Safe Patient Handling and Mobility Program for Nurse MSDs Reduction
VerifiedAdded on 2020/01/07
|25
|9632
|262
Dissertation
AI Summary
This dissertation investigates the effectiveness of Safe Patient Handling and Mobility (SPHM) programs in reducing musculoskeletal disorders (MSDs) among nurses in direct care units. The study begins with an introduction highlighting the prevalence of workplace injuries among healthcare workers, particularly nurses, and the significant impact of lifting and moving patients on MSDs. A literature review examines existing research on the causes of MSDs, the benefits of SPHM programs, and the barriers to their implementation. The dissertation explores various search strategies and inclusion/exclusion criteria used in the literature review. The study also focuses on the importance of leadership and quality improvement in facilitating SPHM program implementation, including leadership theories and styles. It further outlines the steps involved in introducing an SPHM program, such as recognition, analysis, preparation, implementation, evaluation, and sustaining change. The research emphasizes the need for evidence-based practices and the use of patient handling equipment to reduce injuries, improve working conditions, and enhance nurse recruitment and retention. The conclusion and recommendations provide insights for improving local services and promoting the widespread adoption of SPHM programs to enhance nurse safety and patient care.
Dissertation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
TABLE OF CONTENTS
Safe patient Handling and Mobility program(SPHM) to reduce musculoskeletal
disorders (MSDs) injuries among nurses......................................................................3
Chapter 1 .......................................................................................................................3
1.1. Introduction.............................................................................................................3
1.2 Dissertation Aim.......................................................................................................5
Chapter 2........................................................................................................................6
Literature review ...........................................................................................................6
2.1 Literature Review (LR)............................................................................................6
2.2 Search strategies ......................................................................................................6
2.3 Safe patient handling and mobility(SPHM) program in control of Musculoskeletal
disorders (MSDs) injuries with nurses in work environment.........................................7
2.4. The barriers that avoid SPHM program from implementation.............................12
Conclusion....................................................................................................................14
Recommendation for local services improvement:......................................................14
Chapter 3......................................................................................................................15
Quality improvement (QI)............................................................................................15
3.1.The importance of leadership in facilitating improvements...................................15
3.2.Leadership in health care organisations.................................................................16
3.2. Leadership theories................................................................................................17
3.4. Leadership styles...................................................................................................17
3.5. Introducing SPHM program in local practice.......................................................19
Recognition..................................................................................................................19
Analysis........................................................................................................................20
Preparation....................................................................................................................20
Implementation.............................................................................................................21
Plan...............................................................................................................................21
Do.................................................................................................................................22
Study.............................................................................................................................23
Act................................................................................................................................23
Evaluating the Change..................................................................................................23
Sustaining the change...................................................................................................23
Barriers to implementation...........................................................................................24
Ethical consideration....................................................................................................24
Chapter 4 .....................................................................................................................24
4.1.Conclusion .............................................................................................................24
4.2.Recommendation....................................................................................................25
Safe patient Handling and Mobility program(SPHM) to reduce musculoskeletal
disorders (MSDs) injuries among nurses......................................................................3
Chapter 1 .......................................................................................................................3
1.1. Introduction.............................................................................................................3
1.2 Dissertation Aim.......................................................................................................5
Chapter 2........................................................................................................................6
Literature review ...........................................................................................................6
2.1 Literature Review (LR)............................................................................................6
2.2 Search strategies ......................................................................................................6
2.3 Safe patient handling and mobility(SPHM) program in control of Musculoskeletal
disorders (MSDs) injuries with nurses in work environment.........................................7
2.4. The barriers that avoid SPHM program from implementation.............................12
Conclusion....................................................................................................................14
Recommendation for local services improvement:......................................................14
Chapter 3......................................................................................................................15
Quality improvement (QI)............................................................................................15
3.1.The importance of leadership in facilitating improvements...................................15
3.2.Leadership in health care organisations.................................................................16
3.2. Leadership theories................................................................................................17
3.4. Leadership styles...................................................................................................17
3.5. Introducing SPHM program in local practice.......................................................19
Recognition..................................................................................................................19
Analysis........................................................................................................................20
Preparation....................................................................................................................20
Implementation.............................................................................................................21
Plan...............................................................................................................................21
Do.................................................................................................................................22
Study.............................................................................................................................23
Act................................................................................................................................23
Evaluating the Change..................................................................................................23
Sustaining the change...................................................................................................23
Barriers to implementation...........................................................................................24
Ethical consideration....................................................................................................24
Chapter 4 .....................................................................................................................24
4.1.Conclusion .............................................................................................................24
4.2.Recommendation....................................................................................................25
SAFE PATIENT HANDLING AND MOBILITY PROGRAM
(SPHM) TO REDUCE MUSCULOSKELETAL DISORDERS
(MSDS) INJURIES AMONG NURSES
CHAPTER 1
1.1 INTRODUCTION
Safety of nurses in any health institution is an important part to achieve
maximum level of care and services along with continuity of work. Nowadays, many
health issues were raised in the nursing field that negatively affects influence of work
environment work on nurse’s health. Nurses and other healthcare workers face many
hazards in their work environment. Health care environment can be considered to be
the most hazardous. (The Facility Guidelines Institute, 2012). As it is shown by the
Bureau of Labour Statistics, (2012) healthcare and social assistance workers
experience the highest rate of non-fatal occupational injuries and diseases in
comparison to any other sector such as manufacturing and construction. For instance,
more than 600 injury cases per 10,000 full time workers (appendix1) in healthcare and
social sector (Bureau of Labour Statistics, 2012). In addition, according to one survey
drawn from 53 healthcare systems with roughly 1,000 hospitals in all 50 states,
patient handling injuries accounted for 25 percent of all workers’ injuries for the
healthcare industry in 2011 (OSHA, 2013).
The most common and frequent nursing activities are lifting, transferring and
repositioning. Various studies were referred to most of injuries in nursing work
environment that happened from lifting and moving of patients (Howard, 2010).
Lifting and moving patients is the major cause of injuries and musculoskeletal
disorders (MSDs) with nurses (Waters, 2007). Such tasks could result in micro
injuries to the spine (Waters, 2007). Various studies evident that repeated and forceful
movements during providing care and nursing activities could cause major injuries
and MSDs (Nelson and Baptiste, 2004). The nurses could not feel the effects of these
activities immediately but after period of time from practicing such tasks this micro
injuries lead to debilitating injuries (Howard, 2010). As statistics shown by American
Nurses Association (ANA) survey (2011), 62% of nurses reported “developing
MSDs”, 56% of nurses say that they have experienced musculoskeletal pain that
became worse by their job and 80% of nurses reported pain due to MSDs report work
despite experiencing frequent pain. In the UK, back pain and MSDs account for
(SPHM) TO REDUCE MUSCULOSKELETAL DISORDERS
(MSDS) INJURIES AMONG NURSES
CHAPTER 1
1.1 INTRODUCTION
Safety of nurses in any health institution is an important part to achieve
maximum level of care and services along with continuity of work. Nowadays, many
health issues were raised in the nursing field that negatively affects influence of work
environment work on nurse’s health. Nurses and other healthcare workers face many
hazards in their work environment. Health care environment can be considered to be
the most hazardous. (The Facility Guidelines Institute, 2012). As it is shown by the
Bureau of Labour Statistics, (2012) healthcare and social assistance workers
experience the highest rate of non-fatal occupational injuries and diseases in
comparison to any other sector such as manufacturing and construction. For instance,
more than 600 injury cases per 10,000 full time workers (appendix1) in healthcare and
social sector (Bureau of Labour Statistics, 2012). In addition, according to one survey
drawn from 53 healthcare systems with roughly 1,000 hospitals in all 50 states,
patient handling injuries accounted for 25 percent of all workers’ injuries for the
healthcare industry in 2011 (OSHA, 2013).
The most common and frequent nursing activities are lifting, transferring and
repositioning. Various studies were referred to most of injuries in nursing work
environment that happened from lifting and moving of patients (Howard, 2010).
Lifting and moving patients is the major cause of injuries and musculoskeletal
disorders (MSDs) with nurses (Waters, 2007). Such tasks could result in micro
injuries to the spine (Waters, 2007). Various studies evident that repeated and forceful
movements during providing care and nursing activities could cause major injuries
and MSDs (Nelson and Baptiste, 2004). The nurses could not feel the effects of these
activities immediately but after period of time from practicing such tasks this micro
injuries lead to debilitating injuries (Howard, 2010). As statistics shown by American
Nurses Association (ANA) survey (2011), 62% of nurses reported “developing
MSDs”, 56% of nurses say that they have experienced musculoskeletal pain that
became worse by their job and 80% of nurses reported pain due to MSDs report work
despite experiencing frequent pain. In the UK, back pain and MSDs account for
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
approximately 40 per cent of all occupational ill health (National Health Services
(NHS), 2009).
MSDs can be defined as pain in the affected body region (e.g., back or neck)
for a specified duration or frequency (Bernard, 1997) along with other related
symptoms such as numbness and tingling (Jonsson, et al., 1987). Measurement of
MSDs vary from study to study. Many studies were using different ways of
measurement such as self-report and others requiring care or obtaining testing or
diagnosis by a physician. Hoogendoorn and colleagues (1999) observed the health
care workers through video and questionnaires during 3-year. They found that over
exhausted and forceful movement and lifting had a strong influence on the worker’s
low-back pain.
As per the above finding, it is vital to establish program that aimed to reduce
the rapid raise in nursing MSDs injuries related to handling and mobility of patients in
the work environment. Since decades, many health organisations and institutions were
establishing policies and regulations in order to ensure and manage Health and Safety
for nurses Working. For example, in UK, the Health and Safety at Work Act (1974)
was established regulation related to Management of Health and Safety at Work
Regulations and Workplace (Health, Safety and Welfare) Regulations (NHS, 2009).
Traditional strategies were used to reduce the MSDs injuries such as (1) sessions in
body mechanics, (2) training in safe lifting techniques and (3) back belts. In fact, the
above strategies are based on tradition rather then on scientific evidences (Nelson and
Baptiste, 2004, Hignett. et al., 2003, Ignatavicius & Workman, 2013). Nowadays,
many evidence-based practice strategies were implemented such as; (1) patient
handling by equipment/devices, (2) no-lift policies, (3) training on proper use of
patient handling equipment/devices and (4) patient lift teams. According to the
Occupational Safety and Health Administration (OSHA), “almost all successful
injuries and illness prevention programs include six core elements which are (1)
management leadership, (2) employee participation, (3) hazard identification and
assessment, (4) hazard prevention and control, (5) education and training, and (6)
system evaluation and improvement” (OSHA, 2014).
Moreover, The Nurse and Health Care Worker Protection Act of (2013) was
established program that aimed to decrease incidence of injuries of health care
workers (H.R.2480-113th Congress, 2013-2014). One aim of this program was to
eliminate the manual lifting of patients by direct care staff (Nurse). In addition, the
(NHS), 2009).
MSDs can be defined as pain in the affected body region (e.g., back or neck)
for a specified duration or frequency (Bernard, 1997) along with other related
symptoms such as numbness and tingling (Jonsson, et al., 1987). Measurement of
MSDs vary from study to study. Many studies were using different ways of
measurement such as self-report and others requiring care or obtaining testing or
diagnosis by a physician. Hoogendoorn and colleagues (1999) observed the health
care workers through video and questionnaires during 3-year. They found that over
exhausted and forceful movement and lifting had a strong influence on the worker’s
low-back pain.
As per the above finding, it is vital to establish program that aimed to reduce
the rapid raise in nursing MSDs injuries related to handling and mobility of patients in
the work environment. Since decades, many health organisations and institutions were
establishing policies and regulations in order to ensure and manage Health and Safety
for nurses Working. For example, in UK, the Health and Safety at Work Act (1974)
was established regulation related to Management of Health and Safety at Work
Regulations and Workplace (Health, Safety and Welfare) Regulations (NHS, 2009).
Traditional strategies were used to reduce the MSDs injuries such as (1) sessions in
body mechanics, (2) training in safe lifting techniques and (3) back belts. In fact, the
above strategies are based on tradition rather then on scientific evidences (Nelson and
Baptiste, 2004, Hignett. et al., 2003, Ignatavicius & Workman, 2013). Nowadays,
many evidence-based practice strategies were implemented such as; (1) patient
handling by equipment/devices, (2) no-lift policies, (3) training on proper use of
patient handling equipment/devices and (4) patient lift teams. According to the
Occupational Safety and Health Administration (OSHA), “almost all successful
injuries and illness prevention programs include six core elements which are (1)
management leadership, (2) employee participation, (3) hazard identification and
assessment, (4) hazard prevention and control, (5) education and training, and (6)
system evaluation and improvement” (OSHA, 2014).
Moreover, The Nurse and Health Care Worker Protection Act of (2013) was
established program that aimed to decrease incidence of injuries of health care
workers (H.R.2480-113th Congress, 2013-2014). One aim of this program was to
eliminate the manual lifting of patients by direct care staff (Nurse). In addition, the
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
program was encouraged to use of handling equipment; the percentage exposure to
lifting injuries was reduced up to 95%. Using of lifting equipment provide extra
benefits on health and safety of workers such as more satisfying working
environment; improved nursing recruitment and retention as well as reduced costs
associated with injuries.
As a result, evidence-based research has approved the success of program
where the rate of injuries among health workers decreased (OSHA, 2014).
1.2 Dissertation AimPresent dissertation has been evaluating the
effectiveness Safe Patient Handling and mobility (SPHM)
program to reduce MSDs with nurses in direct care units.
Additional aim for this dissertation is to promote the use of
SPHM program in local hospital to prevent health worker’s
(nurses) MSDs injuries as nurses are forefront of health care
delivering.
The next chapter is based on relevant literature review (LR) on requirement of
SPHM program for nurses to reduce MSDs injuries.
CHAPTER 2
LITERATURE REVIEW
2.1 Literature Review (LR)
This chapter is used for the purpose of carrying out research study in a
systematic manner and it is basically related to collecting data as per the subject
matter (Rees, 2011). It is also the most significant section of research study in which
researcher accesses papers, research articles and journals. This section also includes
review of secondary sources for the purpose of specifying suitability of topics.
2.2 Search strategies
Search strategy has been identified after selecting the aim of dissertation;
hence, operation plan is made accordingly. These strategies are used for the purpose
of searching content for study. Further, it is a process that starts from actual searching
and browsing of the collection of data. Different search terms are being used for the
study so that suitable data can be collected. Various key words are being used along
with unique strategies which would also work in electronic database and manual
lifting injuries was reduced up to 95%. Using of lifting equipment provide extra
benefits on health and safety of workers such as more satisfying working
environment; improved nursing recruitment and retention as well as reduced costs
associated with injuries.
As a result, evidence-based research has approved the success of program
where the rate of injuries among health workers decreased (OSHA, 2014).
1.2 Dissertation AimPresent dissertation has been evaluating the
effectiveness Safe Patient Handling and mobility (SPHM)
program to reduce MSDs with nurses in direct care units.
Additional aim for this dissertation is to promote the use of
SPHM program in local hospital to prevent health worker’s
(nurses) MSDs injuries as nurses are forefront of health care
delivering.
The next chapter is based on relevant literature review (LR) on requirement of
SPHM program for nurses to reduce MSDs injuries.
CHAPTER 2
LITERATURE REVIEW
2.1 Literature Review (LR)
This chapter is used for the purpose of carrying out research study in a
systematic manner and it is basically related to collecting data as per the subject
matter (Rees, 2011). It is also the most significant section of research study in which
researcher accesses papers, research articles and journals. This section also includes
review of secondary sources for the purpose of specifying suitability of topics.
2.2 Search strategies
Search strategy has been identified after selecting the aim of dissertation;
hence, operation plan is made accordingly. These strategies are used for the purpose
of searching content for study. Further, it is a process that starts from actual searching
and browsing of the collection of data. Different search terms are being used for the
study so that suitable data can be collected. Various key words are being used along
with unique strategies which would also work in electronic database and manual
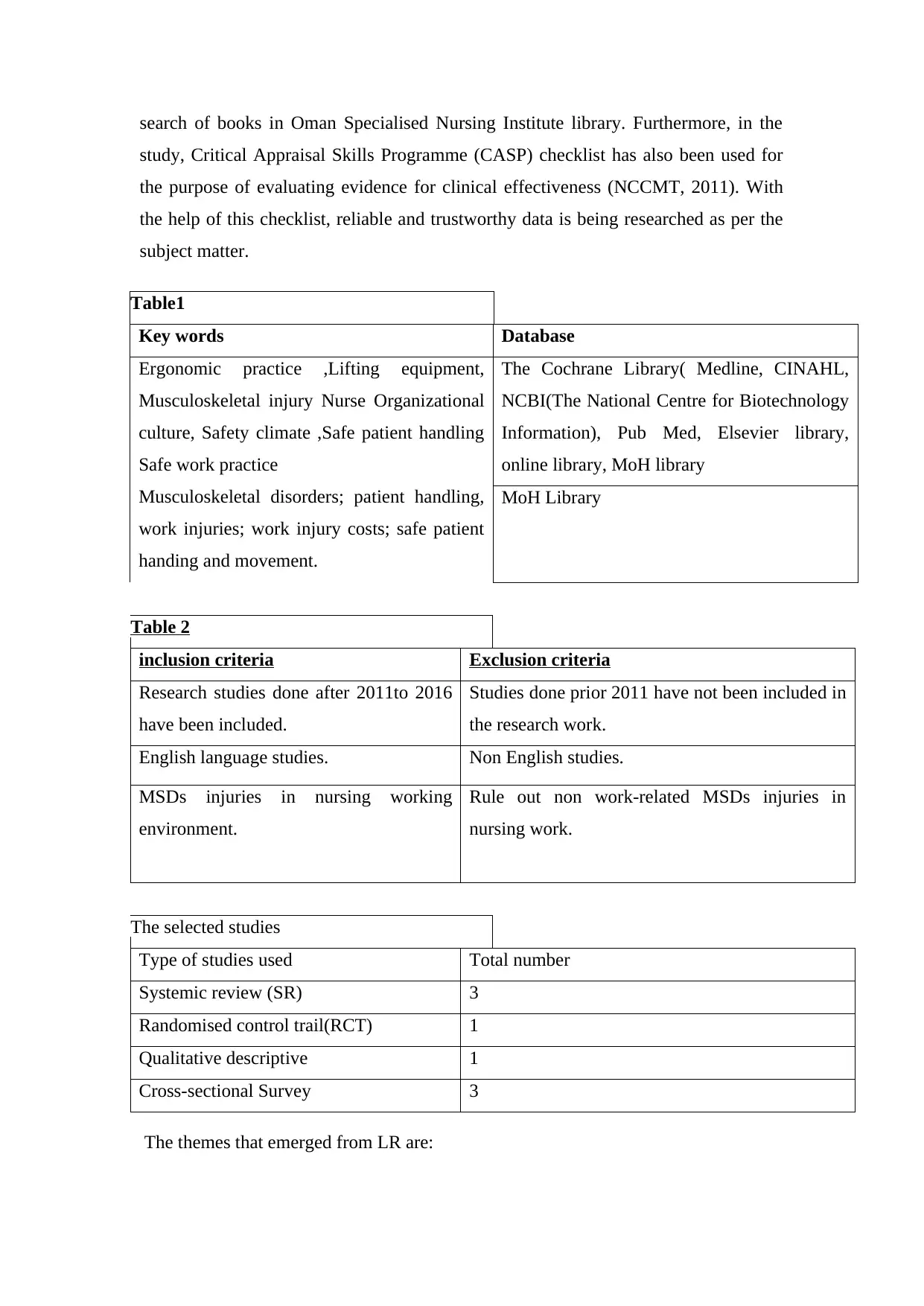
search of books in Oman Specialised Nursing Institute library. Furthermore, in the
study, Critical Appraisal Skills Programme (CASP) checklist has also been used for
the purpose of evaluating evidence for clinical effectiveness (NCCMT, 2011). With
the help of this checklist, reliable and trustworthy data is being researched as per the
subject matter.
Table1
Key words Database
Ergonomic practice ,Lifting equipment,
Musculoskeletal injury Nurse Organizational
culture, Safety climate ,Safe patient handling
Safe work practice
Musculoskeletal disorders; patient handling,
work injuries; work injury costs; safe patient
handing and movement.
The Cochrane Library( Medline, CINAHL,
NCBI(The National Centre for Biotechnology
Information), Pub Med, Elsevier library,
online library, MoH library
MoH Library
Table 2
inclusion criteria Exclusion criteria
Research studies done after 2011to 2016
have been included.
Studies done prior 2011 have not been included in
the research work.
English language studies. Non English studies.
MSDs injuries in nursing working
environment.
Rule out non work-related MSDs injuries in
nursing work.
The selected studies
Type of studies used Total number
Systemic review (SR) 3
Randomised control trail(RCT) 1
Qualitative descriptive 1
Cross-sectional Survey 3
The themes that emerged from LR are:
study, Critical Appraisal Skills Programme (CASP) checklist has also been used for
the purpose of evaluating evidence for clinical effectiveness (NCCMT, 2011). With
the help of this checklist, reliable and trustworthy data is being researched as per the
subject matter.
Table1
Key words Database
Ergonomic practice ,Lifting equipment,
Musculoskeletal injury Nurse Organizational
culture, Safety climate ,Safe patient handling
Safe work practice
Musculoskeletal disorders; patient handling,
work injuries; work injury costs; safe patient
handing and movement.
The Cochrane Library( Medline, CINAHL,
NCBI(The National Centre for Biotechnology
Information), Pub Med, Elsevier library,
online library, MoH library
MoH Library
Table 2
inclusion criteria Exclusion criteria
Research studies done after 2011to 2016
have been included.
Studies done prior 2011 have not been included in
the research work.
English language studies. Non English studies.
MSDs injuries in nursing working
environment.
Rule out non work-related MSDs injuries in
nursing work.
The selected studies
Type of studies used Total number
Systemic review (SR) 3
Randomised control trail(RCT) 1
Qualitative descriptive 1
Cross-sectional Survey 3
The themes that emerged from LR are:
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1- Safe patient handling and mobility program in control of MSDs injuries with
nurses in work environment.
2- The barriers that avoid SPHM program from implementation.
2.3 Safe patient handling and mobility (SPHM) program in control of musculoskeletal
disorders (MSDs) injuries with nurses in work environment
Based on the vital role of nurses in healthcare process; specific attention from
health institutions and organisations is needed to preserve them health and safety
when it is practised during duty. Wide range of literatures state that nurses are expose
to injuries in their environmental work. Next paragraph will review different
literatures regarding prevalence of MSDs injuries among nurses and proper preventive
interventions to reduce it.
Bos et al., 2007 conducted cross-sectional study which indicated the
prevalence of MSDs among healthcare workers (IC nurses, operation room nurses,
and X-ray technologists, and non-specialized nurses). Cross- sectional study can be
defined as ''collecting data at one point in time with no follow-up’’ (Fain, 2009, p25).
The sample consisted of 3,169 employees in eight university hospitals in the
Netherlands. The employees were asked whether they had low back or neck-
shoulder pain during the past year. The results have shown that four professional
groups had high rates of musculoskeletal complaints: low back 76% and neck-
shoulder 60%.
Similarly, Karahan et al. 2009 conducted cross-sectional survey which aimed
to study the prevalence of MSDs and risk factors amongst a variety of Turkish
hospital healthcare workers such as nurses, physicians, physical therapists,
technicians, secretaries and hospital aides. Questionnaires were distributed in Six
Turkish university hospitals. 1600 employees have completed it. 65·8% of
participants had reported low back pain. The highest rate of back pain recorded by
nurses was 77·1%.
Both studies i.e. Karahan et al. 2009 and Bos et al., 2007 analysed that there
are various causal factors that increase the potential to have MSDs injuries such as
working activities involving twisting, bending, heavy lifting, improper posture and
psychological stress.
Therefore, Karahan et al. 2009 and Bos et al., 2007 recommended specified
preventive interventions to be implemented for each healthcare worker especially
nurses in work environment.
2- The barriers that avoid SPHM program from implementation.
2.3 Safe patient handling and mobility (SPHM) program in control of musculoskeletal
disorders (MSDs) injuries with nurses in work environment
Based on the vital role of nurses in healthcare process; specific attention from
health institutions and organisations is needed to preserve them health and safety
when it is practised during duty. Wide range of literatures state that nurses are expose
to injuries in their environmental work. Next paragraph will review different
literatures regarding prevalence of MSDs injuries among nurses and proper preventive
interventions to reduce it.
Bos et al., 2007 conducted cross-sectional study which indicated the
prevalence of MSDs among healthcare workers (IC nurses, operation room nurses,
and X-ray technologists, and non-specialized nurses). Cross- sectional study can be
defined as ''collecting data at one point in time with no follow-up’’ (Fain, 2009, p25).
The sample consisted of 3,169 employees in eight university hospitals in the
Netherlands. The employees were asked whether they had low back or neck-
shoulder pain during the past year. The results have shown that four professional
groups had high rates of musculoskeletal complaints: low back 76% and neck-
shoulder 60%.
Similarly, Karahan et al. 2009 conducted cross-sectional survey which aimed
to study the prevalence of MSDs and risk factors amongst a variety of Turkish
hospital healthcare workers such as nurses, physicians, physical therapists,
technicians, secretaries and hospital aides. Questionnaires were distributed in Six
Turkish university hospitals. 1600 employees have completed it. 65·8% of
participants had reported low back pain. The highest rate of back pain recorded by
nurses was 77·1%.
Both studies i.e. Karahan et al. 2009 and Bos et al., 2007 analysed that there
are various causal factors that increase the potential to have MSDs injuries such as
working activities involving twisting, bending, heavy lifting, improper posture and
psychological stress.
Therefore, Karahan et al. 2009 and Bos et al., 2007 recommended specified
preventive interventions to be implemented for each healthcare worker especially
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
for nurses. For example, arranging proper rest periods, educational programmes to
teach the proper use of body mechanics handling devices and smoking cessation
programmes.
Wide range of literatures that examining effectiveness of Safe patient handling
and mobility (SPHM) program in order to decrease MSDs injuries with nurses.
Evaluating the effectiveness of SPHM program can be through three dimensions;
engineering (modifying suitable work environment through, layout, tools or
equipment used), administrative (modification of job rules and procedures and
financial support of training sessions and purchasing of handling and lifting
equipment) and behavioral (training of staff nurse in body mechanics, training in
proper use of lifting equipment/devices) controls (Kurowski et al.2017 , S.-J. Lee and
J.H. Lee, 2017).
Similarly, Van Bogaert et al. (2013), conducted cross-sectional survey to
explore the nursing practice environment had effect on job outcomes and Nursing care
quality. Questionnaire was used to collect data from 1201 nurses that have
participated in the survey. The survey examined the way in which work is structured
and organized to support nurse’s well-being and safety, team performance, safety and
quality of patient care. Researchers confirmed that leaders should involve staff nurses
on the process of decision-making regarding care process. Hence, nurses are the direct
care staff that interfere in patient’s care process. Moreover, this survey highlights
importance of optimising environment for the best nursing practice.
A systematic review (SR), was undertaken by I. Rivilis et al, 2008 to evaluate
the participatory ergonomic (PE) interventions/program for improving the health of
healthcare worker. PE can be defined as ‘the involvement of people in planning and
controlling of their own work activities with sufficient knowledge in order to achieve
required institute goals (’Wilson and Haines, 1997). SR is process that reviews
literatures with using specific criteria to focus on the important details of evidence
(Rees, 2011). However, it is not introducing new evidence in current clinical practice
being examined.
This SR studied 23 articles which met the required criteria from 1994-2002.
12 studies were classified as ‘medium’ or higher, it provided evidence that PE
program has a positive influence on: decreasing musculoskeletal symptoms, injuries
and reduction in absence days from work due to sickness. Six electronic databases
were searched i.e. Medline, Excerpta Medica database (EMBASE), Cumulative Index
teach the proper use of body mechanics handling devices and smoking cessation
programmes.
Wide range of literatures that examining effectiveness of Safe patient handling
and mobility (SPHM) program in order to decrease MSDs injuries with nurses.
Evaluating the effectiveness of SPHM program can be through three dimensions;
engineering (modifying suitable work environment through, layout, tools or
equipment used), administrative (modification of job rules and procedures and
financial support of training sessions and purchasing of handling and lifting
equipment) and behavioral (training of staff nurse in body mechanics, training in
proper use of lifting equipment/devices) controls (Kurowski et al.2017 , S.-J. Lee and
J.H. Lee, 2017).
Similarly, Van Bogaert et al. (2013), conducted cross-sectional survey to
explore the nursing practice environment had effect on job outcomes and Nursing care
quality. Questionnaire was used to collect data from 1201 nurses that have
participated in the survey. The survey examined the way in which work is structured
and organized to support nurse’s well-being and safety, team performance, safety and
quality of patient care. Researchers confirmed that leaders should involve staff nurses
on the process of decision-making regarding care process. Hence, nurses are the direct
care staff that interfere in patient’s care process. Moreover, this survey highlights
importance of optimising environment for the best nursing practice.
A systematic review (SR), was undertaken by I. Rivilis et al, 2008 to evaluate
the participatory ergonomic (PE) interventions/program for improving the health of
healthcare worker. PE can be defined as ‘the involvement of people in planning and
controlling of their own work activities with sufficient knowledge in order to achieve
required institute goals (’Wilson and Haines, 1997). SR is process that reviews
literatures with using specific criteria to focus on the important details of evidence
(Rees, 2011). However, it is not introducing new evidence in current clinical practice
being examined.
This SR studied 23 articles which met the required criteria from 1994-2002.
12 studies were classified as ‘medium’ or higher, it provided evidence that PE
program has a positive influence on: decreasing musculoskeletal symptoms, injuries
and reduction in absence days from work due to sickness. Six electronic databases
were searched i.e. Medline, Excerpta Medica database (EMBASE), Cumulative Index
to Nursing & Allied Health Literature (CINAHL), Canadian Centre for Occupational
Health and Safety (CCINFO web), Safety Science and Risk as well as Ergonomic
Abstracts. All these databases are considered as professional and are globally
accepted (Rees, 2011).
The main idea of applying this program is formation of an ergonomics team
(managers, health and safety personnel, research experts). Those people undergo
training to develop new knowledge to make improvements in the workplace (Wells et
al., 2004). These studies were monitoring the improvements in health outcomes by
examining process of implementation, changes in exposures and effects on health
outcomes after application of this program.
The most PE interventions were providing training sessions from 1 hour to 20
hour on technical tasks (Bohr, 2000; Carrivick et al., 2001; Evanoff et al., 1999;
Wickstro¨m et al., 1993, Ketola et al., 2002). Another intervention was
implementation of changes to the physical design of equipment and workplaces,
changes in work tasks as well as in formulation of policies (Carrivick et al., 2001;
Moore and Garg, 1998). Another study in this SR created a stretching and exercising
program or improving physical status of workers, maintaining procedures for used
equipment and designing new rooms for rest-breaks (Wickstro¨m et al., 1993,
Laitinen et al., 1997a, Halpern and Dawson, 1997, Evanoff et al., 1999).
The results have shown from 6 out of 12 studies that there is reduction of
MSDs symptoms. In addition, notice reduction of MSDs symptoms are record. As a
result of this, percentage of absence days related to MSDs symptoms was also
decrease.
Another SR was conducted by Jefferson (2010) where 99 articles were
reviewed and 23 articles only met the established criteria. The aim of this SR was to
determine the best interventions in a hospital setting that can reduce patient handling
injuries among healthcare workers. 9 out of 23 articles reflected decrease in injury’s
rate related to lifting patients among healthcare workers. Combination of articles has
shown that use of handling equipment had a great role in reducing the MS injuries
rate. The most studies pointed successful components of SPHM program
implementation are; educational training sessions and availability of handling
equipment's.
In contrast to I. Rivilis et al, (2008) findings related to ergonomic intervention
program made by H.J. Lim et al., (2011) have shown that handling injuries is the most
Health and Safety (CCINFO web), Safety Science and Risk as well as Ergonomic
Abstracts. All these databases are considered as professional and are globally
accepted (Rees, 2011).
The main idea of applying this program is formation of an ergonomics team
(managers, health and safety personnel, research experts). Those people undergo
training to develop new knowledge to make improvements in the workplace (Wells et
al., 2004). These studies were monitoring the improvements in health outcomes by
examining process of implementation, changes in exposures and effects on health
outcomes after application of this program.
The most PE interventions were providing training sessions from 1 hour to 20
hour on technical tasks (Bohr, 2000; Carrivick et al., 2001; Evanoff et al., 1999;
Wickstro¨m et al., 1993, Ketola et al., 2002). Another intervention was
implementation of changes to the physical design of equipment and workplaces,
changes in work tasks as well as in formulation of policies (Carrivick et al., 2001;
Moore and Garg, 1998). Another study in this SR created a stretching and exercising
program or improving physical status of workers, maintaining procedures for used
equipment and designing new rooms for rest-breaks (Wickstro¨m et al., 1993,
Laitinen et al., 1997a, Halpern and Dawson, 1997, Evanoff et al., 1999).
The results have shown from 6 out of 12 studies that there is reduction of
MSDs symptoms. In addition, notice reduction of MSDs symptoms are record. As a
result of this, percentage of absence days related to MSDs symptoms was also
decrease.
Another SR was conducted by Jefferson (2010) where 99 articles were
reviewed and 23 articles only met the established criteria. The aim of this SR was to
determine the best interventions in a hospital setting that can reduce patient handling
injuries among healthcare workers. 9 out of 23 articles reflected decrease in injury’s
rate related to lifting patients among healthcare workers. Combination of articles has
shown that use of handling equipment had a great role in reducing the MS injuries
rate. The most studies pointed successful components of SPHM program
implementation are; educational training sessions and availability of handling
equipment's.
In contrast to I. Rivilis et al, (2008) findings related to ergonomic intervention
program made by H.J. Lim et al., (2011) have shown that handling injuries is the most
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
common among healthcare workers especially nurses. Therefore, ergonomic
intervention program in SPHM is required to reduce the risk of MSDs injuries among
nurse’s personnel. This program encouraged to provide right handling equipment and
training of workers to develop effective practices for handling and lifting of patients.
The data were studied during 2 years pre-intervention and 2 years post-
intervention. The results indicated that intervention group had a 38.1% lower repeated
MSDs injury as compared to the control group (p=0.0005). In addition, sick leave and
time loss days were significantly decrease by 55% in the intervention hospitals (from
36 days to 16.2 days).
Kurowski et al, (2016) supported the previous study’s findings that MSDs
injury’s rate was reduced substantially within three years of beginning
implementation of SPHM program. 136 nursing homes with average annual
employment of 18,571 fulltime equivalents are included in the study over period of 8-
years. Large sample of study was used over long period of observation. Large sample
size increases the reliability and validity of study (Fain, 2013). Reliability examines
the accuracy of data collection method by applying various tests. Whereas, Validity
assesses the extent to which data assembled in research paper is what was proposed to
be collected and examined (Rees, 2011). The main interventions of the program were;
nurse’s training, purchase of mechanical transferring and mobility devices and
detailed maintenance protocols. As training is highly recommended for successful
implementation of SPHM program (Thomas and Thomas, 2014; Hodgson et al.,
2013); Massachusetts Department of Public Health Occupational Health Surveillance
Program, 2014). Results have shown the success of SPHM program and
improvements continued for six years after the SPHM program was implemented.
Randomised Control Trail (RCT) was conducted by Theis. et al, (2013) which
aimed to evaluate the effectiveness of SPHM program in reducing injury due to
patient lifting. RCT is considered as the most accepted research method to examine
and evaluate the intervention in large group sample (Fain, 2013). All those
participants were chosen randomly and did not receive any training sessions in SPHM
program. Randomization process in choosing the participants reduces risk of biasness
in the study (Grove. Et al, 2015). Bias refers to any factor that may affect the accuracy
of results in study (Rees, 2011). 55(98.2%) out of 56 participants (nurses) agreed to
participate in this study. The competency were examining by checklist (Staff Patient
Transfer Pre Competency Check-Off List); to examine the level of knowledge in safe
intervention program in SPHM is required to reduce the risk of MSDs injuries among
nurse’s personnel. This program encouraged to provide right handling equipment and
training of workers to develop effective practices for handling and lifting of patients.
The data were studied during 2 years pre-intervention and 2 years post-
intervention. The results indicated that intervention group had a 38.1% lower repeated
MSDs injury as compared to the control group (p=0.0005). In addition, sick leave and
time loss days were significantly decrease by 55% in the intervention hospitals (from
36 days to 16.2 days).
Kurowski et al, (2016) supported the previous study’s findings that MSDs
injury’s rate was reduced substantially within three years of beginning
implementation of SPHM program. 136 nursing homes with average annual
employment of 18,571 fulltime equivalents are included in the study over period of 8-
years. Large sample of study was used over long period of observation. Large sample
size increases the reliability and validity of study (Fain, 2013). Reliability examines
the accuracy of data collection method by applying various tests. Whereas, Validity
assesses the extent to which data assembled in research paper is what was proposed to
be collected and examined (Rees, 2011). The main interventions of the program were;
nurse’s training, purchase of mechanical transferring and mobility devices and
detailed maintenance protocols. As training is highly recommended for successful
implementation of SPHM program (Thomas and Thomas, 2014; Hodgson et al.,
2013); Massachusetts Department of Public Health Occupational Health Surveillance
Program, 2014). Results have shown the success of SPHM program and
improvements continued for six years after the SPHM program was implemented.
Randomised Control Trail (RCT) was conducted by Theis. et al, (2013) which
aimed to evaluate the effectiveness of SPHM program in reducing injury due to
patient lifting. RCT is considered as the most accepted research method to examine
and evaluate the intervention in large group sample (Fain, 2013). All those
participants were chosen randomly and did not receive any training sessions in SPHM
program. Randomization process in choosing the participants reduces risk of biasness
in the study (Grove. Et al, 2015). Bias refers to any factor that may affect the accuracy
of results in study (Rees, 2011). 55(98.2%) out of 56 participants (nurses) agreed to
participate in this study. The competency were examining by checklist (Staff Patient
Transfer Pre Competency Check-Off List); to examine the level of knowledge in safe
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
transferring of patients and evaluate who need additional training. This checklist
decreases the risk of bias and increases validity of information that was collected
(Fain, 2013). As a result of this, all participants received training sessions on SPHM
from October 2004 through June 2005. Researches were following the results of study
through three time periods (1) Baseline: 1/1/2002–9/31/2004, (2) Post Training:
7/1/2005–12/31/2006 and (3) Long Term: 1/1/2007–6/30/2009.
Results are being measured by putting expected and baseline results as shown
in Appendix 2. The number of nurse’s injuries were significantly reduced at post
training as compared with baseline data (p < .001). When measurement is equal or
less than 0.5 P, then value point to an accepted and notable result (Fain, 2013).
The above study recommended to continue training in SPHM to maintain low
MSDs injuries with nurses in environment work. When there is lack of training, then
it may return back the numbers of MSDs injuries to baseline.
Washington State Department (WSD) of Labour and Industries conducting a
5-year study after implementation of SPHM (2007) at Washington state Hospitals. All
the hospitals of SPHM are included in program by survey and interviewing of the
health worker staffs and administrative staffs about; training of direct care staff,
handling policies, procedures, handling devices purchasing and overall program
implementation through 2007, 2009 and 2011.
This program achieved a great success in reducing rate of MSDs injuries
among health workers. This is commonly known with the direct care staff is that ''no
SPH policy''. 20% of respondents reported either not having or not knowing if they
had a SPH policy. According to SPHM program implementation, the percent of '' No
SPH Policy'' decreased from 20% in 2007 to 3.6% in 2009. This refers to increase the
awareness and knowledge about written policies related to handling and transferring
patients. Moreover, the reporting rate of injuries related to transferring patient
increased from 2007 to 2009. This is due to increased knowledge about a committee
that discusses patient’s handling injuries of staff (p<.001). The staff has become more
aware and they do not accept musculoskeletal pain as “just part of the job”. Therefore,
the percentage of MS symptoms decreased as shown in appendix2. Additionally, the
respondents reported high proportions of using of SPH equipment in both 2007 and
2009. This results evident that the direct health worker (nurses) became capable to
handling equipment properly and effectively.
decreases the risk of bias and increases validity of information that was collected
(Fain, 2013). As a result of this, all participants received training sessions on SPHM
from October 2004 through June 2005. Researches were following the results of study
through three time periods (1) Baseline: 1/1/2002–9/31/2004, (2) Post Training:
7/1/2005–12/31/2006 and (3) Long Term: 1/1/2007–6/30/2009.
Results are being measured by putting expected and baseline results as shown
in Appendix 2. The number of nurse’s injuries were significantly reduced at post
training as compared with baseline data (p < .001). When measurement is equal or
less than 0.5 P, then value point to an accepted and notable result (Fain, 2013).
The above study recommended to continue training in SPHM to maintain low
MSDs injuries with nurses in environment work. When there is lack of training, then
it may return back the numbers of MSDs injuries to baseline.
Washington State Department (WSD) of Labour and Industries conducting a
5-year study after implementation of SPHM (2007) at Washington state Hospitals. All
the hospitals of SPHM are included in program by survey and interviewing of the
health worker staffs and administrative staffs about; training of direct care staff,
handling policies, procedures, handling devices purchasing and overall program
implementation through 2007, 2009 and 2011.
This program achieved a great success in reducing rate of MSDs injuries
among health workers. This is commonly known with the direct care staff is that ''no
SPH policy''. 20% of respondents reported either not having or not knowing if they
had a SPH policy. According to SPHM program implementation, the percent of '' No
SPH Policy'' decreased from 20% in 2007 to 3.6% in 2009. This refers to increase the
awareness and knowledge about written policies related to handling and transferring
patients. Moreover, the reporting rate of injuries related to transferring patient
increased from 2007 to 2009. This is due to increased knowledge about a committee
that discusses patient’s handling injuries of staff (p<.001). The staff has become more
aware and they do not accept musculoskeletal pain as “just part of the job”. Therefore,
the percentage of MS symptoms decreased as shown in appendix2. Additionally, the
respondents reported high proportions of using of SPH equipment in both 2007 and
2009. This results evident that the direct health worker (nurses) became capable to
handling equipment properly and effectively.
Overall, SPHM program intervention has been shown to be effective in
reducing MSDs injuries among nurses. Therefore, it is recommended for health
organisation to implement this program in the hospital. However, nurses and the
health organisation may face difficulties in implementing such intervention. The next
part of this chapter will discuss obstacles and barriers that they faced and solutions to
overcome the same.
2.4. Barriers that avoid SPHM program from implementation
Although the previous studies (I. Rivilis et al, 2008, Silverstein, 2011,
Kurowski et al., 2016, S.-J. Lee and J.H. Lee, 2017, Theis. et al, 2013,) confirmed the
efficacy of SPHM program in reduction of MSDs injuries among nurses. There are
various barriers and challenges that limit the aim of it. Most of the barriers avoid
SPHM program from implementation are related to people, education, time,
environment and equipment.
Regarding the environmental barriers; implementation of ergonomic
interventions require high efforts and resources (Rayan, 2011). The design and order
of rooms in hospital are not prepared for extra modification (Elnitsky,et .al, 2014).
Silverstein, (2011) stated that in the report of Washington State Hospital
Association’s Environmental Survey, most of the hospitals included in survey
reported that room sizes (66%) is the major challenge to apply this program as
compared to other factors. 30.5% of respondents reported that lifting equipment need
enough space storage which results in inaccessibility of lift devices. For example:
they were arranged in the end of the hall/room. Moreover, (30%) of respondents
pointed out the equipment size that limit the practicality of using it. Additionally, high
cost of handling and lifting equipment (17.5%) (Silverstein, 2011) will remain a
barrier due to lack of fund from the higher authority (Hallmark et al. 2015).
Secondly, shortage of staff (50%) and heavy workload has become the second
challenge in applying this program (Silverstein, 2011). SPHM program need
sufficient number of staff nurse’s recruitment to be implemented effectively. From the
side of patient, most of them want immediate mobility and the use of equipment
devices will take time (32%). Alamgir, et al. (2009) confirmed that transfers
performed manually required on average less time (bed to chair transfers: 156.9
seconds, by using assistance devices it will need, 273.6 seconds). So, healthcare
reducing MSDs injuries among nurses. Therefore, it is recommended for health
organisation to implement this program in the hospital. However, nurses and the
health organisation may face difficulties in implementing such intervention. The next
part of this chapter will discuss obstacles and barriers that they faced and solutions to
overcome the same.
2.4. Barriers that avoid SPHM program from implementation
Although the previous studies (I. Rivilis et al, 2008, Silverstein, 2011,
Kurowski et al., 2016, S.-J. Lee and J.H. Lee, 2017, Theis. et al, 2013,) confirmed the
efficacy of SPHM program in reduction of MSDs injuries among nurses. There are
various barriers and challenges that limit the aim of it. Most of the barriers avoid
SPHM program from implementation are related to people, education, time,
environment and equipment.
Regarding the environmental barriers; implementation of ergonomic
interventions require high efforts and resources (Rayan, 2011). The design and order
of rooms in hospital are not prepared for extra modification (Elnitsky,et .al, 2014).
Silverstein, (2011) stated that in the report of Washington State Hospital
Association’s Environmental Survey, most of the hospitals included in survey
reported that room sizes (66%) is the major challenge to apply this program as
compared to other factors. 30.5% of respondents reported that lifting equipment need
enough space storage which results in inaccessibility of lift devices. For example:
they were arranged in the end of the hall/room. Moreover, (30%) of respondents
pointed out the equipment size that limit the practicality of using it. Additionally, high
cost of handling and lifting equipment (17.5%) (Silverstein, 2011) will remain a
barrier due to lack of fund from the higher authority (Hallmark et al. 2015).
Secondly, shortage of staff (50%) and heavy workload has become the second
challenge in applying this program (Silverstein, 2011). SPHM program need
sufficient number of staff nurse’s recruitment to be implemented effectively. From the
side of patient, most of them want immediate mobility and the use of equipment
devices will take time (32%). Alamgir, et al. (2009) confirmed that transfers
performed manually required on average less time (bed to chair transfers: 156.9
seconds, by using assistance devices it will need, 273.6 seconds). So, healthcare
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 25
Related Documents






Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.