University Program Evaluation: SHOW Program for Health Outcomes
VerifiedAdded on 2022/10/14
|12
|2968
|350
Report
AI Summary
This report presents a comprehensive evaluation of the Strengthening Health Outcomes for Women and Children (SHOW) program, a global initiative aimed at reducing poverty and improving health outcomes for women, adolescent girls, and children. The program, with a budget of CAD$65M over 4.5 years, targets vulnerable communities in Bangladesh, Ghana, Haiti, Nigeria, and Senegal. The report details the program's objectives, including improving healthcare access and quality, and outlines its collaborative strategy involving Plan International, Ministries of Health, and local NGOs. The evaluation employs a mixed-methods approach, incorporating literature reviews, stakeholder analysis, and a randomized control trial design for data collection. Quantitative data analysis utilizes MS-Excel, while qualitative data is analyzed using QDA software to assess program progress and make recommendations for improvement. The report also includes a detailed timeline for the evaluation process, spanning six months, and emphasizes the importance of addressing socio-cultural barriers and gender inequalities to enhance the program's effectiveness. The evaluation aims to determine the success rate of the program, assess its impact on the target population, and provide evidence-based recommendations for sustained improvement.
Running head: PROGRAM EVALUATION
PROGRAM EVALUATION:
Global Consultant for Final Evaluation
Strengthening Health Outcomes of Women and Children
Name of the Student
Name of the University
Author Note
PROGRAM EVALUATION:
Global Consultant for Final Evaluation
Strengthening Health Outcomes of Women and Children
Name of the Student
Name of the University
Author Note
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1
PROGRAM EVALUATION
Table of Contents
1.0 Description.................................................................................................................................2
2.0 Literature Review......................................................................................................................3
3.0 Evaluation Strategy....................................................................................................................5
3.1 Evaluation objective..............................................................................................................5
3.2 Evaluation Question...............................................................................................................5
3.3 Objective rationale.................................................................................................................5
3.4 Evaluation design...................................................................................................................6
3.5 Rationale................................................................................................................................6
4.0 Timeline for the Program...........................................................................................................8
References........................................................................................................................................9
Appendix........................................................................................................................................11
Table 1: Gantt chart...................................................................................................................11
PROGRAM EVALUATION
Table of Contents
1.0 Description.................................................................................................................................2
2.0 Literature Review......................................................................................................................3
3.0 Evaluation Strategy....................................................................................................................5
3.1 Evaluation objective..............................................................................................................5
3.2 Evaluation Question...............................................................................................................5
3.3 Objective rationale.................................................................................................................5
3.4 Evaluation design...................................................................................................................6
3.5 Rationale................................................................................................................................6
4.0 Timeline for the Program...........................................................................................................8
References........................................................................................................................................9
Appendix........................................................................................................................................11
Table 1: Gantt chart...................................................................................................................11
2
PROGRAM EVALUATION
1.0 Description
Strengthening Health Outcomes for Women and Children (SHOW) is a program that
focuses on the reduction of the poverty including child and maternal mortality rate among the
vulnerable communities around the world. In order to carry forward this project the budget has
been allocated was CAD$65M and the projected time for this program was 4.5 years in total. The
target population for the program is children, adolescent girls and vulnerable women of
reproductive age. The primary aim of SHOW is to develop quality, accessibility, utilization and
low cost care providence to women of reproductive age and children in order to sustain against
the poverty of these people. The target of this program was to improve care facility for
approximately 1,594,257 women of reproductive age which includes 330,563 adolescent girls
and 914,572 children included with 454,000 girls. The plan also focuses on involving 1,522,785
male population including 339,000 adolescent boys from vulnerable areas of Bangladesh, Ghana,
Haiti, Nigeria and Senegal.
The primary objectives of the program are as follows:
Health care access improvement for the women of reproductive age, adolescent girls,
newborns and children under 5 living in vulnerable areas.
Health care quality improvement for the women of reproductive age, adolescent girls,
newborns and children under 5 living in vulnerable areas.
Primary strategy of the program:
SHOW focuses on the collaborative strategy for the health promotion. The health
promotion would be conducted by Plan International Country Offices of Plan
International Canada and it has collaborated with Ministries of Health, Ministries of
Women’s Affairs/Gender and Local NGOs. It has also formed partnership with
PROGRAM EVALUATION
1.0 Description
Strengthening Health Outcomes for Women and Children (SHOW) is a program that
focuses on the reduction of the poverty including child and maternal mortality rate among the
vulnerable communities around the world. In order to carry forward this project the budget has
been allocated was CAD$65M and the projected time for this program was 4.5 years in total. The
target population for the program is children, adolescent girls and vulnerable women of
reproductive age. The primary aim of SHOW is to develop quality, accessibility, utilization and
low cost care providence to women of reproductive age and children in order to sustain against
the poverty of these people. The target of this program was to improve care facility for
approximately 1,594,257 women of reproductive age which includes 330,563 adolescent girls
and 914,572 children included with 454,000 girls. The plan also focuses on involving 1,522,785
male population including 339,000 adolescent boys from vulnerable areas of Bangladesh, Ghana,
Haiti, Nigeria and Senegal.
The primary objectives of the program are as follows:
Health care access improvement for the women of reproductive age, adolescent girls,
newborns and children under 5 living in vulnerable areas.
Health care quality improvement for the women of reproductive age, adolescent girls,
newborns and children under 5 living in vulnerable areas.
Primary strategy of the program:
SHOW focuses on the collaborative strategy for the health promotion. The health
promotion would be conducted by Plan International Country Offices of Plan
International Canada and it has collaborated with Ministries of Health, Ministries of
Women’s Affairs/Gender and Local NGOs. It has also formed partnership with
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3
PROGRAM EVALUATION
Promundo-US, Sick Children-Centre for Global Child Health, and adolescent-led research on
SRHR in Senegal and HPIC for the medicinal aid in this program.
2.0 Literature Review
According to Sialubanje et al. (2015), the maternity waiting homes (MWH) are aiming to
develop better and improved care providence. The facilities have been working on the skill based
development of the care facility. It has been stated that for the improvement of the care facility
and development of the health care access for the pregnant women is dependent on the beliefs of
them (Lori et al. 2013). The factor of the rural health care access development in Zambian
context has been evaluated in this study. The authors conducted 32 interviews of which 22 are in
health care facility with MWH and 10 without MWH. In this interview the authors explored the
aspects of that affect the MWH care facility development. The aspect of the belief of the
pregnant women and their decision of obtaining care from the MWH are the primary factors that
affect the care facility development for the prenatal and postnatal care for the vulnerable women
population of age 15 to 45. Based on the results of the study it has been found that the women
are accepting this skill based care facility. However, lack of decision-making by women, low
socioeconomic status, socio-cultural norms and prevalent gender inequalities produce the barrier
of utilising these services by the pregnant women (Gabrysch et al. 2011). Hence, the authors
concluded that the education development of women for decision making skill development and
also addressing the gender and cultural biases would be required as the intervention of these
issues (Sialubanje et al. 2014). In order to develop MWH facility properly, the above mentioned
ways should be considered for improvement of the maternal care.
Based on the views of Gao and Kelley (2019), United Nations has developed eight
Millennium Development Goals (MDG) on 2000 which focuses on the reduction of the poverty,
PROGRAM EVALUATION
Promundo-US, Sick Children-Centre for Global Child Health, and adolescent-led research on
SRHR in Senegal and HPIC for the medicinal aid in this program.
2.0 Literature Review
According to Sialubanje et al. (2015), the maternity waiting homes (MWH) are aiming to
develop better and improved care providence. The facilities have been working on the skill based
development of the care facility. It has been stated that for the improvement of the care facility
and development of the health care access for the pregnant women is dependent on the beliefs of
them (Lori et al. 2013). The factor of the rural health care access development in Zambian
context has been evaluated in this study. The authors conducted 32 interviews of which 22 are in
health care facility with MWH and 10 without MWH. In this interview the authors explored the
aspects of that affect the MWH care facility development. The aspect of the belief of the
pregnant women and their decision of obtaining care from the MWH are the primary factors that
affect the care facility development for the prenatal and postnatal care for the vulnerable women
population of age 15 to 45. Based on the results of the study it has been found that the women
are accepting this skill based care facility. However, lack of decision-making by women, low
socioeconomic status, socio-cultural norms and prevalent gender inequalities produce the barrier
of utilising these services by the pregnant women (Gabrysch et al. 2011). Hence, the authors
concluded that the education development of women for decision making skill development and
also addressing the gender and cultural biases would be required as the intervention of these
issues (Sialubanje et al. 2014). In order to develop MWH facility properly, the above mentioned
ways should be considered for improvement of the maternal care.
Based on the views of Gao and Kelley (2019), United Nations has developed eight
Millennium Development Goals (MDG) on 2000 which focuses on the reduction of the poverty,
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4
PROGRAM EVALUATION
disease and lack of education in rural areas. MDG also focuses on the reduction of maternal
mortality and providing quality care in the reproductive care process within 2015. However, it
has been seen that the MDG has not been able to address the aim close to the desired proportion.
Hence, it can be stated that the factor of the reducing the ill situation has not been addressed.
Thus the requirement of the proper planning and educating the people from the lower socio-
economic structure needed to be considered (Masters et al. 2013). Moreover, the authors have
used Geographic Information Systems (GIS) for understanding the situation and based on the
understanding they recommended the required changes for the condition. On this context they
have found that a not only rural area where the maternal care facility is remote but also in the
urban areas the care processes is comprised with disparity (Kitui, Lewis and Davey 2013).
Hence, the quality of care is hampered as well. The study also helped in the knowledge
development about the condition of the maternal care in the rural and urban areas of the
unprivileged and remote countries. On the other hand the context of the requirement of education
and other plans has also been highlighted by the study.
Michael, Hole and Pl (2016), highlighted that the US government has been developing
new strategies that addresses the aspect of the low income group care facility. It has been seen
that the factor of the health are disparities are the factors that affect the health outcome of the
people from the low socio-economic group. Hence, the Earned Income Tax Credit (EITC) has
been developed by the US government in order to provide repeated care to the unprivileged
socio-economic group. However, there are still some disparities present. Hence, the factor of the
care should be provided to the children with higher priority. The “StreetCred” is a program
which has been developed to provide the families of low socio-economic group to access the
EITC and also improved health care. EITC is one of the most effective antipoverty tool that
PROGRAM EVALUATION
disease and lack of education in rural areas. MDG also focuses on the reduction of maternal
mortality and providing quality care in the reproductive care process within 2015. However, it
has been seen that the MDG has not been able to address the aim close to the desired proportion.
Hence, it can be stated that the factor of the reducing the ill situation has not been addressed.
Thus the requirement of the proper planning and educating the people from the lower socio-
economic structure needed to be considered (Masters et al. 2013). Moreover, the authors have
used Geographic Information Systems (GIS) for understanding the situation and based on the
understanding they recommended the required changes for the condition. On this context they
have found that a not only rural area where the maternal care facility is remote but also in the
urban areas the care processes is comprised with disparity (Kitui, Lewis and Davey 2013).
Hence, the quality of care is hampered as well. The study also helped in the knowledge
development about the condition of the maternal care in the rural and urban areas of the
unprivileged and remote countries. On the other hand the context of the requirement of education
and other plans has also been highlighted by the study.
Michael, Hole and Pl (2016), highlighted that the US government has been developing
new strategies that addresses the aspect of the low income group care facility. It has been seen
that the factor of the health are disparities are the factors that affect the health outcome of the
people from the low socio-economic group. Hence, the Earned Income Tax Credit (EITC) has
been developed by the US government in order to provide repeated care to the unprivileged
socio-economic group. However, there are still some disparities present. Hence, the factor of the
care should be provided to the children with higher priority. The “StreetCred” is a program
which has been developed to provide the families of low socio-economic group to access the
EITC and also improved health care. EITC is one of the most effective antipoverty tool that
5
PROGRAM EVALUATION
would help in deriving $66 billion annual tax benefit and thus helps in providence of improved
care providence to the unprivileged pediatric subjects. Hence, the implementation of EITC is
important and the factor of the care process development for the lower socio-economic group is
required with higher consideration as the condition of the pediatric health is not good enough in
terms of the low amount of morbidity and mortality rate. Thus the requirement of the program
for the improvement of the condition is required.
3.0 Evaluation Strategy
3.1 Evaluation objective
To determine the direction of the program that is the success rate of the program.
To determine the percentage of the women of reproductive age and children has been
addressed up to the present timeframe of the program.
To recommend the adequate ways and plans for the development of the success of
SHOW and also effectively provide the evidence based process for the improvement of
the care process.
3.2 Evaluation Question
What is the condition of SHOW program for the improvement of the health outcome of
the women of reproductive age and children in the global and also in Canadian perspective?
3.3 Objective rationale
On the basis of the evaluation question and the objectives it can be stated that the
requirement of the evaluation is to determine the success rate of the program. The process of the
evaluation will seek the progress of SHOW and also recommend any kind of the changes would
be required. The factor of the SHOW should be evaluated based on the progress or the regression
of the condition among the target population.
PROGRAM EVALUATION
would help in deriving $66 billion annual tax benefit and thus helps in providence of improved
care providence to the unprivileged pediatric subjects. Hence, the implementation of EITC is
important and the factor of the care process development for the lower socio-economic group is
required with higher consideration as the condition of the pediatric health is not good enough in
terms of the low amount of morbidity and mortality rate. Thus the requirement of the program
for the improvement of the condition is required.
3.0 Evaluation Strategy
3.1 Evaluation objective
To determine the direction of the program that is the success rate of the program.
To determine the percentage of the women of reproductive age and children has been
addressed up to the present timeframe of the program.
To recommend the adequate ways and plans for the development of the success of
SHOW and also effectively provide the evidence based process for the improvement of
the care process.
3.2 Evaluation Question
What is the condition of SHOW program for the improvement of the health outcome of
the women of reproductive age and children in the global and also in Canadian perspective?
3.3 Objective rationale
On the basis of the evaluation question and the objectives it can be stated that the
requirement of the evaluation is to determine the success rate of the program. The process of the
evaluation will seek the progress of SHOW and also recommend any kind of the changes would
be required. The factor of the SHOW should be evaluated based on the progress or the regression
of the condition among the target population.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6
PROGRAM EVALUATION
3.4 Evaluation design
The evaluation process would be dependent on the target selection and also obtaining the
knowledge about the condition of the health care system for the below poverty level women of
reproductive age and children. Hence, the nurses, government organization professionals
involved in the program, physicians, antenatal and postnatal care specialist, women of
reproductive age, adolescent girls and the children will be selected as the sample population. The
sampling method will be randomised that is the randomised control trial (Eldridge et al. 2016).
The selection of the sample population will be done randomly and the people will be randomly
assigned for the interview process. The method of the data collection will be mixed method as
the process will be done based on both the quantitative and qualitative method (Palinkas et al.
2015). Open ended and closed ended questionnaires will be used as the data collection tool.
Moreover, the process will be dependent on the Geographic Information Systems (GIS) as the
program is targeting global population especially Bangladesh, Ghana, Haiti, Nigeria and
Senegal. Collected data will be analysed based on the statistical process that is the statistical data
analysis process with the help of the MS-excel software and also the qualitative data analysis
process with the help of the QDA software.
3.5 Rationale
The evaluation program is dependent on different factors including the sample selection,
data collection and data analysis. Based on these data collection and analysis the
evaluation of the process can be done. The aspect of the sample selection here will be
random as SHOW has been conducted on a number of people from different areas of the
world and from different age group, different background. The factor of the randomised
control trial on the other hand provides the security of reducing biasness in the process
PROGRAM EVALUATION
3.4 Evaluation design
The evaluation process would be dependent on the target selection and also obtaining the
knowledge about the condition of the health care system for the below poverty level women of
reproductive age and children. Hence, the nurses, government organization professionals
involved in the program, physicians, antenatal and postnatal care specialist, women of
reproductive age, adolescent girls and the children will be selected as the sample population. The
sampling method will be randomised that is the randomised control trial (Eldridge et al. 2016).
The selection of the sample population will be done randomly and the people will be randomly
assigned for the interview process. The method of the data collection will be mixed method as
the process will be done based on both the quantitative and qualitative method (Palinkas et al.
2015). Open ended and closed ended questionnaires will be used as the data collection tool.
Moreover, the process will be dependent on the Geographic Information Systems (GIS) as the
program is targeting global population especially Bangladesh, Ghana, Haiti, Nigeria and
Senegal. Collected data will be analysed based on the statistical process that is the statistical data
analysis process with the help of the MS-excel software and also the qualitative data analysis
process with the help of the QDA software.
3.5 Rationale
The evaluation program is dependent on different factors including the sample selection,
data collection and data analysis. Based on these data collection and analysis the
evaluation of the process can be done. The aspect of the sample selection here will be
random as SHOW has been conducted on a number of people from different areas of the
world and from different age group, different background. The factor of the randomised
control trial on the other hand provides the security of reducing biasness in the process
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7
PROGRAM EVALUATION
(Eldridge et al. 2016). Hence, the random selection of the sample population will be
considered as the required process here.
The data collection process here is the mixed method which is the collective terminology
for the qualitative and quantitative method. In this process the target population will be
interviewed with an open ended questionnaire for the in-depth interview (Palinkas et al.
2015). The process of the qualitative interview will be conducted among the care
professionals (nurses, physicians, antenatal and postnatal care specialist), women of
reproductive age, adolescent girls and the children. Based on the detailed responses of the
participants the idea about the progress of the program will be obtained. Moreover, the
quantitative data collection will be done by the evaluation of the government data and the
reported data of the change of the condition for the program, SHOW. The close ended
questionnaire will be used to conduct the survey interview about the progress and the
changes after the program implementation will be done. The interview participants will
be the government organization professionals involved in the program, physicians,
antenatal and postnatal care specialist (Ramlo 2016).
After the data collected the quantitative data will be recorded and uploaded to the MS-
excel software for the analysis of the data and the result will be developed from the
analysis (Ramus et al. 2016). On the other hand the qualitative data will also be uploaded
to the QDA software for the qualitative data analysis (Sechelski and Onwuegbuzie 2019).
The qualitative data analysis result will deliver the idea about the context of the changes
and the feelings of the patients and the care professionals about this program.
Based on the analysis result the positive and negative aspects will be identified about the
program. Hence, recommendation for the positive changes will be developed as well.
PROGRAM EVALUATION
(Eldridge et al. 2016). Hence, the random selection of the sample population will be
considered as the required process here.
The data collection process here is the mixed method which is the collective terminology
for the qualitative and quantitative method. In this process the target population will be
interviewed with an open ended questionnaire for the in-depth interview (Palinkas et al.
2015). The process of the qualitative interview will be conducted among the care
professionals (nurses, physicians, antenatal and postnatal care specialist), women of
reproductive age, adolescent girls and the children. Based on the detailed responses of the
participants the idea about the progress of the program will be obtained. Moreover, the
quantitative data collection will be done by the evaluation of the government data and the
reported data of the change of the condition for the program, SHOW. The close ended
questionnaire will be used to conduct the survey interview about the progress and the
changes after the program implementation will be done. The interview participants will
be the government organization professionals involved in the program, physicians,
antenatal and postnatal care specialist (Ramlo 2016).
After the data collected the quantitative data will be recorded and uploaded to the MS-
excel software for the analysis of the data and the result will be developed from the
analysis (Ramus et al. 2016). On the other hand the qualitative data will also be uploaded
to the QDA software for the qualitative data analysis (Sechelski and Onwuegbuzie 2019).
The qualitative data analysis result will deliver the idea about the context of the changes
and the feelings of the patients and the care professionals about this program.
Based on the analysis result the positive and negative aspects will be identified about the
program. Hence, recommendation for the positive changes will be developed as well.
8
PROGRAM EVALUATION
4.0 Timeline for the Program
The evaluation program will be long process as the data collection from different region
will take a large amount of time. Moreover, the literature review process and the data analysis
process will take a certain amount of time. As per the program the timeframe will be as divided
in several stages such as the program background knowledge development, strategy
development, and literature review for the background knowledge of the issues and the effects of
the program, data collection, data analysis and result, conclusion, recommendation development.
Total time requirement for the evaluation program will be approximately six months or 24
weeks.
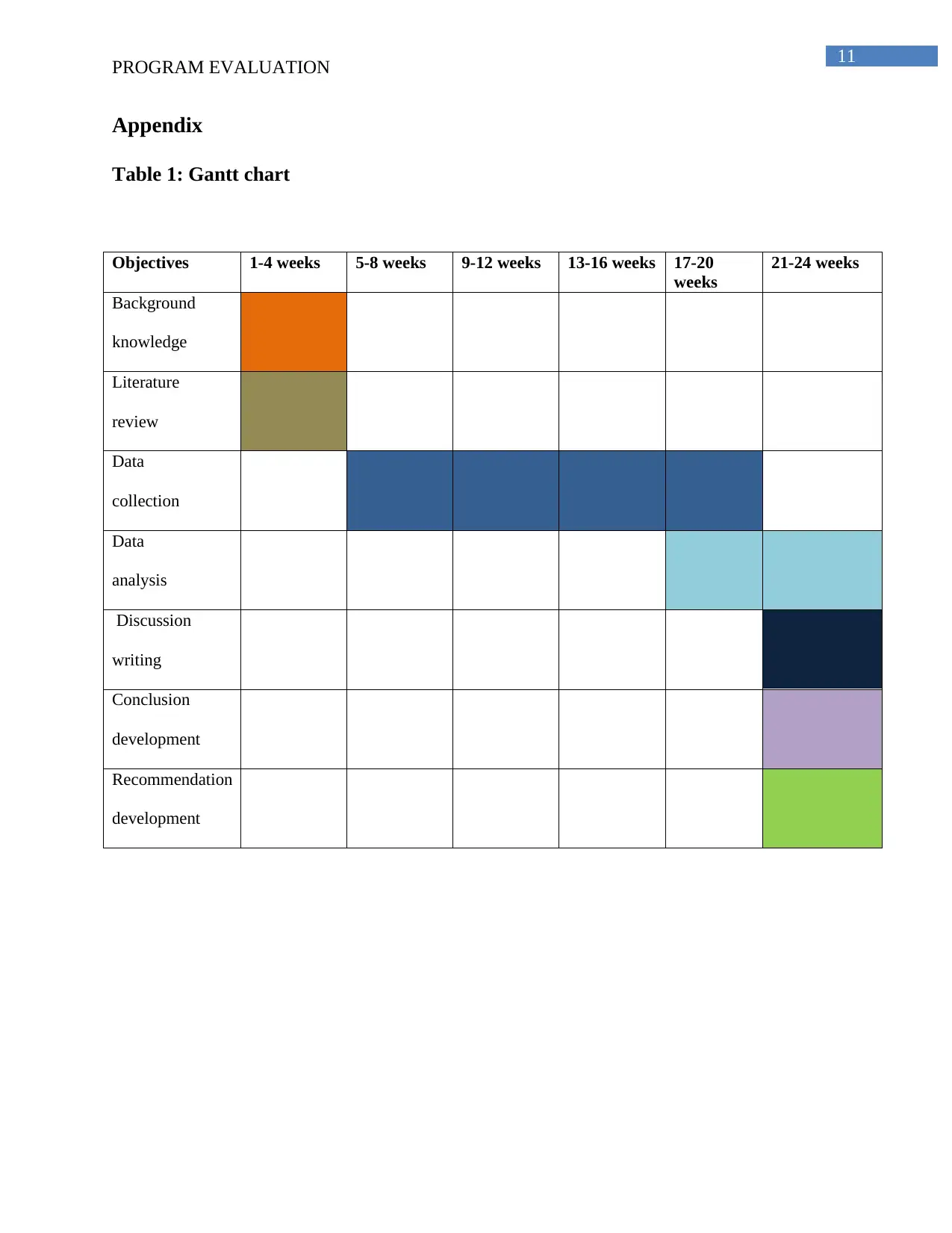
Firstly, the program selection and background knowledge development by the literature
review will take up to three weeks. Secondly, the data collection process will take up to fourteen
weeks as there are several travelling needs and also a large amount of sample will be required for
the data collection. Thirdly, the data analysis process will take approximately four weeks. Finally
the process of the result, conclusion and recommendation development will take up to three
weeks. (Refer to the appendix)
PROGRAM EVALUATION
4.0 Timeline for the Program
The evaluation program will be long process as the data collection from different region
will take a large amount of time. Moreover, the literature review process and the data analysis
process will take a certain amount of time. As per the program the timeframe will be as divided
in several stages such as the program background knowledge development, strategy
development, and literature review for the background knowledge of the issues and the effects of
the program, data collection, data analysis and result, conclusion, recommendation development.
Total time requirement for the evaluation program will be approximately six months or 24
weeks.
Firstly, the program selection and background knowledge development by the literature
review will take up to three weeks. Secondly, the data collection process will take up to fourteen
weeks as there are several travelling needs and also a large amount of sample will be required for
the data collection. Thirdly, the data analysis process will take approximately four weeks. Finally
the process of the result, conclusion and recommendation development will take up to three
weeks. (Refer to the appendix)
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9
PROGRAM EVALUATION
References
Eldridge, S.M., Lancaster, G.A., Campbell, M.J., Thabane, L., Hopewell, S., Coleman, C.L. and
Bond, C.M., 2016. Defining feasibility and pilot studies in preparation for randomised controlled
trials: development of a conceptual framework. PloS one, 11(3), p.e0150205.
Gabrysch, S., Cousens, S., Cox, J. and Campbell, O.M., 2011. The influence of distance and
level of care on delivery place in rural Zambia: a study of linked national data in a geographic
information system. PLoS medicine, 8(1), p.e1000394.
Gao, X. and Kelley, D.W., 2019. Understanding how distance to facility and quality of care
affect maternal health service utilization in Kenya and Haiti: A comparative geographic
information system study. Geospatial health, 14(1).
Kitui, J., Lewis S. and Davey, G., 2013. Factors influencing place of delivery for women in
Kenya: an analysis of the Kenya Demographic and Health Survey, 2008/2009. BMC Pregnancy
Childbirth 13:1-10.
Lori, J.R., Munro, M.L., Rominski, S., Williams, G., Dahn, B.T., Boyd, C.J., Moore, J.E. and
Gwenegale, W., 2013. Maternity waiting homes and traditional midwives in rural Liberia.
International Journal of Gynecology & Obstetrics, 123(2), pp.114-118.
Masters, S. H., Burstein, R., Amofah, G., Abaogye, P., Kumar, S. and Hanlon, M., 2013. Travel
time to maternity care and its effect on utilization in rural Ghana: A multilevel analysis. Social
Sci Med 93:147-54.
Michael, K., Hole, M.D. and Pl, D., 2016. Improving Access to Evidence-Based Antipoverty
Government Programs in the United States A Novel Primary Care Initiative.
Palinkas, L.A., Horwitz, S.M., Green, C.A., Wisdom, J.P., Duan, N. and Hoagwood, K., 2015.
Purposeful sampling for qualitative data collection and analysis in mixed method implementation
PROGRAM EVALUATION
References
Eldridge, S.M., Lancaster, G.A., Campbell, M.J., Thabane, L., Hopewell, S., Coleman, C.L. and
Bond, C.M., 2016. Defining feasibility and pilot studies in preparation for randomised controlled
trials: development of a conceptual framework. PloS one, 11(3), p.e0150205.
Gabrysch, S., Cousens, S., Cox, J. and Campbell, O.M., 2011. The influence of distance and
level of care on delivery place in rural Zambia: a study of linked national data in a geographic
information system. PLoS medicine, 8(1), p.e1000394.
Gao, X. and Kelley, D.W., 2019. Understanding how distance to facility and quality of care
affect maternal health service utilization in Kenya and Haiti: A comparative geographic
information system study. Geospatial health, 14(1).
Kitui, J., Lewis S. and Davey, G., 2013. Factors influencing place of delivery for women in
Kenya: an analysis of the Kenya Demographic and Health Survey, 2008/2009. BMC Pregnancy
Childbirth 13:1-10.
Lori, J.R., Munro, M.L., Rominski, S., Williams, G., Dahn, B.T., Boyd, C.J., Moore, J.E. and
Gwenegale, W., 2013. Maternity waiting homes and traditional midwives in rural Liberia.
International Journal of Gynecology & Obstetrics, 123(2), pp.114-118.
Masters, S. H., Burstein, R., Amofah, G., Abaogye, P., Kumar, S. and Hanlon, M., 2013. Travel
time to maternity care and its effect on utilization in rural Ghana: A multilevel analysis. Social
Sci Med 93:147-54.
Michael, K., Hole, M.D. and Pl, D., 2016. Improving Access to Evidence-Based Antipoverty
Government Programs in the United States A Novel Primary Care Initiative.
Palinkas, L.A., Horwitz, S.M., Green, C.A., Wisdom, J.P., Duan, N. and Hoagwood, K., 2015.
Purposeful sampling for qualitative data collection and analysis in mixed method implementation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10
PROGRAM EVALUATION
research. Administration and policy in mental health and mental health services research, 42(5),
pp.533-544.
Ramlo, S., 2016. Mixed method lessons learned from 80 years of Q methodology. Journal of
Mixed Methods Research, 10(1), pp.28-45.
Ramus, C., Hovasse, A., Marcellin, M., Hesse, A.M., Mouton-Barbosa, E., Bouyssié, D., Vaca,
S., Carapito, C., Chaoui, K., Bruley, C. and Garin, J., 2016. Spiked proteomic standard dataset
for testing label-free quantitative software and statistical methods. Data in brief, 6, pp.286-294.
Sechelski, A.N. and Onwuegbuzie, A.J., 2019. A Call for Enhancing Saturation at the Qualitative
Data Analysis Stage via the Use of Multiple Qualitative Data Analysis Approaches. The
Qualitative Report, 24(4), pp.795-821.
Sialubanje, C., Massar, K., Hamer, D.H. and Ruiter, R.A., 2014. Understanding the psychosocial
and environmental factors and barriers affecting utilization of maternal healthcare services in
Kalomo, Zambia: a qualitative study. Health education research, 29(3), pp.521-532.
Sialubanje, C., Massar, K., van der Pijl, M.S., Kirch, E.M., Hamer, D.H. and Ruiter, R.A., 2015.
Improving access to skilled facility-based delivery services: Women’s beliefs on facilitators and
barriers to the utilisation of maternity waiting homes in rural Zambia. Reproductive health,
12(1), p.61.
PROGRAM EVALUATION
research. Administration and policy in mental health and mental health services research, 42(5),
pp.533-544.
Ramlo, S., 2016. Mixed method lessons learned from 80 years of Q methodology. Journal of
Mixed Methods Research, 10(1), pp.28-45.
Ramus, C., Hovasse, A., Marcellin, M., Hesse, A.M., Mouton-Barbosa, E., Bouyssié, D., Vaca,
S., Carapito, C., Chaoui, K., Bruley, C. and Garin, J., 2016. Spiked proteomic standard dataset
for testing label-free quantitative software and statistical methods. Data in brief, 6, pp.286-294.
Sechelski, A.N. and Onwuegbuzie, A.J., 2019. A Call for Enhancing Saturation at the Qualitative
Data Analysis Stage via the Use of Multiple Qualitative Data Analysis Approaches. The
Qualitative Report, 24(4), pp.795-821.
Sialubanje, C., Massar, K., Hamer, D.H. and Ruiter, R.A., 2014. Understanding the psychosocial
and environmental factors and barriers affecting utilization of maternal healthcare services in
Kalomo, Zambia: a qualitative study. Health education research, 29(3), pp.521-532.
Sialubanje, C., Massar, K., van der Pijl, M.S., Kirch, E.M., Hamer, D.H. and Ruiter, R.A., 2015.
Improving access to skilled facility-based delivery services: Women’s beliefs on facilitators and
barriers to the utilisation of maternity waiting homes in rural Zambia. Reproductive health,
12(1), p.61.
11
PROGRAM EVALUATION
Appendix
Table 1: Gantt chart
Objectives 1-4 weeks 5-8 weeks 9-12 weeks 13-16 weeks 17-20
weeks
21-24 weeks
Background
knowledge
Literature
review
Data
collection
Data
analysis
Discussion
writing
Conclusion
development
Recommendation
development
PROGRAM EVALUATION
Appendix
Table 1: Gantt chart
Objectives 1-4 weeks 5-8 weeks 9-12 weeks 13-16 weeks 17-20
weeks
21-24 weeks
Background
knowledge
Literature
review
Data
collection
Data
analysis
Discussion
writing
Conclusion
development
Recommendation
development
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 12
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.