Evaluating TAVI for Aortic Stenosis: A Review of RCTs & Outcomes
VerifiedAdded on 2023/04/05
|14
|3736
|96
Report
AI Summary
This report provides an overview of aortic stenosis (AS), its pathophysiology, and the emergence of Transcatheter Aortic-Valve Implantation (TAVI) as a less invasive treatment option. It discusses the pathology of AS, highlighting risk factors and diagnostic methods. The report analyzes three key randomized controlled trials (RCTs): PARTNER 1, PARTNER 2, and PARTNER 3, which compare TAVI with standard therapy or surgical aortic valve replacement (SAVR) in patients with varying risk levels. The findings from these trials demonstrate the efficacy and non-inferiority or superiority of TAVI in reducing mortality, stroke, and rehospitalization rates compared to traditional methods, suggesting its potential to become the standard of care for severe AS.

Running head: ASSIGNMENT 1
Assignment 1
Course number-
Lecturer name-
Word Count-
Assignment 1
Course number-
Lecturer name-
Word Count-
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
1ASSIGNMENT 1
Introduction
Aortic (valve) stenosis (AS) is an obstruction to blood flow from the
left ventricle (LV) to the aorta due to a fixed stenosis located in the aortic
valve. AS is the most frequent valvular heart disorder in Western
countries. The most common cause of aortic stenosis is degenerative
calcification of the aortic valve leaflets. Less common causes include
rheumatic heart disease and congenital aortic stenosis seen in younger patients.
The prevalence of aortic stenosis increases with age affecting 4 % of patients
aged above 85 (1). The estimated prevalence of AS in New Zealand is
approximately 103 per 100,000 population (2). Natural history studies have
shown that once patients become symptomatic, they have a rapid downhill
course with expected life expectancy of 5 years, 3 years and 2 years with the
onset of angina, dyspnoea and syncope respectively (3). The current gold
standard of treatment of aortic stenosis is surgical aortic valve replacement.
However it is estimated that approximately one third of patients with
symptomatic severe AS may be inoperable due to multiple factors (4).
Transcatheter aortic-valve implantation (TAVI) is a revolutionary new
procedure in which a new tissue valve is implanted at the site of the native
valve via a catheter. Ever since the first procedure was performed in 2002,
there has been an explosion in the number of cases performed throughout the
world.This assignment focuses on the pathophysiology of aortic stenosis, the
emergence of TAVI as a less invasive therapeutic option for patients at varying
risk strata supported by randomised controlled trials and the potential for
TAVI to become the standard of care for severe AS in the future.
Pathology
Roughly as much as 2% individuals aged above 65 years of age and 3%
people who are aged more than 75 years suffer from AS. In addition, 4%
people aged beyond 85 years also suffer from the condition, with an increased
prevalence observed amid older adults living in Europe and North America
(Manning, 2013). Some of the most common risk factors that are known to
create an influence on the progress of the disease encompass lifestyle habits,
hypertension, male gender, diabetes mellitus, metabolic syndrome, smoking,
Introduction
Aortic (valve) stenosis (AS) is an obstruction to blood flow from the
left ventricle (LV) to the aorta due to a fixed stenosis located in the aortic
valve. AS is the most frequent valvular heart disorder in Western
countries. The most common cause of aortic stenosis is degenerative
calcification of the aortic valve leaflets. Less common causes include
rheumatic heart disease and congenital aortic stenosis seen in younger patients.
The prevalence of aortic stenosis increases with age affecting 4 % of patients
aged above 85 (1). The estimated prevalence of AS in New Zealand is
approximately 103 per 100,000 population (2). Natural history studies have
shown that once patients become symptomatic, they have a rapid downhill
course with expected life expectancy of 5 years, 3 years and 2 years with the
onset of angina, dyspnoea and syncope respectively (3). The current gold
standard of treatment of aortic stenosis is surgical aortic valve replacement.
However it is estimated that approximately one third of patients with
symptomatic severe AS may be inoperable due to multiple factors (4).
Transcatheter aortic-valve implantation (TAVI) is a revolutionary new
procedure in which a new tissue valve is implanted at the site of the native
valve via a catheter. Ever since the first procedure was performed in 2002,
there has been an explosion in the number of cases performed throughout the
world.This assignment focuses on the pathophysiology of aortic stenosis, the
emergence of TAVI as a less invasive therapeutic option for patients at varying
risk strata supported by randomised controlled trials and the potential for
TAVI to become the standard of care for severe AS in the future.
Pathology
Roughly as much as 2% individuals aged above 65 years of age and 3%
people who are aged more than 75 years suffer from AS. In addition, 4%
people aged beyond 85 years also suffer from the condition, with an increased
prevalence observed amid older adults living in Europe and North America
(Manning, 2013). Some of the most common risk factors that are known to
create an influence on the progress of the disease encompass lifestyle habits,
hypertension, male gender, diabetes mellitus, metabolic syndrome, smoking,
2ASSIGNMENT 1
and end stage renal disease (Mancini et al., 2014). In addition, AS has been
recognised as a major progressive condition and is an end-stage illness that
might eventually result in death, by bringing about an obstruction in the left
ventricular outflow (Otto & Prendergast, 2014). According to Pasic,
Unbehaun, Buz, Drews and Hetzer (2015) during subsequent expansion of the
left ventricle, closure of the aortic valves prevent the backflow of blood
through the dorsal aorta to the left ventricle. Calcification leads to narrowing
and constriction of the aortic valves opening, thereby leading to AS. Bicuspid
and degenerative AS are most common and typically begin with injuries that
are caused to the endothelial cells, which in turn can be accredited to
endothelial damage occurring due to mechanical stress (Thaden, Nkomo &
Enriquez-Sarano, 2014).
Further research evidences have also elaborated on the fact that AS can
be commonly cited as the end outcome of an inflammatory procedure that is
brought about by leaflet thickening, lipid penetration that results in the onset of
fibrosis, and calcification. In addition, calcific AS also leads to an increase in
stiffness of the leaflets, and narrowing of the aortic valve orifice, subsequently
generating a pressure gradient, across the major valves (Joseph, Naqvi, Giri &
Goldberg, 2017). Findings from a meta-analysis have also elaborated on the
fact diagnosis of AS is generally conducted by echocardiography that depends
on conducting a subjective assessment of diffuse or focal aortic valve
thickening, in addition to the presence of increased echogenicity. This
echogenicity suggests calcification (Coffey, Cox & Williams, 2014).
Progressive narrowing of the aortic valves, in addition to simultaneous
pressure overload in the left ventricles, and left ventricular hypertrophy result
in the onset of aortic stenosis classic triad symptoms namely, syncope, heart
failure, and angina (Scappini, Maffei & Menditto, 2015).
There is mounting evidence for the fact that transcatheter aortic valve
replacement (TAVR) is an effective and minimally invasive process that helps
in the replacement of narrowed and constricted aortic valve, which cannot
open properly due to AS (Popma et al., 2016). Also referred to as transcatheter
aortic valve implantation (TAVI), the procedure is implemented for patients
who are recognised at a high risk of intermediate risk, of suffering from
and end stage renal disease (Mancini et al., 2014). In addition, AS has been
recognised as a major progressive condition and is an end-stage illness that
might eventually result in death, by bringing about an obstruction in the left
ventricular outflow (Otto & Prendergast, 2014). According to Pasic,
Unbehaun, Buz, Drews and Hetzer (2015) during subsequent expansion of the
left ventricle, closure of the aortic valves prevent the backflow of blood
through the dorsal aorta to the left ventricle. Calcification leads to narrowing
and constriction of the aortic valves opening, thereby leading to AS. Bicuspid
and degenerative AS are most common and typically begin with injuries that
are caused to the endothelial cells, which in turn can be accredited to
endothelial damage occurring due to mechanical stress (Thaden, Nkomo &
Enriquez-Sarano, 2014).
Further research evidences have also elaborated on the fact that AS can
be commonly cited as the end outcome of an inflammatory procedure that is
brought about by leaflet thickening, lipid penetration that results in the onset of
fibrosis, and calcification. In addition, calcific AS also leads to an increase in
stiffness of the leaflets, and narrowing of the aortic valve orifice, subsequently
generating a pressure gradient, across the major valves (Joseph, Naqvi, Giri &
Goldberg, 2017). Findings from a meta-analysis have also elaborated on the
fact diagnosis of AS is generally conducted by echocardiography that depends
on conducting a subjective assessment of diffuse or focal aortic valve
thickening, in addition to the presence of increased echogenicity. This
echogenicity suggests calcification (Coffey, Cox & Williams, 2014).
Progressive narrowing of the aortic valves, in addition to simultaneous
pressure overload in the left ventricles, and left ventricular hypertrophy result
in the onset of aortic stenosis classic triad symptoms namely, syncope, heart
failure, and angina (Scappini, Maffei & Menditto, 2015).
There is mounting evidence for the fact that transcatheter aortic valve
replacement (TAVR) is an effective and minimally invasive process that helps
in the replacement of narrowed and constricted aortic valve, which cannot
open properly due to AS (Popma et al., 2016). Also referred to as transcatheter
aortic valve implantation (TAVI), the procedure is implemented for patients
who are recognised at a high risk of intermediate risk, of suffering from
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
3ASSIGNMENT 1
associated cardiovascular complications, due to aortic valve replacement,
thereby replacing the constricted aortic valve (Leon et al., 2016). Efficacy of
TAVR has been demonstrated by researchers who subjected patient suffering
from severe AS to this procedure and correlated TAVR with a significant
increased survival rate of patients, in comparison to surgical aortic-valve
replacement (Adams et al., 2014). In addition, results from a meta-analysis
conducted by Giordana et al. (2014) that reported on the independent mortality
predictors after TAVR implantation also supported the aforementioned claims.
Upon conducting a systematic review the procedure was found to be effective
and safe for severe AS patients. 7.5% patients (n = 663) died at 30 days, and
the mortality rates were found to be an estimated 21.6% (n = 1,917).
In addition, the meta-analysis results also provided evidence for pre-
procedural hospital admission for heart failure (OR 9.4, 95% CI 2.6 to 35),
acute kidney injury (AKI) stage ≥2 (OR 18.0, 95% CI 6.3 to 52), elevated
levels of pro–brain natriuretic peptide (pro-BNP) levels (OR 5.4, 95% CI 1.7
to 16.5), and peri-procedural acute myocardial infarction (OR 8.5, 95% CI 2.6
to 33.5) being significant predictors of mortality (Giordana et al., 2014). The
evidences discussed above were also supported by findings from another
original investigation where, following a month of TAVR, as much as 92.6%
(n=313) patients were found to report improved functional status. Moreover,
the general 1-year survival rate was 83.2% for all patients who were subjected
to TACR, for the treatment of degenerated bioprosthetic aortic valves (Dvir et
al., 2014). However, recently the procedure is not recommended for patients
who are at a low risk, nonetheless, it is being increasingly implemented to
intermediate risk patients, by collecting evidences that demonstrate its non-
inferiority over surgical aortic valve replacement therapy.
Study presentation
PARTNER 1 trial
The researchers grounded their study on previous evidences that
replacing the constricted aortic valves by surgical procedures helps in
lessening the appearance of AS symptoms among patients and also improves
their overall survival rates. Nonetheless, they also acquired information from
associated cardiovascular complications, due to aortic valve replacement,
thereby replacing the constricted aortic valve (Leon et al., 2016). Efficacy of
TAVR has been demonstrated by researchers who subjected patient suffering
from severe AS to this procedure and correlated TAVR with a significant
increased survival rate of patients, in comparison to surgical aortic-valve
replacement (Adams et al., 2014). In addition, results from a meta-analysis
conducted by Giordana et al. (2014) that reported on the independent mortality
predictors after TAVR implantation also supported the aforementioned claims.
Upon conducting a systematic review the procedure was found to be effective
and safe for severe AS patients. 7.5% patients (n = 663) died at 30 days, and
the mortality rates were found to be an estimated 21.6% (n = 1,917).
In addition, the meta-analysis results also provided evidence for pre-
procedural hospital admission for heart failure (OR 9.4, 95% CI 2.6 to 35),
acute kidney injury (AKI) stage ≥2 (OR 18.0, 95% CI 6.3 to 52), elevated
levels of pro–brain natriuretic peptide (pro-BNP) levels (OR 5.4, 95% CI 1.7
to 16.5), and peri-procedural acute myocardial infarction (OR 8.5, 95% CI 2.6
to 33.5) being significant predictors of mortality (Giordana et al., 2014). The
evidences discussed above were also supported by findings from another
original investigation where, following a month of TAVR, as much as 92.6%
(n=313) patients were found to report improved functional status. Moreover,
the general 1-year survival rate was 83.2% for all patients who were subjected
to TACR, for the treatment of degenerated bioprosthetic aortic valves (Dvir et
al., 2014). However, recently the procedure is not recommended for patients
who are at a low risk, nonetheless, it is being increasingly implemented to
intermediate risk patients, by collecting evidences that demonstrate its non-
inferiority over surgical aortic valve replacement therapy.
Study presentation
PARTNER 1 trial
The researchers grounded their study on previous evidences that
replacing the constricted aortic valves by surgical procedures helps in
lessening the appearance of AS symptoms among patients and also improves
their overall survival rates. Nonetheless, they also acquired information from
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
4ASSIGNMENT 1
previous evidences that suggested the impacts of advancing age, and left
ventricular dysfunction that often eliminates the need of conducting surgeries.
358 patients were randomly assigned based on the presence of severe AS, and
who were not considered fitting candidates by surgeons for replacement of the
valves. They recruited PARTNER trial patients for this investigation and all of
the enrolled patients had class II, III, or IV symptoms that were in accordance
to the New York Heart Association (NYHA). Patients who had noncalcified or
bicuspid aortic valve, history of acute myocardial infarction, left ventricular
ejection fraction fewer than 20%, or aortic annulus diameter less than and
greater than 18 mm and 25 mm, respectively were excluded from the trial
(Leon et al., 2010).
Rate of death was considered as the primary end point. Following
randomisation of the patients to standard therapy that comprised of balloon
aortic valvuloplasty, and TAVR of balloon-expandable bovine pericardial
valve, it was found that rate of death was 30.7% with TAVI, in comparison to
50.7% from standard therapy (HR TAVI, 0.55; 95% CI, 0.40 to 0.74;
p<0.001). In addition, TAVI demonstrated 42.5% rate of end point death, as
contrasted with 71.6% from standard therapy. Furthermore, TAVI subjected
patients also demonstrated fewer cardiac symptoms, in contrast to their control
counterparts (Leon et al., 2010). This made the researchers conclude that TAVI
was able to bring about significant reduction in the rates of death amid AS
patients who were not considered fitting for surgical procedures. Despite the
high incidence of vascular complications and stroke, the TAVI subjected
patients also demonstrated lesser instances of repeated admissions at hospitals
and/or end point of death, thereby providing efficacy of the procedure.
PARTNER 2 trial
The investigators based their research on the fact that in previously
conducted trials that involved patients who had been identified at high-risk for
AS, similarities were observed in the survival rates of those who had been
subjected to surgical aorticvalve replacement and TAVR. A randomised
controlled trial was conducted by the researches among 2032 intermediate-risk
patients having severe AS, across 57 centres. Following patient enrolment that
previous evidences that suggested the impacts of advancing age, and left
ventricular dysfunction that often eliminates the need of conducting surgeries.
358 patients were randomly assigned based on the presence of severe AS, and
who were not considered fitting candidates by surgeons for replacement of the
valves. They recruited PARTNER trial patients for this investigation and all of
the enrolled patients had class II, III, or IV symptoms that were in accordance
to the New York Heart Association (NYHA). Patients who had noncalcified or
bicuspid aortic valve, history of acute myocardial infarction, left ventricular
ejection fraction fewer than 20%, or aortic annulus diameter less than and
greater than 18 mm and 25 mm, respectively were excluded from the trial
(Leon et al., 2010).
Rate of death was considered as the primary end point. Following
randomisation of the patients to standard therapy that comprised of balloon
aortic valvuloplasty, and TAVR of balloon-expandable bovine pericardial
valve, it was found that rate of death was 30.7% with TAVI, in comparison to
50.7% from standard therapy (HR TAVI, 0.55; 95% CI, 0.40 to 0.74;
p<0.001). In addition, TAVI demonstrated 42.5% rate of end point death, as
contrasted with 71.6% from standard therapy. Furthermore, TAVI subjected
patients also demonstrated fewer cardiac symptoms, in contrast to their control
counterparts (Leon et al., 2010). This made the researchers conclude that TAVI
was able to bring about significant reduction in the rates of death amid AS
patients who were not considered fitting for surgical procedures. Despite the
high incidence of vascular complications and stroke, the TAVI subjected
patients also demonstrated lesser instances of repeated admissions at hospitals
and/or end point of death, thereby providing efficacy of the procedure.
PARTNER 2 trial
The investigators based their research on the fact that in previously
conducted trials that involved patients who had been identified at high-risk for
AS, similarities were observed in the survival rates of those who had been
subjected to surgical aorticvalve replacement and TAVR. A randomised
controlled trial was conducted by the researches among 2032 intermediate-risk
patients having severe AS, across 57 centres. Following patient enrolment that
5ASSIGNMENT 1
occurred from December-November 2013, death due to any cause and/or
disabling stroke were measured as the primary end point. The researchers
hypothesised that TAVR would not be less effective than surgical aortic valve
replacement. The patients were added to either of the two cohorts, PARTNER
cohort B trial, and PARTNER cohort A trial, following which 23.7% were
placed in transthoracic-access, and 76.3% in transfemoral-access.The
procedure of transthoracic placement employed similar valve that had beeen
placed either through the transaortic or transapical access route. Additionally,
all patients were subjected to 81 mg aspirin and >300 mg clopidogrel prior to,
and heparin, during the procedure. Clopidogrel and aspirin were taken
indefinitely for at least a month after the procedure (Leon et al., 2016).
There was no significant difference in the mortality between the
surgery and TAVR group (p=0.001 for noninferiority). However, rates of
Kaplan–Meier event were 21.1% and 19.3% in the surgery and intervention
group, respectively (HR TAVR group, 0.89; 95% CI, 0.73 to 1.09; p=0.25).
TAVR was correlated with reduced death and disabling stroke in transfemoral-
access cohort, when compared to surgery (HR 0.79; 95% CI, 0.62 to 1.00;
p=0.05). However, the researchers failed to observe any significant difference
between the two groups in transthoracic-access cohort. TAVR was also allied
with greater aortic valve regions, reduced acute renal injuries, bleeding, and
new-onset atrial fibrillation. In contrast, the surgical procedure was associated
with lesser cases of vascular complications and had fewer instances of
paravalvular aortic regurgitation (Leon et al., 2016). This made the researchers
conclude that TAVR was in no way different to surgical replacement of aortic
valve among intermediate-risk patients, in relation to disabling stroke and/or
death end point.
PARTNER 3 trial
With the aim of comparing between the consequences of surgical aortic
valve replacement (SAVR) and transcatheter aortic valve replacement
(TAVR), a randomised control trial was conducted amid patients who had been
diagnosed with AS, and were at high or intermediate-risk for death due to
surgery (Mack et al., 2019). The research was based on previous evidences
occurred from December-November 2013, death due to any cause and/or
disabling stroke were measured as the primary end point. The researchers
hypothesised that TAVR would not be less effective than surgical aortic valve
replacement. The patients were added to either of the two cohorts, PARTNER
cohort B trial, and PARTNER cohort A trial, following which 23.7% were
placed in transthoracic-access, and 76.3% in transfemoral-access.The
procedure of transthoracic placement employed similar valve that had beeen
placed either through the transaortic or transapical access route. Additionally,
all patients were subjected to 81 mg aspirin and >300 mg clopidogrel prior to,
and heparin, during the procedure. Clopidogrel and aspirin were taken
indefinitely for at least a month after the procedure (Leon et al., 2016).
There was no significant difference in the mortality between the
surgery and TAVR group (p=0.001 for noninferiority). However, rates of
Kaplan–Meier event were 21.1% and 19.3% in the surgery and intervention
group, respectively (HR TAVR group, 0.89; 95% CI, 0.73 to 1.09; p=0.25).
TAVR was correlated with reduced death and disabling stroke in transfemoral-
access cohort, when compared to surgery (HR 0.79; 95% CI, 0.62 to 1.00;
p=0.05). However, the researchers failed to observe any significant difference
between the two groups in transthoracic-access cohort. TAVR was also allied
with greater aortic valve regions, reduced acute renal injuries, bleeding, and
new-onset atrial fibrillation. In contrast, the surgical procedure was associated
with lesser cases of vascular complications and had fewer instances of
paravalvular aortic regurgitation (Leon et al., 2016). This made the researchers
conclude that TAVR was in no way different to surgical replacement of aortic
valve among intermediate-risk patients, in relation to disabling stroke and/or
death end point.
PARTNER 3 trial
With the aim of comparing between the consequences of surgical aortic
valve replacement (SAVR) and transcatheter aortic valve replacement
(TAVR), a randomised control trial was conducted amid patients who had been
diagnosed with AS, and were at high or intermediate-risk for death due to
surgery (Mack et al., 2019). The research was based on previous evidences
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
6ASSIGNMENT 1
where TAVR had been proved to be either non-inferior are superior to
conventional therapies, including SAVR. The researchers grounded their study
on the technological advancements that have resulted in an increase in the
number of patients who are subjected to TAVR, in comparison to isolated
surgeries, in the US. The investigators conducted a multicenter randomised
PARTNER 3 trial, whereby comparison was drawn between standard SAVR
procedure and TAVR procedure, with the use of third-generation balloon
expandable valves.
The randomisation process involved 1000 patients located at 71
centres, with the mean age being 73 years. Stroke, rate of rehospitalisation
within a year, and death were the primary endpoints. Superiority and non-
inferiority testing were also performed in the target population. Results
obtained from Kaplan–Meier estimate indicated significant lessening in the
primary composite endpoint in TAVR group at 1 year, when compared to their
surgical counterparts (8.5% vs. 15.1%; absolute difference, −6.6 percentage
points; 95% CI, −10.8 to −2.5; p<0.001 for non-inferiority; HR 0.54; 95% CI,
0.37 to 0.79; p=0.001 for superiority) (Mack et al., 2019). In addition, TAVR
was also found to reduce the rate of strokes, death due to surgery and
recurrence of atrial fibrillation, than the surgical method. Efficacy of the trial
was also determined by a significant reduced index hospitalization in TAVR
procedure, besides showing a decreased risk of poor health outcomes at the end
of a month (p<0.001). The researchers did not find any significant differences
in permanent insertion of pacemakers, major vascular complications, or
paravalvular regurgitation. Thus, TAVR was found to be more effective than
SAVR among high and intermediate-risk AS patients.
Study PARTNER 1 PARTNER 2 PARTNER 3
Design RCT among 358
patients having
AS and not
considered
suitable for
surgery
RCT among
2032
intermediate-
risk patients
RCT among 1000
patients
approximately 73
years old
Intervention TAVI or standard Surgical TAVR using
where TAVR had been proved to be either non-inferior are superior to
conventional therapies, including SAVR. The researchers grounded their study
on the technological advancements that have resulted in an increase in the
number of patients who are subjected to TAVR, in comparison to isolated
surgeries, in the US. The investigators conducted a multicenter randomised
PARTNER 3 trial, whereby comparison was drawn between standard SAVR
procedure and TAVR procedure, with the use of third-generation balloon
expandable valves.
The randomisation process involved 1000 patients located at 71
centres, with the mean age being 73 years. Stroke, rate of rehospitalisation
within a year, and death were the primary endpoints. Superiority and non-
inferiority testing were also performed in the target population. Results
obtained from Kaplan–Meier estimate indicated significant lessening in the
primary composite endpoint in TAVR group at 1 year, when compared to their
surgical counterparts (8.5% vs. 15.1%; absolute difference, −6.6 percentage
points; 95% CI, −10.8 to −2.5; p<0.001 for non-inferiority; HR 0.54; 95% CI,
0.37 to 0.79; p=0.001 for superiority) (Mack et al., 2019). In addition, TAVR
was also found to reduce the rate of strokes, death due to surgery and
recurrence of atrial fibrillation, than the surgical method. Efficacy of the trial
was also determined by a significant reduced index hospitalization in TAVR
procedure, besides showing a decreased risk of poor health outcomes at the end
of a month (p<0.001). The researchers did not find any significant differences
in permanent insertion of pacemakers, major vascular complications, or
paravalvular regurgitation. Thus, TAVR was found to be more effective than
SAVR among high and intermediate-risk AS patients.
Study PARTNER 1 PARTNER 2 PARTNER 3
Design RCT among 358
patients having
AS and not
considered
suitable for
surgery
RCT among
2032
intermediate-
risk patients
RCT among 1000
patients
approximately 73
years old
Intervention TAVI or standard Surgical TAVR using
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
7ASSIGNMENT 1
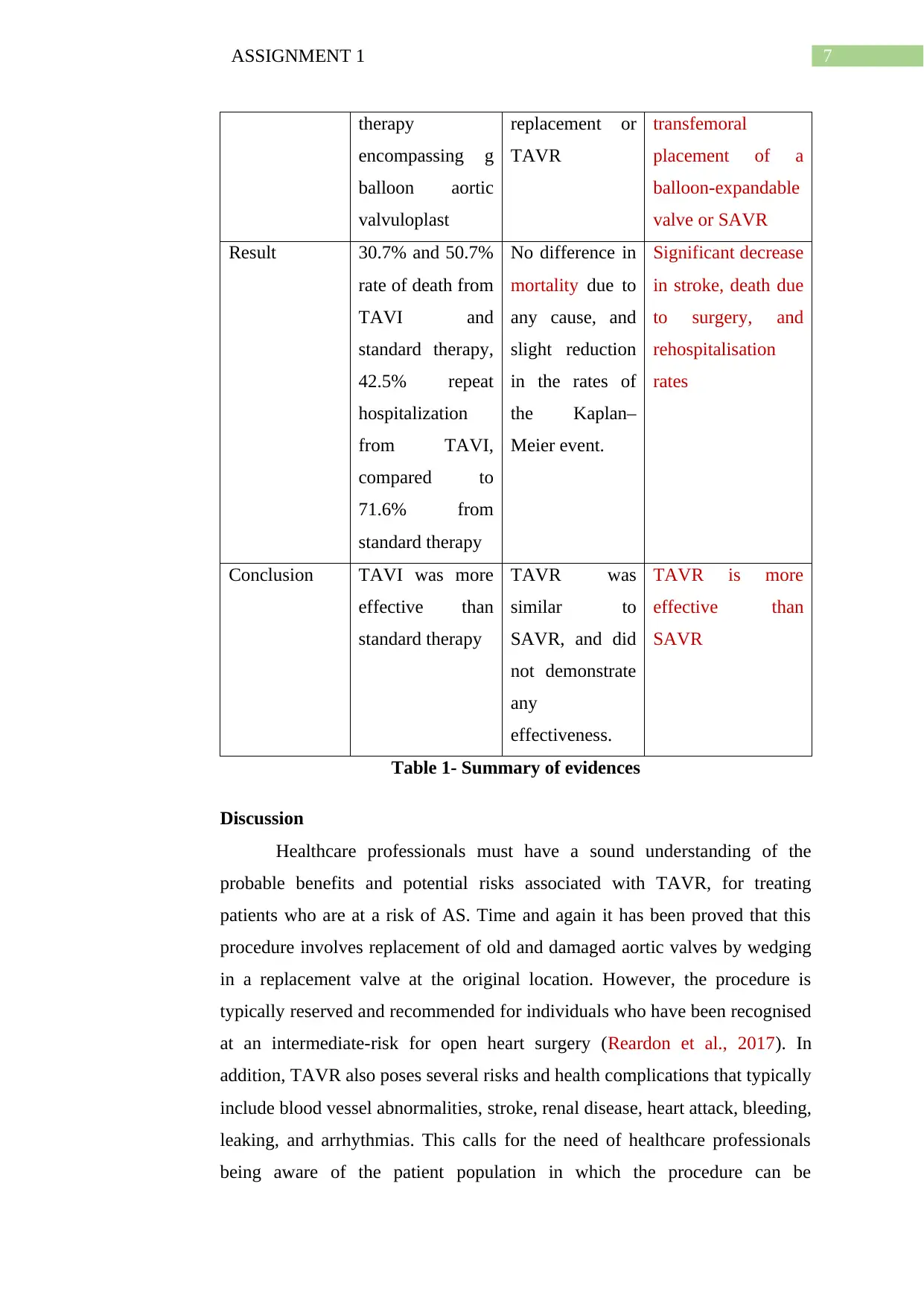
therapy
encompassing g
balloon aortic
valvuloplast
replacement or
TAVR
transfemoral
placement of a
balloon-expandable
valve or SAVR
Result 30.7% and 50.7%
rate of death from
TAVI and
standard therapy,
42.5% repeat
hospitalization
from TAVI,
compared to
71.6% from
standard therapy
No difference in
mortality due to
any cause, and
slight reduction
in the rates of
the Kaplan–
Meier event.
Significant decrease
in stroke, death due
to surgery, and
rehospitalisation
rates
Conclusion TAVI was more
effective than
standard therapy
TAVR was
similar to
SAVR, and did
not demonstrate
any
effectiveness.
TAVR is more
effective than
SAVR
Table 1- Summary of evidences
Discussion
Healthcare professionals must have a sound understanding of the
probable benefits and potential risks associated with TAVR, for treating
patients who are at a risk of AS. Time and again it has been proved that this
procedure involves replacement of old and damaged aortic valves by wedging
in a replacement valve at the original location. However, the procedure is
typically reserved and recommended for individuals who have been recognised
at an intermediate-risk for open heart surgery (Reardon et al., 2017). In
addition, TAVR also poses several risks and health complications that typically
include blood vessel abnormalities, stroke, renal disease, heart attack, bleeding,
leaking, and arrhythmias. This calls for the need of healthcare professionals
being aware of the patient population in which the procedure can be
therapy
encompassing g
balloon aortic
valvuloplast
replacement or
TAVR
transfemoral
placement of a
balloon-expandable
valve or SAVR
Result 30.7% and 50.7%
rate of death from
TAVI and
standard therapy,
42.5% repeat
hospitalization
from TAVI,
compared to
71.6% from
standard therapy
No difference in
mortality due to
any cause, and
slight reduction
in the rates of
the Kaplan–
Meier event.
Significant decrease
in stroke, death due
to surgery, and
rehospitalisation
rates
Conclusion TAVI was more
effective than
standard therapy
TAVR was
similar to
SAVR, and did
not demonstrate
any
effectiveness.
TAVR is more
effective than
SAVR
Table 1- Summary of evidences
Discussion
Healthcare professionals must have a sound understanding of the
probable benefits and potential risks associated with TAVR, for treating
patients who are at a risk of AS. Time and again it has been proved that this
procedure involves replacement of old and damaged aortic valves by wedging
in a replacement valve at the original location. However, the procedure is
typically reserved and recommended for individuals who have been recognised
at an intermediate-risk for open heart surgery (Reardon et al., 2017). In
addition, TAVR also poses several risks and health complications that typically
include blood vessel abnormalities, stroke, renal disease, heart attack, bleeding,
leaking, and arrhythmias. This calls for the need of healthcare professionals
being aware of the patient population in which the procedure can be
8ASSIGNMENT 1
implemented, with limited or no risks to their health. An analysis of the articles
discussed above helped in identification of the fact that currently used devices
for TAVR comprise of balloon expandable SAPIEN prosthesis and self-
expandable CoreValve prosthesis (Barbanti et al., 2015). Owing to the fact that
the procedure is still in the initial stages of implementation, information from
the randomised controlled trials added to evidences (Reardon et al., 2015).
It can be deduced from the aforementioned studies and additional
references suggested that patients having echocardiographic mean gradient
higher than 40 mm Hg and aortic valve area (AVA) lesser than 0.8 square cm
are typically considered suitable for TAVR. The PARTNER I trial that took
into consideration the Edwards SAPIEN first-generation valves was one of the
first investigations that tried to draw a comparison between TAVR and SAVR,
or other medical therapies (Kapadia et al., 2014). The findings presented above
are in accordance with results from supplementary scholarly evidences that
have illustrated the procedural success of TAVR in as much as 90% case
scenarios. The efficacy of TAVR intervention, as discussed in the randomised
controlled trials were also congruent with those of a retrospective study
conducted between 2005 and 2015, whereby 269 and 174 patients were
subjected to TAVR and SAVR, respectively. Structural valve deterioration
(SVD) was found common among TAVR patients in the long run, the rates of
which were significantly alike to those of SAVR. Hence, Aldalati et al. (2018)
could not find noteworthy difference between the two procedures and their
impact on AS patients. The fact that there does not exist any major variation
between the two procedures, commonly employed for the management of AS
was also highlighted in another recent systematic review that reported similar
rates of 30-day all-cause readmissions, post-SAVR and post-TAVR (16% and
17%, respectively). Some of the most recurrent events were most frequent
causes involving infection, arrhythmia, heart failure, and respiratory problems
(Danielsen et al., 2018). In addition, it is imperative for healthcare
professionals to characterise aortic regurgitation following TAVR, on the basis
of severity, location, and cause, besides integrating paravalvular and central
origin for estimating the general volumetric impact of the
procedure.Paravalvular leaks have been found to occur due to prosthesis
implemented, with limited or no risks to their health. An analysis of the articles
discussed above helped in identification of the fact that currently used devices
for TAVR comprise of balloon expandable SAPIEN prosthesis and self-
expandable CoreValve prosthesis (Barbanti et al., 2015). Owing to the fact that
the procedure is still in the initial stages of implementation, information from
the randomised controlled trials added to evidences (Reardon et al., 2015).
It can be deduced from the aforementioned studies and additional
references suggested that patients having echocardiographic mean gradient
higher than 40 mm Hg and aortic valve area (AVA) lesser than 0.8 square cm
are typically considered suitable for TAVR. The PARTNER I trial that took
into consideration the Edwards SAPIEN first-generation valves was one of the
first investigations that tried to draw a comparison between TAVR and SAVR,
or other medical therapies (Kapadia et al., 2014). The findings presented above
are in accordance with results from supplementary scholarly evidences that
have illustrated the procedural success of TAVR in as much as 90% case
scenarios. The efficacy of TAVR intervention, as discussed in the randomised
controlled trials were also congruent with those of a retrospective study
conducted between 2005 and 2015, whereby 269 and 174 patients were
subjected to TAVR and SAVR, respectively. Structural valve deterioration
(SVD) was found common among TAVR patients in the long run, the rates of
which were significantly alike to those of SAVR. Hence, Aldalati et al. (2018)
could not find noteworthy difference between the two procedures and their
impact on AS patients. The fact that there does not exist any major variation
between the two procedures, commonly employed for the management of AS
was also highlighted in another recent systematic review that reported similar
rates of 30-day all-cause readmissions, post-SAVR and post-TAVR (16% and
17%, respectively). Some of the most recurrent events were most frequent
causes involving infection, arrhythmia, heart failure, and respiratory problems
(Danielsen et al., 2018). In addition, it is imperative for healthcare
professionals to characterise aortic regurgitation following TAVR, on the basis
of severity, location, and cause, besides integrating paravalvular and central
origin for estimating the general volumetric impact of the
procedure.Paravalvular leaks have been found to occur due to prosthesis
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
9ASSIGNMENT 1
insufficient inflation and/or calcific deposition, which in turn prevents
appropriate positioning and sealing of the valve unit, within the annulus (Qian
et al., 2017).
Conclusion
To conclude, during contraction of the left ventricle, oxygenated blood
is generally forced through the valves into the dorsal aorta that subsequently
gets distributed to different regions of the body. Aortic stenosis is a common
valve illness and occurs due to narrowing and constriction of aortic valves. The
report found that AS brings about a restriction in the flow of blood from the
left ventricles to dorsal aorta, and also creates an impact on the pressure in the
left auricle. Since only one of the three randomised clinical trials was able to
demonstrate that TAVR is more effective and can be implemented among
intermediate and high-risk AS patients, all healthcare professionals must gain
an insight into the risk factors that are associated with TAVR.
insufficient inflation and/or calcific deposition, which in turn prevents
appropriate positioning and sealing of the valve unit, within the annulus (Qian
et al., 2017).
Conclusion
To conclude, during contraction of the left ventricle, oxygenated blood
is generally forced through the valves into the dorsal aorta that subsequently
gets distributed to different regions of the body. Aortic stenosis is a common
valve illness and occurs due to narrowing and constriction of aortic valves. The
report found that AS brings about a restriction in the flow of blood from the
left ventricles to dorsal aorta, and also creates an impact on the pressure in the
left auricle. Since only one of the three randomised clinical trials was able to
demonstrate that TAVR is more effective and can be implemented among
intermediate and high-risk AS patients, all healthcare professionals must gain
an insight into the risk factors that are associated with TAVR.
Paraphrase This Document
Need a fresh take? Get an instant paraphrase of this document with our AI Paraphraser
10ASSIGNMENT 1
References
Adams, D. H., Popma, J. J., Reardon, M. J., Yakubov, S. J., Coselli, J. S.,
Deeb, G. M., ... & Chetcuti, S. (2014). Transcatheter aortic-valve
replacement with a self-expanding prosthesis. New England Journal of
Medicine, 370(19), 1790-1798. DOI: 10.1056/NEJMoa1400590
Aldalati, O., Kaura, A., Khan, H., Dworakowski, R., Byrne, J., Eskandari,
M., ... & MacCarthy, P. (2018). Bioprosthetic structural valve
deterioration: How do TAVR and SAVR prostheses
compare?. International journal of cardiology, 268, 170-175.
https://doi.org/10.1016/j.ijcard.2018.04.091
Barbanti, M., Petronio, A. S., Ettori, F., Latib, A., Bedogni, F., De Marco,
F., ... & Colombo, A. (2015). 5-year outcomes after transcatheter aortic
valve implantation with CoreValve prosthesis. JACC: Cardiovascular
interventions, 8(8), 1084-1091. DOI: 10.1016/j.jcin.2015.03.024
Coffey, S., Cox, B., & Williams, M. J. (2014). The prevalence, incidence,
progression, and risks of aortic valve sclerosis: a systematic review and
meta-analysis. Journal of the American College of Cardiology, 63(25
Part A), 2852-2861. DOI: 10.1016/j.jacc.2014.04.018
Danielsen, S. O., Moons, P., Sandven, I., Leegaard, M., Solheim, S.,
Tønnessen, T., & Lie, I. (2018). Thirty-day readmissions in surgical
and transcatheter aortic valve replacement: A systematic review and
meta-analysis. International journal of cardiology, 268, 85-91.
https://doi.org/10.1016/j.ijcard.2018.05.026
Dvir, D., Webb, J. G., Bleiziffer, S., Pasic, M., Waksman, R., Kodali, S., ... &
Treede, H. (2014). Transcatheter aortic valve implantation in failed
bioprosthetic surgical valves. Jama, 312(2), 162-170.
doi:10.1001/jama.2014.7246
Giordana, F., D'Ascenzo, F., Nijhoff, F., Moretti, C., D'Amico, M., Zoccai, G.
B., ... & Dumonteil, N. (2014). Meta-analysis of predictors of all-cause
mortality after transcatheter aortic valve implantation. The American
References
Adams, D. H., Popma, J. J., Reardon, M. J., Yakubov, S. J., Coselli, J. S.,
Deeb, G. M., ... & Chetcuti, S. (2014). Transcatheter aortic-valve
replacement with a self-expanding prosthesis. New England Journal of
Medicine, 370(19), 1790-1798. DOI: 10.1056/NEJMoa1400590
Aldalati, O., Kaura, A., Khan, H., Dworakowski, R., Byrne, J., Eskandari,
M., ... & MacCarthy, P. (2018). Bioprosthetic structural valve
deterioration: How do TAVR and SAVR prostheses
compare?. International journal of cardiology, 268, 170-175.
https://doi.org/10.1016/j.ijcard.2018.04.091
Barbanti, M., Petronio, A. S., Ettori, F., Latib, A., Bedogni, F., De Marco,
F., ... & Colombo, A. (2015). 5-year outcomes after transcatheter aortic
valve implantation with CoreValve prosthesis. JACC: Cardiovascular
interventions, 8(8), 1084-1091. DOI: 10.1016/j.jcin.2015.03.024
Coffey, S., Cox, B., & Williams, M. J. (2014). The prevalence, incidence,
progression, and risks of aortic valve sclerosis: a systematic review and
meta-analysis. Journal of the American College of Cardiology, 63(25
Part A), 2852-2861. DOI: 10.1016/j.jacc.2014.04.018
Danielsen, S. O., Moons, P., Sandven, I., Leegaard, M., Solheim, S.,
Tønnessen, T., & Lie, I. (2018). Thirty-day readmissions in surgical
and transcatheter aortic valve replacement: A systematic review and
meta-analysis. International journal of cardiology, 268, 85-91.
https://doi.org/10.1016/j.ijcard.2018.05.026
Dvir, D., Webb, J. G., Bleiziffer, S., Pasic, M., Waksman, R., Kodali, S., ... &
Treede, H. (2014). Transcatheter aortic valve implantation in failed
bioprosthetic surgical valves. Jama, 312(2), 162-170.
doi:10.1001/jama.2014.7246
Giordana, F., D'Ascenzo, F., Nijhoff, F., Moretti, C., D'Amico, M., Zoccai, G.
B., ... & Dumonteil, N. (2014). Meta-analysis of predictors of all-cause
mortality after transcatheter aortic valve implantation. The American
11ASSIGNMENT 1
journal of cardiology, 114(9), 1447-1455.
https://doi.org/10.1016/j.amjcard.2014.07.081
Joseph, J., Naqvi, S. Y., Giri, J., & Goldberg, S. (2017). Aortic stenosis:
pathophysiology, diagnosis, and therapy. The American journal of
medicine, 130(3), 253-263.
https://doi.org/10.1016/j.amjmed.2016.10.005
Kapadia, S. R., Leon, M. B., Makkar, R. R., Tuzcu, E. M., Svensson, L. G.,
Kodali, S., ... & Babaliaros, V. C. (2015). 5-year outcomes of
transcatheter aortic valve replacement compared with standard
treatment for patients with inoperable aortic stenosis (PARTNER 1): a
randomised controlled trial. The Lancet, 385(9986), 2485-2491.
https://doi.org/10.1016/S0140-6736(15)60290-2
Leon, M. B., Smith, C. R., Mack, M. J., Makkar, R. R., Svensson, L. G.,
Kodali, S. K., ... & Doshi, D. (2016). Transcatheter or surgical aortic-
valve replacement in intermediate-risk patients. New England Journal
of Medicine, 374(17), 1609-1620. DOI: 10.1056/NEJMoa1514616
Leon, M. B., Smith, C. R., Mack, M. J., Makkar, R. R., Svensson, L. G.,
Kodali, S. K., ... & Doshi, D. (2016). Transcatheter or surgical aortic-
valve replacement in intermediate-risk patients. New England Journal
of Medicine, 374(17), 1609-1620. DOI: 10.1056/NEJMoa1514616
Leon, M. B., Smith, C. R., Mack, M., Miller, D. C., Moses, J. W., Svensson, L.
G., ... & Brown, D. L. (2010). Transcatheter aortic-valve implantation
for aortic stenosis in patients who cannot undergo surgery. New
England Journal of Medicine, 363(17), 1597-1607. DOI:
10.1056/NEJMoa1008232
Mack, M. J., Leon, M. B., Thourani, V. H., Makkar, R., Kodali, S. K., Russo,
M., ... & Leipsic, J. (2019). Transcatheter Aortic-Valve Replacement
with a Balloon-Expandable Valve in Low-Risk Patients. New England
Journal of Medicine. DOI: 10.1056/NEJMoa1814052
Mancini, G. J., Gosselin, G., Chow, B., Kostuk, W., Stone, J., Yvorchuk, K. J.,
... & Connelly, K. (2014). Canadian Cardiovascular Society guidelines
journal of cardiology, 114(9), 1447-1455.
https://doi.org/10.1016/j.amjcard.2014.07.081
Joseph, J., Naqvi, S. Y., Giri, J., & Goldberg, S. (2017). Aortic stenosis:
pathophysiology, diagnosis, and therapy. The American journal of
medicine, 130(3), 253-263.
https://doi.org/10.1016/j.amjmed.2016.10.005
Kapadia, S. R., Leon, M. B., Makkar, R. R., Tuzcu, E. M., Svensson, L. G.,
Kodali, S., ... & Babaliaros, V. C. (2015). 5-year outcomes of
transcatheter aortic valve replacement compared with standard
treatment for patients with inoperable aortic stenosis (PARTNER 1): a
randomised controlled trial. The Lancet, 385(9986), 2485-2491.
https://doi.org/10.1016/S0140-6736(15)60290-2
Leon, M. B., Smith, C. R., Mack, M. J., Makkar, R. R., Svensson, L. G.,
Kodali, S. K., ... & Doshi, D. (2016). Transcatheter or surgical aortic-
valve replacement in intermediate-risk patients. New England Journal
of Medicine, 374(17), 1609-1620. DOI: 10.1056/NEJMoa1514616
Leon, M. B., Smith, C. R., Mack, M. J., Makkar, R. R., Svensson, L. G.,
Kodali, S. K., ... & Doshi, D. (2016). Transcatheter or surgical aortic-
valve replacement in intermediate-risk patients. New England Journal
of Medicine, 374(17), 1609-1620. DOI: 10.1056/NEJMoa1514616
Leon, M. B., Smith, C. R., Mack, M., Miller, D. C., Moses, J. W., Svensson, L.
G., ... & Brown, D. L. (2010). Transcatheter aortic-valve implantation
for aortic stenosis in patients who cannot undergo surgery. New
England Journal of Medicine, 363(17), 1597-1607. DOI:
10.1056/NEJMoa1008232
Mack, M. J., Leon, M. B., Thourani, V. H., Makkar, R., Kodali, S. K., Russo,
M., ... & Leipsic, J. (2019). Transcatheter Aortic-Valve Replacement
with a Balloon-Expandable Valve in Low-Risk Patients. New England
Journal of Medicine. DOI: 10.1056/NEJMoa1814052
Mancini, G. J., Gosselin, G., Chow, B., Kostuk, W., Stone, J., Yvorchuk, K. J.,
... & Connelly, K. (2014). Canadian Cardiovascular Society guidelines
⊘ This is a preview!⊘
Do you want full access?
Subscribe today to unlock all pages.
Trusted by 1+ million students worldwide
1 out of 14
Related Documents




Your All-in-One AI-Powered Toolkit for Academic Success.
+13062052269
info@desklib.com
Available 24*7 on WhatsApp / Email
![[object Object]](/_next/static/media/star-bottom.7253800d.svg)
Unlock your academic potential
Copyright © 2020–2026 A2Z Services. All Rights Reserved. Developed and managed by ZUCOL.