Assessment Task 1: Clinical Case Scenario Analysis - Slipped Disc
VerifiedAdded on 2023/03/20
|3
|1154
|98
Case Study
AI Summary
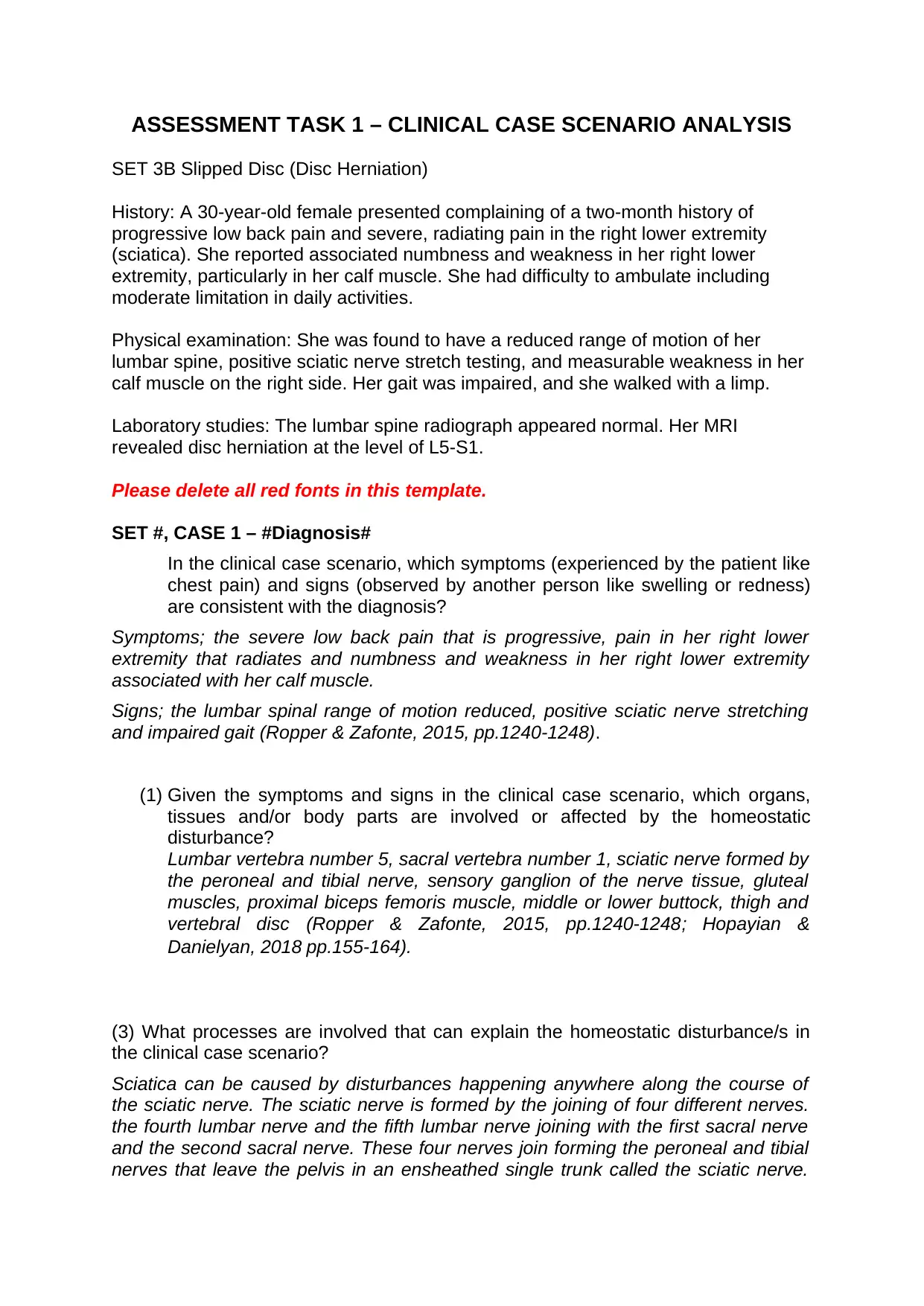
This assignment is a clinical case study analysis focusing on a 30-year-old female patient diagnosed with a slipped disc (disc herniation) at the L5-S1 level. The patient presented with a two-month history of progressive low back pain, radiating pain in the right lower extremity (sciatica), numbness, weakness in the right lower extremity, and difficulty ambulating. The physical examination revealed reduced lumbar spine range of motion, positive sciatic nerve stretch testing, and calf muscle weakness. The case study addresses the symptoms and signs consistent with the diagnosis, including the pain, numbness, weakness, and gait abnormalities. The assignment identifies the organs, tissues, and body parts involved, such as the lumbar and sacral vertebrae, sciatic nerve, and related muscles. Furthermore, it explores the processes underlying the homeostatic disturbance, including the mechanism of sciatica caused by nerve compression due to the disc herniation and related inflammatory responses. The analysis references several medical journals and textbooks to support the findings.


1 out of 3
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.