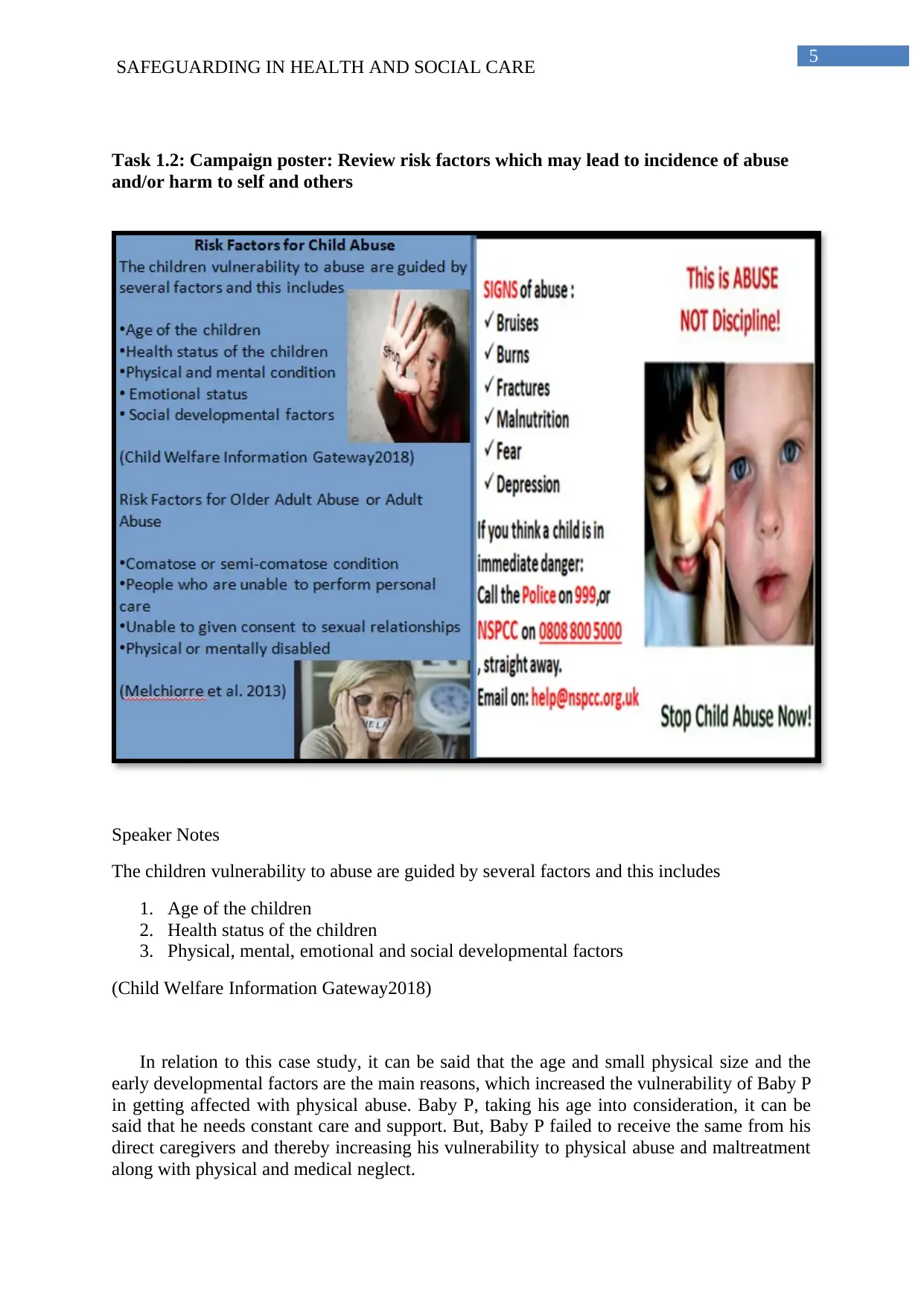
The children vulnerability to abuse are guided by several factors and this includes
1. Age of the children
2. Health status of the children
3. Physical, mental, emotional and social developmental factors
(Child Welfare Information Gateway2018)
In relation to this case study, it can be said that the age and small physical size and the
early developmental factors are the main reasons, which increased the vulnerability of Baby P
in getting affected with physical abuse. Baby P, taking his age into consideration, it can be
said that he needs constant care and support. But, Baby P failed to receive the same from his
direct caregivers and thereby increasing his vulnerability to physical abuse and maltreatment
along with physical and medical neglect.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 1.2: Campaign poster: Review risk factors which may lead to incidence of abuse
and/or harm to self and others
Speaker Notes
The children vulnerability to abuse are guided by several factors and this includes
1. Age of the children
2. Health status of the children
3. Physical, mental, emotional and social developmental factors
(Child Welfare Information Gateway2018)
In relation to this case study, it can be said that the age and small physical size and the
early developmental factors are the main reasons, which increased the vulnerability of Baby P
in getting affected with physical abuse. Baby P, taking his age into consideration, it can be
said that he needs constant care and support. But, Baby P failed to receive the same from his
direct caregivers and thereby increasing his vulnerability to physical abuse and maltreatment
along with physical and medical neglect.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
SAFEGUARDING IN HEALTH AND SOCIAL CARE
According to Child Welfare Information Gateway (2018), children who are under the age
group of 0 to 4 years are more vulnerable to become victims of physical and mental abuse.
This vulnerability increases if the children have any predispose learning disabilities, physical
disability or are mentally impaired.
Children who resides in community care, orphanage, day care, residential care are also
vulnerable towards physical or mental abuse
The individuals who are above 56 to 70 years of age are also vulnerable to abuse. If these
older adults are comatose or semi-comatose, their vulnerability increases further.
People who are dependent upon others for personal care like the older adults or lack
the proper mental capacity in order to give consent for the sexual relationships or the adults
who do not have social awareness also experiences abuse from the society both physical or
mental which is detrimental for the health and well-being (Melchiorre et al. 2013).
The common signs of children abuse include
Fractures
Burns
Bruises
Malnutrition
Fear
Depression
It is the duty of the parents to look for these signs and symptoms in order to point-out any
visible relevance of child-abuse. They can also take help from professional and voluntary
agencies like the Safe Guarding Children from Harm and Child Protection.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
According to Child Welfare Information Gateway (2018), children who are under the age
group of 0 to 4 years are more vulnerable to become victims of physical and mental abuse.
This vulnerability increases if the children have any predispose learning disabilities, physical
disability or are mentally impaired.
Children who resides in community care, orphanage, day care, residential care are also
vulnerable towards physical or mental abuse
The individuals who are above 56 to 70 years of age are also vulnerable to abuse. If these
older adults are comatose or semi-comatose, their vulnerability increases further.
People who are dependent upon others for personal care like the older adults or lack
the proper mental capacity in order to give consent for the sexual relationships or the adults
who do not have social awareness also experiences abuse from the society both physical or
mental which is detrimental for the health and well-being (Melchiorre et al. 2013).
The common signs of children abuse include
Fractures
Burns
Bruises
Malnutrition
Fear
Depression
It is the duty of the parents to look for these signs and symptoms in order to point-out any
visible relevance of child-abuse. They can also take help from professional and voluntary
agencies like the Safe Guarding Children from Harm and Child Protection.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 1.3: Report: Analyse the impact of social and cultural factors on different types of
abuse and/or harm to self and others
Introduction
The aim of this report is to critically analyze the social and the cultural factors that
cast a significant impact on different types of abuse and/or harm to self or other. The impact
of the social and the cultural risk factor will be discussed in detailed reference to the case
study of Baby P who died at an age of 17-month due to physical abuse coming from his own
family members.
Discussion
The main social factors, impact the vulnerability to abuse and/or self harm include
health, housing, poverty level, the educational qualification, the level of social exclusion,
falling under the disadvantage group and networks of support. The principal cultural factors,
which promote self harm or abuse from others, include ethnic and spiritual belief (Shelter
2006).
According to Mental Health Foundation (2018) self-harm is often influenced by
factors like depression, anxiety, social isolation, bullying, low self-esteem, substance abuse
and in other transition states like change in school. As a result of the change in the
surrounding social environment or mental anxiety the emotional suffering or the emotional
load of the person increases leading to panic and ultimately ending up in self-harm. Mental
Health Foundation (2018) is of the opinion that self-harm is done in order to get temporary
relief.
In this case study, Baby P is a victim of child abuse. The underlying reason behind
Baby P’s child abuse is problematic childhood of Baby P’s mother. According to Mental
Health Foundation (2018), high level of parental stress in combination with the traumatic
childhood of the parents may result in increase in the chances of child abuse. Both Ms A and
her brother have a problematic childhood. Ms A’s father was a sexual abuser along with a
paedophile family relative who used to abuse Ms A and her brother. This previous
victimization of Ms A might have increased the vindictive nature of the Ms A against her
own son. The housing or the family environment under which Baby P used to reside was not
comfortable. Ms A’s boyfriend, Mr. H was an illiterate with poor intellect level as
highlighted in the case study. He was fascinated with pain and he took immense pleasure in
toughening up Baby P as he himself was bullied during his childhood days by his older
brother. Both Mr H’s and his brother, Mr L has previous reported history of older adult abuse
(their own grand-mother) for property related issues. Thus unhealthy or unsafe surrounding
social environment with disturbed mental and the educational qualification is reason behind
the increase in the vulnerability of physical abuse over Baby P (Jütte et al. 2014). According
to Shelter (2006), children growing up in bad housing are more vulnerable in getting affected
with physical abuse.
According to Browne (2009), under-achievement in the working class or social
isolation or poor cultural background also increase a criminal mindset and a sense of
depression among the adults and these provoke them to cause harm to the child as it gives
them an unparallel pleasure and this was the case for Mr. H.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 1.3: Report: Analyse the impact of social and cultural factors on different types of
abuse and/or harm to self and others
Introduction
The aim of this report is to critically analyze the social and the cultural factors that
cast a significant impact on different types of abuse and/or harm to self or other. The impact
of the social and the cultural risk factor will be discussed in detailed reference to the case
study of Baby P who died at an age of 17-month due to physical abuse coming from his own
family members.
Discussion
The main social factors, impact the vulnerability to abuse and/or self harm include
health, housing, poverty level, the educational qualification, the level of social exclusion,
falling under the disadvantage group and networks of support. The principal cultural factors,
which promote self harm or abuse from others, include ethnic and spiritual belief (Shelter
2006).
According to Mental Health Foundation (2018) self-harm is often influenced by
factors like depression, anxiety, social isolation, bullying, low self-esteem, substance abuse
and in other transition states like change in school. As a result of the change in the
surrounding social environment or mental anxiety the emotional suffering or the emotional
load of the person increases leading to panic and ultimately ending up in self-harm. Mental
Health Foundation (2018) is of the opinion that self-harm is done in order to get temporary
relief.
In this case study, Baby P is a victim of child abuse. The underlying reason behind
Baby P’s child abuse is problematic childhood of Baby P’s mother. According to Mental
Health Foundation (2018), high level of parental stress in combination with the traumatic
childhood of the parents may result in increase in the chances of child abuse. Both Ms A and
her brother have a problematic childhood. Ms A’s father was a sexual abuser along with a
paedophile family relative who used to abuse Ms A and her brother. This previous
victimization of Ms A might have increased the vindictive nature of the Ms A against her
own son. The housing or the family environment under which Baby P used to reside was not
comfortable. Ms A’s boyfriend, Mr. H was an illiterate with poor intellect level as
highlighted in the case study. He was fascinated with pain and he took immense pleasure in
toughening up Baby P as he himself was bullied during his childhood days by his older
brother. Both Mr H’s and his brother, Mr L has previous reported history of older adult abuse
(their own grand-mother) for property related issues. Thus unhealthy or unsafe surrounding
social environment with disturbed mental and the educational qualification is reason behind
the increase in the vulnerability of physical abuse over Baby P (Jütte et al. 2014). According
to Shelter (2006), children growing up in bad housing are more vulnerable in getting affected
with physical abuse.
According to Browne (2009), under-achievement in the working class or social
isolation or poor cultural background also increase a criminal mindset and a sense of
depression among the adults and these provoke them to cause harm to the child as it gives
them an unparallel pleasure and this was the case for Mr. H.
8
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Conclusion
Thus from the above discussion, it can be concluded that the troubled childhood of the
direct care givers of the Baby P along with lack of proper education and unsuccessful
professional life are the main guiding factors behind the increase in the impact of child abuse.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Conclusion
Thus from the above discussion, it can be concluded that the troubled childhood of the
direct care givers of the Baby P along with lack of proper education and unsuccessful
professional life are the main guiding factors behind the increase in the impact of child abuse.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 2.1: Essay: Analyse the strength and weaknesses in current legislation and policy
relating to those vulnerable to abuse
Introduction
According to Peroni and Timmer (2013), there are numerous policies, acts and
guidance in order to protect the rights of the vulnerable individuals. However, numerous
reports have highlighted that these policies either have certain gaps in their rule execution or
are not executed in a comprehensive manner. As a result, the target group for who the policy
is directed suffer the most. The following essay aims of analyze the strength and the
weakness in the cultural legislation and policy designed for the group of individuals who are
vulnerable to physical or mental abuse. The essay will mainly focus on the case of the
Winterbourne View Hospital (WVH), which procures care for the people with learning
disabilities, autism and other complex mental health problems. As per the case study, many
patients in the WVH are slapped forcefully restrained under their hairs and are given forced
medications. This resulted in the poor health outcomes of the patients.
Discussion
The first act that can be highlighted in relation to this case study is Safeguarding
Vulnerable Groups Act [SVGA] (2006). This act led to an establishment of Independent
Safeguarding Authority which eventually merged with Criminal Records Bureau in 2012 and
led to the foundation of Disclosure and Barring Service (DBS). The act prevents harm or
risk of harm of vulnerable population by restricting staffs with dubious character to indulge
into the professional of care giving process to the vulnerable children and adults. Under this
Act, a social or healthcare worker who has previous professional history of abusing
vulnerable children or adults is black listed (Social Care Institute for Excellence 2013).
However, the main gap in this Act, persons, who are found unsuitable to for working under
UK legislation, can able to do so abroad. Moreover, the case study of the WVH so revealed
that SVGA is not implemented comprehensively as there are many people in the hospital
whose exact duty was not defined or convincing.
The second act that can be discussed is Protection of Vulnerable Adults Scheme
(POVA). The act was introduced by the Care Standards Act 2000 and the regulations are
similar to that of SVGA. POVA mainly has a list of people who are banned from serving as a
care-giver in any registered care home or domiciliary care agency. However, from the case
study it can be highlighted the employees are abusive who used to forcefully restrained the
patients and used to give them forceful medications. Thus it can be said that the employees of
WVH are either novice or the POVA was implemented during the recruitment of the
employees.
In this context, the third and the most important right that can be discussed include the
Human Rights Act (HRA) 1998. The Act came into effect during 2000 under the European
Convection on Human Rights (ECHR) and it mainly focuses on the fair treatment for all the
people. However, the outcome of the WVH highlighted that the Human Rights Act is not
implemented nor the government of the UK take strict considerations for the comprehensive
implementation of the Act. As per the case study review, there was weakness in the justice
system’s ability to hold the management of the healthcare organisations in order to account
for the quality and safety of the patient care. Peroni and Timmer (2013) further highlighted
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task 2.1: Essay: Analyse the strength and weaknesses in current legislation and policy
relating to those vulnerable to abuse
Introduction
According to Peroni and Timmer (2013), there are numerous policies, acts and
guidance in order to protect the rights of the vulnerable individuals. However, numerous
reports have highlighted that these policies either have certain gaps in their rule execution or
are not executed in a comprehensive manner. As a result, the target group for who the policy
is directed suffer the most. The following essay aims of analyze the strength and the
weakness in the cultural legislation and policy designed for the group of individuals who are
vulnerable to physical or mental abuse. The essay will mainly focus on the case of the
Winterbourne View Hospital (WVH), which procures care for the people with learning
disabilities, autism and other complex mental health problems. As per the case study, many
patients in the WVH are slapped forcefully restrained under their hairs and are given forced
medications. This resulted in the poor health outcomes of the patients.
Discussion
The first act that can be highlighted in relation to this case study is Safeguarding
Vulnerable Groups Act [SVGA] (2006). This act led to an establishment of Independent
Safeguarding Authority which eventually merged with Criminal Records Bureau in 2012 and
led to the foundation of Disclosure and Barring Service (DBS). The act prevents harm or
risk of harm of vulnerable population by restricting staffs with dubious character to indulge
into the professional of care giving process to the vulnerable children and adults. Under this
Act, a social or healthcare worker who has previous professional history of abusing
vulnerable children or adults is black listed (Social Care Institute for Excellence 2013).
However, the main gap in this Act, persons, who are found unsuitable to for working under
UK legislation, can able to do so abroad. Moreover, the case study of the WVH so revealed
that SVGA is not implemented comprehensively as there are many people in the hospital
whose exact duty was not defined or convincing.
The second act that can be discussed is Protection of Vulnerable Adults Scheme
(POVA). The act was introduced by the Care Standards Act 2000 and the regulations are
similar to that of SVGA. POVA mainly has a list of people who are banned from serving as a
care-giver in any registered care home or domiciliary care agency. However, from the case
study it can be highlighted the employees are abusive who used to forcefully restrained the
patients and used to give them forceful medications. Thus it can be said that the employees of
WVH are either novice or the POVA was implemented during the recruitment of the
employees.
In this context, the third and the most important right that can be discussed include the
Human Rights Act (HRA) 1998. The Act came into effect during 2000 under the European
Convection on Human Rights (ECHR) and it mainly focuses on the fair treatment for all the
people. However, the outcome of the WVH highlighted that the Human Rights Act is not
implemented nor the government of the UK take strict considerations for the comprehensive
implementation of the Act. As per the case study review, there was weakness in the justice
system’s ability to hold the management of the healthcare organisations in order to account
for the quality and safety of the patient care. Peroni and Timmer (2013) further highlighted
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
SAFEGUARDING IN HEALTH AND SOCIAL CARE
that the HRA fails to provide a comprehensive coverage to the marginalised subjects leading
to discrimination. The same instance was reflected in the scenario of the WVH where rights
of the residence of WVH were undermined brutally. The people who indulging under
physical restrained must be counted to be guilty under the Disability Hate Crimes (DHC)
which is based on the ignorance, hate and prejudice. 6 out of the 11 accused employees of
WVH were jailed and this can be highlighted as the strength of HRA (National Health
Service (NHS) News 2012). However, overall implementation of the DHC is time consuming
and expensive process with multiple trials at the court.
While describing about the legislations and policy about the people with mental health
complications who are vulnerable to physical as well as mental abuse under the context of the
WVH case study, the most important act is Mental Health Act (2007). It was initially
implemented on 1983 and later amended on 2007. The amended act provides powers of
compulsion and introduces compulsory community treatment orders. It makes patient’s
compliance with treatment in the form of statutory requirement (Community Care UK 2018).
One of the strength of this law is it provides legal decision making framework on behalf of
the adults who are 16 years or older and lack the intellectual ability to make decision for
themselves (Mental Health Alliance 2012). The scenario of WVH highlighted weakness in
the ability of the justice system in the domain of holding their management accountable for
the safety and quality of the service users. Moreover, there is gaps in the segmentations of the
patients in WVH which lead to gaps in the significant implementation of the MHA (2007).
The investigation revealed that there are people in the hospital who do not have potential
reasons to be in the hospital. Some patients were initially admitted under the terms and
conditions of MHA however, their extended period of stay in the hospital ended the tenure of
the MHA (National Health Service (NHS) News 2012). While others were admitted as an
informal basis and then gradually became sectioned. Thus, it can be said that there are mis-
appropriate application of MHA in WVH.
Another strong act in this domain is the Mental Capacity Act of 2005 (MCA). MCA
is designed to protect the vulnerable individuals and thereby empowering individuals to lack
the mental capacity like the people who are suffering from autism, dementia, brain injury and
other complex mental health complications. The act is applicable for the people who are aged
16 and over. The principal disadvantage of the act is that if a person is at risk or in danger to
the society, they will be treated appropriately or might be sectioned against his or her will
leading to hamper in the autonomy. The same instant occurred in the WVH where rules are
not abided systematically in order to re-evaluate the patient’s state of safety.
Conclusion
Thus from the above discussion, it can be concluded that there are several legislation
and policies in order to protect the rights and the safety of the people who are vulnerable to
the mental and the physical abuse. The analysis of these laws in relation to the case study of
the WVH highlighted that there are gaps in the implementation of the law in WVH
organizations like Safeguarding Vulnerable Group Act [SVGA] (2006) and Protection of
Vulnerable Adults Scheme (POVA). These gaps in the implementation of the law lead to
unwanted outcome of the residents of WVH.
SAFEGUARDING IN HEALTH AND SOCIAL CARE
that the HRA fails to provide a comprehensive coverage to the marginalised subjects leading
to discrimination. The same instance was reflected in the scenario of the WVH where rights
of the residence of WVH were undermined brutally. The people who indulging under
physical restrained must be counted to be guilty under the Disability Hate Crimes (DHC)
which is based on the ignorance, hate and prejudice. 6 out of the 11 accused employees of
WVH were jailed and this can be highlighted as the strength of HRA (National Health
Service (NHS) News 2012). However, overall implementation of the DHC is time consuming
and expensive process with multiple trials at the court.
While describing about the legislations and policy about the people with mental health
complications who are vulnerable to physical as well as mental abuse under the context of the
WVH case study, the most important act is Mental Health Act (2007). It was initially
implemented on 1983 and later amended on 2007. The amended act provides powers of
compulsion and introduces compulsory community treatment orders. It makes patient’s
compliance with treatment in the form of statutory requirement (Community Care UK 2018).
One of the strength of this law is it provides legal decision making framework on behalf of
the adults who are 16 years or older and lack the intellectual ability to make decision for
themselves (Mental Health Alliance 2012). The scenario of WVH highlighted weakness in
the ability of the justice system in the domain of holding their management accountable for
the safety and quality of the service users. Moreover, there is gaps in the segmentations of the
patients in WVH which lead to gaps in the significant implementation of the MHA (2007).
The investigation revealed that there are people in the hospital who do not have potential
reasons to be in the hospital. Some patients were initially admitted under the terms and
conditions of MHA however, their extended period of stay in the hospital ended the tenure of
the MHA (National Health Service (NHS) News 2012). While others were admitted as an
informal basis and then gradually became sectioned. Thus, it can be said that there are mis-
appropriate application of MHA in WVH.
Another strong act in this domain is the Mental Capacity Act of 2005 (MCA). MCA
is designed to protect the vulnerable individuals and thereby empowering individuals to lack
the mental capacity like the people who are suffering from autism, dementia, brain injury and
other complex mental health complications. The act is applicable for the people who are aged
16 and over. The principal disadvantage of the act is that if a person is at risk or in danger to
the society, they will be treated appropriately or might be sectioned against his or her will
leading to hamper in the autonomy. The same instant occurred in the WVH where rules are
not abided systematically in order to re-evaluate the patient’s state of safety.
Conclusion
Thus from the above discussion, it can be concluded that there are several legislation
and policies in order to protect the rights and the safety of the people who are vulnerable to
the mental and the physical abuse. The analysis of these laws in relation to the case study of
the WVH highlighted that there are gaps in the implementation of the law in WVH
organizations like Safeguarding Vulnerable Group Act [SVGA] (2006) and Protection of
Vulnerable Adults Scheme (POVA). These gaps in the implementation of the law lead to
unwanted outcome of the residents of WVH.
11
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task: 2.2: Report: Explain how key professionals are involved in the protection of
individuals and groups vulnerable to abuse
Introduction
The Care Act (2014) sets standards for the statutory responsibility for the proper
integration of support and care between the health and the local care authorities in order to
protect the people who are vulnerable to mental or physical abuse. The entire work process is
guided by the NHS England and the Clinical Commissioning Groups. The following report
aims to analyze the key professionals who are involved in protecting the individuals or group
of individuals, vulnerable to abuse (NHS England 2014).
Discussion
The key professionals who are involved in giving protection to the individuals and
groups who are vulnerable to abuse include social and healthcare commissioners, clinicians
and social workers, police and the criminal justice system, service and professional
regulators, specialist safeguarding staff, social and healthcare providers and safe guarding
adult board members (Care Quality Commission 2014).
The role of the clinicians applies clinical governance standards in order to execute
conduct, care and treatment along with proper sharing of the information. The role of the
clinicians also deals with reporting of the incidence of the abuse of neglect or undignified
treatment while leading support and enquiries to neglect (Care Quality Commission 2014).
However, case study of Winterbourne View Hospital (WVH) highlighted that there is lack of
proper reporting of the cases where mental health patients were forcefully restrained.
Moreover, there were evidences, which suggest inappropriate prescribing of the antipsychotic
drugs. The serious case review, also highlighted that the health of the residents of WVH is
poor with the majority of the individuals are affected with preventable healthcare conditions
like constipation and dental problems (National Health Service (NHS) News 2012). The role
of social workers or the care managers is to identify and respond to the concerns of the
people who are vulnerable to physical or mental abuse and act as their representatives in
order to report their concerns. Their duty also deals with managing safeguarding risks and
benefits into planning care with people. They also review the care plan (Care Quality
Commission 2014). WVH shows that they do not have any care plans as the residents out
there are forcefully given medications. Specialist safeguarding staffs provide specialist advice
and co-ordination and responds to the concerns of the vulnerable group of individuals. The
case study of WVH showed that the concerns of the residents went mainly unheard as there
was an incidence where a patient was restrained for 45 times during the tenure of five months
(National Health Service (NHS) News 2012).
Police also has the role of key stakeholder in the protection of the vulnerable
population. Their role is to investigate possible crimes via conducting joint investigations.
The role of the police also deals with gathering best possible evidence in order to increase the
prospects for the prosecuting offenders (Care Quality Commission 2014).
Conclusion
SAFEGUARDING IN HEALTH AND SOCIAL CARE
Task: 2.2: Report: Explain how key professionals are involved in the protection of
individuals and groups vulnerable to abuse
Introduction
The Care Act (2014) sets standards for the statutory responsibility for the proper
integration of support and care between the health and the local care authorities in order to
protect the people who are vulnerable to mental or physical abuse. The entire work process is
guided by the NHS England and the Clinical Commissioning Groups. The following report
aims to analyze the key professionals who are involved in protecting the individuals or group
of individuals, vulnerable to abuse (NHS England 2014).
Discussion
The key professionals who are involved in giving protection to the individuals and
groups who are vulnerable to abuse include social and healthcare commissioners, clinicians
and social workers, police and the criminal justice system, service and professional
regulators, specialist safeguarding staff, social and healthcare providers and safe guarding
adult board members (Care Quality Commission 2014).
The role of the clinicians applies clinical governance standards in order to execute
conduct, care and treatment along with proper sharing of the information. The role of the
clinicians also deals with reporting of the incidence of the abuse of neglect or undignified
treatment while leading support and enquiries to neglect (Care Quality Commission 2014).
However, case study of Winterbourne View Hospital (WVH) highlighted that there is lack of
proper reporting of the cases where mental health patients were forcefully restrained.
Moreover, there were evidences, which suggest inappropriate prescribing of the antipsychotic
drugs. The serious case review, also highlighted that the health of the residents of WVH is
poor with the majority of the individuals are affected with preventable healthcare conditions
like constipation and dental problems (National Health Service (NHS) News 2012). The role
of social workers or the care managers is to identify and respond to the concerns of the
people who are vulnerable to physical or mental abuse and act as their representatives in
order to report their concerns. Their duty also deals with managing safeguarding risks and
benefits into planning care with people. They also review the care plan (Care Quality
Commission 2014). WVH shows that they do not have any care plans as the residents out
there are forcefully given medications. Specialist safeguarding staffs provide specialist advice
and co-ordination and responds to the concerns of the vulnerable group of individuals. The
case study of WVH showed that the concerns of the residents went mainly unheard as there
was an incidence where a patient was restrained for 45 times during the tenure of five months
(National Health Service (NHS) News 2012).
Police also has the role of key stakeholder in the protection of the vulnerable
population. Their role is to investigate possible crimes via conducting joint investigations.
The role of the police also deals with gathering best possible evidence in order to increase the
prospects for the prosecuting offenders (Care Quality Commission 2014).
Conclusion
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 27
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.