Health Equality Assessment Report: Stormlands Health Inequity Audit
VerifiedAdded on 2021/04/19
|16
|2854
|286
Report
AI Summary
This comprehensive health equality assessment report presents an audit of health inequities conducted in Stormlands, focusing on the distribution of health services and resources across 16 subzones. The report identifies key determinants of health inequalities, including socioeconomic disparities (education, income, and occupation), geographic location, gender-based inequalities, and lifestyle factors (smoking, nutrition, exercise). The audit reveals significant differences in health outcomes, risks, and service utilization across various demographic groups. It highlights the impact of socioeconomic status on health, the influence of geographical location on access to services and overall health, and the role of gender and lifestyle choices in shaping health outcomes. The report recommends the implementation of national indicators to monitor progress, assessment of primary care service distribution, and collaborative efforts between the NHS and local authorities to address health inequalities. The report underscores the need for targeted interventions, data-driven decision-making, and a multi-faceted approach to improve health equity within Stormlands.

Running head: HEALTH EQUALITY ASSESSMENT REPORT 1
Health Equality Assessment Report
Name
Institutional Affiliation
Health Equality Assessment Report
Name
Institutional Affiliation
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH EQUALITY ASSESSMENT REPORT 2
Table of Contents
Executive Summary.........................................................................................................................3
Introduction......................................................................................................................................4
Health Inequities..............................................................................................................................6
Socioeconomic Inequalities.........................................................................................................6
Geographic Place of Residence....................................................................................................8
Gender Health Inequalities.........................................................................................................10
Lifestyle Inequalities..................................................................................................................11
Recommendations..........................................................................................................................12
Conclusion.....................................................................................................................................13
Glossary.........................................................................................................................................14
References......................................................................................................................................15
Table of Contents
Executive Summary.........................................................................................................................3
Introduction......................................................................................................................................4
Health Inequities..............................................................................................................................6
Socioeconomic Inequalities.........................................................................................................6
Geographic Place of Residence....................................................................................................8
Gender Health Inequalities.........................................................................................................10
Lifestyle Inequalities..................................................................................................................11
Recommendations..........................................................................................................................12
Conclusion.....................................................................................................................................13
Glossary.........................................................................................................................................14
References......................................................................................................................................15
HEALTH EQUALITY ASSESSMENT REPORT 3
Health Equality Audit Report
Executive Summary
Health equality is a concept that draws from the idea that every individual should have
access to health services and attain complete health potential, and more significantly, no person
is disadvantaged from achieving this potential (VicHealth, 2004). Health inequalities had
probably not been the primary concern in the Department of Health. However, the country had
identified the importance of reducing the inequities in health; thus the government is currently
undertaking a commendable work through the Ministry of Public Health and National Health
Services (NHS. Therefore, we conducted an audit of health inequities in various local zones to
collect evidence of the state of the health inequities in the identified areas. The main aim of
health equality audit conducted was to find out how impartially the health services and other
health-related resources are distributed considering health requirements of different subzones and
people in Storm lands.
We must have a role in encouraging health equity in Victoria. Notwithstanding the
methods of measuring health, by means of usage, need, and accessibility of services or risk
factors or outcome, we find out that specific groups of people are always disadvantaged
regarding health. In the audit, we have found out that there is a healthy relationship between
socioeconomic and health. People in poor socioeconomic status in term of occupation, education,
income are more likely to experience poorer health than those who are slightly in a better
position of socioeconomically.
Handling these socioeconomic, cultural, age, gender, and geographical health inequalities
need a population health process that embraces impacts on the wellbeing as well as the approach
on the techniques that should be undertaken for the improvement of general wellbeing. The
principles of health equity must be adhered to in any kind of actions involved in with the aim that
Health Equality Audit Report
Executive Summary
Health equality is a concept that draws from the idea that every individual should have
access to health services and attain complete health potential, and more significantly, no person
is disadvantaged from achieving this potential (VicHealth, 2004). Health inequalities had
probably not been the primary concern in the Department of Health. However, the country had
identified the importance of reducing the inequities in health; thus the government is currently
undertaking a commendable work through the Ministry of Public Health and National Health
Services (NHS. Therefore, we conducted an audit of health inequities in various local zones to
collect evidence of the state of the health inequities in the identified areas. The main aim of
health equality audit conducted was to find out how impartially the health services and other
health-related resources are distributed considering health requirements of different subzones and
people in Storm lands.
We must have a role in encouraging health equity in Victoria. Notwithstanding the
methods of measuring health, by means of usage, need, and accessibility of services or risk
factors or outcome, we find out that specific groups of people are always disadvantaged
regarding health. In the audit, we have found out that there is a healthy relationship between
socioeconomic and health. People in poor socioeconomic status in term of occupation, education,
income are more likely to experience poorer health than those who are slightly in a better
position of socioeconomically.
Handling these socioeconomic, cultural, age, gender, and geographical health inequalities
need a population health process that embraces impacts on the wellbeing as well as the approach
on the techniques that should be undertaken for the improvement of general wellbeing. The
principles of health equity must be adhered to in any kind of actions involved in with the aim that
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH EQUALITY ASSESSMENT REPORT 4
those activities aid in reducing inequalities in health. The recommended framework for
intervention involves developing and executing approaches in four phases:
Structural: - In this phase, the causes of disparities in health such as social,
cultural, economic and historical aspects are tackled.
Intermediate paths: - Psychosocial, elemental or behavioral aspects which
facilitate the effect of a structural element on healthiness inequalities are put into
consideration.
Health and disability services: - Certain activities within disability services
and health are undertaken.
Impact: - The influence of incapacity and ailment on socioeconomic status
is minimized.
Besides, WHO (2017) encourages an inter-sectorial approach that necessitates a
particular line of action at different phases of policymaking. WHO (2017) works with the
Member States with the aim of building and sustaining their institutional and human capacities.
This enables health inequities to be solved through particular lines of action, comprising of
review of public health policies, facilitation, and training.
There are health policies that address gender, vulnerable groups, local level governance,
and subnational governance. These policies ensure that inequalities in health are reduced to bare
minimum if they are appropriately implemented. The systems will promote gender equity,
improve the health of vulnerable individuals, and strengthens local and subnational government.
Introduction
Health inequalities are widespread all over the world. This report provides a perfect
synthesis of the health inequality audit carried out in Stormlands that was divided into 16
subzones. According to HM Treasury (2002) about the Cross-Cutting Review on Health
those activities aid in reducing inequalities in health. The recommended framework for
intervention involves developing and executing approaches in four phases:
Structural: - In this phase, the causes of disparities in health such as social,
cultural, economic and historical aspects are tackled.
Intermediate paths: - Psychosocial, elemental or behavioral aspects which
facilitate the effect of a structural element on healthiness inequalities are put into
consideration.
Health and disability services: - Certain activities within disability services
and health are undertaken.
Impact: - The influence of incapacity and ailment on socioeconomic status
is minimized.
Besides, WHO (2017) encourages an inter-sectorial approach that necessitates a
particular line of action at different phases of policymaking. WHO (2017) works with the
Member States with the aim of building and sustaining their institutional and human capacities.
This enables health inequities to be solved through particular lines of action, comprising of
review of public health policies, facilitation, and training.
There are health policies that address gender, vulnerable groups, local level governance,
and subnational governance. These policies ensure that inequalities in health are reduced to bare
minimum if they are appropriately implemented. The systems will promote gender equity,
improve the health of vulnerable individuals, and strengthens local and subnational government.
Introduction
Health inequalities are widespread all over the world. This report provides a perfect
synthesis of the health inequality audit carried out in Stormlands that was divided into 16
subzones. According to HM Treasury (2002) about the Cross-Cutting Review on Health
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH EQUALITY ASSESSMENT REPORT 5
Inequalities, the obligations of the government were stipulated to minimize inequities in the
health sector and recognize that sustainable action on the broader contributing factors of health
inequities is necessitated if the generation cycle of poverty and health is to be shattered.
According to Graham (2002), national policy and strategy indicate a collection of clarifications
and interpretations of the meaning of tackling health inequities.
This report discusses four significant determinants of health inequities in Stormlands.
These contributing factors are general socioeconomic and environmental conditions, gender,
ethnic identity, and geographic place of residence. For instance, general socioeconomic and
environmental conditions, that is, the status people have in the society regarding education and
incomes can affect the ability of a person to access health services (HFA, 2000).
In the following report, health inequity is conveyed in three ways:
Health outcomes: - where the mortality (life quantity) and morbidity (life
quality) are considered.
Health risks: - where behavioral, biological, and environmental factors are
considered.
Utilization of health services: - where the rehabilitation, prevention and
treatment measures are put into consideration.
Taking into consideration the failure to minimize inequalities in the health sector, we
decided to carry out an audit in Stormlands, primarily to identify what more the local
government could ensure to improve the outcome. Our focus was the input the NHS and
Department of Health have made in securing health equity. The following were our terms of
reference:
Inequalities, the obligations of the government were stipulated to minimize inequities in the
health sector and recognize that sustainable action on the broader contributing factors of health
inequities is necessitated if the generation cycle of poverty and health is to be shattered.
According to Graham (2002), national policy and strategy indicate a collection of clarifications
and interpretations of the meaning of tackling health inequities.
This report discusses four significant determinants of health inequities in Stormlands.
These contributing factors are general socioeconomic and environmental conditions, gender,
ethnic identity, and geographic place of residence. For instance, general socioeconomic and
environmental conditions, that is, the status people have in the society regarding education and
incomes can affect the ability of a person to access health services (HFA, 2000).
In the following report, health inequity is conveyed in three ways:
Health outcomes: - where the mortality (life quantity) and morbidity (life
quality) are considered.
Health risks: - where behavioral, biological, and environmental factors are
considered.
Utilization of health services: - where the rehabilitation, prevention and
treatment measures are put into consideration.
Taking into consideration the failure to minimize inequalities in the health sector, we
decided to carry out an audit in Stormlands, primarily to identify what more the local
government could ensure to improve the outcome. Our focus was the input the NHS and
Department of Health have made in securing health equity. The following were our terms of
reference:
HEALTH EQUALITY ASSESSMENT REPORT 6
Whether the government, through the Ministry of Health, has met its
public service targets in respect to health inequalities ;
The accomplishment of NHS organizations to co-coordinate activities with
local authorities and other relevant organization in handling the issue of disparities;
The efficiency of the Department of Health in co-coordinating policies and
strategies with the local government departments, in an attempt at minimizing health
inequalities;
The quality and distribution of GP services and their impact on health
inequalities, and how the outcome and quality structure might be applied to reduce
disparities in the health sector; and
The efficiency of public health services in minimizing health inequalities
by aiming at the leading causes of disparities such as smoking in local areas.
Health Inequities
Health inequities in Stomlands society are documented in several aspects. Health and
other relevant agencies usually collect health statistics, and available in a range of source
documentations which we immensely relied on. There are limitations in the available data
regarding methods of collections, interpretation, and quality. However, regardless of the
restrictions, the information evidently indicates health inequalities across the subzones of
Stormlands in the stated measures: gender, socio-economic status, cultural uniqueness, and
geographical dwelling place.
Socioeconomic Inequalities
Health and possibilities of untimely deaths are caused by socioeconomic factors
prevailing throughout the life and across the generation (Davey-Smith et al., 1997). Therefore,
health in the middle or old age is subject to the previous socioeconomic status along with the
Whether the government, through the Ministry of Health, has met its
public service targets in respect to health inequalities ;
The accomplishment of NHS organizations to co-coordinate activities with
local authorities and other relevant organization in handling the issue of disparities;
The efficiency of the Department of Health in co-coordinating policies and
strategies with the local government departments, in an attempt at minimizing health
inequalities;
The quality and distribution of GP services and their impact on health
inequalities, and how the outcome and quality structure might be applied to reduce
disparities in the health sector; and
The efficiency of public health services in minimizing health inequalities
by aiming at the leading causes of disparities such as smoking in local areas.
Health Inequities
Health inequities in Stomlands society are documented in several aspects. Health and
other relevant agencies usually collect health statistics, and available in a range of source
documentations which we immensely relied on. There are limitations in the available data
regarding methods of collections, interpretation, and quality. However, regardless of the
restrictions, the information evidently indicates health inequalities across the subzones of
Stormlands in the stated measures: gender, socio-economic status, cultural uniqueness, and
geographical dwelling place.
Socioeconomic Inequalities
Health and possibilities of untimely deaths are caused by socioeconomic factors
prevailing throughout the life and across the generation (Davey-Smith et al., 1997). Therefore,
health in the middle or old age is subject to the previous socioeconomic status along with the
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH EQUALITY ASSESSMENT REPORT 7
current situation. In Stormlands, the subzones have registered a group of people with low level of
education. This always results in underpaid jobs which are vulnerable and expose them to
chemical and physical menaces, and inadequate housing.
There are several reasons behind the social-economic disadvantaged people in these
zones to less likely embrace the beneficial health demeanors (Marmot & Bell, 2013). First, the
relevant information as a guide on how they should healthily behave is not reaching them.
Moreover, they lack the necessary resources that can enable them to live healthily, furthermore,
the environment (swampy and infested with mosquitoes) where they live negatively affect their
health. It is also apparent that demeanors such as smoking are characterized and more inbuilt in
those people with low socio-economic status.
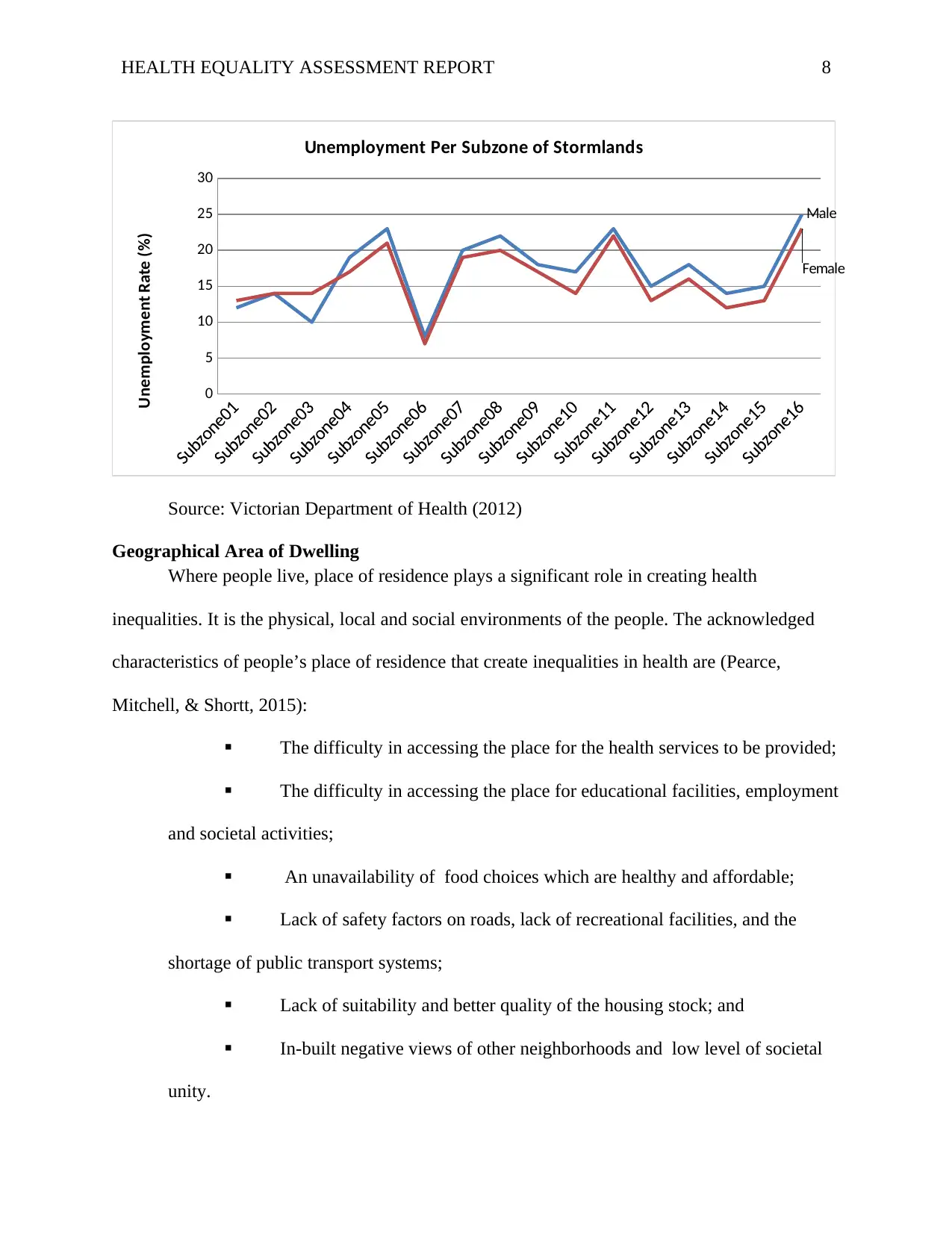
Health in Stormlands is improving, however, over the last decade inequalities in health
between the social classes have become widespread. The gap has increased by 11% among
women, and by 3% among men (Jelfs, 2016). Figure 1 below illustrates the employment rate in
Stormlands. Subzone 06 records the lowest rate of unemployment of about 7% among females
and 8% among males. Subzone 16 marks the highest percentage of unemployment of about 23%
among females and 25% among males. This scenario explains the inequalities in health across
the subzones which are as a result of unemployment.
Figure 1: Unemployment rate per subzone of Stormlands
current situation. In Stormlands, the subzones have registered a group of people with low level of
education. This always results in underpaid jobs which are vulnerable and expose them to
chemical and physical menaces, and inadequate housing.
There are several reasons behind the social-economic disadvantaged people in these
zones to less likely embrace the beneficial health demeanors (Marmot & Bell, 2013). First, the
relevant information as a guide on how they should healthily behave is not reaching them.
Moreover, they lack the necessary resources that can enable them to live healthily, furthermore,
the environment (swampy and infested with mosquitoes) where they live negatively affect their
health. It is also apparent that demeanors such as smoking are characterized and more inbuilt in
those people with low socio-economic status.
Health in Stormlands is improving, however, over the last decade inequalities in health
between the social classes have become widespread. The gap has increased by 11% among
women, and by 3% among men (Jelfs, 2016). Figure 1 below illustrates the employment rate in
Stormlands. Subzone 06 records the lowest rate of unemployment of about 7% among females
and 8% among males. Subzone 16 marks the highest percentage of unemployment of about 23%
among females and 25% among males. This scenario explains the inequalities in health across
the subzones which are as a result of unemployment.
Figure 1: Unemployment rate per subzone of Stormlands
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH EQUALITY ASSESSMENT REPORT 8
0
5
10
15
20
25
30
Male
Female
Unemployment Per Subzone of Stormlands
Unemployment Rate (%)
Source: Victorian Department of Health (2012)
Geographical Area of Dwelling
Where people live, place of residence plays a significant role in creating health
inequalities. It is the physical, local and social environments of the people. The acknowledged
characteristics of people’s place of residence that create inequalities in health are (Pearce,
Mitchell, & Shortt, 2015):
The difficulty in accessing the place for the health services to be provided;
The difficulty in accessing the place for educational facilities, employment
and societal activities;
An unavailability of food choices which are healthy and affordable;
Lack of safety factors on roads, lack of recreational facilities, and the
shortage of public transport systems;
Lack of suitability and better quality of the housing stock; and
In-built negative views of other neighborhoods and low level of societal
unity.
0
5
10
15
20
25
30
Male
Female
Unemployment Per Subzone of Stormlands
Unemployment Rate (%)
Source: Victorian Department of Health (2012)
Geographical Area of Dwelling
Where people live, place of residence plays a significant role in creating health
inequalities. It is the physical, local and social environments of the people. The acknowledged
characteristics of people’s place of residence that create inequalities in health are (Pearce,
Mitchell, & Shortt, 2015):
The difficulty in accessing the place for the health services to be provided;
The difficulty in accessing the place for educational facilities, employment
and societal activities;
An unavailability of food choices which are healthy and affordable;
Lack of safety factors on roads, lack of recreational facilities, and the
shortage of public transport systems;
Lack of suitability and better quality of the housing stock; and
In-built negative views of other neighborhoods and low level of societal
unity.
HEALTH EQUALITY ASSESSMENT REPORT 9
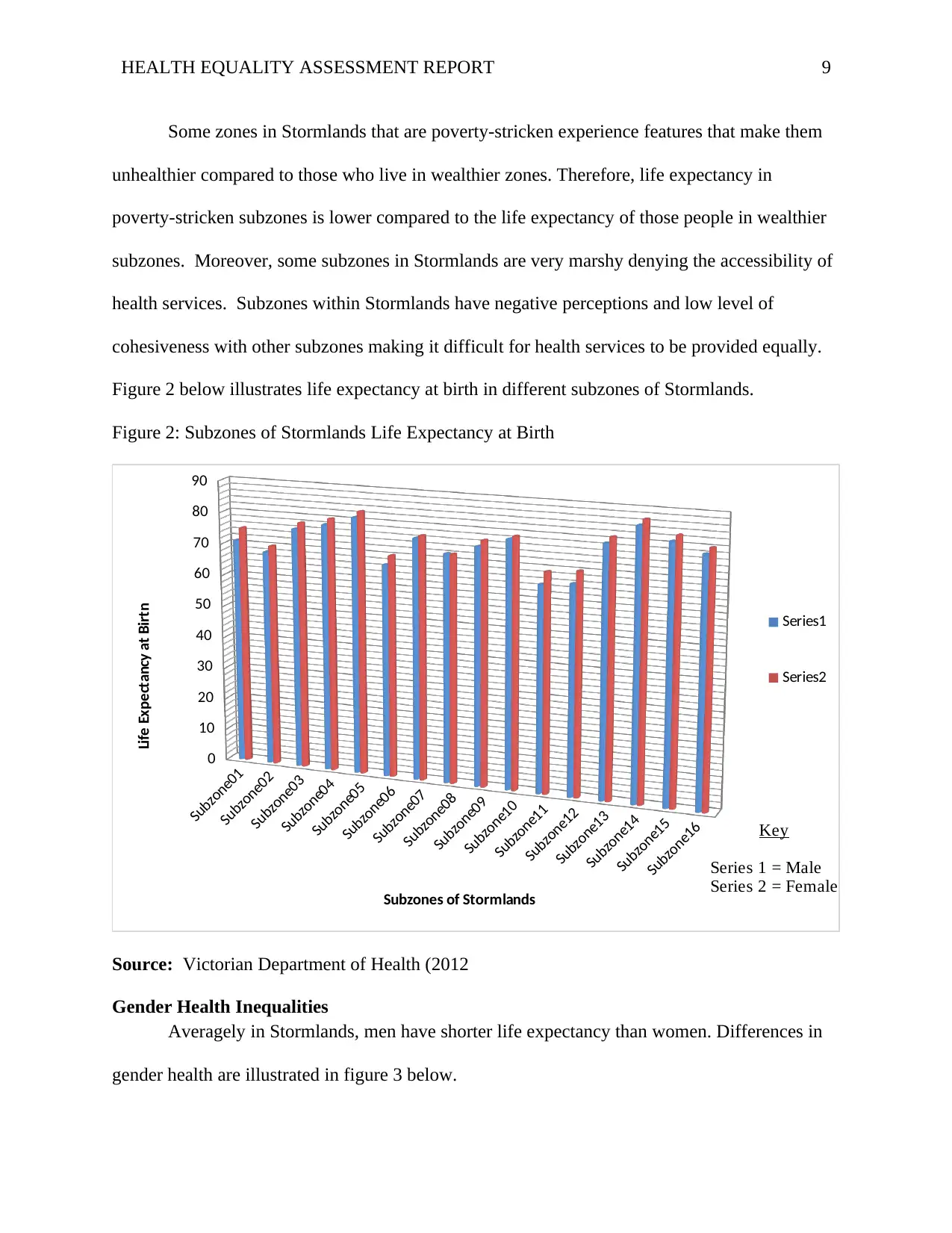
Some zones in Stormlands that are poverty-stricken experience features that make them
unhealthier compared to those who live in wealthier zones. Therefore, life expectancy in
poverty-stricken subzones is lower compared to the life expectancy of those people in wealthier
subzones. Moreover, some subzones in Stormlands are very marshy denying the accessibility of
health services. Subzones within Stormlands have negative perceptions and low level of
cohesiveness with other subzones making it difficult for health services to be provided equally.
Figure 2 below illustrates life expectancy at birth in different subzones of Stormlands.
Figure 2: Subzones of Stormlands Life Expectancy at Birth
Subzone01
Subzone02
Subzone03
Subzone04
Subzone05
Subzone06
Subzone07
Subzone08
Subzone09
Subzone10
Subzone11
Subzone12
Subzone13
Subzone14
Subzone15
Subzone16
0
10
20
30
40
50
60
70
80
90
Series1
Series2
Subzones of Stormlands
Life Expectancy at Birtn
Key
Series 1 = Male
Series 2 = Female
Source: Victorian Department of Health (2012
Gender Health Inequalities
Averagely in Stormlands, men have shorter life expectancy than women. Differences in
gender health are illustrated in figure 3 below.
Some zones in Stormlands that are poverty-stricken experience features that make them
unhealthier compared to those who live in wealthier zones. Therefore, life expectancy in
poverty-stricken subzones is lower compared to the life expectancy of those people in wealthier
subzones. Moreover, some subzones in Stormlands are very marshy denying the accessibility of
health services. Subzones within Stormlands have negative perceptions and low level of
cohesiveness with other subzones making it difficult for health services to be provided equally.
Figure 2 below illustrates life expectancy at birth in different subzones of Stormlands.
Figure 2: Subzones of Stormlands Life Expectancy at Birth
Subzone01
Subzone02
Subzone03
Subzone04
Subzone05
Subzone06
Subzone07
Subzone08
Subzone09
Subzone10
Subzone11
Subzone12
Subzone13
Subzone14
Subzone15
Subzone16
0
10
20
30
40
50
60
70
80
90
Series1
Series2
Subzones of Stormlands
Life Expectancy at Birtn
Key
Series 1 = Male
Series 2 = Female
Source: Victorian Department of Health (2012
Gender Health Inequalities
Averagely in Stormlands, men have shorter life expectancy than women. Differences in
gender health are illustrated in figure 3 below.
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
HEALTH EQUALITY ASSESSMENT REPORT 10
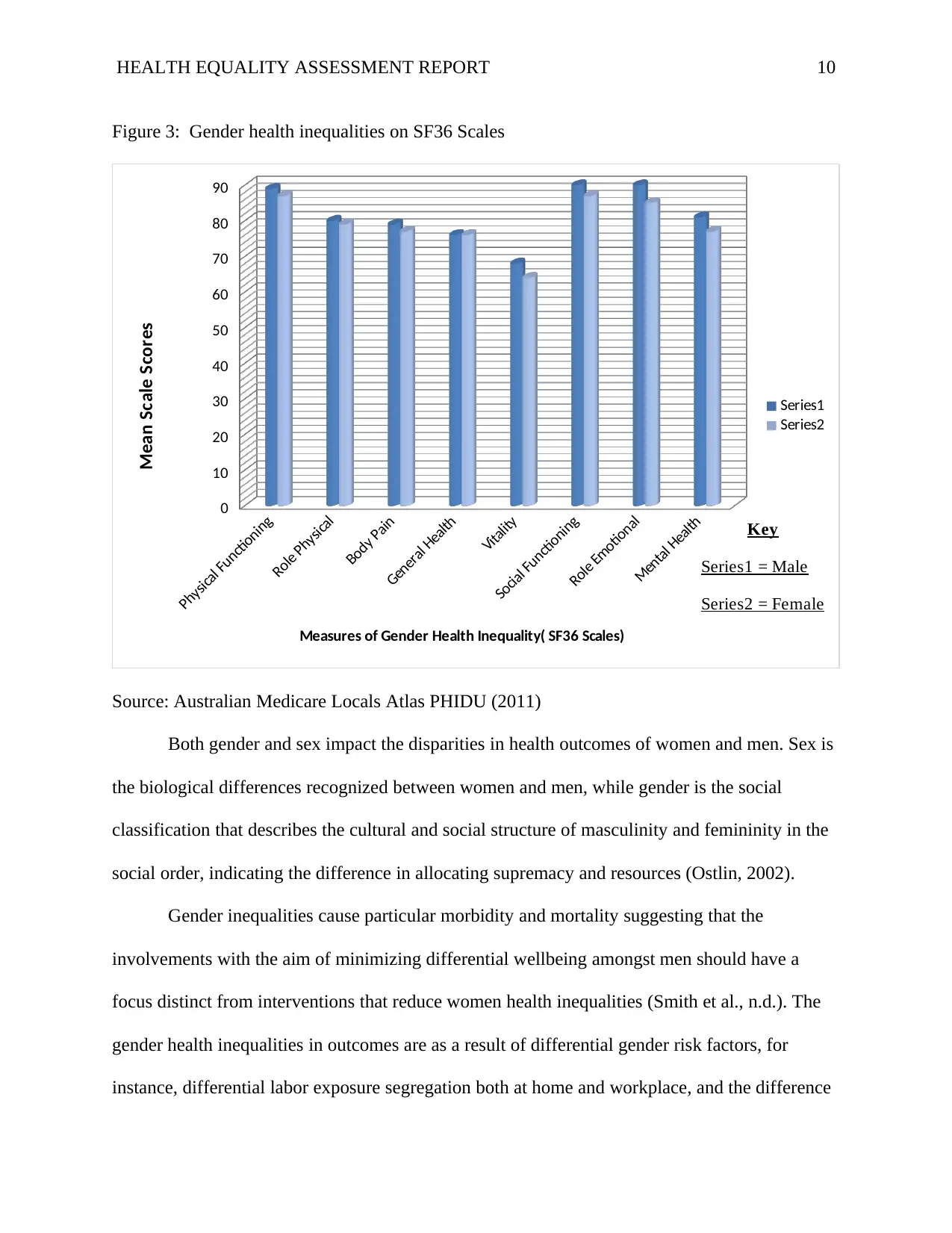
Figure 3: Gender health inequalities on SF36 Scales
Physical Functioning
Role Physical
Body Pain
General Health
Vitality
Social Functioning
Role Emotional
Mental Health
0
10
20
30
40
50
60
70
80
90
Series1
Series2
Measures of Gender Health Inequality( SF36 Scales)
Mean Scale Scores
Key
Series1 = Male
Series2 = Female
Source: Australian Medicare Locals Atlas PHIDU (2011)
Both gender and sex impact the disparities in health outcomes of women and men. Sex is
the biological differences recognized between women and men, while gender is the social
classification that describes the cultural and social structure of masculinity and femininity in the
social order, indicating the difference in allocating supremacy and resources (Ostlin, 2002).
Gender inequalities cause particular morbidity and mortality suggesting that the
involvements with the aim of minimizing differential wellbeing amongst men should have a
focus distinct from interventions that reduce women health inequalities (Smith et al., n.d.). The
gender health inequalities in outcomes are as a result of differential gender risk factors, for
instance, differential labor exposure segregation both at home and workplace, and the difference
Figure 3: Gender health inequalities on SF36 Scales
Physical Functioning
Role Physical
Body Pain
General Health
Vitality
Social Functioning
Role Emotional
Mental Health
0
10
20
30
40
50
60
70
80
90
Series1
Series2
Measures of Gender Health Inequality( SF36 Scales)
Mean Scale Scores
Key
Series1 = Male
Series2 = Female
Source: Australian Medicare Locals Atlas PHIDU (2011)
Both gender and sex impact the disparities in health outcomes of women and men. Sex is
the biological differences recognized between women and men, while gender is the social
classification that describes the cultural and social structure of masculinity and femininity in the
social order, indicating the difference in allocating supremacy and resources (Ostlin, 2002).
Gender inequalities cause particular morbidity and mortality suggesting that the
involvements with the aim of minimizing differential wellbeing amongst men should have a
focus distinct from interventions that reduce women health inequalities (Smith et al., n.d.). The
gender health inequalities in outcomes are as a result of differential gender risk factors, for
instance, differential labor exposure segregation both at home and workplace, and the difference
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
HEALTH EQUALITY ASSESSMENT REPORT 11
in accessing economic and social resources. The health of both women and men is affected by
gender policies and gender roles. Awareness programs need to be established in Stormlands to
sensitize the influence of roles which expose gender to health hazards, utilization of available
health services and health outcomes.
Lifestyle Inequalities
The lifestyle factors which impact inequalities in health are also referred to as the
‘proximate’ causes of inequalities in health since they are the direct originators of illnesses as
opposed to the ‘broader determinants ‘such as socio-economic factors (Kristenson, 2006). These
factors are smoking, nutrition, exercise, alcohol consumption, drug use, and sexual behavior. In
Stormlands, the statistic shows that higher percentage of men smoke than women.
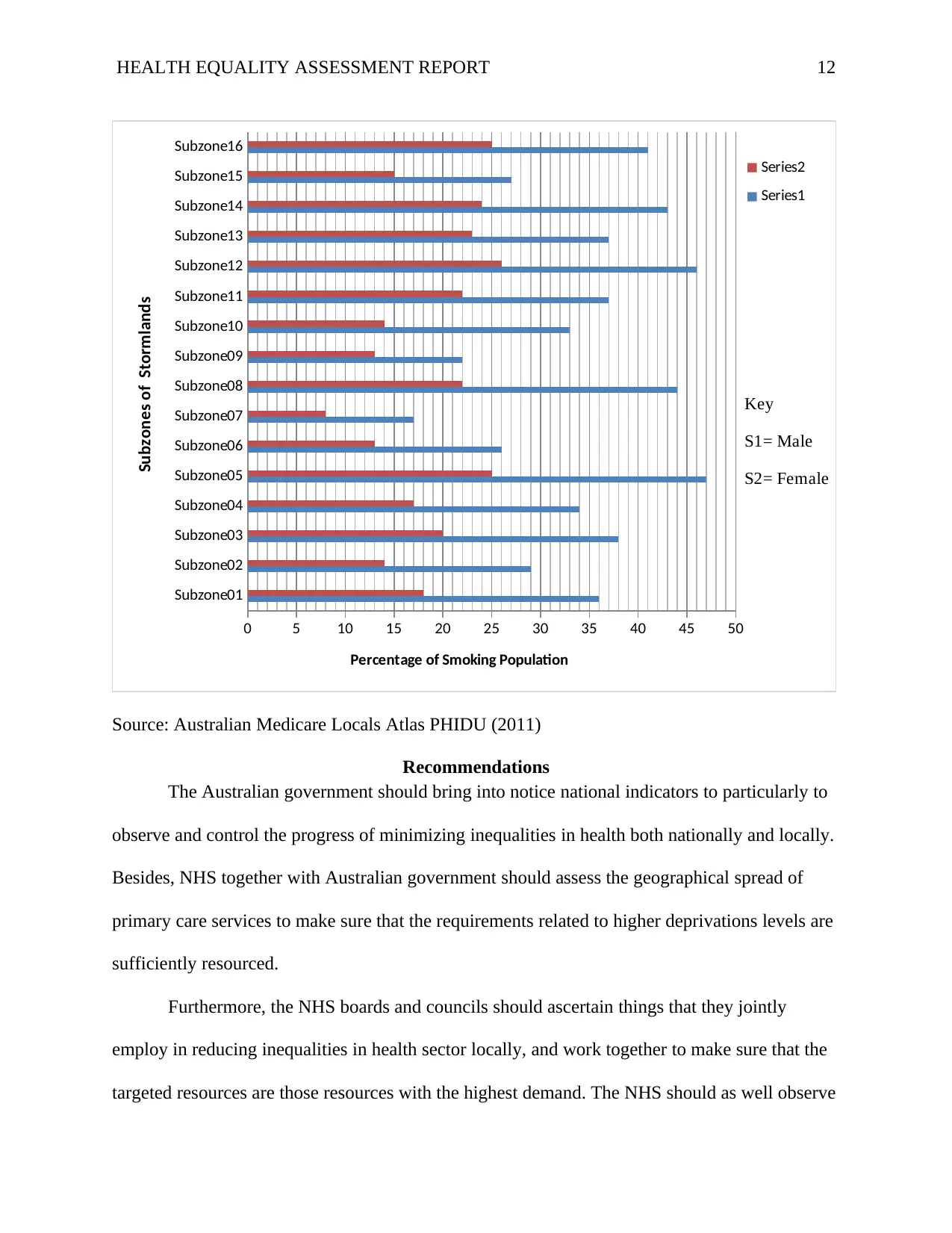
Figure 4 indicates levels of smoking among adults in the subzones of Stormlands.
Amongst male adults, daily cigarette smoking varies from an estimate of 17% to in Subzone 07
to 47% in Subzone 05 in Stormlands. Females recorded the lowest and highest percentage in
cigarette smoking; 8% in Subzone 07 and 26% in Subzone 12 respectively.
Figure 4: Percentage of adults smoking in Stormlands
in accessing economic and social resources. The health of both women and men is affected by
gender policies and gender roles. Awareness programs need to be established in Stormlands to
sensitize the influence of roles which expose gender to health hazards, utilization of available
health services and health outcomes.
Lifestyle Inequalities
The lifestyle factors which impact inequalities in health are also referred to as the
‘proximate’ causes of inequalities in health since they are the direct originators of illnesses as
opposed to the ‘broader determinants ‘such as socio-economic factors (Kristenson, 2006). These
factors are smoking, nutrition, exercise, alcohol consumption, drug use, and sexual behavior. In
Stormlands, the statistic shows that higher percentage of men smoke than women.
Figure 4 indicates levels of smoking among adults in the subzones of Stormlands.
Amongst male adults, daily cigarette smoking varies from an estimate of 17% to in Subzone 07
to 47% in Subzone 05 in Stormlands. Females recorded the lowest and highest percentage in
cigarette smoking; 8% in Subzone 07 and 26% in Subzone 12 respectively.
Figure 4: Percentage of adults smoking in Stormlands
HEALTH EQUALITY ASSESSMENT REPORT 12
Subzone01
Subzone02
Subzone03
Subzone04
Subzone05
Subzone06
Subzone07
Subzone08
Subzone09
Subzone10
Subzone11
Subzone12
Subzone13
Subzone14
Subzone15
Subzone16
0 5 10 15 20 25 30 35 40 45 50
Series2
Series1
Percentage of Smoking Population
Subzones of Stormlands
Key
S1= Male
S2= Female
Source: Australian Medicare Locals Atlas PHIDU (2011)
Recommendations
The Australian government should bring into notice national indicators to particularly to
observe and control the progress of minimizing inequalities in health both nationally and locally.
Besides, NHS together with Australian government should assess the geographical spread of
primary care services to make sure that the requirements related to higher deprivations levels are
sufficiently resourced.
Furthermore, the NHS boards and councils should ascertain things that they jointly
employ in reducing inequalities in health sector locally, and work together to make sure that the
targeted resources are those resources with the highest demand. The NHS should as well observe
Subzone01
Subzone02
Subzone03
Subzone04
Subzone05
Subzone06
Subzone07
Subzone08
Subzone09
Subzone10
Subzone11
Subzone12
Subzone13
Subzone14
Subzone15
Subzone16
0 5 10 15 20 25 30 35 40 45 50
Series2
Series1
Percentage of Smoking Population
Subzones of Stormlands
Key
S1= Male
S2= Female
Source: Australian Medicare Locals Atlas PHIDU (2011)
Recommendations
The Australian government should bring into notice national indicators to particularly to
observe and control the progress of minimizing inequalities in health both nationally and locally.
Besides, NHS together with Australian government should assess the geographical spread of
primary care services to make sure that the requirements related to higher deprivations levels are
sufficiently resourced.
Furthermore, the NHS boards and councils should ascertain things that they jointly
employ in reducing inequalities in health sector locally, and work together to make sure that the
targeted resources are those resources with the highest demand. The NHS should as well observe
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 16
Related Documents





Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.